

Associations between Periodontal Status and Liver Function in the Japanese Population: A Cross-Sectional Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Clinical Examinations
2.3. Statistical Analysis
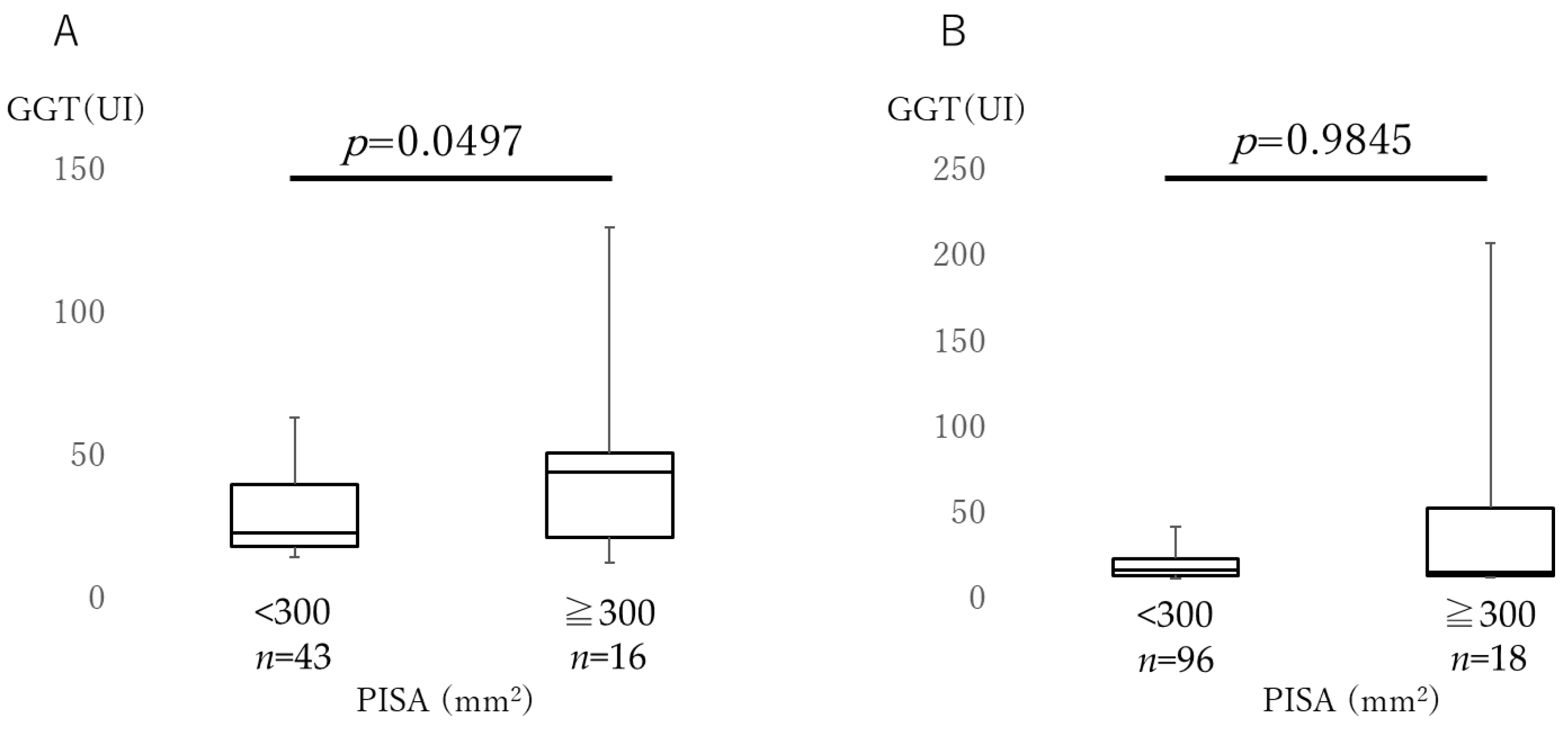
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Papapanou, P.N. Periodontal diseases: Epidemiology. Ann. Periodontol. 1996, 1, 1–36. [Google Scholar] [CrossRef] [PubMed]
- Rapp, L.; Sourdet, S.; Vellas, B.; Lacoste-Ferré, M.H. Oral health and the frail elderly. J. Frailty Aging 2017, 6, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Beck, J.D.; Papapanou, P.N.; Philips, K.H.; Offenbacher, S. Periodontal Medicine: 100 Years of Progress. J. Dent. Res. 2019, 98, 1053–1062. [Google Scholar] [CrossRef] [PubMed]
- Hajishengallis, G.; Lamont, R.J.; Koo, H. Oral polymicrobial communities: Assembly, function, and impact on diseases. Cell Host Microbe 2023, 31, 528–538. [Google Scholar] [CrossRef]
- Dominy, S.S.; Lynch, C.; Ermini, F.; Benedyk, M.; Marczyk, A.; Konradi, A.; Nguyen, M.; Haditsch, U.; Raha, D.; Griffin, C.; et al. Porphyromonas gingivalis in Alzheimer’s disease brains: Evidence for disease causation and treatment with small-molecule inhibitors. Sci. Adv. 2019, 5, 3333. [Google Scholar] [CrossRef] [Green Version]
- Kitamoto, S.; Nagao-Kitamoto, H.; Jiao, Y.; Gillilland, M.G., III; Hayashi, A.; Imai, J.; Sugihara, K.; Miyoshi, M.; Brazil, J.C.; Kuffa, P.; et al. The intermucosal connection between the mouth and gut in commensal pathobiont-driven colitis. Cell 2020, 182, 447–462. [Google Scholar] [CrossRef]
- Socransky, S.S.; Haffajee, A.D. Dental biofilms: Difficult therapeutic targets. Periodontol. 2000 2002, 28, 12–55. [Google Scholar] [CrossRef]
- Yu, Y.H.; Chasman, D.I.; Buring, J.E.; Rose, L.; Ridker, P.M. Cardiovascular risks associated with incident and prevalent periodontal disease. J. Clin. Periodontol. 2015, 42, 21–28. [Google Scholar] [CrossRef] [Green Version]
- Sanz, M.; Marco Del Castillo, A.; Jepsen, S.; Gonzalez-Juanatey, J.R.; D’Aiuto, F.; Bouchard, P.; Chapple, I.; Dietrich, T.; Gotsman, I.; Graziani, F.; et al. Periodontitis and cardiovascular diseases: Consensus report. J. Clin. Periodontol. 2020, 47, 268–288. [Google Scholar] [CrossRef]
- Polak, D.; Shapira, L. An update on the evidence for pathogenic mechanisms that may link periodontitis and diabetes. J. Clin. Periodontol. 2018, 45, 150–166. [Google Scholar] [CrossRef]
- Li, X.; Kolltveit, K.M.; Tronstad, L.; Olsen, I. Systemic diseases caused by oral infection. Clin. Microbiol. Rev. 2000, 13, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Ceriello, A.; Buysschaert, M.; Chapple, I.; Demmer, R.T.; Graziani, F.; Herrera, D.; Jepsen, S.; Lione, L.; Madianos, P.; et al. Scientific evidence on the links between periodontal diseases and diabetes: Consensus report and guidelines of the joint workshop on periodontal diseases and diabetes by the International Diabetes Federation and the European Federation of Periodontology. J. Clin. Periodontol. 2018, 45, 138–149. [Google Scholar] [CrossRef]
- Priyamvara, A.; Dey, A.K.; Bandyopadhyay, D.; Katikineni, V.; Zaghlol, R.; Basyal, B.; Barssoum, K.; Amarin, R.; Bhatt, D.L.; Lavie, C.J. Periodontal Inflammation and the Risk of Cardiovascular Disease. Curr. Atheroscler. Rep. 2020, 22, 28. [Google Scholar] [CrossRef]
- Chen, Y.; Yang, Y.C.; Zhu, B.L.; Wu, C.C.; Lin, R.F.; Zhang, X. Association between periodontal disease, tooth loss and liver diseases risk. J. Clin. Periodontol. 2020, 47, 1053–1063. [Google Scholar] [CrossRef] [PubMed]
- Tajiri, K.; Shimizu, Y. Liver physiology and liver diseases in the elderly. World J. Gastroenterol. 2013, 46, 8459–8467. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.; Hydes, T.; Hamid, A.; Cuthbertson, D.J. Emerging and Established Therapeutic Approaches for Nonalcoholic Fatty Liver Disease. Clin. Ther. 2021, 43, 1476–1504. [Google Scholar] [CrossRef] [PubMed]
- Hamed, A.E.; Elsahar, M.; Elwan, N.M.; El-Nakeep, S.; Naguib, M.; Soliman, H.H.; Ahmed Aboubakr, A.; AbdelMaqsod, A.; Sedrak, H.; Assaad, S.N.; et al. Managing diabetes and liver disease association. Arab. J. Gastroenterol. 2018, 19, 166–179. [Google Scholar] [CrossRef]
- Zhang, H.; Wang, Y.; Chen, C.; Wang, B.; Chen, J.; Tan, X.; Xia, F.; Zhang, J.; Lu, Y.; Wang, N. Non-alcoholic fatty liver disease, sleep behaviors, and incident type 2 diabetes. J. Gastroenterol. Hepatol. 2022, 37, 1633–1640. [Google Scholar] [CrossRef]
- Delire, B.; Lebrun, V.; Selvais, C.; Henriet, P.; Bertrand, A.; Horsmans, Y.; Leclercq, I.A. Aging enhances liver fibrotic response in mice through hampering extracellular matrix remodeling. Aging 2016, 9, 98–113. [Google Scholar] [CrossRef] [Green Version]
- Maddrey, W.C. Alcohol-induced liver disease. Clin. Liver Dis. 2000, 4, 115–131. [Google Scholar] [CrossRef]
- Nagasaki, A.; Sakamoto, S.; Arai, T.; Kato, M.; Ishida, E.; Furusho, H.; Fujii, M.; Takata, T.; Miyauchi, M. Elimination of porphyromonas gingivalis inhibits liver fibrosis and inflammation in NASH. J. Clin. Periodontol. 2021, 48, 1367–1378. [Google Scholar] [CrossRef] [PubMed]
- Komazaki, R.; Katagiri, S.; Takahashi, H.; Maekawa, S.; Shiba, T.; Takeuchi, Y.; Kitajima, Y.; Ohtsu, A.; Udagawa, S.; Sasaki, N.; et al. Periodontal pathogenic bacteria, Aggregatibacter actinomycetemcomitans affect non-alcoholic fatty liver disease by altering gut microbiota and glucose metabolism. Sci. Rep. 2017, 7, 13950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, S.; Kamata, Y.; Kessoku, T.; Shimizu, T.; Kobayashi, T.; Kurihashi, T.; Takashiba, S.; Hatanaka, K.; Hamada, N.; Kodama, T.; et al. A cross-sectional study assessing the relationship between non-alcoholic fatty liver disease and periodontal disease. Sci. Rep. 2022, 12, 13621. [Google Scholar] [CrossRef] [PubMed]
- Hatasa, M.; Yoshida, S.; Takahashi, H.; Tanaka, K.; Kubotsu, Y.; Ohsugi, Y.; Katagiri, T.; Iwata, T.; Katagiri, S. Relationship between NAFLD and Periodontal Disease from the View of Clinical and Basic Research, and Immunological Response. Int. J. Mol. Sci. 2021, 22, 3728. [Google Scholar] [CrossRef]
- Katzke, V.; Johnson, T.; Sookthai, D.; Hüsing, A.; Kühn, T.; Kaaks, R. Circulating liver enzymes and risks of chronic diseases and mortality in the prospective EPIC-Heidelberg case-cohort study. BMJ Open 2020, 10, e033532. [Google Scholar] [CrossRef] [Green Version]
- Čolak, D.; Pintar, T.; Cmok Kučič, A.; Salobir, J.; Gašpirc, B.; Gašperšič, R. Periodontal and Hepatic Parameters in Obese Patients Undergoing Bariatric Surgery. Oral Health Prev. Dent. 2022, 20, 295–304. [Google Scholar]
- Kwo, P.Y.; Cohen, S.M.; Lim, J.K. ACG clinical guideline: Evaluation of abnormal liver chemistries. Am. J. Gastroenterol. 2017, 112, 18–35. [Google Scholar] [CrossRef]
- Quan, Y.; Tian, G.E.; Zhou, J.T.; Wu, W.C.; Liu, X.J. The observation of liver and kidney injury and the activation of macrophages in the overload pressure induced cardiac hypertrophy/heart failure mouse model. Sichuan Da Xue Xue Bao Yi Xue Ban 2020, 51, 331–336. [Google Scholar]
- Whitfield, J.B. Gamma glutamyl transferase. Crit. Rev. Clin. Lab. Sci. 2001, 38, 263–355. [Google Scholar] [CrossRef]
- Xing, M.; Gao, M.; Li, J.; Han, P.; Mei, L.; Zhao, L. Characteristics of peripheral blood Gamma-glutamyl transferase in different liver diseases. Medicine 2022, 101, e28443. [Google Scholar] [CrossRef]
- Koenig, G.; Seneff, S. Gamma-glutamyltransferase: A predictive biomarker of cellular antioxidant inadequacy and disease risk. Dis. Markers 2015, 2015, 818570. [Google Scholar] [CrossRef] [Green Version]
- Rinella, M.E.; Lazarus, J.V.; Ratziu, V.; Francque, S.M.; Sanyal, A.J.; Kanwal, F.; Romero, D.; Abdelmalek, M.F.; Anstee, Q.M.; Arab, J.P.; et al. A multi-society Delphi consensus statement on new fatty liver disease nomenclature. Hepatology 2023, 101133. [Google Scholar] [CrossRef]
- Nesse, W.; Abbas, F.; van der Ploeg, I.; Spijkervet, F.K.; Dijkstra, P.U.; Vissink, A. Periodontal inflamed surface area: Quantifying inflammatory burden. J. Clin. Periodontol. 2008, 35, 668–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamata, Y.; Kessoku, T.; Shimizu, T.; Sato, S.; Kobayashi, T.; Kurihashi, T.; Morozumi, T.; Iwasaki, T.; Takashiba, S.; Hatanaka, K.; et al. Periodontal Treatment and Usual Care for Nonalcoholic Fatty Liver Disease: A Multicenter, Randomized Controlled Trial. Clin. Transl. Gastroenterol. 2022, 13, 00520. [Google Scholar] [CrossRef] [PubMed]
- Leira, Y.; Martín-Lancharro, P.; Blanco, J. Periodontal inflamed surface area and periodontal case definition classification. Acta Odontol. Scand. 2018, 76, 195–198. [Google Scholar] [CrossRef]
- Pietropaoli, D.; Del Pinto, R.; Ferri, C.; Marzo, G.; Giannoni, M.; Ortu, E.; Monaco, A. Association between periodontal inflammation and hypertension using periodontal inflamed surface area and bleeding on probing. J. Clin. Periodontol. 2020, 47, 160–172. [Google Scholar] [CrossRef]
- Nesse, W.; Linde, A.; Abbas, F.; Spijkervet, F.K.; Dijkstra, P.U.; de Brabander, E.C.; Gerstenbluth, I.; Vissink, A. Dose-response relationship between periodontal inflamed surface area and HbA1c in type 2 diabetics. J. Clin. Periodontol. 2009, 36, 295–300. [Google Scholar] [CrossRef] [Green Version]
- Widita, E.; Yoshihara, A.; Hanindriyo, L.; Miyazaki, H. Relationship between clinical periodontal parameters and changes in liver enzymes levels over an 8-year period in an elderly Japanese population. J. Clin. Periodontol. 2018, 45, 311–321. [Google Scholar] [CrossRef]
- Zhang, F.; Zhao, D.; Xu, X.; Wen, P.; Li, H.; Yu, R.; Cheng, T.; Zheng, Z.; Yang, H.; Yang, C.; et al. Periodontitis links to concurrent metabolic disorders and abnormal liver function in pregnant women. Oral Dis. 2022. [Google Scholar] [CrossRef]
- Koyama, T.; Hamada, H.; Nishida, M.; Naess, P.A.; Gaarder, C.; Sakamoto, T. Defining the optimal cut-off values for liver enzymes in diagnosing blunt liver injury. BMC Res. Notes 2016, 9, 41. [Google Scholar] [CrossRef] [Green Version]
- Iwasaki, T.; Hirose, A.; Azuma, T.; Ohashi, T.; Watanabe, K.; Obora, A.; Deguchi, F.; Kojima, T.; Isozaki, A.; Tomofuji, T. Correlation between ultrasound-diagnosed non-alcoholic fatty liver and periodontal condition in a cross-sectional study in Japan. Sci. Rep. 2018, 8, 7496. [Google Scholar] [CrossRef] [PubMed]
- Duseja, A.; Chahal, G.S.; Jain, A.; Mehta, M.; Ranjan, A.; Grover, V. Association between nonalcoholic fatty liver disease and inflammatory periodontal disease: A case-control study. J. Indian Soc. Periodontol. 2021, 25, 47–54. [Google Scholar] [PubMed]
- Takagi, Y. Enzyme. In Standard Clinical Laboratory Medicine, 4th ed.; Takagi, Y., Yamada, T., Eds.; Igaku-Shoin Ltd.: Tokyo, Japan, 2013; pp. 203–217. [Google Scholar]
- Helenius-Hietala, J.; Suominen, A.L.; Ruokonen, H.; Knuuttila, M.; Puukka, P.; Jula, A.; Meurman, J.H.; Åberg, F. Periodontitis is associated with incident chronic liver disease—A population-based cohort study. Liver Int. 2019, 39, 583–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.Y.; Lee, G.N.; Song, H.C.; Park, Y.M.; Ahn, Y.B.; Han, K.; Ko, S.H. Association between Fatty Liver Index and Periodontitis: The Korea National Health and Nutrition Examination Survey. Sci. Rep. 2020, 10, 3805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuman, M.G.; Malnick, S.; Chertin, L. Gamma glutamyl transferase—An underestimated marker for cardiovascular disease and the metabolic syndrome. J. Pharm. Sci. 2020, 23, 65–74. [Google Scholar] [CrossRef] [Green Version]
- Kuraji, R.; Sekino, S.; Kapila, Y.; Numabe, Y. Periodontal disease-related nonalcoholic fatty liver disease and nonalcoholic steatohepatitis: An emerging concept of oral-liver axis. Periodontol. 2000 2021, 87, 204–240. [Google Scholar] [CrossRef]
- Xu, W.; Zhang, Z.; Yao, L.; Xue, B.; Xi, H.; Wang, X.; Sun, S. Exploration of shared gene signatures and molecular mechanisms between periodontitis and nonalcoholic fatty liver disease. Front. Genet. 2022, 13, 939751. [Google Scholar] [CrossRef]
- Chu, L.; Wu, Y.; Xu, X.; Phillips, L.; Kolodrubetz, D. Glutathione catabolism by Treponema denticola impacts its pathogenic potential. Anaerobe 2020, 62, 102170. [Google Scholar] [CrossRef]
- Morita, T.; Yamazaki, Y.; Fujiharu, C.; Ishii, T.; Seto, M.; Nishinoue, N.; Sasaki, Y.; Kawato, T.; Motohashi, M.; Maeno, M. Serum γ-glutamyltransferase level is associated with periodontal disease independent of drinking habits in Japanese adults. Med. Sci. Monit. 2014, 20, 2109–2116. [Google Scholar]
- Teschke, R.; Rauen, J.; Neuefeind, M.; Petrides, A.S.; Strohmeyer, G. Alcoholic liver disease associated with increased gamma-glutamyltransferase activities in serum and liver. Adv. Exp. Med. Biol. 1980, 132, 647–654. [Google Scholar]
- Park, J.B.; Han, K.; Park, Y.G.; Ko, Y. Association between alcohol consumption and periodontal disease: The 2008 to 2010 Korea National Health and Nutrition Examination Survey. J. Periodontol. 2014, 85, 1521–1528. [Google Scholar] [CrossRef]
- Cobb, C.M.; Sottosanti, J.S. A re-evaluation of scaling and root planning. J. Periodontol. 2021, 92, 1370–1378. [Google Scholar] [CrossRef] [PubMed]
- Aydinyurt, H.S.; Akbal, D.; Altindal, D.; Bozoglan, A.; Ertugrul, A.S.; Demir, H. Evaluation of biochemical and clinical effects of hyaluronic acid on non-surgical periodontal treatment: A randomized controlled trial. Ir. J. Med. Sci. 2020, 189, 1485–1494. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.O.; Esteves Lima, R.P.; Costa, A.M.; Costa, A.A.; Mattos Pereira, G.H.; Cortelli, S.C.; Cortelli, J.R.; Magalhães Cyrino, R.; Aparecida Silva, T.; Miranda Cota, L.O. Adjunctive effects of photodynamic therapy using indocyanine green in residual pockets during periodontal maintenance therapy: A split-mouth randomized controlled trial. J. Periodontol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Youngman, L.D.; Campbell, T.C. Inhibition of aflatoxin B1-induced gamma-glutamyltranspeptidase positive (GGT+) hepatic preneoplastic foci and tumors by low protein diets: Evidence that altered GGT+ foci indicate neoplastic potential. Carcinogen 1992, 13, 1607–1613. [Google Scholar] [CrossRef]
- Yu, L.; Zhou, C.; Wei, Z.; Shi, Z. Effect of combined periodontal-orthodontic treatment on NOD-like receptor protein 3 and high mobility group box-1 expressions in patients with periodontitis and its clinical significance. Medicine 2019, 98, e17724. [Google Scholar] [CrossRef]
- D’Abbondanza, M.; Ministrini, S.; Pucci, G.; Nulli Migliola, E.; Martorelli, E.E.; Gandolfo, V.; Siepi, D.; Lupattelli, G.; Vaudo, G. Very Low-Carbohydrate Ketogenic Diet for the Treatment of Severe Obesity and Associated Non-Alcoholic Fatty Liver Disease: The Role of Sex Differences. Nutrients 2020, 12, 2748. [Google Scholar] [CrossRef]
- Hendriks, H.F.J. Alcohol and Human Health: What Is the Evidence? Ann. Rev. Food Sci. Technol. 2020, 11, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Sankaranarayanan, R.; Saxlin, T.; Knuuttila, M.; Ylöstalo, P.; Suominen, A.L. Alcohol use and the development of periodontal pockets: An 11-year follow-up study. J. Periodontol. 2020, 91, 1621–1631. [Google Scholar] [CrossRef]
- Sankaranarayanan, R.; Keränen, A.L.; Saxlin, T.; Myllykangas, R.; Knuuttila, M.; Ylöstalo, P.; Suominen, A.L. Association between alcohol use and periodontal pockets in Finnish adult population. Acta Odontol. Scand. 2019, 77, 371–379. [Google Scholar] [CrossRef]
- Baeza, M.; Morales, A.; Cisterna, C.; Cavalla, F.; Jara, G.; Isamitt, Y.; Pino, P.; Gamonal, J. Effect of periodontal treatment in patients with periodontitis and diabetes: Systematic review and meta-analysis. J. Appl. Oral Sci. 2020, 28, e20190248. [Google Scholar] [CrossRef]
- Stanko, P.; Holla, L.I. Bidirectional association between diabetes mellitus and inflammatory periodontal disease. A review. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc. Czech Repub. 2014, 158, 35–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aoyama, N.; Fujii, T.; Kida, S.; Nozawa, I.; Taniguchi, K.; Fujiwara, M.; Iwane, T.; Tamaki, K.; Minabe, M. Association of Periodontal Status, Number of Teeth, and Obesity: A Cross-Sectional Study in Japan. J. Clin. Med. 2021, 10, 208. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.Z.; Cheng, X.Q.; Li, J.Y.; Zhang, P.; Yi, P.; Xu, X.; Zhou, X.D. Saliva in the diagnosis of diseases. Int. J. Oral Sci. 2016, 8, 133–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.; Kim, J. Usefulness of salivary testing machine on oral care management: Pilot study. Int. J. Clin. Prev. Dent. 2018, 14, 89–94. [Google Scholar] [CrossRef]
- Bimstein, E.; Small, P.A., Jr.; Magnusson, I. Leukocyte esterase and protein levels in saliva, as indicators of gingival and periodontal diseases in children. Pediatr. Dent. 2004, 26, 310–315. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | |
|---|---|
| n | 173 |
| Sex [female %] | 65.9 |
| Age [years] | 69 (60, 76) 1 |
| Number of teeth | 25 (22, 27) 1 |
| PISA [mm2] | 151.3 (69.8, 270.0) 1 |
| HbA1c [%] | 5.7 (5.4, 6.0) 1 |
| Blood glucose [mg/dL] | 111.0 (98.5, 128.5) 1 |
| Probing depth [mm] | 2.2 (2.1, 2.4) 1 |
| Bleeding on probing [%] | 18 (9, 33) 1 |
| Leukocyte score in saliva | 67 (40, 79) 1 |
| Protein score in saliva | 45 (30, 67) 1 |
| AST [U/L] | 21 (18, 25) 1 |
| ALT [U/L] | 17 (13, 25) 1 |
| GGT [UI] | 20 (16, 35) 1 |
| PISA [mm2] < 300 | PISA [mm2] ≧ 300 | p-Value | |
|---|---|---|---|
| Age [years] | 69 (50, 75) | 71.5 (58, 79) | 0.48 |
| Sex [female %] | 55.5 | 10.4 | 0.07 |
| Number of teeth | 25 (22, 27) | 26 (22, 28) | 0.40 |
| HbA1c [%] | 5.6 (5.4, 5.9) | 5.8 (5.4, 6.4) | 0.24 |
| Blood glucose [mg/dL] | 110 (98, 127) | 112 (99, 175) | 0.25 |
| Probing depth [mm] | 2.2 (2.0, 2.4) | 3.0 (2.5, 3.3) | <0.0001 |
| Bleeding on probing [%] | 14 (8, 23) | 47 (35, 62) | <0.0001 |
| Leukocyte score in saliva | 59 (35, 77) | 77 (70, 89) | <0.0001 |
| Protein score in saliva | 42 (28, 65) | 58 (43, 83) | 0.0001 |
| Increased AST [%] | 48.2 | 52.9 | 0.62 |
| Increased ALT [%] | 35.3 | 47.0 | 0.20 |
| Increased GGT [%] | 10.8 | 29.4 | 0.0056 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fujii, T.; Aoyama, N.; Kida, S.; Taniguchi, K.; Yata, T.; Minabe, M.; Komaki, M. Associations between Periodontal Status and Liver Function in the Japanese Population: A Cross-Sectional Study. J. Clin. Med. 2023, 12, 4759. https://doi.org/10.3390/jcm12144759
Fujii T, Aoyama N, Kida S, Taniguchi K, Yata T, Minabe M, Komaki M. Associations between Periodontal Status and Liver Function in the Japanese Population: A Cross-Sectional Study. Journal of Clinical Medicine. 2023; 12(14):4759. https://doi.org/10.3390/jcm12144759
Chicago/Turabian StyleFujii, Toshiya, Norio Aoyama, Sayuri Kida, Kentaro Taniguchi, Tomomi Yata, Masato Minabe, and Motohiro Komaki. 2023. "Associations between Periodontal Status and Liver Function in the Japanese Population: A Cross-Sectional Study" Journal of Clinical Medicine 12, no. 14: 4759. https://doi.org/10.3390/jcm12144759