
Complicated Pocket Infection in Patients Undergoing Lead Extraction: Characteristics and Outcomes
 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. TLE Procedure
- ‘Complete success’ was classified as the removal of the entire lead system.
- ‘Partial success’ was defined as when most of the lead was removed, leaving at most 4 cm of coil and/or insulation and/or lead tip.
- ‘Failure’ was defined if more than ≥4 cm of the tip remained.
2.2. Principles of Antimicrobial Therapy
2.3. Statistical Analysis
3. Results
3.1. Demographic, Clinical, and Device Data
3.1.1. Patient Characteristics
3.1.2. Infection Manifestation
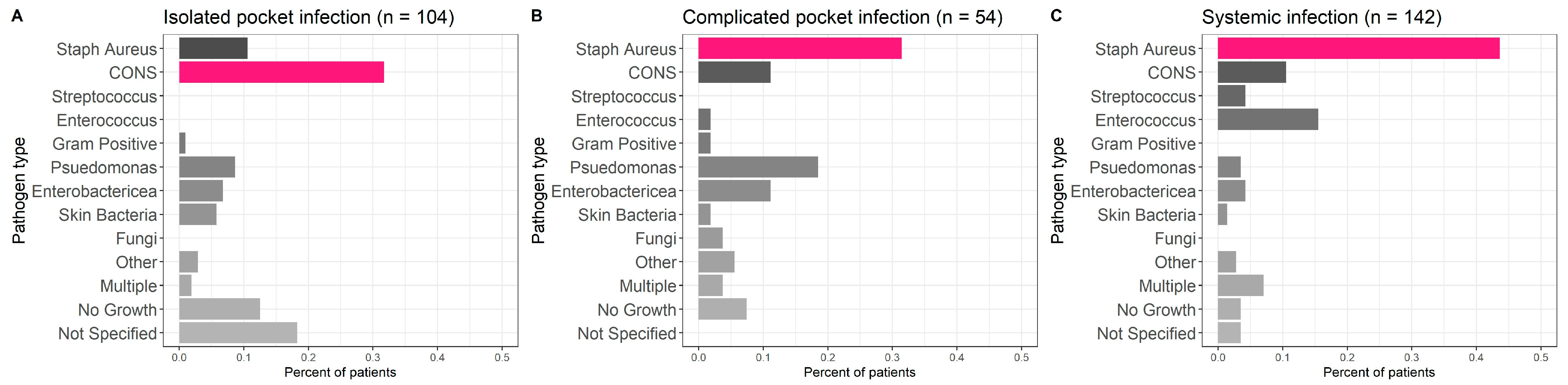
3.1.3. Infectious Pathogens
3.2. Outcomes
3.2.1. Procedural Outcomes
3.2.2. Reinfection Outcomes
3.2.3. Mortality
4. Discussion
4.1. Patient Characteristics
4.2. Infection Manifestation
4.3. Outcomes
4.4. Mortality
5. Conclusions
6. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brignole, M.; Auricchio, A.; Baron-Esquivias, G.; Bordachar, P.; Boriani, G.; Breithardt, O.A.; Cleland, J.G.F.; Deharo, J.-C.; Delgado, V.; Elliott, P.M.; et al. 2013 ESC guidelines on cardiac pacing and cardiac resynchronization therapy: The task force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Europace 2013, 15, 1070–1118. [Google Scholar] [PubMed]
- Epstein, A.E.; Dimarco, J.P.; Ellenbogen, K.A.; Estes, N.A., 3rd; Freedman, R.A.; Gettes, L.S.; American College of Cardiology/American Heart Association Task Force on Practice; American Association for Thoracic Surgery; Society of Thoracic Surgeons. ACC/AHA/HRS 2008 guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: Executive summary. Heart Rhythm 2008, 5, 934–955. [Google Scholar] [CrossRef] [PubMed]
- Wilkoff, B.L.; Love, C.J.; Byrd, C.L.; Bongiorni, M.G.; Carrillo, R.G.; Crossley, G.H., 3rd; Epstein, L.M.; Friedman, R.A.; Ken-nergren, C.E.; Mitkowski, P.; et al. Transvenous lead extraction: Heart Rhythm Society expert consensus on facilities, training, indications, and patient man-agement: This document was endorsed by the American Heart Association (AHA). Heart Rhythm 2009, 6, 1085–1104. [Google Scholar] [CrossRef] [PubMed]
- Baddour, L.M.; Epstein, A.E.; Erickson, C.C.; Knight, B.P.; Levison, M.E.; Lockhart, P.B.; Masoudi, F.A.; Okum, E.J.; Wilson, W.R.; Beerman, L.B.; et al. Update on cardiovascular implantable electronic device infections and their management: A scientific statement from the American Heart Association. Circulation 2010, 121, 458–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maytin, M.; Epstein, L.M. The challenges of transvenous lead extraction. Heart 2011, 97, 425–434. [Google Scholar] [CrossRef]
- Deharo, J.C.; Bongiorni, M.G.; Rozkovec, A.; Bracke, F.; Defaye, P.; Fernandez-Lozano, I.; Golzio, P.G.; Hansky, B.; Kennergren, C.; Manolis, A.; et al. Pathways for training and accreditation for transvenous lead extraction: A European Heart Rhythm Association position paper. Europace 2012, 14, 124–134. [Google Scholar]
- Sohal, M.; Williams, S.E.; Arujuna, A.; Chen, Z.; Bostock, J.; Gill, J.S.; Rinaldi, C.A. The current practice and perception of cardiac implantable electronic device transvenous lead extraction in the UK. Europace 2013, 15, 865–870. [Google Scholar] [CrossRef]
- Blomström-Lundqvist, C.; Traykov, V.; Erba, P.A.; Burri, H.; Nielsen, J.C.; Bongiorni, M.G.; Poole, J.; Boriani, G.; Costa, R.; Deharo, J.C.; et al. European Heart Rhythm Association (EHRA) international consensus document on how to prevent, diagnose, and treat cardiac implantable electronic device infections-endorsed by the Heart Rhythm Society (HRS), the Asia Pacific Heart Rhythm Society (APHRS), the Latin American Heart Rhythm Society (LAHRS), International Society for Cardiovascular Infectious Diseases (ISCVID), and the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2020, 41, 2012–2032. [Google Scholar]
- Kleemann, T.; Becker, T.; Strauss, M.; Dyck, N.; Weisse, U.; Saggau, W.; Burkhardt, U.; Seidl, K. Prevalence of bacterial colonization of generator pockets in implantable cardioverter defibrillator patients without signs of infection undergoing generator replacement or lead revision. Europace 2010, 12, 58–63. [Google Scholar] [CrossRef]
- Chambers, S.T. Diagnosis and management of staphylococcal infections of pacemakers and cardiac defibrillators. Intern. Med. J. 2005, 35 (Suppl. 2), S63–S71. [Google Scholar] [CrossRef]
- Klug, D.; Lacroix, D.; Savoye, C.; Goullard, L.; Grandmougin, D.; Hennequin, J.L.; Kacet, S.; Lekieffre, J. Systemic infection related to endocarditis on pacemaker leads: Clinical presentation and management. Circulation 1997, 95, 2098–2107. [Google Scholar] [CrossRef]
- Hussein, A.A.; Baghdy, Y.; Wazni, O.M.; Brunner, M.P.; Kabbach, G.; Shao, M.; Gordon, S.; Saliba, W.I.; Wilkoff, B.L.; Tarakji, K.G. Microbiology of cardiac implantable electronic device infections. JACC Clin. Electrophysiol. 2016, 2, 498–505. [Google Scholar] [CrossRef]
- Bongiorni, M.G.; Tascini, C.; Tagliaferri, E.; Di Cori, A.; Soldati, E.; Leonildi, A.; Zucchelli, G.; Ciullo, I.; Menichetti, F. Microbiology of cardiac implantable electronic device infections. Europace 2012, 14, 1334–1339. [Google Scholar] [CrossRef]
- Younis, A.; Glikson, M.; Meitus, A.; Arwas, N.; Natanzon, S.S.; Lotan, D.; Luria, D.; Beinart, R.; Nof, E. Transvenous lead extraction with laser reduces need for femoral approach during the procedure. PLoS ONE 2019, 14, e0215589. [Google Scholar] [CrossRef]
- Sandoe, J.A.; Barlow, G.; Chambers, J.B.; Gammage, M.; Guleri, A.; Howard, P.; Olson, E.; Perry, J.D.; Prendergast, B.D.; Spry, M.J.; et al. Guidelines for the diagnosis, prevention and management of implantable cardiac electronic device infection. Report of a joint Working Party project on behalf of the British Society for Antimicrobial Chemotherapy (BSAC, host organization), British Heart Rhythm Society (BHRS), British Cardiovascular Society (BCS), British Heart Valve Society (BHVS) and British Society for Echocardiography (BSE). J. Antimicrob. Chemother. 2015, 70, 325–359. [Google Scholar]
- Tarakji, K.G.; Chan, E.J.; Cantillon, D.J.; Doonan, A.L.; Hu, T.; Schmitt, S.; Fraser, T.G.; Kim, A.; Gordon, S.M.; Wilkoff, B.L. Cardiac implantable electronic device infections: Presentation, management, and patient outcomes. Heart Rhythm 2010, 7, 1043–1047. [Google Scholar] [CrossRef] [PubMed]
- Polyzos, K.A.; Konstantelias, A.A.; Falagas, M.E. Risk factors for cardiac implantable electronic device infection: A systematic review and meta-analysis. Europace 2015, 17, 767–777. [Google Scholar] [CrossRef]
- Milman, A.; Zahavi, G.; Meitus, A.; Kariv, S.; Shafir, Y.; Glikson, M.; Luria, D.; Beinart, R.; Nof, E. Predictors of short-term mortality in patients undergoing a successful uncomplicated extraction procedure. J. Cardiovasc. Electrophysiol. 2020, 31, 1155–1162. [Google Scholar] [CrossRef]
- Hörnsten, J.; Axelsson, L.; Westling, K. Cardiac Implantable Electronic Device Infections; Long-Term Outcome after Extraction and Antibiotic Treatment. Infect. Dis. Rep. 2021, 13, 59. [Google Scholar] [CrossRef]
- Uslan, D.Z.; Sohail, M.R.; St Sauver, J.L.; Friedman, P.A.; Hayes, D.L.; Stoner, S.M.; Wilson, W.R.; Steckelberg, J.M.; Baddour, L.M. Permanent pacemaker and implantable cardioverter defibrillator infection: A population-based study. Arch. Intern. Med. 2007, 167, 669–675. [Google Scholar] [CrossRef] [Green Version]
- Fukunaga, M.; Goya, M.; Nagashima, M.; Hiroshima, K.; Yamada, T.; An, Y.; Hayashi, K.; Makihara, Y.; Ohe, M.; Ichihashi, K.; et al. Identification of causative organism in cardiac implantable electronic device infections. J. Cardiol. 2017, 70, 411–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrasco, F.; Anguita, M.; Ruiz, M.; Castillo, J.C.; Delgado, M.; Mesa, D.; Romo, E.; Pan, M.; De Lezo, J.S. Clinical features and changes in epidemiology of infective endocarditis on pacemaker devices over a 27-year period (1987–2013). Europace 2016, 18, 836–841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esquer Garrigos, Z.; George, M.P.; Vijayvargiya, P.; Tan, E.M.; Farid, S.; Abu Saleh, O.M.; Friedman, P.A.; Steckelberg, J.M.; DeSimone, D.C.; Wilson, W.R.; et al. Clinical Presentation, Management, and Outcomes of Cardiovascular Implantable Electronic Device Infections Due to Gram-Negative Versus Gram-Positive Bacteria. Mayo Clin. Proc. 2019, 94, 1268–1277. [Google Scholar] [CrossRef] [PubMed]
- Boyle, T.A.; Uslan, D.Z.; Prutkin, J.M.; Greenspon, A.J.; Baddour, L.M.; Danik, S.B.; Tolosana, J.M.; Le, K.; Miro, J.M.; Peacock, J.; et al. Reimplantation and Repeat Infection After Cardiac-Implantable Electronic Device Infections: Experience from the MEDIC (Multicenter Electrophysiologic Device Infection Cohort) Database. Circ. Arrhythm. Electrophysiol. 2017, 10, e004822. [Google Scholar] [CrossRef]
- Tarakji, K.G.; Wazni, O.M.; Harb, S.; Hsu, A.; Saliba, W.; Wilkoff, B.L. Risk factors for 1-year mortality among patients with cardiac implantable electronic device infection undergoing transvenous lead extraction: The impact of the infection type and the presence of vegetation on survival. Europace 2014, 16, 1490–1495. [Google Scholar] [CrossRef]
- Bongiorni, M.G.; Kennergren, C.; Butter, C.; Deharo, J.C.; Kutarski, A.; Rinaldi, C.A.; Romano, S.L.; Maggioni, A.P.; Andarala, M.; Auricchio, A.; et al. The European Lead Extraction ConTRolled (ELECTRa) study: A European Heart Rhythm Association (EHRA) Registry of Transvenous Lead Extraction Outcomes. Eur. Heart J. 2017, 38, 2995–3005. [Google Scholar] [CrossRef]
- Nishii, N.; Morimoto, Y.; Miyoshi, A.; Tsukuda, S.; Miyamoto, M.; Kawada, S.; Nakagawa, K.; Watanabe, A.; Nakamura, K.; Morita, H.; et al. Prognosis after lead extraction in patients with cardiac implantable electronic devices infection: Comparison of lead-related infective endocarditis with pocket infection in a Japanese single-center experience. J. Arrhythm. 2019, 35, 654–663. [Google Scholar] [CrossRef]
- Ihlemann, N.; Møller-Hansen, M.; Salado-Rasmussen, K.; Videbæk, R.; Moser, C.; Iversen, K.; Bundgaard, H. CIED infection with either pocket or systemic infection presentation—Complete device removal and long-term antibiotic treatment; long-term outcome. Scand. Cardiovasc. J. 2016, 50, 52–57. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Infection Type | Overall | Pocket Infection | Systemic | p Value | ||
|---|---|---|---|---|---|---|
| Isolated | Complicated | |||||
| Number of patients | 300 | 104 | 54 | 142 | ||
| Demographics | ||||||
| Female | 67 (22.3) | 22 (21.2) | 11 (20.4) | 34 (23.9) | 0.812 | |
| Age (mean ± SD) | 66.6 ± 15.5 | 66.6 ± 16.6 | 64.2 ± 18.8 | 67.5 ± 13.0 | 0.414 | |
| Referral from other center | 205 (68.3) | 71 (68.3) | 35 (64.8) | 99 (69.7) | 0.805 | |
| Comorbiditis | ||||||
| Smoking | 78 (26.0) | 25 (24.0) | 14 (25.9) | 39 (27.5) | 0.833 | |
| Atrial fibrillation | 110 (36.7) | 40 (38.5) | 13 (24.1) | 57 (40.1) | 0.102 | |
| Hypertension | 180 (60.0) | 62 (59.6) | 26 (48.1) | 92 (64.8) | 0.104 | |
| Heart failure | 135 (45.0) | 44 (42.3) | 26 (48.1) | 65 (45.8) | 0.758 | |
| Stroke | 42 (14.0) | 14 (13.5) | 4 (7.4) | 24 (16.9) | 0.227 | |
| Vascular disease | 168 (56.0) | 58 (55.8) | 27 (50.0) | 83 (58.5) | 0.566 | |
| Malignancy | 21 (7.0) | 8 (7.7) | 3 (5.6) | 10 (7.0) | 0.882 | |
| Diabetes mellitus | 131 (43.7) | 35 (33.7) | 19 (35.2) | 77 (54.2) | 0.002 | |
| LVEF (%±SD) | 40.5 ± 16.5 | 40.7 ± 15.4 | 39.4 ± 17.1 | 40.8 ± 17.2 | 0.878 | |
| Prosthetic valve | 0.061 | |||||
| Biological | 14 (4.7) | 2 (1.9) | 1 (1.9) | 11 (7.7) | ||
| Mechanical | 15 (5.0) | 6 (5.8) | 5 (9.3) | 4 (2.8) | ||
| No | 271 (90.3) | 96 (92.3) | 48 (88.9) | 127 (89.4) | ||
| Device type | 0.546 | |||||
| CRT-D | 74 (24.7) | 29 (27.9) | 13 (24.1) | 32 (22.5) | ||
| CRT-P | 9 (3.0) | 4 (3.8) | 3 (5.6) | 2 (1.4) | ||
| ICD | 38 (12.7) | 14 (13.5) | 8 (14.8) | 16 (11.3) | ||
| PM | 179 (59.7) | 57 (54.8) | 30 (55.6) | 92 (64.8) | ||
| Infection Type | Overall | Systemic | p Value | |||
|---|---|---|---|---|---|---|
| Isolated | Complicated | |||||
| Number of patients | 300 | 104 | 54 | 142 | ||
| Prior device infection | 44 (14.7) | 19 (18.3) | 9 (16.7) | 16 (11.3) | 0.278 | |
| Temperature > 37.8 °C | <0.001 | |||||
| No | 156 (52.0) | 94 (90.4) | 28 (51.9) | 34 (23.9) | ||
| Yes | 134 (44.7) | 9 (8.7) | 23 (42.6) | 102 (71.8) | ||
| Unspecified | 10 (3.3) | 1 (1.0) | 3 (5.6) | 6 (4.2) | ||
| Lekuocytosis > 10K | 113 (37.7) | 23 (22.1) | 19 (35.2) | 71 (50.0) | <0.001 | |
| Duration of antibiotics (days) | 27.7 ± 19.8 | 16.5 ± 11.5 | 32.1 ± 24.6 | 34.1 ± 19.3 | <0.001 | |
| Lab results | ||||||
| Creatinine (mg/dL) | 1.4 ± 1.0 | 1.2 ± 0.7 | 1.3 ± 0.8 | 1.6 ± 1.1 | 0.001 | |
| Hemoglobin (g/dL) | 11.1 ± 1.9 | 12.0 ± 1.7 | 11.9 ± 1.5 | 10.2 ± 1.6 | <0.001 | |
| Albumin (g/dL) | 3.2 ± 0.7 | 3.7 ± 0.5 | 3.5 ± 0.5 | 2.8 ± 0.7 | <0.001 | |
| Pocket Dehiscence | <0.001 | |||||
| Negative | 179 (59.7) | 25 (24.0) | 15 (27.8) | 139 (97.9) | ||
| Positive | 117 (39.0) | 78 (75.0) | 39 (72.2) | 0 (0.0) | ||
| Unspecified | 4 (1.3) | 1 (1.0) | 0 (0.0) | 3 (2.1) | ||
| Pocket Culture | <0.001 | |||||
| Negative | 130 (43.3) | 15 (14.4) | 5 (9.3) | 110 (77.5) | ||
| Positive | 154 (51.3) | 87 (83.7) | 48 (88.9) | 19 (13.4) | ||
| Not performed | 10 (3.3) | 0 (0.0) | 0 (0.0) | 10 (7.0) | ||
| Unspecified | 6 (2.0) | 2 (1.9) | 1 (1.9) | 3 (2.1) | ||
| Blood Culture | <0.001 | |||||
| Negative | 149 (49.7) | 102 (98.1) | 24 (44.4) | 23 (16.2) | ||
| Positive | 148 (49.3) | 0 (0.0) | 29 (53.7) | 119 (83.8) | ||
| Not performed | 2 (0.7) | 1 (1.0) | 1 (1.9) | 0 (0.0) | ||
| Unspecified | 1 (0.3) | 1 (1.0) | 0 (0.0) | 0 (0.0) | ||
| Lead Culture | 0.501 | |||||
| Negative | 205 (68.3) | 67 (64.4) | 39 (72.2) | 99 (69.7) | ||
| Positive | 85 (28.3) | 31 (29.8) | 14 (25.9) | 40 (28.2) | ||
| Not performed | 8 (2.7) | 5 (4.8) | 1 (1.9) | 2 (1.4) | ||
| Unspecified | 2 (0.7) | 1 (1.0) | 0 (0.0) | 1 (0.7) | ||
| Transthoracic Echocardiography | 0.002 | |||||
| No vegetation | 166 (55.3) | 61 (58.7) | 34 (63.0) | 71 (50.0) | ||
| Vegetation | 25 (8.3) | 0 (0.0) | 9 (16.7) | 16 (11.3) | ||
| Not performed | 69 (23.0) | 21 (20.2) | 10 (18.5) | 38 (26.8) | ||
| Unspecified | 40 (13.3) | 22 (21.2) | 1 (1.9) | 17 (12.0) | ||
| Transesophageal Echocardiography | <0.001 | |||||
| No vegetation | 75 (25.0) | 40 (38.5) | 12 (22.2) | 23 (16.2) | ||
| Vegetation | 102 (34.0) | 0 (0.0) | 28 (51.9) | 74 (52.1) | ||
| Not performed | 29 (9.7) | 22 (21.2) | 3 (5.6) | 4 (2.8) | ||
| Unspecified | 94 (31.3) | 42 (40.4) | 11 (20.4) | 41 (28.9) | ||
| Infection Type | Overall | Systemic | p Value | ||
|---|---|---|---|---|---|
| Isolated | Complicated | ||||
| Number of patients | 300 | 104 | 54 | 142 | |
| First device to extraction (days) | 2691.7 ± 2187.3 | 2966.6 ± 2417.3 | 2814.0 ± 2003.0 | 2442.9 ± 2058.2 | 0.163 |
| Current device to extraction (days) | 1394.7 ± 1485.7 | 1170.1 ± 1304.9 | 1293.9 ± 1527.0 | 1600.9 ± 1576.6 | 0.076 |
| Last intervention to extraction (days) | 907.3 ± 975.1 | 705.5 ± 842.1 | 521.2 ± 684.3 | 1183.8 ± 1068.3 | <0.001 |
| Entries to pocket | 2.0 (1.1) | 2.4 (1.2) | 2.2 (1.2) | 1.6 (0.9) | <0.001 |
| Extraction type | 0.078 | ||||
| Simple | 88 (29.3) | 31 (29.8) | 9 (16.7) | 48 (33.8) | |
| Complex | 209 (69.7) | 73 (70.2) | 43 (79.6) | 93 (65.5) | |
| Unspecified | 3 (1.0) | 0 (0.0) | 2 (3.7) | 1 (0.7) | |
| Number of leads extracted | 2.2 (0.9) | 2.3 (0.9) | 2.4 (1.0) | 2.2 (0.8) | 0.314 |
| Extraction success | 0.724 | ||||
| Full | 274 (91.3) | 94 (90.4) | 49 (90.7) | 131 (92.3) | |
| Partial | 18 (6.0) | 8 (7.7) | 2 (3.7) | 8 (5.6) | |
| Failure | 6 (2.0) | 2 (1.9) | 2 (3.7) | 2 (1.4) | |
| Unspecified | 2 (0.7) | 0 (0.0) | 1 (1.9) | 1 (0.7) | |
| Minor complications | 11 (3.7) | 4 (3.8) | 2 (3.7) | 5 (3.5) | 0.991 |
| Major complications | 7 (2.3) | 3 (2.9) | 2 (3.7) | 2 (1.4) | 0.572 |
| Temporary reimplant | 77 (25.7) | 27 (26.0) | 19 (35.2) | 31 (21.8) | 0.160 |
| Intra-procedural death | 2 (0.7) | 1 (1.0) | 1 (1.9) | 0 (0.0) | 0.327 |
| Infection Type | Overall | Systemic | p Value | ||
|---|---|---|---|---|---|
| Isolated | Complicated | ||||
| Number of patients | 300 | 104 | 54 | 142 | |
| Permanent reimplant | 230 (76.7) | 84 (80.8) | 49 (90.7) | 97 (68.3) | 0.002 |
| Time to reimplant (days) | 46 ± 103 | 53 ± 111 | 55 ± 78 | 34 ± 106 | 0.557 |
| Infection within 30 days | 0.108 | ||||
| No | 134 (44.7) | 53 (51.0) | 25 (46.3) | 56 (39.4) | |
| Yes | 11 (3.7) | 1 (1.0) | 1 (1.9) | 9 (6.3) | |
| Unspecified | 155 (51.7) | 50 (48.1) | 28 (51.9) | 77 (54.2) | |
| At 30 days | ||||
| Mortality at 30 days | Odds ratio | Lower CI 95% | Upper CI 95% | p value |
| Diabetes mellitus | 1.14 | 0.5 | 2.61 | 0.748 |
| Creatinine (mg/dL) | 1.43 | 1.03 | 1.99 | 0.034 |
| Albumin (g/dL) | 0.44 | 0.2 | 0.96 | 0.038 |
| Hemoglobin (g/dL) | 1.01 | 0.75 | 1.35 | 0.973 |
| Lekuocytosis > 10K | 1.43 | 0.63 | 3.25 | 0.392 |
| Temperature > 37.8 | 0.79 | 0.29 | 2.17 | 0.654 |
| Staph aureus | 1.46 | 0.62 | 3.39 | 0.384 |
| Isolated pocket infection | 0.54 | 0.1 | 2.87 | 0.471 |
| Systemic infection | 1.43 | 0.42 | 4.89 | 0.557 |
| At 1 year | ||||
| Mortality at 1 year | Odds ratio | Lower CI 95% | Upper CI 95% | p value |
| Age | 1.04 | 1 | 1.07 | 0.017 |
| Atrial fibrillation | 2.35 | 1.22 | 4.55 | 0.01 |
| Heart failure | 1.36 | 0.68 | 2.73 | 0.386 |
| Vascular disease | 1.11 | 0.53 | 2.29 | 0.785 |
| Diabetes mellitus | 1.04 | 0.52 | 2.09 | 0.905 |
| Creatinine (mg/dL) | 1.69 | 1.21 | 2.35 | 0.001 |
| Albumin (g/dL) | 0.33 | 0.17 | 0.64 | < 0.001 |
| Hemoglobin (g/dL) | 1.12 | 0.88 | 1.43 | 0.339 |
| Lekuocytosis > 10K | 1.2 | 0.61 | 2.36 | 0.597 |
| Temperature > 37.8 | 0.52 | 0.22 | 1.23 | 0.13 |
| Staph aureus | 1.34 | 0.64 | 2.8 | 0.433 |
| Isolated pocket infection | 1.06 | 0.32 | 3.48 | 0.925 |
| Systemic infection | 2.24 | 0.8 | 6.23 | 0.113 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milman, A.; Wieder-Finesod, A.; Zahavi, G.; Meitus, A.; Kariv, S.; Shafir, Y.; Beinart, R.; Rahav, G.; Nof, E. Complicated Pocket Infection in Patients Undergoing Lead Extraction: Characteristics and Outcomes. J. Clin. Med. 2023, 12, 4397. https://doi.org/10.3390/jcm12134397
Milman A, Wieder-Finesod A, Zahavi G, Meitus A, Kariv S, Shafir Y, Beinart R, Rahav G, Nof E. Complicated Pocket Infection in Patients Undergoing Lead Extraction: Characteristics and Outcomes. Journal of Clinical Medicine. 2023; 12(13):4397. https://doi.org/10.3390/jcm12134397
Chicago/Turabian StyleMilman, Anat, Anat Wieder-Finesod, Guy Zahavi, Amit Meitus, Saar Kariv, Yuval Shafir, Roy Beinart, Galia Rahav, and Eyal Nof. 2023. "Complicated Pocket Infection in Patients Undergoing Lead Extraction: Characteristics and Outcomes" Journal of Clinical Medicine 12, no. 13: 4397. https://doi.org/10.3390/jcm12134397