
Prognostic Role of Metabolic Exercise Testing in Heart Failure

Abstract
:1. Overview of Heart Failure
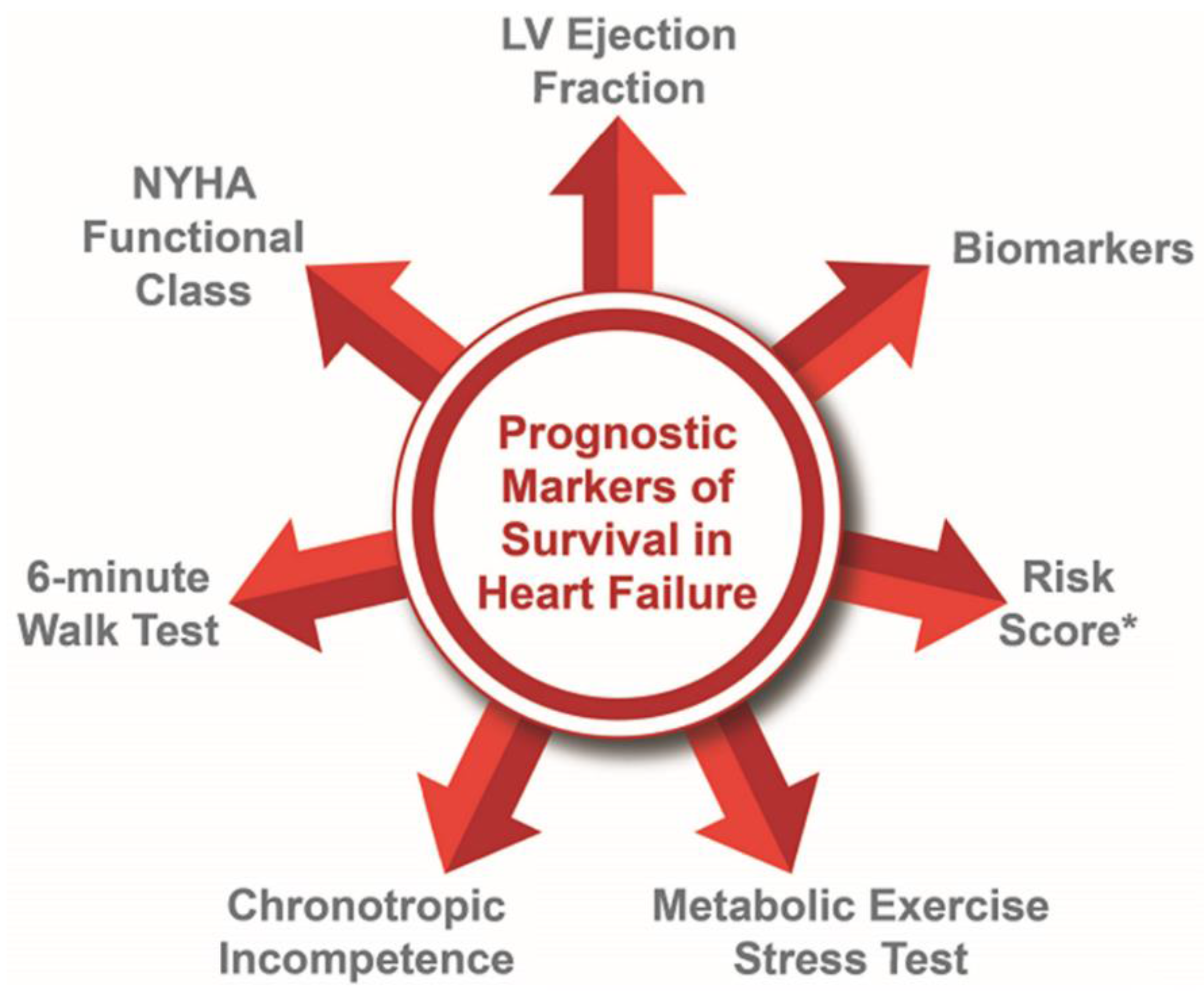
2. Risk Prediction in Heart Failure
2.1. Left Ventricular Ejection Fraction
2.2. New York Heart Association Functional Class
2.3. Six-Minute Walk Test
2.4. Chronotropic Incompetence
2.5. Risk Score Models
2.6. Cardiac Biomarkers
3. Overview of Metabolic Exercise Test
3.1. Performing the Metabolic Exercise Test
3.2. Variables Obtained in Metabolic Exercise Test
4. Metabolic Exercise Test in Patients with Heart Failure
4.1. VO2
4.2. VE/VCO2 Slope
4.3. Exercise Oscillatory Ventilation
4.4. Circulatory Power
4.5. VO2/WR Slope and VO2/HR
4.6. Ventilatory Power
4.7. Hemodynamic Gain Index
4.8. Metabolic Exercise Test in Patients with Mechanical Circulatory Support and Cardiac Transplantation
4.8.1. Orthotopic Heart Transplantation
4.8.2. Durable Mechanical Circulatory Support
4.8.3. Invasive Metabolic Exercise Test
4.8.4. Metabolic Exercise Test as Clinical Endpoints
5. Conclusions
Funding
Data Availability Statement
Conflicts of Interest
References
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Anderson, C.A.M.; Arora, P.; Avery, C.L.; Baker-Smith, C.M.; Beaton, A.Z.; Boehme, A.K.; Buxton, A.E.; et al. Heart Disease and Stroke Statistics-2023 Update: A Report from the American Heart Association. Circulation 2023, 147, e93–e621. [Google Scholar] [PubMed]
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Albert, N.M.; Allen, L.A.; Bluemke, D.A.; Butler, J.; Fonarow, G.C.; Ikonomidis, J.S.; Khavjou, O.; Konstam, M.A.; Maddox, T.M.; et al. Forecasting the impact of heart failure in the United States: A policy statement from the American Heart Association. Circ. Heart Fail. 2013, 6, 606–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2021 Update: A Report From the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [PubMed]
- Bozkurt, B.; Coats, A.J.; Tsutsui, H.; Abdelhamid, M.; Adamopoulos, S.; Albert, N.; Anker, S.D.; Atherton, J.; Bohm, M.; Butler, J.; et al. Universal Definition and Classification of Heart Failure: A Report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure. J. Card. Fail. 2021, 27, 387–413. [Google Scholar]
- Lewis, G.D.; Zlotoff, D.A. Cardiopulmonary Exercise Testing-Based Risk Stratification in the Modern Era of Advanced Heart Failure Management. JACC Heart Fail. 2021, 9, 237–240. [Google Scholar] [CrossRef]
- Yap, J.; Lim, F.Y.; Gao, F.; Teo, L.L.; Lam, C.S.; Yeo, K.K. Correlation of the New York Heart Association Classification and the 6-Minute Walk Distance: A Systematic Review. Clin. Cardiol. 2015, 38, 621–628. [Google Scholar] [CrossRef] [Green Version]
- Ambrosio, G.; Carluccio, E. Prognostic role of left ventricular ejection fraction in heart failure: Back to the future? Int. J. Cardiol. 2018, 273, 189–190. [Google Scholar] [CrossRef]
- Calkins, D.R.; Rubenstein, L.V.; Cleary, P.D.; Davies, A.R.; Jette, A.M.; Fink, A.; Kosecoff, J.; Young, R.T.; Brook, R.H.; Delbanco, T.L. Failure of physicians to recognize functional disability in ambulatory patients. Ann. Intern. Med. 1991, 114, 451–454. [Google Scholar] [CrossRef]
- Fonarow, G.C.; Adams, K.F., Jr.; Abraham, W.T.; Yancy, C.W.; Boscardin, W.J.; Adhere Scientific Advisory Committee, Study Group. Risk stratification for in-hospital mortality in acutely decompensated heart failure: Classification and regression tree analysis. JAMA 2005, 293, 572–580. [Google Scholar] [CrossRef] [Green Version]
- Peterson, P.N.; Rumsfeld, J.S.; Liang, L.; Albert, N.M.; Hernandez, A.F.; Peterson, E.D.; Fonarow, G.C.; Masoudi, F.A. A validated risk score for in-hospital mortality in patients with heart failure from the American Heart Association get with the guidelines program. Circ. Cardiovasc. Qual. Outcomes 2010, 3, 25–32. [Google Scholar] [CrossRef] [Green Version]
- Pocock, S.J.; Wang, D.; Pfeffer, M.A.; Yusuf, S.; McMurray, J.J.; Swedberg, K.B.; Ostergren, J.; Michelson, E.L.; Pieper, K.S.; Granger, C.B. Predictors of mortality and morbidity in patients with chronic heart failure. Eur. Heart J. 2006, 27, 65–75. [Google Scholar] [CrossRef] [Green Version]
- Wedel, H.; McMurray, J.J.; Lindberg, M.; Wikstrand, J.; Cleland, J.G.; Cornel, J.H.; Dunselman, P.; Hjalmarson, A.; Kjekshus, J.; Komajda, M.; et al. Predictors of fatal and non-fatal outcomes in the Controlled Rosuvastatin Multinational Trial in Heart Failure (CORONA): Incremental value of apolipoprotein A-1, high-sensitivity C-reactive peptide and N-terminal pro B-type natriuretic peptide. Eur. J. Heart Fail. 2009, 11, 281–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, D.S.; Austin, P.C.; Rouleau, J.L.; Liu, P.P.; Naimark, D.; Tu, J.V. Predicting mortality among patients hospitalized for heart failure: Derivation and validation of a clinical model. JAMA 2003, 290, 2581–2587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connor, C.M.; Hasselblad, V.; Mehta, R.H.; Tasissa, G.; Califf, R.M.; Fiuzat, M.; Rogers, J.G.; Leier, C.V.; Stevenson, L.W. Triage after hospitalization with advanced heart failure: The ESCAPE (Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization Effectiveness) risk model and discharge score. J. Am. Coll. Cardiol. 2010, 55, 872–878. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, C.; Fiuzat, M.; Mulder, H.; Coles, A.; Ahmad, T.; Ezekowitz, J.A.; Adams, K.F.; Pina, I.L.; Anstrom, K.J.; Cooper, L.S.; et al. Clinical factors related to morbidity and mortality in high-risk heart failure patients: The GUIDE-IT predictive model and risk score. Eur. J. Heart Fail. 2019, 21, 770–778. [Google Scholar] [CrossRef] [PubMed]
- Aaronson, K.D.; Schwartz, J.S.; Chen, T.M.; Wong, K.L.; Goin, J.E.; Mancini, D.M. Development and prospective validation of a clinical index to predict survival in ambulatory patients referred for cardiac transplant evaluation. Circulation 1997, 95, 2660–2667. [Google Scholar] [CrossRef]
- O’Connor, C.M.; Whellan, D.J.; Wojdyla, D.; Leifer, E.; Clare, R.M.; Ellis, S.J.; Fine, L.J.; Fleg, J.L.; Zannad, F.; Keteyian, S.J.; et al. Factors related to morbidity and mortality in patients with chronic heart failure with systolic dysfunction: The HF-ACTION predictive risk score model. Circ. Heart Fail. 2012, 5, 63–71. [Google Scholar] [CrossRef] [Green Version]
- Pocock, S.J.; Ariti, C.A.; McMurray, J.J.; Maggioni, A.; Kober, L.; Squire, I.B.; Swedberg, K.; Dobson, J.; Poppe, K.K.; Whalley, G.A.; et al. Predicting survival in heart failure: A risk score based on 39 372 patients from 30 studies. Eur. Heart J. 2013, 34, 1404–1413. [Google Scholar] [CrossRef]
- Komajda, M.; Carson, P.E.; Hetzel, S.; McKelvie, R.; McMurray, J.; Ptaszynska, A.; Zile, M.R.; Demets, D.; Massie, B.M. Factors associated with outcome in heart failure with preserved ejection fraction: Findings from the Irbesartan in Heart Failure with Preserved Ejection Fraction Study (I-PRESERVE). Circ. Heart Fail. 2011, 4, 27–35. [Google Scholar] [CrossRef] [Green Version]
- Simpson, J.; Jhund, P.S.; Lund, L.H.; Padmanabhan, S.; Claggett, B.L.; Shen, L.; Petrie, M.C.; Abraham, W.T.; Desai, A.S.; Dickstein, K.; et al. Prognostic Models Derived in PARADIGM-HF and Validated in ATMOSPHERE and the Swedish Heart Failure Registry to Predict Mortality and Morbidity in Chronic Heart Failure. JAMA Cardiol. 2020, 5, 432–441. [Google Scholar] [CrossRef] [PubMed]
- Levy, W.C.; Mozaffarian, D.; Linker, D.T.; Sutradhar, S.C.; Anker, S.D.; Cropp, A.B.; Anand, I.; Maggioni, A.; Burton, P.; Sullivan, M.D.; et al. The Seattle Heart Failure Model: Prediction of survival in heart failure. Circulation 2006, 113, 1424–1433. [Google Scholar] [CrossRef] [PubMed]
- Angraal, S.; Mortazavi, B.J.; Gupta, A.; Khera, R.; Ahmad, T.; Desai, N.R.; Jacoby, D.L.; Masoudi, F.A.; Spertus, J.A.; Krumholz, H.M. Machine Learning Prediction of Mortality and Hospitalization in Heart Failure with Preserved Ejection Fraction. JACC Heart Fail. 2020, 8, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Nedeljkovic, I.; Banovic, M.; Stepanovic, J.; Giga, V.; Djordjevic-Dikic, A.; Trifunovic, D.; Nedeljkovic, M.; Petrovic, M.; Dobric, M.; Dikic, N.; et al. The combined exercise stress echocardiography and cardiopulmonary exercise test for identification of masked heart failure with preserved ejection fraction in patients with hypertension. Eur. J. Prev. Cardiol. 2016, 23, 71–77. [Google Scholar] [CrossRef]
- Weber, K.T.; Janicki, J.S. Cardiopulmonary exercise testing for evaluation of chronic cardiac failure. Am. J. Cardiol. 1985, 55, 22A–31A. [Google Scholar] [CrossRef]
- Lucas, C.; Stevenson, L.W.; Johnson, W.; Hartley, H.; Hamilton, M.A.; Walden, J.; Lem, V.; Eagen-Bengsten, E. The 6-min walk and peak oxygen consumption in advanced heart failure: Aerobic capacity and survival. Am. Heart J. 1999, 138 Pt 1, 618–624. [Google Scholar] [CrossRef]
- Smart, N.; Haluska, B.; Leano, R.; Case, C.; Mottram, P.M.; Marwick, T.H. Determinants of functional capacity in patients with chronic heart failure: Role of filling pressure and systolic and diastolic function. Am. Heart J. 2005, 149, 152–158. [Google Scholar] [CrossRef]
- Savarese, G.; Stolfo, D.; Sinagra, G.; Lund, L.H. Heart failure with mid-range or mildly reduced ejection fraction. Nat. Rev. Cardiol. 2022, 19, 100–116. [Google Scholar] [CrossRef]
- Lam, C.S.P.; Yancy, C. Universal Definition and Classification of Heart Failure: Is It universal? Does It Define Heart Failure? J. Card. Fail. 2021, 27, 509–511. [Google Scholar]
- Wehner, G.J.; Jing, L.; Haggerty, C.M.; Suever, J.D.; Leader, J.B.; Hartzel, D.N.; Kirchner, H.L.; Manus, J.N.A.; James, N.; Ayar, Z.; et al. Routinely reported ejection fraction and mortality in clinical practice: Where does the nadir of risk lie? Eur. Heart J. 2020, 41, 1249–1257. [Google Scholar] [CrossRef] [Green Version]
- Solomon, S.D.; Anavekar, N.; Skali, H.; McMurray, J.J.; Swedberg, K.; Yusuf, S.; Granger, C.B.; Michelson, E.L.; Wang, D.; Pocock, S.; et al. Influence of ejection fraction on cardiovascular outcomes in a broad spectrum of heart failure patients. Circulation 2005, 112, 3738–3744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curtis, J.P.; Sokol, S.I.; Wang, Y.; Rathore, S.S.; Ko, D.T.; Jadbabaie, F.; Portnay, E.L.; Marshalko, S.J.; Radford, M.J.; Krumholz, H.M. The association of left ventricular ejection fraction, mortality, and cause of death in stable outpatients with heart failure. J. Am. Coll. Cardiol. 2003, 42, 736–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, T.; Pencina, M.J.; Schulte, P.J.; O’Brien, E.; Whellan, D.J.; Pina, I.L.; Kitzman, D.W.; Lee, K.L.; O’Connor, C.M.; Felker, G.M. Clinical implications of chronic heart failure phenotypes defined by cluster analysis. J. Am. Coll. Cardiol. 2014, 64, 1765–1774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancini, D.M.; Eisen, H.; Kussmaul, W.; Mull, R.; Edmunds, L.H., Jr.; Wilson, J.R. Value of peak exercise oxygen consumption for optimal timing of cardiac transplantation in ambulatory patients with heart failure. Circulation 1991, 83, 778–786. [Google Scholar] [CrossRef] [Green Version]
- Chomsky, D.B.; Lang, C.C.; Rayos, G.H.; Shyr, Y.; Yeoh, T.K.; Pierson, R.N., 3rd; Davis, S.F.; Wilson, J.R. Hemodynamic exercise testing. A valuable tool in the selection of cardiac transplantation candidates. Circulation 1996, 94, 3176–3183. [Google Scholar] [CrossRef]
- McGowan, J.H.; Cleland, J.G. Reliability of reporting left ventricular systolic function by echocardiography: A systematic review of 3 methods. Am. Heart J. 2003, 146, 388–397. [Google Scholar] [CrossRef]
- Konstam, M.A.; Abboud, F.M. Ejection Fraction: Misunderstood and Overrated (Changing the Paradigm in Categorizing Heart Failure). Circulation 2017, 135, 717–719. [Google Scholar] [CrossRef] [Green Version]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation 2017, 136, e137–e161. [Google Scholar]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar]
- Dunselman, P.H.; Kuntze, C.E.; van Bruggen, A.; Beekhuis, H.; Piers, B.; Scaf, A.H.; Wesseling, H.; Lie, K.I. Value of New York Heart Association classification, radionuclide ventriculography, and cardiopulmonary exercise tests for selection of patients for congestive heart failure studies. Am. Heart J. 1988, 116 Pt 1, 1475–1482. [Google Scholar] [CrossRef]
- Nadruz, W., Jr.; West, E.; Sengelov, M.; Santos, M.; Groarke, J.D.; Forman, D.E.; Claggett, B.; Skali, H.; Shah, A.M. Prognostic Value of Cardiopulmonary Exercise Testing in Heart Failure with Reduced, Midrange, and Preserved Ejection Fraction. J. Am. Heart Assoc. 2017, 6, e006000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guazzi, M. Cardiopulmonary exercise testing in heart failure preserved ejection fraction: Time to expand the paradigm in the prognostic algorithm. Am. Heart J. 2016, 174, 164–166. [Google Scholar] [CrossRef] [PubMed]
- Raphael, C.; Briscoe, C.; Davies, J.; Ian Whinnett, Z.; Manisty, C.; Sutton, R.; Mayet, J.; Francis, D.P. Limitations of the New York Heart Association functional classification system and self-reported walking distances in chronic heart failure. Heart 2007, 93, 476–482. [Google Scholar] [CrossRef] [Green Version]
- Severo, M.; Gaio, R.; Lourenco, P.; Alvelos, M.; Bettencourt, P.; Azevedo, A. Indirect calibration between clinical observers-application to the New York Heart Association functional classification system. BMC Res. Notes 2011, 4, 276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goode, K.M.; Nabb, S.; Cleland, J.G.; Clark, A.L. A comparison of patient and physician-rated New York Heart Association class in a community-based heart failure clinic. J. Card. Fail. 2008, 14, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Castel, M.A.; Magnani, S.; Mont, L.; Roig, E.; Tamborero, D.; Mendez-Zurita, F.; Femenia, J.F.; Tolosana, J.M.; Perez-Villa, F.; Brugada, J. Survival in New York Heart Association class IV heart failure patients treated with cardiac resynchronization therapy compared with patients on optimal pharmacological treatment. Europace 2010, 12, 1136–1140. [Google Scholar] [CrossRef]
- Muntwyler, J.; Abetel, G.; Gruner, C.; Follath, F. One-year mortality among unselected outpatients with heart failure. Eur. Heart J. 2002, 23, 1861–1866. [Google Scholar] [CrossRef] [Green Version]
- Glikson, M.; Nielsen, J.C.; Kronborg, M.B.; Michowitz, Y.; Auricchio, A.; Barbash, I.M.; Barrabes, J.A.; Boriani, G.; Braunschweig, F.; Brignole, M.; et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur. Heart J. 2021, 42, 3427–3520. [Google Scholar] [CrossRef]
- Zou, H.; Zhu, X.; Zhang, J.; Wang, Y.; Wu, X.; Liu, F.; Xie, X.; Chen, X. Reference equations for the six-minute walk distance in the healthy Chinese population aged 18-59 years. PLoS ONE 2017, 12, e0184669. [Google Scholar] [CrossRef] [Green Version]
- Uszko-Lencer, N.; Mesquita, R.; Janssen, E.; Werter, C.; Brunner-La Rocca, H.P.; Pitta, F.; Wouters, E.F.M.; Spruit, M.A. Reliability, construct validity and determinants of 6-minute walk test performance in patients with chronic heart failure. Int. J. Cardiol. 2017, 240, 285–290. [Google Scholar] [CrossRef] [Green Version]
- Harris, K.M.; Anderson, D.R.; Landers, J.D.; Emery, C.F. Utility of Walk Tests in Evaluating Functional Status Among Participants in an Outpatient Cardiac Rehabilitation Program. J. Cardiopulm. Rehabil. Prev. 2017, 37, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Sullivan, M.J.; Thompson, P.J.; Fallen, E.L.; Pugsley, S.O.; Taylor, D.W.; Berman, L.B. The 6-minute walk: A new measure of exercise capacity in patients with chronic heart failure. Can. Med. Assoc. J. 1985, 132, 919–923. [Google Scholar] [PubMed]
- Lee, R.; Chan, Y.H.; Wong, J.; Lau, D.; Ng, K. The 6-minute walk test predicts clinical outcome in Asian patients with chronic congestive heart failure on contemporary medical therapy: A study of the multiracial population in Singapore. Int. J. Cardiol. 2007, 119, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Rostagno, C.; Olivo, G.; Comeglio, M.; Boddi, V.; Banchelli, M.; Galanti, G.; Gensini, G.F. Prognostic value of 6-minute walk corridor test in patients with mild to moderate heart failure: Comparison with other methods of functional evaluation. Eur. J. Heart Fail. 2003, 5, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Wilkoff, B.L.; Corey, J.; Blackburn, G. A Mathematical Model of the Cardiac Chronotropic Response to Exercise. J. Electrophysiol. 1989, 3, 176–180. [Google Scholar] [CrossRef]
- Witte, K.K.; Cleland, J.G.; Clark, A.L. Chronic heart failure, chronotropic incompetence, and the effects of beta blockade. Heart 2006, 92, 481–486. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.N.; Pothier, C.E.; Lauer, M.S. Chronotropic incompetence as a predictor of death among patients with normal electrograms taking beta blockers (metoprolol or atenolol). Am. J. Cardiol. 2005, 96, 1328–1333. [Google Scholar] [CrossRef]
- Brubaker, P.H.; Kitzman, D.W. Chronotropic incompetence: Causes, consequences, and management. Circulation 2011, 123, 1010–1020. [Google Scholar] [CrossRef] [Green Version]
- Zweerink, A.; van der Lingen, A.C.J.; Handoko, M.L.; van Rossum, A.C.; Allaart, C.P. Chronotropic Incompetence in Chronic Heart Failure. Circ. Heart Fail. 2018, 11, e004969. [Google Scholar] [CrossRef]
- Benes, J.; Kotrc, M.; Borlaug, B.A.; Lefflerova, K.; Jarolim, P.; Bendlova, B.; Jabor, A.; Kautzner, J.; Melenovsky, V. Resting heart rate and heart rate reserve in advanced heart failure have distinct pathophysiologic correlates and prognostic impact: A prospective pilot study. JACC Heart Fail. 2013, 1, 259–266. [Google Scholar] [CrossRef]
- Dobre, D.; Zannad, F.; Keteyian, S.J.; Stevens, S.R.; Rossignol, P.; Kitzman, D.W.; Landzberg, J.; Howlett, J.; Kraus, W.E.; Ellis, S.J. Association between resting heart rate, chronotropic index, and long-term outcomes in patients with heart failure receiving beta-blocker therapy: Data from the HF-ACTION trial. Eur. Heart J. 2013, 34, 2271–2280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agostoni, P.; Paolillo, S.; Mapelli, M.; Gentile, P.; Salvioni, E.; Veglia, F.; Bonomi, A.; Corra, U.; Lagioia, R.; Limongelli, G.; et al. Multiparametric prognostic scores in chronic heart failure with reduced ejection fraction: A long-term comparison. Eur. J. Heart Fail. 2018, 20, 700–710. [Google Scholar] [CrossRef] [PubMed]
- Levy, W.C.; Dardas, T.F. Comparison of cardiopulmonary-based risk models with a clinical heart failure risk model. Eur. J. Heart Fail. 2018, 20, 711–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nutter, A.L.; Tanawuttiwat, T.; Silver, M.A. Evaluation of 6 prognostic models used to calculate mortality rates in elderly heart failure patients with a fatal heart failure admission. Congest. Heart Fail. 2010, 16, 196–201. [Google Scholar] [CrossRef]
- Baughman, K.L. B-type natriuretic peptide -- a window to the heart. N. Engl. J. Med. 2002, 347, 158–159. [Google Scholar] [CrossRef]
- Hartmann, F.; Packer, M.; Coats, A.J.; Fowler, M.B.; Krum, H.; Mohacsi, P.; Rouleau, J.L.; Tendera, M.; Castaigne, A.; Anker, S.D.; et al. Prognostic impact of plasma N-terminal pro-brain natriuretic peptide in severe chronic congestive heart failure: A substudy of the Carvedilol Prospective Randomized Cumulative Survival (COPERNICUS) trial. Circulation 2004, 110, 1780–1786. [Google Scholar] [CrossRef] [Green Version]
- Berezin, A.E. Prognostication in Different Heart Failure Phenotypes: The Role of Circulating Biomarkers. J. Circ. Biomark. 2016, 5, 6. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Li, Z.; Chen, J.; Zhao, H.; Luo, L.; Chen, C.; Xu, X.; Zhang, W.; Gao, K.; Li, B.; et al. Metabolomic identification of diagnostic plasma biomarkers in humans with chronic heart failure. Mol. Biosyst. 2013, 9, 2618–2626. [Google Scholar] [CrossRef] [PubMed]
- Lekavich, C.L.; Barksdale, D.J.; Neelon, V.; Wu, J.R. Heart failure preserved ejection fraction (HFpEF): An integrated and strategic review. Heart Fail. Rev. 2015, 20, 643–653. [Google Scholar] [CrossRef]
- Zile, M.R.; Baicu, C.F. Biomarkers of diastolic dysfunction and myocardial fibrosis: Application to heart failure with a preserved ejection fraction. J. Cardiovasc. Transl. Res. 2013, 6, 501–515. [Google Scholar] [CrossRef]
- D’Elia, E.; Vaduganathan, M.; Gori, M.; Gavazzi, A.; Butler, J.; Senni, M. Role of biomarkers in cardiac structure phenotyping in heart failure with preserved ejection fraction: Critical appraisal and practical use. Eur. J. Heart Fail. 2015, 17, 1231–1239. [Google Scholar] [CrossRef]
- Wilcox, J.E.; Fonarow, G.C.; Ardehali, H.; Bonow, R.O.; Butler, J.; Sauer, A.J.; Epstein, S.E.; Khan, S.S.; Kim, R.J.; Sabbah, H.N.; et al. “Targeting the Heart” in Heart Failure: Myocardial Recovery in Heart Failure with Reduced Ejection Fraction. JACC Heart Fail. 2015, 3, 661–669. [Google Scholar] [CrossRef]
- Hillege, H.L.; Nitsch, D.; Pfeffer, M.A.; Swedberg, K.; McMurray, J.J.; Yusuf, S.; Granger, C.B.; Michelson, E.L.; Ostergren, J.; Cornel, J.H.; et al. Renal function as a predictor of outcome in a broad spectrum of patients with heart failure. Circulation 2006, 113, 671–678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guazzi, M.; Wilhelm, M.; Halle, M.; Van Craenenbroeck, E.; Kemps, H.; de Boer, R.A.; Coats, A.J.S.; Lund, L.; Mancini, D.; Borlaug, B.; et al. Exercise testing in heart failure with preserved ejection fraction: An appraisal through diagnosis, pathophysiology and therapy—A clinical consensus statement of the Heart Failure Association and European Association of Preventive Cardiology of the European Society of Cardiology. Eur. J. Heart Fail. 2022, 24, 1327–1345. [Google Scholar] [PubMed]
- Guazzi, M.; Bandera, F.; Ozemek, C.; Systrom, D.; Arena, R. Cardiopulmonary Exercise Testing: What Is its Value? J. Am. Coll. Cardiol. 2017, 70, 1618–1636. [Google Scholar] [CrossRef]
- Guazzi, M.; Arena, R.; Halle, M.; Piepoli, M.F.; Myers, J.; Lavie, C.J. 2016 focused update: Clinical recommendations for cardiopulmonary exercise testing data assessment in specific patient populations. Eur. Heart J. 2018, 39, 1144–1161. [Google Scholar] [CrossRef] [PubMed]
- Piepoli, M.F.; Corra, U.; Agostoni, P. Cardiopulmonary Exercise Testing in Patients with Heart Failure with Specific Comorbidities. Ann. Am. Thorac. Soc. 2017, 14 (Suppl. S1), S110–S115. [Google Scholar] [CrossRef]
- Skalski, J.; Allison, T.G.; Miller, T.D. The safety of cardiopulmonary exercise testing in a population with high-risk cardiovascular diseases. Circulation 2012, 126, 2465–2472. [Google Scholar] [CrossRef] [Green Version]
- Ross, R.; Blair, S.N.; Arena, R.; Church, T.S.; Despres, J.P.; Franklin, B.A.; Haskell, W.L.; Kaminsky, L.A.; Levine, B.D.; Lavie, C.J.; et al. Importance of Assessing Cardiorespiratory Fitness in Clinical Practice: A Case for Fitness as a Clinical Vital Sign: A Scientific Statement from the American Heart Association. Circulation 2016, 134, e653–e99. [Google Scholar] [CrossRef]
- Gibbons, R.J.; Balady, G.J.; Beasley, J.W.; Bricker, J.T.; Duvernoy, W.F.; Froelicher, V.F.; Mark, D.B.; Marwick, T.H.; McCallister, B.D.; Thompson, P.D.; et al. ACC/AHA guidelines for exercise testing: Executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Exercise Testing). Circulation 1997, 96, 345–354. [Google Scholar] [CrossRef]
- Fletcher, G.F.; Ades, P.A.; Kligfield, P.; Arena, R.; Balady, G.J.; Bittner, V.A.; Coke, L.A.; Fleg, J.L.; Forman, D.E.; Gerber, T.C.; et al. Exercise standards for testing and training: A scientific statement from the American Heart Association. Circulation 2013, 128, 873–934. [Google Scholar] [CrossRef]
- Roger, V.L.; Jacobsen, S.J.; Pellikka, P.A.; Miller, T.D.; Bailey, K.R.; Gersh, B.J. Prognostic value of treadmill exercise testing: A population-based study in Olmsted County, Minnesota. Circulation 1998, 98, 2836–2841. [Google Scholar] [CrossRef] [Green Version]
- Balady, G.J.; Arena, R.; Sietsema, K.; Myers, J.; Coke, L.; Fletcher, G.F.; Forman, D.; Franklin, B.; Guazzi, M.; Gulati, M.; et al. Clinician’s Guide to cardiopulmonary exercise testing in adults: A scientific statement from the American Heart Association. Circulation 2010, 122, 191–225. [Google Scholar] [CrossRef] [Green Version]
- Corra, U.; Agostoni, P.G.; Anker, S.D.; Coats, A.J.S.; Crespo Leiro, M.G.; de Boer, R.A.; Harjola, V.P.; Hill, L.; Lainscak, M.; Lund, L.H.; et al. Role of cardiopulmonary exercise testing in clinical stratification in heart failure. A position paper from the Committee on Exercise Physiology and Training of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2018, 20, 3–15. [Google Scholar] [CrossRef]
- Leclerc, K. Cardiopulmonary exercise testing: A contemporary and versatile clinical tool. Cleve Clin. J. Med. 2017, 84, 161–168. [Google Scholar] [CrossRef] [PubMed]
- American Thoracic, S.; American College of Chest, P. ATS/ACCP Statement on cardiopulmonary exercise testing. Am. J. Respir. Crit. Care Med. 2003, 167, 211–277. [Google Scholar]
- Finet, J.E.; Van Iterson, E.H.; Wilson Tang, W.H. Invasive Hemodynamic and Metabolic Evaluation of HFpEF. Curr. Treat. Options Cardiovasc. Med. 2021, 23, 32. [Google Scholar] [CrossRef]
- Glaab, T.; Taube, C. Practical guide to cardiopulmonary exercise testing in adults. Respir. Res. 2022, 23, 9. [Google Scholar] [CrossRef]
- Triantafyllidi, H.; Birmpa, D.; Benas, D.; Trivilou, P.; Fambri, A.; Iliodromitis, E.K. Cardiopulmonary Exercise Testing: The ABC for the Clinical Cardiologist. Cardiology 2022, 147, 62–71. [Google Scholar] [CrossRef] [PubMed]
- Agostoni, P.; Dumitrescu, D. How to perform and report a cardiopulmonary exercise test in patients with chronic heart failure. Int. J. Cardiol. 2019, 288, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Dumitrescu, D.; Rosenkranz, S. Graphical Data Display for Clinical Cardiopulmonary Exercise Testing. Ann. Am. Thorac. Soc. 2017, 14 (Suppl. S1), S12–S21. [Google Scholar] [CrossRef]
- Aaronson, K.D.; Mancini, D.M. Is percentage of predicted maximal exercise oxygen consumption a better predictor of survival than peak exercise oxygen consumption for patients with severe heart failure? J. Heart Lung Transplant. 1995, 14, 981–989. [Google Scholar]
- Cohen-Solal, A.; Tabet, J.Y.; Logeart, D.; Bourgoin, P.; Tokmakova, M.; Dahan, M. A non-invasively determined surrogate of cardiac power (‘circulatory power’) at peak exercise is a powerful prognostic factor in chronic heart failure. Eur. Heart J. 2002, 23, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Agostoni, P.; Corra, U.; Cattadori, G.; Veglia, F.; Battaia, E.; La Gioia, R.; Scardovi, A.B.; Emdin, M.; Metra, M.; Sinagra, G.; et al. Prognostic value of indeterminable anaerobic threshold in heart failure. Circ. Heart Fail. 2013, 6, 977–987. [Google Scholar] [CrossRef] [Green Version]
- Chua, T.P.; Ponikowski, P.; Harrington, D.; Anker, S.D.; Webb-Peploe, K.; Clark, A.L.; Poole-Wilson, P.A.; Coats, A.J. Clinical correlates and prognostic significance of the ventilatory response to exercise in chronic heart failure. J. Am. Coll. Cardiol. 1997, 29, 1585–1590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleber, F.X.; Vietzke, G.; Wernecke, K.D.; Bauer, U.; Opitz, C.; Wensel, R.; Sperfeld, A.; Glaser, S. Impairment of ventilatory efficiency in heart failure: Prognostic impact. Circulation 2000, 101, 2803–2809. [Google Scholar] [CrossRef] [Green Version]
- Arena, R.; Myers, J.; Abella, J.; Peberdy, M.A.; Bensimhon, D.; Chase, P.; Guazzi, M. Development of a ventilatory classification system in patients with heart failure. Circulation 2007, 115, 2410–2417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arena, R.; Myers, J.; Aslam, S.S.; Varughese, E.B.; Peberdy, M.A. Peak VO2 and VE/VCO2 slope in patients with heart failure: A prognostic comparison. Am. Heart J. 2004, 147, 354–360. [Google Scholar] [CrossRef]
- Hollenberg, M.; Tager, I.B. Oxygen uptake efficiency slope: An index of exercise performance and cardiopulmonary reserve requiring only submaximal exercise. J. Am. Coll. Cardiol. 2000, 36, 194–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baba, R.; Nagashima, M.; Goto, M.; Nagano, Y.; Yokota, M.; Tauchi, N.; Nishibata, K. Oxygen uptake efficiency slope: A new index of cardiorespiratory functional reserve derived from the relation between oxygen uptake and minute ventilation during incremental exercise. J. Am. Coll. Cardiol. 1996, 28, 1567–1572. [Google Scholar] [CrossRef]
- Davies, L.C.; Wensel, R.; Georgiadou, P.; Cicoira, M.; Coats, A.J.; Piepoli, M.F.; Francis, D.P. Enhanced prognostic value from cardiopulmonary exercise testing in chronic heart failure by non-linear analysis: Oxygen uptake efficiency slope. Eur. Heart J. 2006, 27, 684–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsumoto, A.; Itoh, H.; Eto, Y.; Kobayashi, T.; Kato, M.; Omata, M.; Watanabe, H.; Kato, K.; Momomura, S. End-tidal CO2 pressure decreases during exercise in cardiac patients: Association with severity of heart failure and cardiac output reserve. J. Am. Coll. Cardiol. 2000, 36, 242–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olson, L.J.; Arruda-Olson, A.M.; Somers, V.K.; Scott, C.G.; Johnson, B.D. Exercise oscillatory ventilation: Instability of breathing control associated with advanced heart failure. Chest 2008, 133, 474–481. [Google Scholar] [CrossRef] [Green Version]
- Corra, U.; Pistono, M.; Mezzani, A.; Braghiroli, A.; Giordano, A.; Lanfranchi, P.; Bosimini, E.; Gnemmi, M.; Giannuzzi, P. Sleep and exertional periodic breathing in chronic heart failure: Prognostic importance and interdependence. Circulation 2006, 113, 44–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wasserman, K.; Hansen, J.E.; Sue, D.Y.; Whipp, B.J.; Froelicher, V.F. Principles of Exercise Testing and Interpretation. J. Cardiopulm. Rehabil. Prev. 1987, 7, 189. [Google Scholar] [CrossRef]
- Takken, T.; Mylius, C.F.; Paap, D.; Broeders, W.; Hulzebos, H.J.; Van Brussel, M.; Bongers, B.C. Reference values for cardiopulmonary exercise testing in healthy subjects—An updated systematic review. Expert Rev. Cardiovasc. Ther. 2019, 17, 413–426. [Google Scholar] [CrossRef] [Green Version]
- Myers, J.; Kaminsky, L.A.; Lima, R.; Christle, J.W.; Ashley, E.; Arena, R. A Reference Equation for Normal Standards for VO(2) Max: Analysis from the Fitness Registry and the Importance of Exercise National Database (FRIEND Registry). Prog. Cardiovasc. Dis. 2017, 60, 21–29. [Google Scholar] [CrossRef]
- Hansen, J.E.; Sue, D.Y.; Wasserman, K. Predicted values for clinical exercise testing. Am. Rev. Respir. Dis. 1984, 129 Pt 2, S49–S55. [Google Scholar] [CrossRef]
- Dorken Gallastegi, A.; Ergi, G.D.; Kahraman, U.; Yagmur, B.; Cinar, E.; Karapolat, H.; Nalbantgil, S.; Engin, C.; Yagdi, T.; Ozbaran, M. Prognostic Value of Cardiopulmonary Exercise Test Parameters in Ventricular Assist Device Therapy. ASAIO J. 2022, 68, 808–813. [Google Scholar] [CrossRef]
- Kaminsky, L.A.; Arena, R.; Myers, J.; Peterman, J.E.; Bonikowske, A.R.; Harber, M.P.; Medina Inojosa, J.R.; Lavie, C.J.; Squires, R.W. Updated Reference Standards for Cardiorespiratory Fitness Measured with Cardiopulmonary Exercise Testing: Data from the Fitness Registry and the Importance of Exercise National Database (FRIEND). Mayo Clin. Proc. 2022, 97, 285–293. [Google Scholar] [CrossRef]
- Weber, K.T.; Kinasewitz, G.T.; Janicki, J.S.; Fishman, A.P. Oxygen utilization and ventilation during exercise in patients with chronic cardiac failure. Circulation 1982, 65, 1213–1223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Neill, J.O.; Young, J.B.; Pothier, C.E.; Lauer, M.S. Peak oxygen consumption as a predictor of death in patients with heart failure receiving beta-blockers. Circulation 2005, 111, 2313–2318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, L.R.; Schechtman, K.B.; Ewald, G.A.; Geltman, E.M.; Meyer, T.; Krekeler, P.; Rogers, J.G. The effect of beta-adrenergic blockers on the prognostic value of peak exercise oxygen uptake in patients with heart failure. J. Heart Lung Transplant. 2003, 22, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Cohn, J.N.; Rector, T.S. Prognosis of congestive heart failure and predictors of mortality. Am. J. Cardiol. 1988, 62, 25A–30A. [Google Scholar] [CrossRef]
- Keteyian, S.J.; Patel, M.; Kraus, W.E.; Brawner, C.A.; McConnell, T.R.; Pina, I.L.; Leifer, E.S.; Fleg, J.L.; Blackburn, G.; Fonarow, G.C.; et al. Variables Measured During Cardiopulmonary Exercise Testing as Predictors of Mortality in Chronic Systolic Heart Failure. J. Am. Coll. Cardiol. 2016, 67, 780–789. [Google Scholar] [CrossRef]
- Dhakal, B.P.; Malhotra, R.; Murphy, R.M.; Pappagianopoulos, P.P.; Baggish, A.L.; Weiner, R.B.; Houstis, N.E.; Eisman, A.S.; Hough, S.S.; Lewis, G.D. Mechanisms of exercise intolerance in heart failure with preserved ejection fraction: The role of abnormal peripheral oxygen extraction. Circ. Heart Fail. 2015, 8, 286–294. [Google Scholar] [CrossRef] [Green Version]
- Haykowsky, M.J.; Brubaker, P.H.; John, J.M.; Stewart, K.P.; Morgan, T.M.; Kitzman, D.W. Determinants of exercise intolerance in elderly heart failure patients with preserved ejection fraction. J. Am. Coll. Cardiol. 2011, 58, 265–274. [Google Scholar] [CrossRef] [Green Version]
- Ciani, O.; Piepoli, M.; Smart, N.; Uddin, J.; Walker, S.; Warren, F.C.; Zwisler, A.D.; Davos, C.H.; Taylor, R.S. Validation of Exercise Capacity as a Surrogate Endpoint in Exercise-Based Rehabilitation for Heart Failure: A Meta-Analysis of Randomized Controlled Trials. JACC Heart Fail. 2018, 6, 596–604. [Google Scholar] [CrossRef]
- De Marco, T.; Wolfel, E.; Feldman, A.M.; Lowes, B.; Higginbotham, M.B.; Ghali, J.K.; Wagoner, L.; Kirlin, P.C.; Kennett, J.D.; Goel, S.; et al. Impact of cardiac resynchronization therapy on exercise performance, functional capacity, and quality of life in systolic heart failure with QRS prolongation: COMPANION trial sub-study. J. Card. Fail. 2008, 14, 9–18. [Google Scholar] [CrossRef]
- Gitt, A.K.; Wasserman, K.; Kilkowski, C.; Kleemann, T.; Kilkowski, A.; Bangert, M.; Schneider, S.; Schwarz, A.; Senges, J. Exercise anaerobic threshold and ventilatory efficiency identify heart failure patients for high risk of early death. Circulation 2002, 106, 3079–3084. [Google Scholar] [CrossRef] [Green Version]
- Chaudhry, S.; Arena, R.; Wasserman, K.; Hansen, J.E.; Lewis, G.D.; Myers, J.; Chronos, N.; Boden, W.E. Exercise-induced myocardial ischemia detected by cardiopulmonary exercise testing. Am. J. Cardiol. 2009, 103, 615–619. [Google Scholar] [CrossRef] [Green Version]
- Shafiq, A.; Brawner, C.A.; Aldred, H.A.; Lewis, B.; Williams, C.T.; Tita, C.; Schairer, J.R.; Ehrman, J.K.; Velez, M.; Selektor, Y.; et al. Prognostic value of cardiopulmonary exercise testing in heart failure with preserved ejection fraction. The Henry Ford HospITal CardioPulmonary EXercise Testing (FIT-CPX) project. Am. Heart J. 2016, 174, 167–172. [Google Scholar] [CrossRef] [Green Version]
- Franciosa, J.A.; Leddy, C.L.; Wilen, M.; Schwartz, D.E. Relation between hemodynamic and ventilatory responses in determining exercise capacity in severe congestive heart failure. Am. J. Cardiol. 1984, 53, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, R.; Bakken, K.; D’Elia, E.; Lewis, G.D. Cardiopulmonary Exercise Testing in Heart Failure. JACC Heart Fail. 2016, 4, 607–616. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.L., Jr. Gas exchange efficiency in congestive heart failure II. Circulation 2001, 103, 916–918. [Google Scholar] [CrossRef] [Green Version]
- Lewis, G.D.; Shah, R.V.; Pappagianopolas, P.P.; Systrom, D.M.; Semigran, M.J. Determinants of ventilatory efficiency in heart failure: The role of right ventricular performance and pulmonary vascular tone. Circ. Heart Fail. 2008, 1, 227–233. [Google Scholar] [CrossRef] [Green Version]
- Jaussaud, J.; Aimable, L.; Douard, H. The time for a new strong functional parameter in heart failure: The VE/VCO2 slope. Int. J. Cardiol. 2011, 147, 189–190. [Google Scholar] [CrossRef]
- Cornelis, J.; Taeymans, J.; Hens, W.; Beckers, P.; Vrints, C.; Vissers, D. Prognostic respiratory parameters in heart failure patients with and without exercise oscillatory ventilation—A systematic review and descriptive meta-analysis. Int. J. Cardiol. 2015, 182, 476–486. [Google Scholar] [CrossRef] [PubMed]
- Arena, R.; Guazzi, M.; Cahalin, L.P.; Myers, J. Revisiting cardiopulmonary exercise testing applications in heart failure: Aligning evidence with clinical practice. Exerc. Sport Sci. Rev. 2014, 42, 153–160. [Google Scholar] [CrossRef]
- Nayor, M.; Xanthakis, V.; Tanguay, M.; Blodgett, J.B.; Shah, R.V.; Schoenike, M.; Sbarbaro, J.; Farrell, R.; Malhotra, R.; Houstis, N.E.; et al. Clinical and Hemodynamic Associations and Prognostic Implications of Ventilatory Efficiency in Patients with Preserved Left Ventricular Systolic Function. Circ. Heart Fail. 2020, 13, e006729. [Google Scholar] [CrossRef]
- Forman, D.E.; Guazzi, M.; Myers, J.; Chase, P.; Bensimhon, D.; Cahalin, L.P.; Peberdy, M.A.; Ashley, E.; West, E.; Daniels, K.M.; et al. Ventilatory power: A novel index that enhances prognostic assessment of patients with heart failure. Circ. Heart Fail. 2012, 5, 621–626. [Google Scholar] [CrossRef] [Green Version]
- Arena, R.; Myers, J.; Aslam, S.S.; Varughese, E.B.; Peberdy, M.A. Influence of subject effort on the prognostic value of peak VO2 and the VE/VCO2 slope in patients with heart failure. J. Cardiopulm. Rehabil. 2004, 24, 317–320. [Google Scholar] [CrossRef]
- Lala, A.; Shah, K.B.; Lanfear, D.E.; Thibodeau, J.T.; Palardy, M.; Ambardekar, A.V.; McNamara, D.M.; Taddei-Peters, W.C.; Baldwin, J.T.; Jeffries, N.; et al. Predictive Value of Cardiopulmonary Exercise Testing Parameters in Ambulatory Advanced Heart Failure. JACC Heart Fail. 2021, 9, 226–236. [Google Scholar] [CrossRef]
- Dhakal, B.P.; Murphy, R.M.; Lewis, G.D. Exercise oscillatory ventilation in heart failure. Trends Cardiovasc. Med. 2012, 22, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.G.; Hansen, J.E.; Beshai, J.F.; Wasserman, K. Oscillatory breathing and exercise gas exchange abnormalities prognosticate early mortality and morbidity in heart failure. J. Am. Coll. Cardiol. 2010, 55, 1814–1823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, R.M.; Shah, R.V.; Malhotra, R.; Pappagianopoulos, P.P.; Hough, S.S.; Systrom, D.M.; Semigran, M.J.; Lewis, G.D. Exercise oscillatory ventilation in systolic heart failure: An indicator of impaired hemodynamic response to exercise. Circulation 2011, 124, 1442–1451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stringer, W.W.; Hansen, J.E.; Wasserman, K. Cardiac output estimated noninvasively from oxygen uptake during exercise. J. Appl. Physiol. (1985) 1997, 82, 908–912. [Google Scholar] [CrossRef]
- Hansen, J.E.; Sue, D.Y.; Oren, A.; Wasserman, K. Relation of oxygen uptake to work rate in normal men and men with circulatory disorders. Am. J. Cardiol. 1987, 59, 669–674. [Google Scholar] [CrossRef]
- Vainshelboim, B.; Kokkinos, P.; Myers, J. Prognostic Value and Clinical Usefulness of the Hemodynamic Gain Index in Men. Am. J. Cardiol. 2019, 124, 644–649. [Google Scholar] [CrossRef]
- Vainshelboim, B.; Kokkinos, P.; Myers, J. Hemodynamic gain index in women: A validation study. Int. J. Cardiol. 2020, 308, 15–19. [Google Scholar] [CrossRef]
- Chaikijurajai, T.; Wu, Y.; Grodin, J.L.; Harb, S.; Jaber, W.; Tang, W.H.W. Validation of prognostic value of the hemodynamic gain index in different groups of patients undergoing exercise stress testing. Am. Heart J. Plus. 2022, 18, 100174. [Google Scholar] [CrossRef] [PubMed]
- Gobel, F.L.; Norstrom, L.A.; Nelson, R.R.; Jorgensen, C.R.; Wang, Y. The rate-pressure product as an index of myocardial oxygen consumption during exercise in patients with angina pectoris. Circulation 1978, 57, 549–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehra, M.R.; Canter, C.E.; Hannan, M.M.; Semigran, M.J.; Uber, P.A.; Baran, D.A.; Danziger-Isakov, L.; Kirklin, J.K.; Kirk, R.; Kushwaha, S.S.; et al. The 2016 International Society for Heart Lung Transplantation listing criteria for heart transplantation: A 10-year update. J. Heart Lung Transplant. 2016, 35, 1–23. [Google Scholar] [CrossRef]
- Agostoni, P.; Corra, U.; Cattadori, G.; Veglia, F.; La Gioia, R.; Scardovi, A.B.; Emdin, M.; Metra, M.; Sinagra, G.; Limongelli, G.; et al. Metabolic exercise test data combined with cardiac and kidney indexes, the MECKI score: A multiparametric approach to heart failure prognosis. Int. J. Cardiol. 2013, 167, 2710–2718. [Google Scholar] [CrossRef] [PubMed]
- Guazzi, M.; Boracchi, P.; Arena, R.; Myers, J.; Vicenzi, M.; Peberdy, M.A.; Bensimhon, D.; Chase, P.; Reina, G. Development of a cardiopulmonary exercise prognostic score for optimizing risk stratification in heart failure: The (P)e(R)i(O)dic (B)reathing during (E)xercise (PROBE) study. J. Card. Fail. 2010, 16, 799–805. [Google Scholar] [CrossRef]
- Yardley, M.; Gullestad, L.; Bendz, B.; Bjorkelund, E.; Rolid, K.; Arora, S.; Nytroen, K. Long-term effects of high-intensity interval training in heart transplant recipients: A 5-year follow-up study of a randomized controlled trial. Clin. Transplant. 2017, 31, e12868. [Google Scholar] [CrossRef]
- Pelliccia, A.; Sharma, S.; Gati, S.; Back, M.; Borjesson, M.; Caselli, S.; Collet, J.P.; Corrado, D.; Drezner, J.A.; Halle, M.; et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur. Heart J. 2021, 42, 17–96. [Google Scholar] [CrossRef]
- Myers, J.; Geiran, O.; Simonsen, S.; Ghuyoumi, A.; Gullestad, L. Clinical and exercise test determinants of survival after cardiac transplantation. Chest 2003, 124, 2000–2005. [Google Scholar] [CrossRef]
- Yardley, M.; Havik, O.E.; Grov, I.; Relbo, A.; Gullestad, L.; Nytroen, K. Peak oxygen uptake and self-reported physical health are strong predictors of long-term survival after heart transplantation. Clin. Transplant. 2016, 30, 161–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, H.Y.; Tsai, W.J.; Kuo, L.Y.; Lin, Y.S.; Chen, B.Y.; Lin, W.H.; Shen, S.L.; Huang, H.Y. Oxygen Consumption at Anaerobic Threshold Predicts Cardiac Events After Heart Transplantation. Transplant. Proc. 2018, 50, 2742–2746. [Google Scholar] [CrossRef]
- Iglesias, D.; Masson, W.; Barbagelata, L.; Rossi, E.; Mora, M.; Cornejo, G.; Lagoria, J.; Belziti, C.; Vulcano, N.; Marenchino, R.; et al. Prognostic value of cardiopulmonary exercise test after heart transplantation. Clin. Transplant. 2021, 35, e14387. [Google Scholar] [CrossRef] [PubMed]
- Grinstein, J.; Sawalha, Y.; Medvedofsky, D.A.; Ahmad, S.; Hofmeyer, M.; Rodrigo, M.; Kadakkal, A.; Barnett, C.; Kalantari, S.; Talati, I.; et al. VE/VCO2 slope predicts RV dysfunction and mortality after left ventricular assist device: A fresh look at cardiopulmonary stress testing for prognostication. J. Artif. Organs 2021, 24, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Trombara, F.; Apostolo, A.; Vignati, C.; Naliato, M.; Ceriani, R.; Agostoni, P. Effects of left ventricular assist device on cardiopulmonary exercise performance. Eur. J. Heart Fail. 2020, 22, 381–382. [Google Scholar] [CrossRef]
- Mancini, D.; Goldsmith, R.; Levin, H.; Beniaminovitz, A.; Rose, E.; Catanese, K.; Flannery, M.; Oz, M. Comparison of exercise performance in patients with chronic severe heart failure versus left ventricular assist devices. Circulation 1998, 98, 1178–1183. [Google Scholar] [CrossRef] [PubMed]
- Leibner, E.S.; Cysyk, J.; Eleuteri, K.; El-Banayosy, A.; Boehmer, J.P.; Pae, W.E. Changes in the functional status measures of heart failure patients with mechanical assist devices. ASAIO J. 2013, 59, 117–122. [Google Scholar] [CrossRef]
- Mirza, K.K.; Szymanski, M.K.; Schmidt, T.; de Jonge, N.; Brahmbhatt, D.H.; Billia, F.; Hsu, S.; MacGowan, G.A.; Jakovljevic, D.G.; Agostoni, P.; et al. Prognostic Value of Peak Oxygen Uptake in Patients Supported with Left Ventricular Assist Devices (PRO-VAD). JACC Heart Fail. 2021, 9, 758–767. [Google Scholar] [CrossRef]
- Moss, N.; Rakita, V.; Lala, A.; Parikh, A.; Roldan, J.; Mitter, S.S.; Anyanwu, A.; Campoli, M.; Burkhoff, D.; Mancini, D.M. Hemodynamic Response to Exercise in Patients Supported by Continuous Flow Left Ventricular Assist Devices. JACC Heart Fail. 2020, 8, 291–301. [Google Scholar] [CrossRef]
- Dunlay, S.M.; Allison, T.G.; Pereira, N.L. Changes in cardiopulmonary exercise testing parameters following continuous flow left ventricular assist device implantation and heart transplantation. J. Card. Fail. 2014, 20, 548–554. [Google Scholar] [CrossRef] [Green Version]
- Dorken Gallastegi, A.; Ozturk, P.; Demir, E.; Engin, C.; Nalbantgil, S.; Yagdi, T.; Ozbaran, M. Prospective evaluation of ventricular assist device risk scores’ capacity to predict cardiopulmonary exercise parameters. Interact. Cardiovasc. Thorac. Surg. 2020, 30, 223–228. [Google Scholar] [CrossRef]
- Rosenbaum, A.N.; Dunlay, S.M.; Pereira, N.L.; Allison, T.G.; Maltais, S.; Stulak, J.M.; Joyce, L.D.; Kushwaha, S.S. Determinants of Improvement in Cardiopulmonary Exercise Testing After Left Ventricular Assist Device Implantation. ASAIO J. 2018, 64, 610–615. [Google Scholar] [CrossRef] [PubMed]
- Maybaum, S.; Mancini, D.; Xydas, S.; Starling, R.C.; Aaronson, K.; Pagani, F.D.; Miller, L.W.; Margulies, K.; McRee, S.; Frazier, O.H.; et al. Cardiac improvement during mechanical circulatory support: A prospective multicenter study of the LVAD Working Group. Circulation 2007, 115, 2497–2505. [Google Scholar] [CrossRef] [Green Version]
- Noor, M.R.; Bowles, C.; Banner, N.R. Relationship between pump speed and exercise capacity during HeartMate II left ventricular assist device support: Influence of residual left ventricular function. Eur. J. Heart Fail. 2012, 14, 613–620. [Google Scholar] [CrossRef]
- Jung, M.H.; Hansen, P.B.; Sander, K.; Olsen, P.S.; Rossing, K.; Boesgaard, S.; Russell, S.D.; Gustafsson, F. Effect of increasing pump speed during exercise on peak oxygen uptake in heart failure patients supported with a continuous-flow left ventricular assist device. A double-blind randomized study. Eur. J. Heart Fail. 2014, 16, 403–408. [Google Scholar] [CrossRef]
- Mancini, D.; Gibson, G.T. Survival of the Fittest. JACC Heart Fail. 2021, 9, 768–770. [Google Scholar] [CrossRef]
- Tolle, J.J.; Waxman, A.B.; Van Horn, T.L.; Pappagianopoulos, P.P.; Systrom, D.M. Exercise-induced pulmonary arterial hypertension. Circulation 2008, 118, 2183–2189. [Google Scholar] [CrossRef] [Green Version]
- Guazzi, M.; Myers, J.; Peberdy, M.A.; Bensimhon, D.; Chase, P.; Arena, R. Cardiopulmonary exercise testing variables reflect the degree of diastolic dysfunction in patients with heart failure-normal ejection fraction. J. Cardiopulm. Rehabil. Prev. 2010, 30, 165–172. [Google Scholar] [CrossRef] [Green Version]
- Fu, Q.; Vangundy, T.B.; Galbreath, M.M.; Shibata, S.; Jain, M.; Hastings, J.L.; Bhella, P.S.; Levine, B.D. Cardiac origins of the postural orthostatic tachycardia syndrome. J. Am. Coll. Cardiol. 2010, 55, 2858–2868. [Google Scholar] [CrossRef] [Green Version]
- Lewis, G.D.; Murphy, R.M.; Shah, R.V.; Pappagianopoulos, P.P.; Malhotra, R.; Bloch, K.D.; Systrom, D.M.; Semigran, M.J. Pulmonary vascular response patterns during exercise in left ventricular systolic dysfunction predict exercise capacity and outcomes. Circ. Heart Fail. 2011, 4, 276–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maron, B.A.; Cockrill, B.A.; Waxman, A.B.; Systrom, D.M. The invasive cardiopulmonary exercise test. Circulation 2013, 127, 1157–1164. [Google Scholar] [CrossRef] [PubMed]
- Psotka, M.A.; Abraham, W.T.; Fiuzat, M.; Filippatos, G.; Lindenfeld, J.; Ahmad, T.; Felker, G.M.; Jacob, R.; Kitzman, D.W.; Leifer, E.S.; et al. Functional and Symptomatic Clinical Trial Endpoints: The HFC-ARC Scientific Expert Panel. JACC Heart Fail. 2022, 10, 889–901. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Metabolic Exercise Variable | Normal Expected Range |
|---|---|
| Peak RER | 1.10–1.50 |
| Peak work-rate | >85% predicted peak Watts |
| Peak VO2 | >85% predicted peak VO2 |
| Rest VO2 | 2–5 mL/kg/min |
| VO2 at VAT | 40–75% predicted peak VO2 |
| CI | 0.80–1.30 |
| Peak VO2/HR | >85% predicted peak VO2/HR |
| VO2/WR slope | 8.5–12.5 mL/min/watts |
| Peak SpO2 | >95% |
| Peak VE | <85% predicted peak VE |
| Peak RR | <60 breaths/min |
| Peak VT | 1.5–3.0 liters |
| Peak PETCO2 | 35–41 mmHg |
| VE/VCO2 slope | <30 |
| EOV | None |
| Peak RPP | >18,966 mmHg × bpm |
| HGI | >1.06 bpm/mmHg |
| Circulatory Power | >3047 mmHg × mL/min/kg |
| OUES | >1.85 L/min |
| POUES | >0.88 L/min |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agdamag, A.C.; Van Iterson, E.H.; Tang, W.H.W.; Finet, J.E. Prognostic Role of Metabolic Exercise Testing in Heart Failure. J. Clin. Med. 2023, 12, 4438. https://doi.org/10.3390/jcm12134438
Agdamag AC, Van Iterson EH, Tang WHW, Finet JE. Prognostic Role of Metabolic Exercise Testing in Heart Failure. Journal of Clinical Medicine. 2023; 12(13):4438. https://doi.org/10.3390/jcm12134438
Chicago/Turabian StyleAgdamag, Arianne Clare, Erik H. Van Iterson, W. H. Wilson Tang, and J. Emanuel Finet. 2023. "Prognostic Role of Metabolic Exercise Testing in Heart Failure" Journal of Clinical Medicine 12, no. 13: 4438. https://doi.org/10.3390/jcm12134438