
Microleakage of Restorative Materials Used for Temporization of Endodontic Access Cavities
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Temporary Filling Materials
2.2. Bacterial Strains
2.3. Determination of Antibiotic Susceptibility Profiles
2.4. Preparation of Human-Extracted Teeth
2.5. Preparation of 3D-Printed Hollow Test Specimens
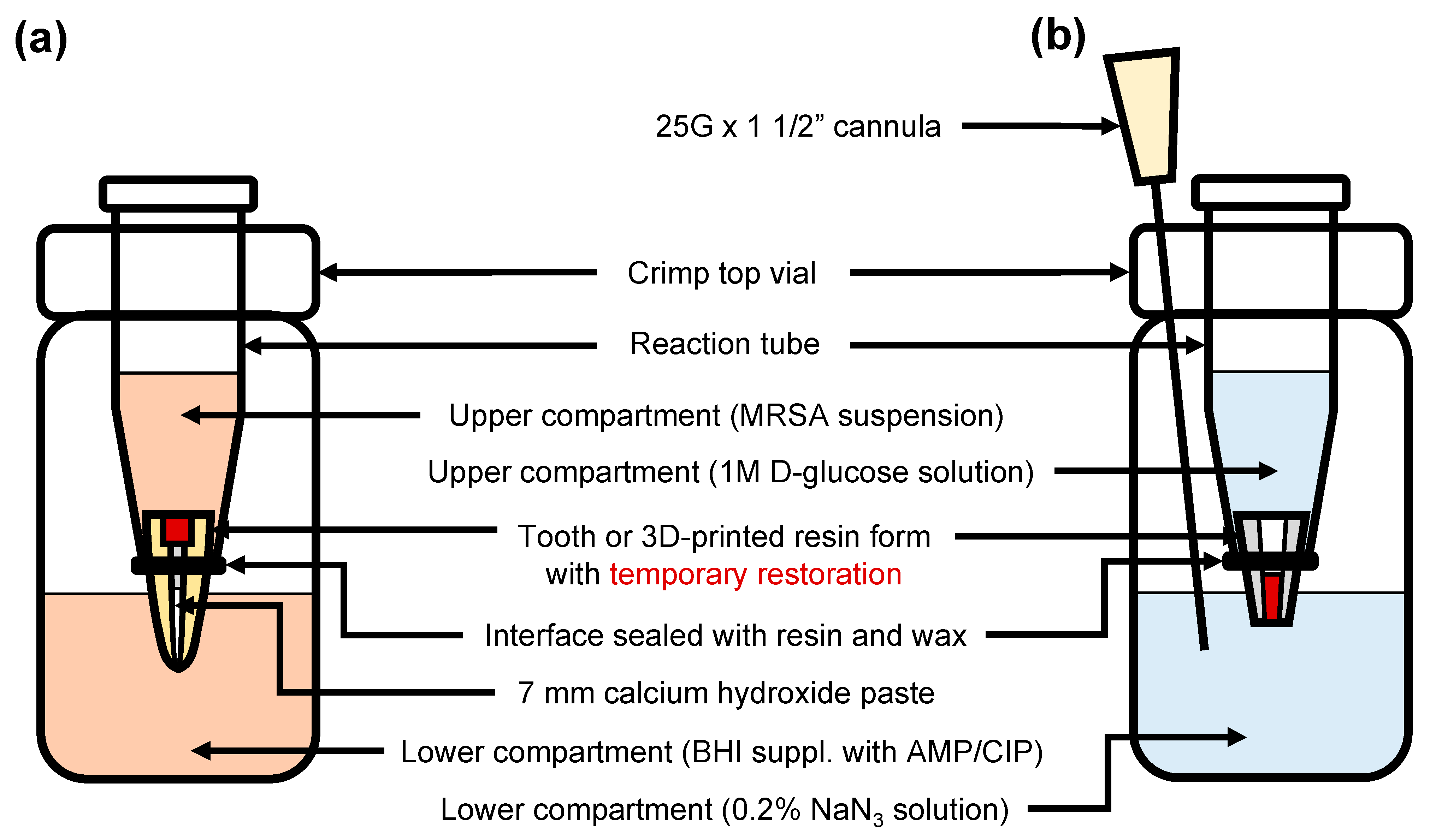
2.6. Bacterial Penetration
2.7. Quantitative Microleakage
2.8. Statistical Analyses
3. Results
3.1. Minimum Inhibitory Concentrations
3.2. Bacterial Penetration
3.3. Glucose Leakage
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nair, P.N.R. On the Causes of Persistent Apical Periodontitis: A Review. Int. Endod. J. 2006, 39, 249–281. [Google Scholar] [CrossRef] [PubMed]
- Giovarruscio, M.; Sauro, S.; Makeeva, I.; Foschi, F. Strategies to Reduce the Risk of Reinfection and Cross-Contamination in Endodontics. Clin. Dent. Rev. 2019, 3, 8. [Google Scholar] [CrossRef] [Green Version]
- Ørstavik, D.; Qvist, V.; Stoltze, K. A Multivariate Analysis of the Outcome of Endodontic Treatment. Eur. J. Oral Sci. 2004, 112, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Ray, H.A.; Trope, M. Periapical Status of Endodontically Treated Teeth in Relation to the Technical Quality of the Root Filling and the Coronal Restoration. Int. Endod. J. 1995, 28, 12–18. [Google Scholar] [CrossRef]
- Abbott, P.V. Factors Associated with Continuing Pain in Endodontics. Aust. Dent. J. 1994, 39, 157–161. [Google Scholar] [CrossRef]
- Naoum, H.J.; Chandler, N.P. Temporization for Endodontics. Int. Endod. J. 2002, 35, 964–978. [Google Scholar] [CrossRef]
- Chen, P.; Chen, Z.; Teoh, Y.-Y.; Peters, O.A.; Peters, C.I. Orifice Barriers to Prevent Coronal Microleakage after Root Canal Treatment: Systematic Review and Meta-Analysis. Aust. Dent. J. 2023, 68, 78–91. [Google Scholar] [CrossRef]
- Chailertvanitkul, P.; Abbott, P.V.; Riley, T.V.; Sooksuntisakoonchai, N. Bacterial and Dye Penetration through Interim Restorations Used during Endodontic Treatment of Molar Teeth. J. Endod. 2009, 35, 1017–1022. [Google Scholar] [CrossRef]
- De Castro, P.H.D.F.; Pereira, J.V.; Sponchiado, E.C.J.; Marques, A.A.F.; Garcia, L.D.F.R. Evaluation of Marginal Leakage of Different Temporary Restorative Materials in Endodontics. Contemp. Clin. Dent. 2013, 4, 472–475. [Google Scholar] [CrossRef]
- Odabas, M.E.; Tulunoglu, O.; Ozalp, S.O.; Bodur, H. Microleakage of Different Temporary Filling Materials in Primary Teeth. J. Clin. Pediatr. Dent. 2009, 34, 157–160. [Google Scholar] [CrossRef]
- McDougal, R.A.; Delano, E.O.; Caplan, D.; Sigurdsson, A.; Trope, M. Success of an Alternative for Interim Management of Irreversible Pulpitis. J. Am. Dent. Assoc. 2004, 135, 1707–1712. [Google Scholar] [CrossRef] [PubMed]
- Barthel, C.R.; Strobach, A.; Briedigkeit, H.; Göbel, U.B.; Roulet, J.F. Leakage in Roots Coronally Sealed with Different Temporary Fillings. J. Endod. 1999, 25, 731–734. [Google Scholar] [CrossRef] [PubMed]
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing, 30th ed.; CLSI Supplement M100; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2020. [Google Scholar]
- CLSI. Methods for Antimicrobial Dilution and Disk Susceptibility Testing of Infrequently Isolated or Fastidious Bacteria, 3rd ed.; CLSI Supplement M45; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2015. [Google Scholar]
- Torabinejad, M.; Rastegar, A.F.; Kettering, J.D.; Pitt Ford, T.R. Bacterial Leakage of Mineral Trioxide Aggregate as a Root-End Filling Material. J. Endod. 1995, 21, 109–112. [Google Scholar] [CrossRef] [PubMed]
- Wuersching, S.N.; Diegritz, C.; Hickel, R.; Huth, K.C.; Kollmuss, M. A Comprehensive In Vitro Comparison of the Biological and Physicochemical Properties of Bioactive Root Canal Sealers. Clin. Oral Investig. 2022, 26, 6209–6222. [Google Scholar] [CrossRef] [PubMed]
- Xu, Q.; Fan, M.; Fan, B.; Cheung, G.S.P.; Hu, H. A New Quantitative Method Using Glucose for Analysis of Endodontic Leakage. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 99, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Kollmuss, M.; Preis, C.E.; Kist, S.; Hickel, R.; Huth, K.C. Differences in Physical Characteristics and Sealing Ability of Three Tricalcium Silicate-Based Cements Used as Root-End-Filling Materials. Am. J. Dent. 2017, 30, 185–189. [Google Scholar]
- van Rossum, G.; Drake, F.L. Python 3 Reference Manual; CreateSpace: Scotts Valley, CA, USA, 2019. [Google Scholar]
- Mergoni, G.; Ganim, M.; Lodi, G.; Figini, L.; Gagliani, M.; Manfredi, M. Single versus Multiple Visits for Endodontic Treatment of Permanent Teeth. Cochrane Database Syst. Rev. 2022, 12, CD005296. [Google Scholar] [CrossRef]
- Schwendicke, F.; Göstemeyer, G. Single-Visit or Multiple-Visit Root Canal Treatment: Systematic Review, Meta-Analysis and Trial Sequential Analysis. BMJ Open 2017, 7, e013115. [Google Scholar] [CrossRef] [Green Version]
- Sjögren, U.; Figdor, D.; Persson, S.; Sundqvist, G. Influence of Infection at the Time of Root Filling on the Outcome of Endodontic Treatment of Teeth with Apical Periodontitis. Int. Endod. J. 1997, 30, 297–306. [Google Scholar] [CrossRef]
- Smith, E.A.; Marshall, J.G.; Selph, S.S.; Barker, D.R.; Sedgley, C.M. Nonsteroidal Anti-Inflammatory Drugs for Managing Postoperative Endodontic Pain in Patients Who Present with Preoperative Pain: A Systematic Review and Meta-Analysis. J. Endod. 2017, 43, 7–15. [Google Scholar] [CrossRef]
- Siqueira, J.F.J.; Rôças, I.N. Clinical Implications and Microbiology of Bacterial Persistence after Treatment Procedures. J. Endod. 2008, 34, 1291–1301.e3. [Google Scholar] [CrossRef] [PubMed]
- Sundqvist, G.; Figdor, D.; Persson, S.; Sjögren, U. Microbiologic Analysis of Teeth with Failed Endodontic Treatment and the Outcome of Conservative Re-Treatment. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1998, 85, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Gaeta, C.; Marruganti, C.; Ali, I.A.A.; Fabbro, A.; Pinzauti, D.; Santoro, F.; Neelakantan, P.; Pozzi, G.; Grandini, S. The Presence of Enterococcus Faecalis in Saliva as a Risk Factor for Endodontic Infection. Front. Cell. Infect. Microbiol. 2023, 13, 1061645. [Google Scholar] [CrossRef] [PubMed]
- Kampfer, J.; Göhring, T.N.; Attin, T.; Zehnder, M. Leakage of Food-Borne Enterococcus Faecalis through Temporary Fillings in a Simulated Oral Environment. Int. Endod. J. 2007, 40, 471–477. [Google Scholar] [CrossRef]
- Stuart, C.H.; Schwartz, S.A.; Beeson, T.J.; Owatz, C.B. Enterococcus Faecalis: Its Role in Root Canal Treatment Failure and Current Concepts in Retreatment. J. Endod. 2006, 32, 93–98. [Google Scholar] [CrossRef]
- Waltimo, T.; Trope, M.; Haapasalo, M.; Ørstavik, D. Clinical Efficacy of Treatment Procedures in Endodontic Infection Control and One Year Follow-up of Periapical Healing. J. Endod. 2005, 31, 863–866. [Google Scholar] [CrossRef] [Green Version]
- Veríssimo, D.M.; do Vale, M.S. Methodologies for Assessment of Apical and Coronal Leakage of Endodontic Filling Materials: A Critical Review. J. Oral Sci. 2006, 48, 93–98. [Google Scholar] [CrossRef] [Green Version]
- Taylor, M.J.; Lynch, E. Microleakage. J. Dent. 1992, 20, 3–10. [Google Scholar] [CrossRef]
- Souza, E.M.; Pappen, F.G.; Shemesh, H.; Bonanato-Estrela, C.; Bonetti-Filho, I. Reliability of Assessing Dye Penetration along Root Canal Fillings Using Methylene Blue. Aust. Endod. J. 2009, 35, 158–163. [Google Scholar] [CrossRef]
- Friedman, S.; Shani, J.; Stabholz, A.; Kaplawi, J. Comparative Sealing Ability of Temporary Filling Materials Evaluated by Leakage of Radiosodium. Int. Endod. J. 1986, 19, 187–193. [Google Scholar] [CrossRef]
- Timpawat, S.; Amornchat, C.; Trisuwan, W.R. Bacterial Coronal Leakage after Obturation with Three Root Canal Sealers. J. Endod. 2001, 27, 36–39. [Google Scholar] [CrossRef] [PubMed]
- Kist, S.; Kollmuss, M.; Jung, J.; Schubert, S.; Hickel, R.; Huth, K.C. Comparison of Ozone Gas and Sodium Hypochlorite/Chlorhexidine Two-Visit Disinfection Protocols in Treating Apical Periodontitis: A Randomized Controlled Clinical Trial. Clin. Oral Investig. 2017, 21, 995–1005. [Google Scholar] [CrossRef] [PubMed]
- Shemesh, H.; Souza, E.M.; Wu, M.-K.; Wesselink, P.R. Glucose Reactivity with Filling Materials as a Limitation for Using the Glucose Leakage Model. Int. Endod. J. 2008, 41, 869–872. [Google Scholar] [CrossRef]
- Demarco, F.F.; Cenci, M.S.; Montagner, A.F.; de Lima, V.P.; Correa, M.B.; Moraes, R.R.; Opdam, N.J.M. Longevity of Composite Restorations Is Definitely Not Only about Materials. Dent. Mater. 2023, 39, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Beach, C.W.; Calhoun, J.C.; Bramwell, J.D.; Hutter, J.W.; Miller, G.A. Clinical Evaluation of Bacterial Leakage of Endodontic Temporary Filling Materials. J. Endod. 1996, 22, 459–462. [Google Scholar] [CrossRef] [PubMed]
- Blaney, T.D.; Peters, D.D.; Setterstrom, J.; Bernier, W.E. Marginal Sealing Quality of IRM and Cavit as Assessed by Microbiol Penetration. J. Endod. 1981, 7, 453–457. [Google Scholar] [CrossRef]
- Ciftçi, A.; Vardarli, D.A.; Sönmez, I.S. Coronal Microleakage of Four Endodontic Temporary Restorative Materials: An In Vitro Study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 108, e67–e70. [Google Scholar] [CrossRef]
- Tulunoglu, O.; Uçtasli, M.B.; Ozdemir, S. Coronal Microleakage of Temporary Restorations in Previously Restored Teeth with Amalgam and Composite. Oper. Dent. 2005, 30, 331–337. [Google Scholar]
- Križnar, I.; Seme, K.; Fidler, A. Bacterial Microleakage of Temporary Filling Materials Used for Endodontic Access Cavity Sealing. J. Dent. Sci. 2016, 11, 394–400. [Google Scholar] [CrossRef] [Green Version]
- Adnan, S.; Khan, F.R. Comparison of Micro-Leakage around Temporary Restorative Materials Placed in Complex Endodontic Access Cavities: An In-Vitro Study. J. Coll. Physicians Surg. Pak. 2016, 26, 182–186. [Google Scholar]
- Widerman, F.H.; Eames, W.B.; Serene, T.P. The Physical and Biologic Properties of Cavit. J. Am. Dent. Assoc. 1971, 82, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Wongsorachai, R.N.; Thanatvarakorn, O.; Prasansuttiporn, T.; Jittidecharaks, S.; Hosaka, K.; Foxton, R.M.; Nakajima, M. Effect of Polymerization Accelerator on Bond Strength to Eugenol-Contaminated Dentin. J. Adhes. Dent. 2018, 20, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Fujisawa, S.; Kadoma, Y. Effect of Phenolic Compounds on the Polymerization of Methyl Methacrylate. Dent. Mater. 1992, 8, 324–326. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Material | Manufacturer | LOT Number | Material Class | Application Procedure |
|---|---|---|---|---|
| Cavit W (CW) | 3M (St. Paul, MN, USA) | 618059 | Eugenol-free calcium sulphate-zinc oxide-based cement | Apply a 5 mm layer (3 mm for double-layer restorations) to cavity, add moisture to cavity |
| Ketac Molar Aplicap (KM) | 3M | 624122 | Glass ionomer cement | Activate capsule for 2 s, mix at 4300 rpm for 10 s, apply a 2 mm layer to cavity |
| Smart Dentin Replacement flow+ (SDR) | Dentsply Sirona (York, PA, USA) | 1604000968 | Flowable bulk fill composite | Apply adhesive (Scotchbond Universal) to cavity, air dry for 5 s, light cure for 20 s, apply a 3 mm layer of SDR to cavity, light-cure for 20 s |
| Intermediate restorative material (IRM) | Dentsply Sirona | 1606000692 | Zinc oxide eugenol cement | Mix powder and liquid, apply a 3 mm layer to cavity |
| Clip F (CF) | Voco Dental GmbH (Cuxhaven, Germany) | 1615395 | Fluoride-releasing, light-curing restorative material | Apply a 5 mm thick layer to cavity, light cure for 40 s |
| Strain | Antibiotic | Range | MIC (µg/mL) | Interpretation |
|---|---|---|---|---|
| S. mutans | Ampicillin | 0.016–256 | 0.094 | S |
| Ciprofloxacin | 0.002–32 | 1.00 | S | |
| A. actinomycetemcomitans | Ampicillin | 0.016–256 | 1.00 | S |
| Ciprofloxacin | 0.002–32 | 0.004 | S | |
| MRSA | Ampicillin | 0.016–256 | >256 | R |
| Ciprofloxacin | 0.002–32 | >32 | R |
| Cavit W | Cavit W + Ketac Molar | Cavit W + SDR | IRM + Ketac Molar | Clip F | |
|---|---|---|---|---|---|
| AUC Teeth | 6.20 | 14.00 | 17.20 | 14.30 | 16.40 |
| Success after 14 days (%) | 6.67 | 46.67 | 66.67 | 53.33 | 66.67 |
| Success after 28 days (%) | 6.67 | 20.00 | 40.00 | 33.33 | 26.67 |
| AUC Hollow test specimens | 4.93 | 13.17 | 26.80 | 13.07 | 26.07 |
| Success after 14 days (%) | 6.67 | 33.33 | 100.00 | 33.33 | 100.00 |
| Success after 28 days (%) | 0.00 | 33.33 | 93.33 | 13.33 | 86.67 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wuersching, S.N.; Moser, L.; Obermeier, K.T.; Kollmuss, M. Microleakage of Restorative Materials Used for Temporization of Endodontic Access Cavities. J. Clin. Med. 2023, 12, 4762. https://doi.org/10.3390/jcm12144762
Wuersching SN, Moser L, Obermeier KT, Kollmuss M. Microleakage of Restorative Materials Used for Temporization of Endodontic Access Cavities. Journal of Clinical Medicine. 2023; 12(14):4762. https://doi.org/10.3390/jcm12144762
Chicago/Turabian StyleWuersching, Sabina Noreen, Luise Moser, Katharina Theresa Obermeier, and Maximilian Kollmuss. 2023. "Microleakage of Restorative Materials Used for Temporization of Endodontic Access Cavities" Journal of Clinical Medicine 12, no. 14: 4762. https://doi.org/10.3390/jcm12144762