
The Long-Term Outcome and Quality of Life after Replacement of the Ascending Aorta †
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
- A: Supracoronary replacement of the ascending aorta, n = 35;
- B: Wheat-, David- or Bentall-procedure; n = 86.
2.2. Data Collection
2.3. SF-36 Questionnaire
2.4. Specific Questions
2.5. Surgical Procedures and Postoperative Course
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Surgical Procedures
3.3. Postoperative Outcome and Survival
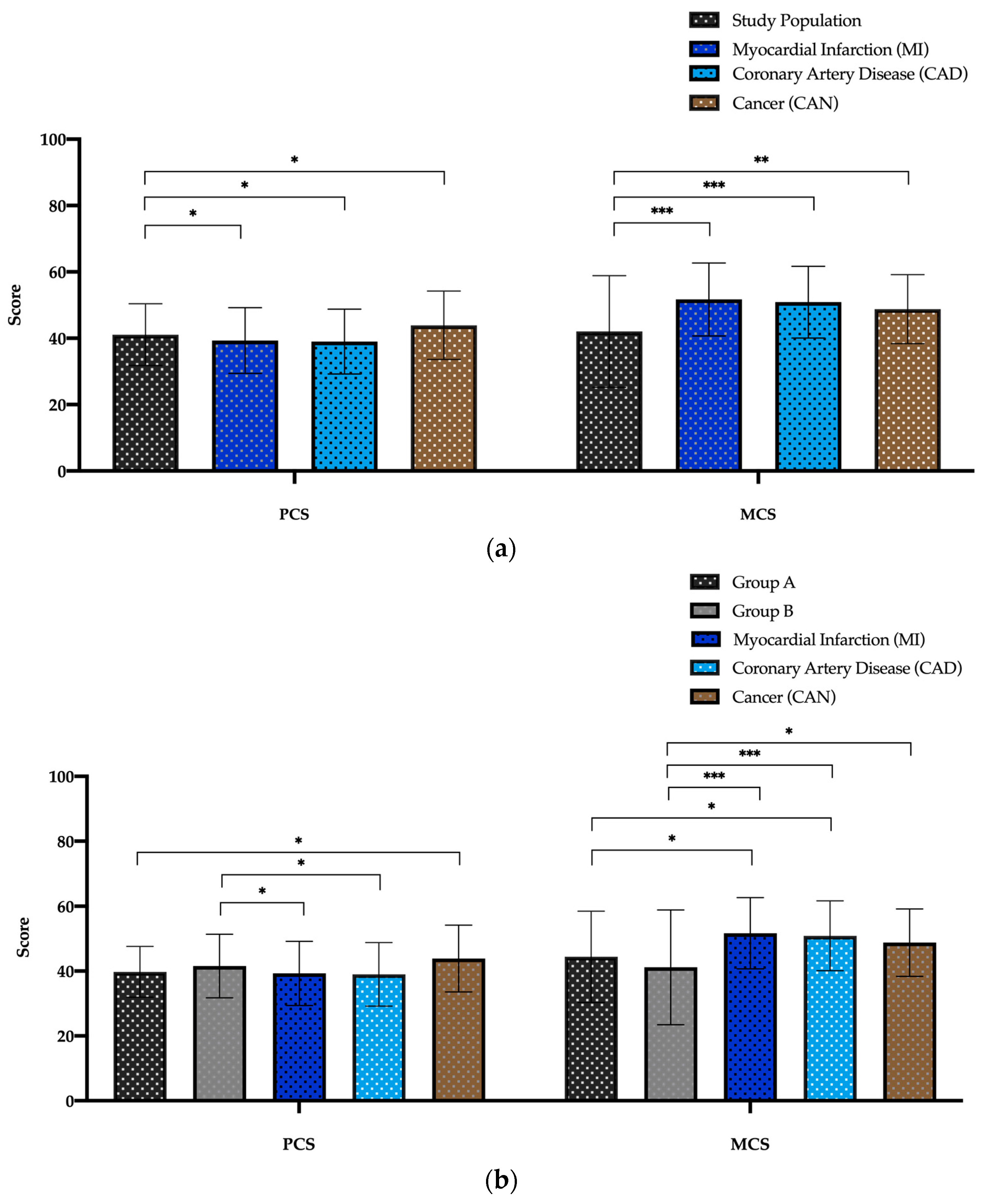
3.4. QoL According to SF-36 Questionnaire
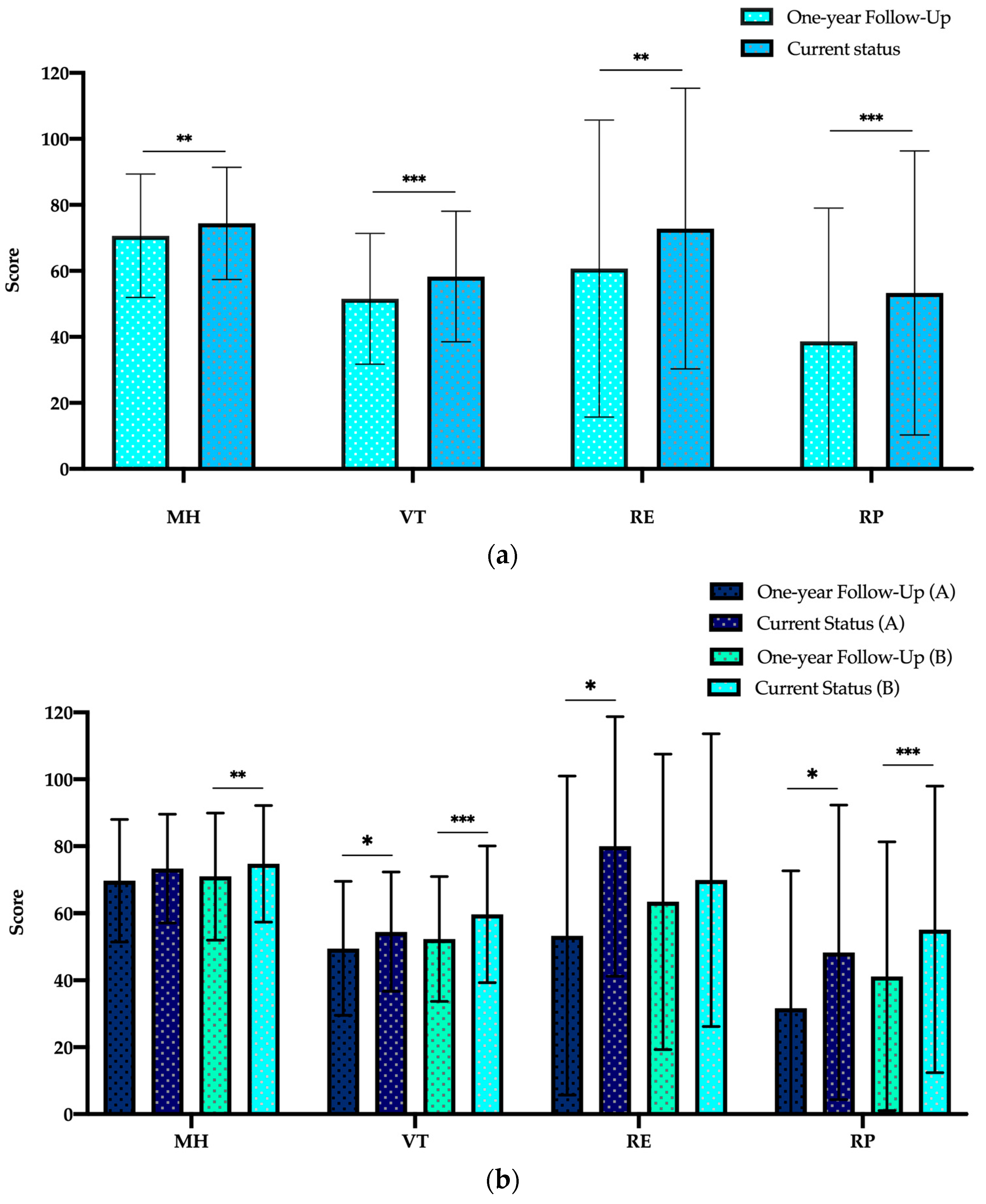
3.5. Follow-Up Questionnaire
4. Discussion
5. Conclusions
6. Limitation
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Elefteriades, J.A. Natural history of thoracic aortic aneurysms: Indications for surgery, and surgical versus nonsurgical risks. Ann. Thorac. Surg. 2002, 74, S1877–S1880; discussion S1892–S1898. [Google Scholar] [CrossRef]
- Borger, M.A.; Preston, M.; Ivanov, J.; Fedak, P.W.M.; Davierwala, P.; Armstrong, S.; David, T.E. Should the ascending aorta be replaced more frequently in patients with bicuspid aortic valve disease? J. Thorac. Cardiovasc. Surg. 2004, 128, 677–683. [Google Scholar] [CrossRef] [Green Version]
- Erbel, R.; Aboyans, V.; Boileau, C.; Bossone, E.; Di Bartolomeo, R.; Eggebrecht, H.; Evangelista, A.; Falk, V.; Frank, H.; Gaemperli, O.; et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2873–2926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Writing Committee Members; Isselbacher, E.M.; Preventza, O.; Black, J.H., III; Augoustides, J.G.; Beck, A.W.; Bolen, M.A.; Braverman, A.C.; Bray, B.E.; Brown-Zimmerman, M.M.; et al. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 80, e223–e393. [Google Scholar] [CrossRef] [PubMed]
- Cohn, L.H.; Rizzo, R.J.; Adams, D.H.; Aranki, S.F.; Couper, G.S.; Beckel, N.; Collins, J.J. Reduced mortality and morbidity for ascending aortic aneurysm resection regardless of cause. Ann. Thorac. Surg. 1996, 62, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Kobuch, R.; Schelker, E.; Hirt, S.; Amann, M.; Diez, C.; Schmid, C. Quality of Life Following Surgery of Ascending Aorta and Aortic Arch with Selective Antegrade Cerebral Perfusion. Thorac. Cardiovasc. Surg. 2012, 60, 496–500. [Google Scholar] [CrossRef]
- Brandt, M.; Abdelkerim, S.; Clemm, S.; Böning, A.; Cremer, J. Composite Valve Graft versus Separate Aortic Valve and Ascending Aortic Replacement. Cardiology 2004, 102, 156–159. [Google Scholar] [CrossRef]
- Stalder, M.; Staffelbach, S.; Immer, F.F.; Englberger, L.; Berdat, P.A.; Eckstein, F.S.; Carrel, T.P. Aortic Root Replacement Does Not Affect Outcome and Quality of Life. Ann. Thorac. Surg. 2007, 84, 775–781. [Google Scholar] [CrossRef]
- Williams, J.B.; Peterson, E.D.; Zhao, Y.; O’Brien, S.M.; Andersen, N.D.; Miller, D.C.; Chen, E.P.; Hughes, G.C. Contemporary Results for Proximal Aortic Replacement in North America. J. Am. Coll. Cardiol. 2012, 60, 1156–1162. [Google Scholar] [CrossRef] [Green Version]
- Houël, R.; Soustelle, C.; Kirsch, M.; Hillion, M.L.; Renaut, C.; Loisance, D.Y. Long-term results of the bentall operation versus separate replacement of the ascending aorta and aortic valve. J. Heart Valve Dis. 2002, 11, 485–491. [Google Scholar]
- Franke, U.F.; Isecke, A.; Nagib, R.; Breuer, M.; Wippermann, J.; Tigges-Limmer, K.; Wahlers, T. Quality of Life after Aortic Root Surgery: Reimplantation Technique Versus Composite Replacement. Ann. Thorac. Surg. 2010, 90, 1869–1875. [Google Scholar] [CrossRef]
- Lohse, F.; Lang, N.; Schiller, W.; Roell, W.; Dewald, O.; Preusse, C.-J.; Welz, A.; Schmitz, C. Quality of life after replacement of the ascending aorta in patients with true aneurysms. Tex. Heart Inst. J. 2009, 36, 104–110. [Google Scholar] [PubMed]
- Olsson, C.; Thelin, S. Quality of life in survivors of thoracic aortic surgery. Ann. Thorac. Surg. 1999, 67, 1262–1267. [Google Scholar] [CrossRef] [PubMed]
- Santini, F.; Montalbano, G.; Messina, A.; Donofrio, A.; Casali, G.; Viscardi, F.; Luciani, G.; Mazzucco, A. Survival and quality of life after repair of acute type A aortic dissection in patients aged 75 years and older justify intervention. Eur. J. Cardio-Thorac. Surg. 2006, 29, 386–391. [Google Scholar] [CrossRef] [Green Version]
- Hamiko, M.; Gestrich, C.; Probst, C.; Mellert, F.; Winkler, K.; Welz, A.; Schiller, W.; Endlich, M. Long-Term Outcome and Quality of Life in Aortic Type A Dissection Survivors. Thorac. Cardiovasc. Surg. 2016, 64, 91–99. [Google Scholar] [CrossRef]
- Jussli-Melchers, J.; Panholzer, B.; Friedrich, C.; Broch, O.; Renner, J.; Schöttler, J.; Rahimi, A.; Cremer, J.; Schoeneich, F.; Haneya, A. Long-term outcome and quality of life following emergency surgery for acute aortic dissection type A: A comparison between young and elderly adults. Eur. J. Cardio-Thorac. Surg. 2017, 51, 465–471. [Google Scholar] [CrossRef]
- Eranki, A.; Wilson-Smith, A.; Williams, M.L.; Saxena, A.; Mejia, R. Quality of life following surgical repair of acute type A aortic dissection: A systematic review. J. Cardiothorac. Surg. 2022, 17, 118. [Google Scholar] [CrossRef]
- Coroneos, C.J.; Mastracci, T.M.; Barlas, S.; Cinà, C.S. The effect of thoracoabdominal aneurysm repair on quality of life. J. Vasc. Surg. 2009, 50, 251–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crawford, R.S.; Pedraza, J.D.; Chung, T.K.; Corey, M.; Conrad, M.F.; Cambria, R.P. Functional outcome after thoracoabdominal aneurysm repair. J. Vasc. Surg. 2008, 48, 828–835.e1. [Google Scholar] [CrossRef] [Green Version]
- Di Luozzo, G.; Shirali, A.S.; Varghese, R.; Lin, H.-M.; Weiss, A.J.; Bischoff, M.S.; Griepp, R.B. Quality of life and survival of septuagenarians and octogenarians after repair of descending and thoracoabdominal aortic aneurysms. J. Thorac. Cardiovasc. Surg. 2013, 145, 378–384. [Google Scholar] [CrossRef] [Green Version]
- Eide, T.M.O.; Romundstad, P.; Klepstad, P.; Myhre, H.O. Health-related quality of life in long term-survivors of thoracoabdominal aortic aneurysm repair. J. Vasc. Nurs. 2005, 23, 88–94; quiz 95. [Google Scholar] [CrossRef]
- Mageae, T.R.; Scott, D.J.; A Dunkley, A.; Johnston, J.S.; Campbell, W.B.; Baird, R.N.; Horrocks, M. Quality of life following surgery for abdominal aortic aneurysm. Br. J. Surg. 1992, 79, 1014–1016. [Google Scholar] [CrossRef] [PubMed]
- Lehr, E.J.; Wang, P.Z.; Oreopoulos, A.; Kanji, H.; Norris, C.; MacArthur, R. Midterm Outcomes and Quality of Life of Aortic Root Replacement: Mechanical vs Biological Conduits. Can. J. Cardiol. 2011, 27, 262.e15–262.e20. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.K.; Gandek, B.; Aaronson, N.K.; Acquadro, C.; Alonso, J.; Apolone, G.; Bullinger, M.; Bjorner, J.; Fukuhara, S.; Kaasa, S.; et al. Cross-cultural comparisons of the content of SF-36 translations across 10 countries: Results from the IQOLA Project. International Quality of Life Assessment. J. Clin. Epidemiol. 1998, 51, 925–932. [Google Scholar] [CrossRef] [PubMed]
- Bullinger, M. German translation and psychometric testing of the SF-36 Health Survey: Preliminary results from the IQOLA Project. International Quality of Life Assessment. Soc. Sci. Med. 1995, 41, 1359–1366. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Ellert, U.; Bellach, B.M. The SF-36 in the Federal Health Survey--description of a current normal sample. Gesundheitswesen 1999, 61, S184–S190. [Google Scholar]
- Barrena-Blázquez, S.; Díez-Alonso, M.; del Moral, L.F.R.; Sanchez-Coll, S.; Alvarez-Mon, M.; Ortega, M.A.; Ruiz-Grande, F. Association of Age and Surgical Technique with the Quality of Life of Male Patients Treated for Abdominal Aorta Aneurysms: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 6580. [Google Scholar] [CrossRef]
- Sharples, L.; Sastry, P.; Freeman, C.; Bicknell, C.; Da Chiu, Y.; Vallabhaneni, S.R.; Cook, A.; Gray, J.; McCarthy, A.; McMeekin, P.; et al. Aneurysm growth, survival, and quality of life in untreated thoracic aortic aneurysms: The effective treatments for thoracic aortic aneurysms study. Eur. Heart J. 2022, 43, 2356–2369. [Google Scholar] [CrossRef]
- Smolock, C.J.; Xiang, F.; Roselli, E.E.; Blackstone, E.H.; Svensson, L.G.; Artis, A.S.; Liu, H.; Tong, M.Z. Health-Related Quality of Life After Extensive Aortic Replacement. Semin. Thorac. Cardiovasc. Surg. 2022, 34, 793–801. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 121) | Group A (n = 35) | Group B (n = 86) | p-Value | |
|---|---|---|---|---|
| Age | 62.02 ± 12.54 | 67.51 ± 9.13 | 59.78 ± 13.08 | 0.003 |
| Sex | <0.001 | |||
| male | 83 (68.6%) | 13 (37.1%) | 70 (81.4%) | |
| female | 38 (31.4%) | 22 (62.9%) | 16 (18.6%) | |
| BMI | 27.67± 5.23 | 28.91 ± 5.18 | 27.17 ± 5.20 | 0.107 |
| Comorbidities | ||||
| Hypertension | 94 (77.7%) | 32 (91.4%) | 62 (72.1%) | 0.021 |
| Hyperlipidemia | 58 (47.9%) | 22 (63.9%) | 36 (41.9%) | 0.036 |
| Diabetes mellitus | 11 (9.1%) | 5 (14.3%) | 6 (7.0%) | 0.293 |
| COPD | 15 (12.4%) | 3 (8.6%) | 12 (14.0%) | 0.550 |
| Smoker | 52 (43.0%) | 16 (45.7%) | 36 (41.9%) | 0.698 |
| pAVD | 4 (3.3%) | 0 (0.0%) | 4 (4.7%) | 0.322 |
| cAVD | 6 (5.0%) | 3 (8.6%) | 3 (3.5%) | 0.354 |
| Stroke | 12 (9.9%) | 3 (8.6%) | 9 (10.5%) | 0.752 |
| Atrial fibrillation (AF) | 38 (31.4%) | 12 (34.3%) | 26 (30.2%) | 0.663 |
| Coronary heart disease (CAD) | 28 (23.1%) | 6 (17.1%) | 22 (25.6%) | 0.318 |
| Myocardial infarction (MI) | 5 (4.1%) | 1 (2.9%) | 4 (4.7%) | 1.000 |
| Former PCI/Stenting | 3 (2.5%) | 1 (2.9%) | 2 (2.3%) | 0.530 |
| Chronic renal failure | 6 (5.0%) | 0 (0.0%) | 6 (7.0%) | 0.180 |
| Ejection fraction | 0.532 | |||
| >50% | 104 (86.0%) | 31 (88.6%) | 73 (84.9%) | |
| 30–50% | 14 (11.6%) | 4 (11.4%) | 10 (11.6%) | |
| <30% | 3 (2.5%) | 0 (0.0%) | 3 (3.5%) | |
| NYHA classification | 0.313 | |||
| 0 | 11 (9.1%) | 4 (11.4%) | 7 (8.1%) | |
| I | 31 (25.6%) | 10 (28.6%) | 21 (24.4%) | |
| II | 38 (31.4%) | 11 (31.4%) | 27 (31.4%) | |
| III | 40 (33.1%) | 10 (28.6%) | 30 (34.9%) | |
| IV | 1 (0.8%) | 0 (0.0%) | 1 (1.2%) | |
| Former Surgeries | ||||
| Cardiac surgery | 8 (6.6.%) | 4 (11.4%) | 4 (4.7%) | 0.227 |
| Aortic surgery | 5 (4.1%) | 1 (2.9%) | 4 (4.7%) | 1.000 |
| Scores | ||||
| Euroscore II | 3.00 ± 1.57 | 2.69 ± 1.64 | 3.13 ± 1.53 | 0.040 |
| Surgical Procedure | Patients n = 121 |
|---|---|
| Supracoronary replacement of AA | 35 (28.9%) |
| Wheat | 40 (33.1%) |
| Bentall | 38 (31.4%) |
| David | 8 (6.6%) |
| Aortic Valve Prosthesis | |
| biological | 65/78 (83.3%) |
| mechanical | 13/78 (16.7%) |
| Total (n = 121) | Group A (n = 35) | Group B (n = 86) | p-Value | |
|---|---|---|---|---|
| Postoperative Complication | ||||
| Stroke | 3 (2.5%) | 0 (0.0%) | 3 (3.5%) | 0.556 |
| Delirium | 13 (10.7%) | 4 (11.4%) | 9 (10.5%) | 1.000 |
| Pericardial effusion | 9 (7.4%) | 0 (0.0%) | 9 (10.5%) | 0.058 |
| Re-thoracotomy due to bleeding | 19 (15.7%) | 0 (0.0%) | 19 (22.1%) | 0.002 |
| Myocardial infarction | 1 (0.8%) | 0 (0.0%) | 1 (1.2%) | 1.000 |
| Sepsis | 3 (2.5%) | 1 (2.9%) | 2 (2.3%) | 1.000 |
| Pneumonia | 7 (5.8%) | 2 (5.7%) | 5 (5.8%) | 1.000 |
| Respiratory failure | 16 (13.2%) | 2 (5.7%) | 14 (16.3%) | 0.148 |
| Wound infection | 6 (5.0%) | 0 (0.0%) | 6 (7.0%) | 0.180 |
| 30-day mortality | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | - |
| In hospital stay | 14.57 ± 6.78 | 12.43 ± 3.38 | 15.44 ± 7.60 | 0.124 |
| ICU stay | 3.22 ± 4.63 | 2.14 ± 1.63 | 3.66 ± 5.34 | 0.125 |
| Discharge | 0.421 | |||
| home | 113 (93.4%) | 34 (97.1%) | 79 (91.9%) | |
| rehabiltation | 4 (3.3%) | 0 (0.0%) | 4 (4.7%) | |
| Other acute care hospital | 4 (3.3%) | 1 (2.9%) | 3 (3.5%) | |
| Follow-up | ||||
| death | 9 (7.4%) | 5 (14.3%) | 4 (4.7%) | 0.119 |
| re-operation during follow-up | 2 (1.6%) | 0 (0.0%) | 2 (1.2%) | 1.000 |
| Employment status | 71 (58.7%) | 13 (37.1%) | 58 (67.4%) | 0.667 |
| retired | 14 (19.7%) | 2 (15.4%) | 12 (20.7%) | |
| returned to work | 57 (80.3%) | 11 (84.6%) | 46 (79.3%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamiko, M.; Jahnel, K.; Rogaczewski, J.; Schafigh, M.; Silaschi, M.; Spaeth, A.; Velten, M.; Roell, W.; Ahmad, A.E.-S.; Bakhtiary, F. The Long-Term Outcome and Quality of Life after Replacement of the Ascending Aorta. J. Clin. Med. 2023, 12, 4498. https://doi.org/10.3390/jcm12134498
Hamiko M, Jahnel K, Rogaczewski J, Schafigh M, Silaschi M, Spaeth A, Velten M, Roell W, Ahmad AE-S, Bakhtiary F. The Long-Term Outcome and Quality of Life after Replacement of the Ascending Aorta. Journal of Clinical Medicine. 2023; 12(13):4498. https://doi.org/10.3390/jcm12134498
Chicago/Turabian StyleHamiko, Marwan, Katja Jahnel, Julia Rogaczewski, Myriam Schafigh, Miriam Silaschi, Andre Spaeth, Markus Velten, Wilhelm Roell, Ali El-Sayed Ahmad, and Farhad Bakhtiary. 2023. "The Long-Term Outcome and Quality of Life after Replacement of the Ascending Aorta" Journal of Clinical Medicine 12, no. 13: 4498. https://doi.org/10.3390/jcm12134498