
Habituation to Pain in Patients with Chronic Pain: Clinical Implications and Future Directions

Abstract
:1. Introduction
2. Materials and Methods
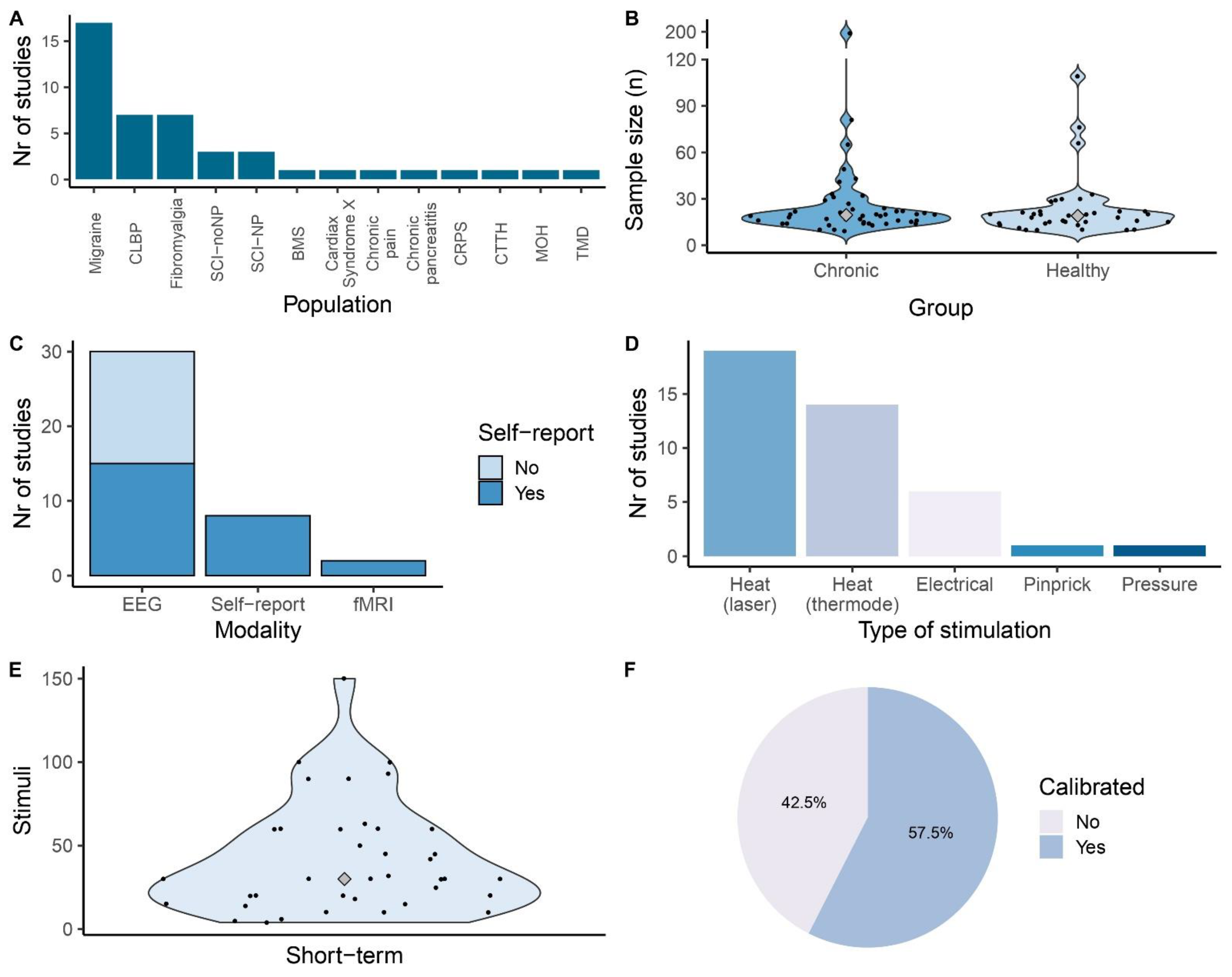
3. Results
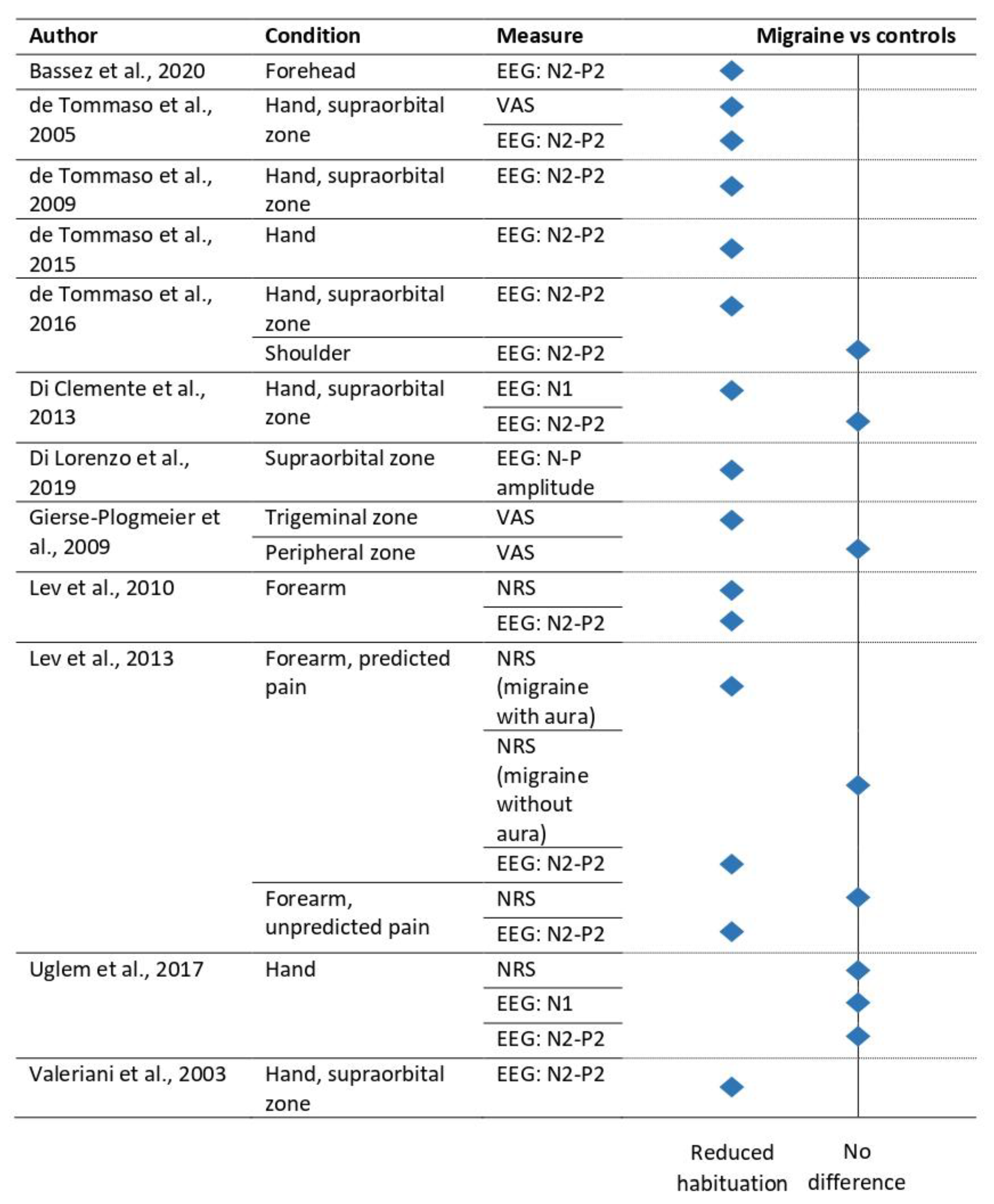
3.1. Headache Disorders

| Sample Size | Timescale | Type of Stimuli | Site | Nr of Stimuli for Habituation Analysis | Duration | ISI | Habituation Measurement | HabituationAnalysis | Main Habituation Result | |
|---|---|---|---|---|---|---|---|---|---|---|
| Bassez et al., 2020 [14] | M = 23 C = 20 | Short-term | Heat (CO2 laser) | Right forehead | 15 | Intensity (and, thus, duration) varied per participant, 15–45 ms | Self-paced, ± 10 s | EEG: N2–P2 amplitude Dynamic causal modelling | % change between first and third block Connectivity changes over blocks | M < C Increased thalamo-somatosensory connectivity in migraine patients |
| Beese et al., 2015 [16] | M = 22 (12 with aura) C = 22 | Short-term | Heat (thermode) | Volar forearm, left and right cheek | 20 | - | 15–18 s | NRS: single trial CHEP: N2–P2 amplitude | Average of first 5 trials vs. last 5 trials Average of first 5 trials vs. last 5 trials | NRS for each site and block: M ↘ C ↘ N2–P2 for each site and block: M ↘ C ↘ |
| de Tommaso et al., 2005 [17] | M = 14 (without aura) C = 10 | Short-term | Heat (CO2 laser) | Right and left hand and supraorbital zone | 60 | 20 ms | 10 s | NRS: single trial EEG: N2–P2 amplitude | Trend over block Trend over block | NRS both hand and face: M ↗ < C ↘ N2-P2 both hand and face: M → < C ↘ No differences between migraine phase |
| de Tommaso et al., 2005 [21] | M = 14 (without aura) C = 10 | Short-term | Heat (CO2 laser) | Right supraorbital zone | 63 | 20 ms | 10 s | VAS: single trial EEG: N2–P2 amplitude | Trend over block Trend over block | VAS: M → C ↘ N2-P2: M → C ↘ |
| de Tommaso et al., 2009 [24] | M = 9 (without aura) C = 10 | Short-term | Heat (CO2 laser) | Right dorsum of the hand and supraorbital zone | 60 | 25 ms | 10–15 s | EEG: N2–P2 amplitude | Ratio of amplitude between block 1 and 3 | Both hand and face: M < C Menstrual cycle affects habituation of N2–P2 |
| de Tommaso et al., 2015 [22] | M = 31 (without aura) C = 19 | Short-term | Heat (CO2 laser) | Dorsum of the right hand | 30 | 30 ms | 10 s | EEG: N2–P2 amplitude | Stimuli were divided in three blocks, % change relative to first block | M < C |
| De Tommaso et al., 2016 [27] | M = 20 C = 20 | Short-term | Heat (CO2 laser) | Dorsum of the right hand, right supraorbital zone and the skin over the right trapezius | 30 | 30 ms | 7 s | EEG: N2–P2 amplitude | Stimuli were divided in three blocks, % change relative to first block | Baseline N2–P2 hand and face: M < C Shoulder: M = C After onabotulintoxin A treatment, N2–P2 habituation at face increased, no effect on hand and shoulder habituation |
| De Tommaso et al., 2021 [28] | M = 17 | Short-term | Heat (CO2 laser) | Dorsum of the right hand and left and right supraorbital zone | 30 | 30 ms | 10 s | EEG: N1, N2, P2 amplitude | Ratio between average of last and first 10 stimuli | No effect of erenumab on N1 and P2 at both sides, increased habituation after erenumab at N2 of left forehead |
| Di Clemente et al., 2013 [25] | M = 13 (without aura) C = 15 | Short-term | Heat (YAP laser) | Dorsum of the right hand and right supraorbital zone | 45 | - | 10 s | EEG: N1 and N2–P2 amplitude | % change between first and third block | N1 hand and face: M < C N2–P2 hand and face: M = C Topiramate reduces N1 habituation deficit/affects habituation |
| Di Lorenzo et al., 2019 [29] | M = 18 (without aura) C = 18 | Short-term | Electrical | Right supraorbital notch | 10 | Train of 3 0.1 ms pulses with 5 ms interal (total 10.3 ms) | 30–35 s | PREP: N–P amplitude | Slope between first and second block | Before treatment: M < C After treatment: no group comparison Ketogenic diet increased habituation in migraine |
| Ferraro et al., 2012 [30] | MOH = 14 (group I treatment effective = 8; group II treatment not effective = 6) C = 14 | Short-term | Heat (CO2 laser) | Dorsum of the right hand and perioral region | 90 | 10 ms | 8–12 s | VAS: after each block EEG: N1 and N2–P2 amplitude | Percentage of the first block Percentage of the first block | VAS: Before treatment for hand and face: MOH group I and II < C After treatment hand: MOH group II < C and MOH group I After treatment face: MOH group I and II = C EEG: N1 hand before treatment: MOH group I and II < C N1 hand after treatment: MOH group I and II = C N1 face before treatment: MOH group II < C N1 face after treatment: MOH group I and II < C N2–P2 hand and face before treatment: MOH group I and II < C N2–P2 hand and face after treatment: MOH group II < C and MOH group I Treatment affected habituation in clinically improved patients |
| Gierse-Plogmeier et al., 2009 [15] | M = 20 (10 with aura) C = 20 | Short-term | Electrical | Trigeminal (masseter region), peripheral (tibial region) | 20 | 1 ms | 2 s | VAS: last stimulus of train | Group comparison of difference score between trains | Trigeminal: M < C Peripheral: M = C |
| Lev et al., 2010 [19] | M = 21 (with aura) C = 22 | Short-term | Heat (thermode) | Left volar forearm | 60 | - | – | NRS: single trial CHEP: N2–P2 amplitude and sLORETA | Group comparison of inter-train changeGroup comparison of inter-train change | NRS: M ↗ < C → N2-P2: M ↗ < C ↘ > M < C activity in contralateral orbitofrontal cortex M > C in contralateral primary somatosensory cortex, insula, parahippocampal cortex, and bilateral posterior cingulate cortex |
| Lev et al., 2013 [18] | MWA = 20MOA = 19 C = 22 | Short-term | Heat (thermode) | Left volar forearm | 50 | - | 10 s | NRS: single trial CHEP: N2–P2 amplitude and sLORETA | Group comparison of inter-train change Group comparison of inter-train change | NRS: Predicted pain: MWA ↗ < C → and MOA → Unpredicted pain: MOA ↗ = MWA ↗ = C → N2-P2: Predicted pain: MOA → and MWA ↗ < C ↘ Unpredicted pain: MOA ↗ and MWA ↗ < C → Predicted pain: MWA < C activity in right inferior frontal gyrus and supplementary motor area MWA > C activity in primary and secondary somatosensory cortex, motor cortex, and bilateral posterior cingulate cortex MOA > C activity in right insula Unpredicted pain: MWA > C activity in bilateral medial frontal cortex, right anterior cingulate cortexMOA > C activity in right motor cortex, primary and secondary somatosensory cortex, left orbitofrontal cortex, parahippocampal cortex, and insula |
| Sava et al., 2018 [26] | M = 14 (without aura) C = 11 | Short-term | Heat (thermode) | Right volar wrist or forehead | 20 | 707 ms | 10–22 s | CHEP: P1–P2 slope | Slope over average of 5 blocks | Mirror did not influence habituation in controls or migraine patients |
| Sebastianelli et al., 2023 [31] | M = 15 | Short-term | Electrical | Supraorbital nerve at the forehead | 18 | Three 0.1 ms pulses with 5 ms interval | 40 s | EEG: N–P amplitude | Slope of the amplitude between the first and third block | No effect of onabotulintoxin A on habituation |
| Uglem et al., 2017 [20] | M = 49 (27 without aura, 4 with, 18 both) C = 30 | Short-term | Heat (YAP laser) | Dorsum of the right hand | 42 | 6 ms | 6–10 s | NRS: single trial EEG: N1 and N2–P2 amplitude | Multilevel models | NRS: M → = C → N1: M → = C → N2-P2: M ↘ = C ↘ Habituation was mainly similar between migraine phases |
| Valeriani et al., 2003 [23] | M = 24 (without aura) CTTH = 19 C = 28 | Short-term | Heat (CO2 laser) | Left and right dorsum of the hand and face | 45 for face, 90 for hand | 10 ms | 8–12 s | EEG: N1–P1 and N2–P2 amplitude | % decrease over blocks | N1–P1 hand: M → C ↘ N1–P1 face: M → C → N2–P2 hand: M ↘ < C ↘, CTTH ↘ = C ↘, M ↘ < CTTH ↘ N2–P2 face: M → < C ↘, CTTH ↘ = C ↘ |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
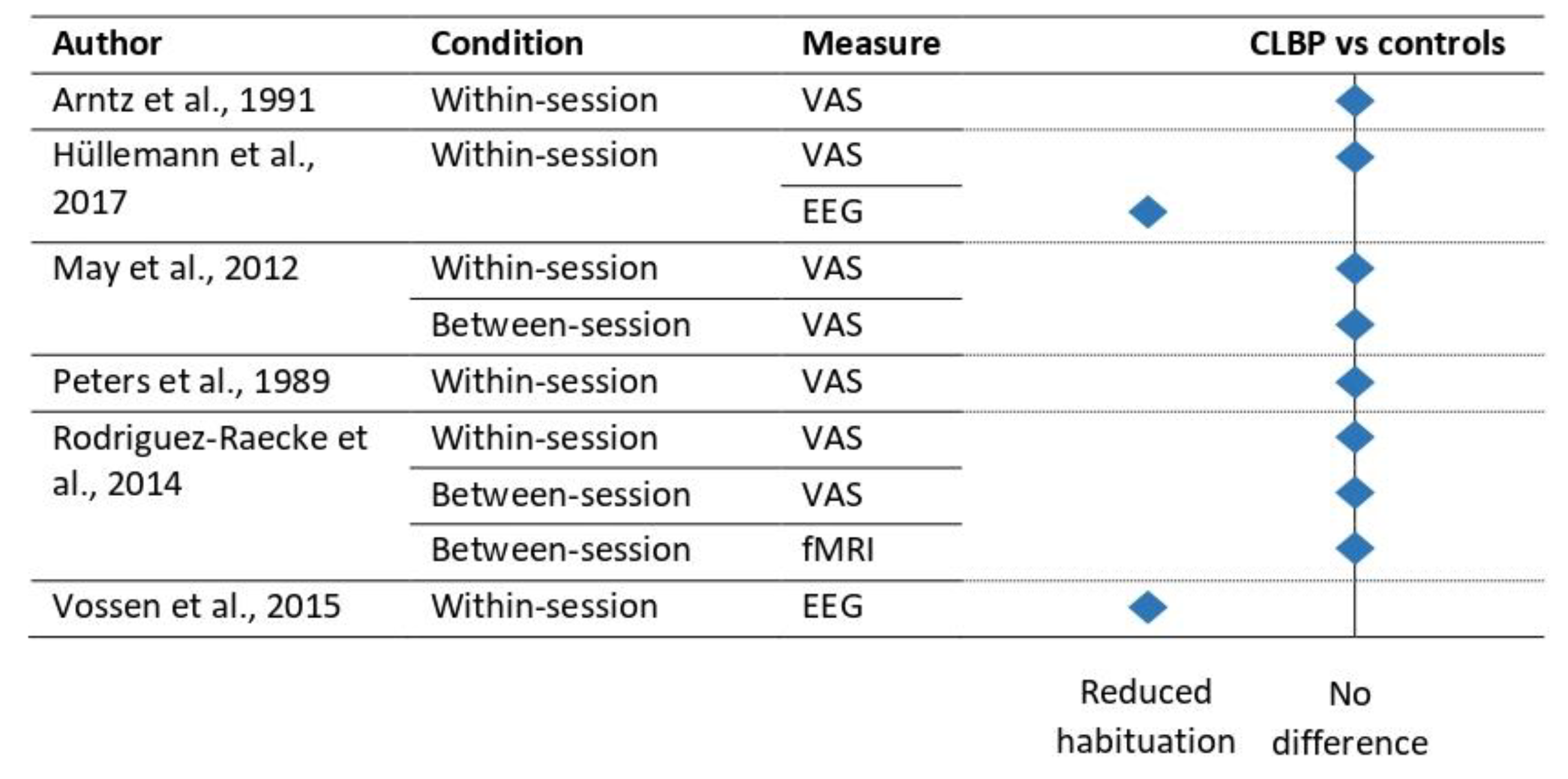
3.2. Chronic Low Back Pain
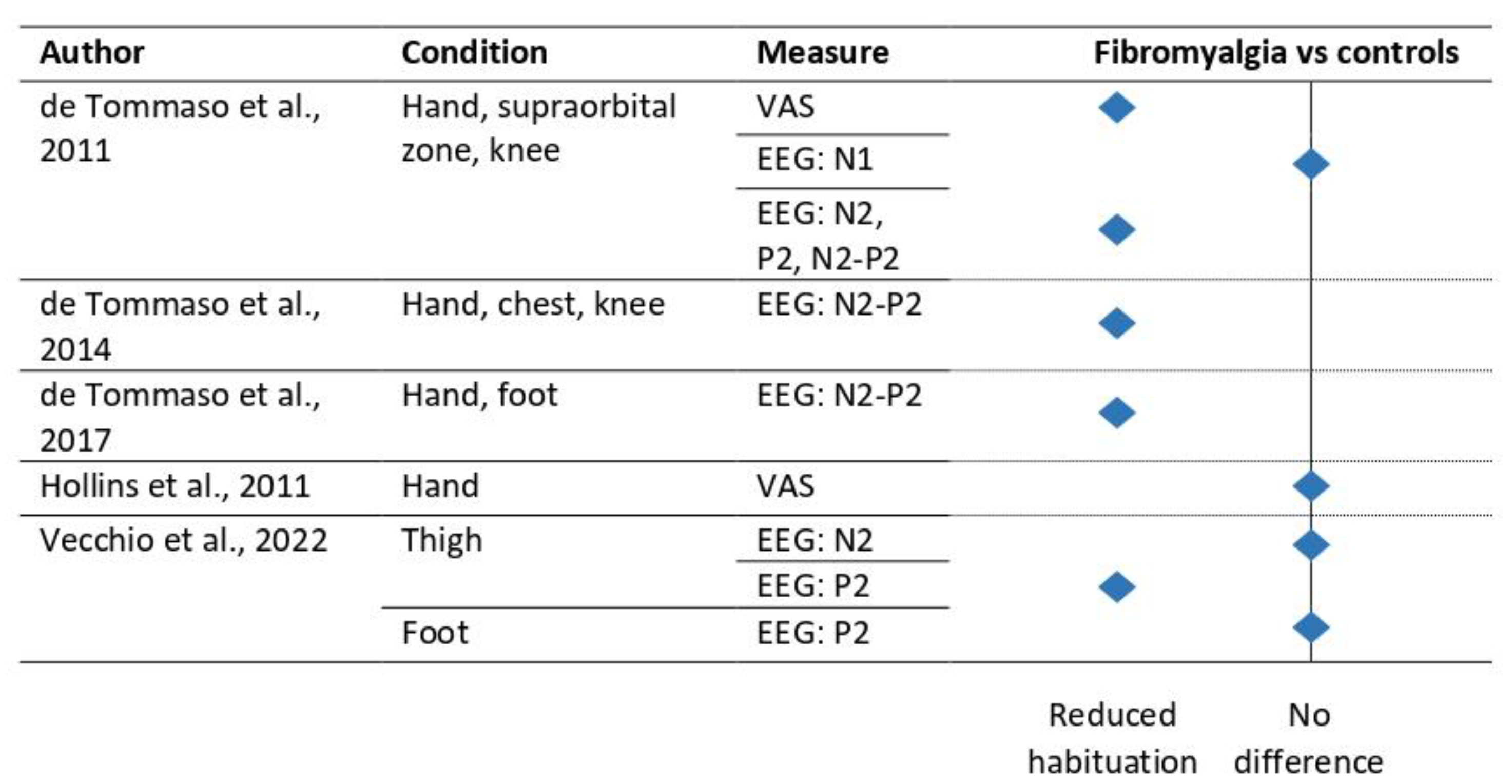
3.3. Fibromyalgia
3.4. Other Chronic Pain Indications
| Sample Size | Timescale | Type of Stimuli | Site | Nr of Stimuli for Habituation Analysis | Duration | ISI | Habituation Measurement | HabituationAnalysis | Main Habituation Result | |
|---|---|---|---|---|---|---|---|---|---|---|
| Albu et al., 2015 [54] | SCI-noNP = 10 SCI-NP = 10 C = 10 | Short-term | Heat (thermode) | Thenar eminence of dominant hand | 10 | - | 20 s | NRS: single trial CHEP: N2–P2 amplitude | Percentage last stimulus with respect to first stimulus | NRS and CHEP: SCI-noNP = SCI-NP = C |
| Hollins et al., 2011 [40] | F = 17 TMD = 29 C = 29 | Short-term | Heat (thermode) | Base of the thumb | 33 | 3 s | 12 s | VAS: single trial | Decrease over blocks | F = TMD = C |
| Kumru et al., 2012 [53] | SCI-noNP = 22 SCI-NP = 32 C = 16 | Short-term | Heat (thermode) | Shoulder | 14 | - | 30 s | NRS: single trial CHEP: N2–P2 amplitude | % change of last compared to first stimulus | NRS and CHEP: SCI-NP < SCI-noNP SCI-NP < C |
| Lütolf et al., 2022 [55] | SCI-noNP = 13, SCI-NP = 17, C = 14 | Short-term | Heat (thermode) | Right volar forearm | 10 | - | 15–19 s | NRS: single trial | Percentage decrease | SCI-noNP = SCI-NP = C |
| Olesen et al., 2013 [52] | Chronic pancreatitis = 15 C = 15 | Short-term | Heat (thermode) | Right forearm and upper abdominal area | 93 | - | 8–12 s | VAS: first and last stimulus of block CHEP: N1 and N2–P2 amplitude | Change over blocks | Abdominal: CP → < C ↘ Forearm: CP → < C ↘ Abdominal: N1: CP = C N2–P2: CP → < C ↘ Forearm: N1: CP = C N2–P2: CP → = C ↘ |
| Scheuren et al., 2023 [56] | CRPS = 20, C = 16 | Short-term | Heat (thermode), pinprick | Affected and control area | 15 | - | 13–17s | NRS: single trial | % change in third compared to first block and trend over blocks | Heat: CRPS → = C → Pinprick: CRPS → = C → |
| Shinozaki et al., 2016 [50] | BMS = 16 C = 15 | Short-term | Heat (thermode) | Right palm and right lower lip | 4 | 32 s | 104 s | NRS: single trial fMRI: BOLD | Stimulus 1 compared to 4 | NRS: Lip: BMS → C ↘ Palm: BMS → C → fMRI: Lip: Reduced activity in BMS patients over time in the right dorsal anterior cingulate cortex, bilateral ventral midcingulate cortex, left posterior cingulate cortex, right angular gyrus, and left cerebellum. Increased activity in controls over time in the left posterior cingulate cortex. |
| Valeriani et al., 2005 [51] | Cardiac syndrome X = 16 Coronary artery disease = 10 C = 13 | Short-term | Heat (CO2 laser) | Dorsum of the right hand and chest | 90 | 10 ms | 8–12 s | VAS: per block EEG: N1–P1 and N2–P2 amplitude | Trend over blocks | Chest: VAS and N2–P2: Cardiac SX → < C ↘ and CAD ↘ N1–P1: Cardiac SX = CAD = C Hand: VAS: Cardiac SX ↗ < C ↘ and CAD ↘ N1–P1: Cardiac SX = CAD = C N2–P2: Cardiac SX = CAD = C |
| Vossen et al., 2018 [57] | Chronic pain (various) = 33 C = 33 | Short-term | Electrical | Left middle finger | 25 | 10 ms | 9–11 s | VRS: single trial EEG: amplitude | Multilevel model with event-related fixed-interval areas | VRS: Chronic pain ↘ = C ↘ No influence of hypervigilance on pain ratings Chronic pain status and hypervigilance independently influenced the EEG-amplitude |
4. Treatments and Clinical Implications
4.1. Habituation to Pain and Clinical Outcomes
4.2. Treatments Targeting Habituation to Pain
4.3. Discussion and Future Directions
5. Challenges in the Field
6. Future Directions for Research
Limitations
7. Conclusions
Supplementary Materials
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rankin, C.H.; Abrams, T.; Barry, R.J.; Bhatnagar, S.; Clayton, D.F.; Colombo, J.; Coppola, G.; Geyer, M.A.; Glanzman, D.L.; Marsland, S. Habituation revisited: An updated and revised description of the behavioral characteristics of habituation. Neurobiol. Learn. Mem. 2009, 92, 135–138. [Google Scholar] [CrossRef] [Green Version]
- McDiarmid, T.A.; Bernardos, A.C.; Rankin, C.H. Habituation is altered in neuropsychiatric disorders-A comprehensive review with recommendations for experimental design and analysis. Neurosci. Biobehav. Rev. 2017, 80, 286–305. [Google Scholar] [CrossRef]
- Thompson, R.F.; Spencer, W.A. Habituation: A model phenomenon for the study of neuronal substrates of behavior. Psychol. Rev. 1966, 73, 16. [Google Scholar] [CrossRef] [Green Version]
- De Paepe, A.L.; Williams, A.C.C.; Crombez, G. Habituation to pain: A motivational-ethological perspective. Pain 2019, 160, 1693–1697. [Google Scholar] [CrossRef] [Green Version]
- IASP. International Association for the Study of Pain (IASP). Available online: https://www.iasp-pain.org/resources/terminology/. (accessed on 11 April 2023).
- Harte, S.E.; Harris, R.E.; Clauw, D.J. The neurobiology of central sensitization. J. Appl. Biobehav. Res. 2018, 23, e12137. [Google Scholar] [CrossRef] [Green Version]
- van den Broeke, E.; Crombez, G.; Vlaeyen, J.W. Re-conceptualizing sensitization in pain: A case for a behavioural approach. PsychArchives 2023. [Google Scholar] [CrossRef]
- Groves, P.M.; Thompson, R.F. Habituation: A dual-process theory. Psychol. Rev. 1970, 77, 419. [Google Scholar] [CrossRef]
- Ramaswami, M. Network plasticity in adaptive filtering and behavioral habituation. Neuron 2014, 82, 1216–1229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- May, A.; Rodriguez-Raecke, R.; Schulte, A.; Ihle, K.; Breimhorst, M.; Birklein, F.; Jürgens, T.P. Within-session sensitization and between-session habituation: A robust physiological response to repetitive painful heat stimulation. Eur. J. Pain 2012, 16, 401–409. [Google Scholar] [CrossRef]
- Rodriguez-Raecke, R.; Ihle, K.; Ritter, C.; Muhtz, C.; Otte, C.; May, A. Neuronal differences between chronic low back pain and depression regarding long-term habituation to pain. Eur. J. Pain 2014, 18, 701–711. [Google Scholar] [CrossRef] [Green Version]
- Leonardi, M.; Steiner, T.J.; Scher, A.T.; Lipton, R.B. The global burden of migraine: Measuring disability in headache disorders with WHO’s Classification of Functioning, Disability and Health (ICF). J. Headache Pain 2005, 6, 429–440. [Google Scholar] [CrossRef] [Green Version]
- Casillo, F.; Sebastianelli, G.; Di Renzo, A.; Cioffi, E.; Parisi, V.; Di Lorenzo, C.; Serrao, M.; Coppola, G. The monoclonal CGRP-receptor blocking antibody erenumab has different effects on brainstem and cortical sensory-evoked responses. Cephalalgia 2022, 42, 1236–1245. [Google Scholar] [CrossRef]
- Bassez, I.; Van de Steen, F.; Ricci, K.; Vecchio, E.; Gentile, E.; Marinazzo, D.; de Tommaso, M. Dynamic Causal Modelling of the Reduced Habituation to Painful Stimuli in Migraine: An EEG Study. Brain Sci. 2020, 10, 712. [Google Scholar] [CrossRef] [PubMed]
- Gierse-Plogmeier, B.; Colak-Ekici, R.; Wolowski, A.; Gralow, I.; Marziniak, M.; Evers, S. Differences in trigeminal and peripheral electrical pain perception in women with and without migraine. J. Headache Pain 2009, 10, 249–254. [Google Scholar] [CrossRef] [Green Version]
- Beese, L.C.; Putzer, D.; Osada, N.; Evers, S.; Marziniak, M. Contact heat evoked potentials and habituation measured interictally in migraineurs. J. Headache Pain 2015, 16, 1. [Google Scholar] [CrossRef] [Green Version]
- de Tommaso, M.; Lo Sito, L.; Di Fruscolo, O.; Sardaro, M.; Pia Prudenzano, M.; Lamberti, P.; Livrea, P. Lack of habituation of nociceptive evoked responses and pain sensitivity during migraine attack. Clin. Neurophysiol. 2005, 116, 1254–1264. [Google Scholar] [CrossRef] [PubMed]
- Lev, R.; Granovsky, Y.; Yarnitsky, D. Enhanced pain expectation in migraine: EEG-based evidence for impaired prefrontal function. Headache 2013, 53, 1054–1070. [Google Scholar] [CrossRef] [PubMed]
- Lev, R.; Granovsky, Y.; Yarnitsky, D. Orbitofrontal disinhibition of pain in migraine with aura: An interictal EEG-mapping study. Cephalalgia 2010, 30, 910–918. [Google Scholar] [CrossRef] [PubMed]
- Uglem, M.; Omland, P.M.; Stjern, M.; Gravdahl, G.B.; Sand, T. Habituation of laser-evoked potentials by migraine phase: A blinded longitudinal study. J. Headache Pain 2017, 18, 100. [Google Scholar] [CrossRef] [Green Version]
- de Tommaso, M.; Libro, G.; Guido, M.; Losito, L.; Lamberti, P.; Livrea, P. Habituation of single CO2 laser-evoked responses during interictal phase of migraine. J. Headache Pain 2005, 6, 195–198. [Google Scholar] [CrossRef] [Green Version]
- de Tommaso, M.; Trotta, G.; Vecchio, E.; Ricci, K.; Van de Steen, F.; Montemurno, A.; Lorenzo, M.; Marinazzo, D.; Bellotti, R.; Stramaglia, S. Functional Connectivity of EEG Signals Under Laser Stimulation in Migraine. Front. Hum. Neurosci. 2015, 9, 640. [Google Scholar] [CrossRef] [Green Version]
- Valeriani, M.; de Tommaso, M.; Restuccia, D.; Le Pera, D.; Guido, M.; Iannetti, G.D.; Libro, G.; Truini, A.; Di Trapani, G.; Puca, F.; et al. Reduced habituation to experimental pain in migraine patients: A CO2 laser evoked potential study. Pain 2003, 105, 57–64. [Google Scholar] [CrossRef]
- de Tommaso, M.; Valeriani, M.; Sardaro, M.; Serpino, C.; Fruscolo, O.D.; Vecchio, E.; Cerbo, R.; Livrea, P. Pain perception and laser evoked potentials during menstrual cycle in migraine. J. Headache Pain 2009, 10, 423–429. [Google Scholar] [CrossRef] [Green Version]
- Di Clemente, L.; Puledda, F.; Biasiotta, A.; Viganò, A.; Vicenzini, E.; Truini, A.; Cruccu, G.; Di Piero, V. Topiramate modulates habituation in migraine: Evidences from nociceptive responses elicited by laser evoked potentials. J. Headache Pain 2013, 14, 25. [Google Scholar] [CrossRef] [Green Version]
- Sava, S.L.; de Pasqua, V.; de Noordhout, A.M.; Schoenen, J. Visually induced analgesia during face or limb stimulation in healthy and migraine subjects. J. Pain Res. 2018, 11, 1821–1828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Tommaso, M.; Delussi, M.; Ricci, K.; Montemurno, A.; Carbone, I.; Vecchio, E. Effects of onabotulintoxinA on habituation of laser evoked responses in chronic migraine. Toxins 2016, 8, 163. [Google Scholar] [CrossRef] [Green Version]
- de Tommaso, M.; Delussi, M.; Gentile, E.; Ricci, K.; Quitadamo, S.G.; Libro, G. Effect of single dose Erenumab on cortical responses evoked by cutaneous a-delta fibers: A pilot study in migraine patients. Cephalalgia 2021, 41, 1004–1014. [Google Scholar] [CrossRef]
- Di Lorenzo, C.; Coppola, G.; Bracaglia, M.; Di Lenola, D.; Sirianni, G.; Rossi, P.; Di Lorenzo, G.; Parisi, V.; Serrao, M.; Cervenka, M.C.; et al. A ketogenic diet normalizes interictal cortical but not subcortical responsivity in migraineurs. BMC Neurol 2019, 19, 136. [Google Scholar] [CrossRef] [PubMed]
- Ferraro, D.; Vollono, C.; Miliucci, R.; Virdis, D.; De Armas, L.; Pazzaglia, C.; Le Pera, D.; Tarantino, S.; Balestri, M.; Di Trapani, G.; et al. Habituation to pain in “medication overuse headache”: A CO2 laser-evoked potential study. Headache 2012, 52, 792–807. [Google Scholar] [CrossRef] [PubMed]
- Sebastianelli, G.; Casillo, F.; Di Renzo, A.; Abagnale, C.; Cioffi, E.; Parisi, V.; Di Lorenzo, C.; Serrao, M.; Pierelli, F.; Schoenen, J.; et al. Effects of Botulinum Toxin Type A on the Nociceptive and Lemniscal Somatosensory Systems in Chronic Migraine: An Electrophysiological Study. Toxins 2023, 15, 76. [Google Scholar] [CrossRef]
- Hoy, D.; Bain, C.; Williams, G.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Vos, T.; Buchbinder, R. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012, 64, 2028–2037. [Google Scholar] [CrossRef] [PubMed]
- Maher, C.; Underwood, M.; Buchbinder, R. Non-specific low back pain. Lancet 2017, 389, 736–747. [Google Scholar] [CrossRef] [Green Version]
- Arntz, A.; Merckelbach, H.; Peters, M.; Schmidt, A.J. Chronic low back pain, response specificity and habituation to painful stimuli. J. Psychophysiol. 1991, 5, 177–188. [Google Scholar]
- Peters, M.L.; Schmidt, A.J.; Van den Hout, M.A. Chronic low back pain and the reaction to repeated acute pain stimulation. Pain 1989, 39, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Hüllemann, P.; von der Brelie, C.; Manthey, G.; Düsterhöft, J.; Helmers, A.K.; Synowitz, M.; Baron, R. Reduced laser-evoked potential habituation detects abnormal central pain processing in painful radiculopathy patients. Eur. J. Pain 2017, 21, 918–926. [Google Scholar] [CrossRef]
- Vossen, C.J.; Vossen, H.G.; Joosten, E.A.; van Os, J.; Lousberg, R. Does habituation differ in chronic low back pain subjects compared to pain-free controls? A cross-sectional pain rating ERP study reanalyzed with the ERFIA multilevel method. Medicine 2015, 94, e865. [Google Scholar] [CrossRef] [PubMed]
- Kersebaum, D.; Fabig, S.C.; Sendel, M.; Muntean, A.C.; Baron, R.; Hullemann, P. Revealing the time course of laser-evoked potential habituation by high temporal resolution analysis. Eur. J. Pain 2021, 25, 2112–2128. [Google Scholar] [CrossRef]
- Häuser, W.; Ablin, J.; Fitzcharles, M.-A.; Littlejohn, G.; Luciano, J.V.; Usui, C.; Walitt, B. Fibromyalgia. Nat. Rev. Dis. Prim. 2015, 1, 15022. [Google Scholar] [CrossRef]
- Hollins, M.; Harper, D.; Maixner, W. Changes in pain from a repetitive thermal stimulus: The roles of adaptation and sensitization. Pain 2011, 152, 1583–1590. [Google Scholar] [CrossRef] [Green Version]
- de Tommaso, M.; Federici, A.; Santostasi, R.; Calabrese, R.; Vecchio, E.; Lapadula, G.; Iannone, F.; Lamberti, P.; Livrea, P. Laser-evoked potentials habituation in fibromyalgia. J. Pain 2011, 12, 116–124. [Google Scholar] [CrossRef]
- de Tommaso, M.; Nolano, M.; Iannone, F.; Vecchio, E.; Ricci, K.; Lorenzo, M.; Delussi, M.; Girolamo, F.; Lavolpe, V.; Provitera, V.; et al. Update on laser-evoked potential findings in fibromyalgia patients in light of clinical and skin biopsy features. J. Neurol. 2014, 261, 461–472. [Google Scholar] [CrossRef] [PubMed]
- de Tommaso, M.; Ricci, K.; Libro, G.; Vecchio, E.; Delussi, M.; Montemurno, A.; Lopalco, G.; Iannone, F. Pain Processing and Vegetative Dysfunction in Fibromyalgia: A Study by Sympathetic Skin Response and Laser Evoked Potentials. Pain Res. Treat. 2017, 2017, 9747148. [Google Scholar] [CrossRef] [Green Version]
- Vecchio, E.; Quitadamo, S.G.; Ricci, K.; Libro, G.; Delussi, M.; Lombardi, R.; Lauria, G.; de Tommaso, M. Laser evoked potentials in fibromyalgia with peripheral small fiber involvement. Clin. Neurophysiol. 2022, 135, 96–106. [Google Scholar] [CrossRef]
- McLoughlin, M.J.; Stegner, A.J.; Cook, D.B. The relationship between physical activity and brain responses to pain in fibromyalgia. J. Pain 2011, 12, 640–651. [Google Scholar] [CrossRef] [Green Version]
- Vecchio, E.; Lombardi, R.; Paolini, M.; Libro, G.; Delussi, M.; Ricci, K.; Quitadamo, S.G.; Gentile, E.; Girolamo, F.; Iannone, F.; et al. Peripheral and central nervous system correlates in fibromyalgia. Eur. J. Pain 2020, 24, 1537–1547. [Google Scholar] [CrossRef]
- Gauer, R.; Semidey, M.J. Diagnosis and treatment of temporomandibular disorders. Am. Fam. Physician 2015, 91, 378–386. [Google Scholar]
- Nicholas, M.; Vlaeyen, J.W.S.; Rief, W.; Barke, A.; Aziz, Q.; Benoliel, R.; Cohen, M.; Evers, S.; Giamberardino, M.A.; Goebel, A.; et al. The IASP classification of chronic pain for ICD-11: Chronic primary pain. Pain 2019, 160, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Jääskeläinen, S.K.; Woda, A. Burning mouth syndrome. Cephalalgia 2017, 37, 627–647. [Google Scholar] [CrossRef] [Green Version]
- Shinozaki, T.; Imamura, Y.; Kohashi, R.; Dezawa, K.; Nakaya, Y.; Sato, Y.; Watanabe, K.; Morimoto, Y.; Shizukuishi, T.; Abe, O.; et al. Spatial and Temporal Brain Responses to Noxious Heat Thermal Stimuli in Burning Mouth Syndrome. J. Dent. Res. 2016, 95, 1138–1146. [Google Scholar] [CrossRef]
- Valeriani, M.; Sestito, A.; Le Pera, D.; De Armas, L.; Infusino, F.; Maiese, T.; Sgueglia, G.A.; Tonali, P.A.; Crea, F.; Restuccia, D.; et al. Abnormal cortical pain processing in patients with cardiac syndrome X. Eur. Heart J. 2005, 26, 975–982. [Google Scholar] [CrossRef] [PubMed]
- Olesen, S.S.; Hansen, T.M.; Graversen, C.; Valeriani, M.; Drewes, A.M. Cerebral excitability is abnormal in patients with painful chronic pancreatitis. Eur. J. Pain 2013, 17, 46–54. [Google Scholar] [CrossRef]
- Kumru, H.; Soler, D.; Vidal, J.; Tormos, J.M.; Pascual-Leone, A.; Valls-Sole, J. Evoked potentials and quantitative thermal testing in spinal cord injury patients with chronic neuropathic pain. Clin. Neurophysiol. 2012, 123, 598–604. [Google Scholar] [CrossRef] [PubMed]
- Albu, S.; Gómez-Soriano, J.; Avila-Martin, G.; Taylor, J. Deficient conditioned pain modulation after spinal cord injury correlates with clinical spontaneous pain measures. Pain 2015, 156, 260–272. [Google Scholar] [CrossRef]
- Lütolf, R.; Rosner, J.; Curt, A.; Hubli, M. Indicators of central sensitization in chronic neuropathic pain after spinal cord injury. Eur. J. Pain 2022, 26, 2162–2175. [Google Scholar] [CrossRef]
- Scheuren, P.S.; De Schoenmacker, I.; Rosner, J.; Brunner, F.; Curt, A.; Hubli, M. Pain-autonomic measures reveal nociceptive sensitization in complex regional pain syndrome. Eur. J. Pain 2023, 27, 72–85. [Google Scholar] [CrossRef] [PubMed]
- Vossen, C.J.; Luijcks, R.; van Os, J.; Joosten, E.A.; Lousberg, R. Does pain hypervigilance further impact the lack of habituation to pain in individuals with chronic pain? A cross-sectional pain ERP study. J. Pain Res. 2018, 11, 395–405. [Google Scholar] [CrossRef] [Green Version]
- Masino, S.A.; Rho, J.M. Mechanisms of Ketogenic Diet Action. In Jasper’s Basic Mechanisms of the Epilepsies; Noebels, J.L., Avoli, M., Rogawski, M.A., Olsen, R.W., Delgado-Escueta, A.V., Eds.; National Center for Biotechnology Information (US): Bethesda, MD, USA, 2012. [Google Scholar]
- Burstein, R.; Blumenfeld, A.M.; Silberstein, S.D.; Manack Adams, A.; Brin, M.F. Mechanism of Action of OnabotulinumtoxinA in Chronic Migraine: A Narrative Review. Headache J. Head Face Pain 2020, 60, 1259–1272. [Google Scholar] [CrossRef]
- Marcianò, G.; Vocca, C.; Evangelista, M.; Palleria, C.; Muraca, L.; Galati, C.; Monea, F.; Sportiello, L.; De Sarro, G.; Capuano, A. The Pharmacological Treatment of Chronic Pain: From Guidelines to Daily Clinical Practice. Pharmaceutics 2023, 15, 1165. [Google Scholar] [CrossRef] [PubMed]
- Chong, M.; Libretto, S.E. The rationale and use of topiramate for treating neuropathic pain. Clin. J. Pain 2003, 19, 59–68. [Google Scholar] [CrossRef]
- Masino, S.A.; Ruskin, D.N. Ketogenic diets and pain. J. Child Neurol. 2013, 28, 993–1001. [Google Scholar] [CrossRef] [Green Version]
- Bauch, E.M.; Andreou, C.; Rausch, V.H.; Bunzeck, N. Neural Habituation to Painful Stimuli Is Modulated by Dopamine: Evidence from a Pharmacological fMRI Study. Front. Hum. Neurosci. 2017, 11, 630. [Google Scholar] [CrossRef] [Green Version]
- Blok, L.E.R.; Boon, M.; van Reijmersdal, B.; Höffler, K.D.; Fenckova, M.; Schenck, A. Genetics, molecular control and clinical relevance of habituation learning. Neurosci. Biobehav. Rev. 2022, 143, 104883. [Google Scholar] [CrossRef]
- Brighina, F.; Cosentino, G.; Fierro, B. Is lack of habituation a biomarker of migraine? A critical perspective. J. Headache Pain 2015, 16, A13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rennefeld, C.; Wiech, K.; Schoell, E.D.; Lorenz, J.; Bingel, U. Habituation to pain: Further support for a central component. Pain 2010, 148, 503–508. [Google Scholar] [CrossRef]
- Ji, R.R.; Kohno, T.; Moore, K.A.; Woolf, C.J. Central sensitization and LTP: Do pain and memory share similar mechanisms? Trends Neurosci. 2003, 26, 696–705. [Google Scholar] [CrossRef]
- Nieuwenhuis, S.; Forstmann, B.U.; Wagenmakers, E.-J. Erroneous analyses of interactions in neuroscience: A problem of significance. Nat. Neurosci. 2011, 14, 1105–1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slepian, P.M.; France, C.R.; Rhudy, J.L.; Himawan, L.K.; Güereca, Y.M.; Kuhn, B.L.; Palit, S. Behavioral Inhibition and Behavioral Activation are Related to Habituation of Nociceptive Flexion Reflex, but Not Pain Ratings. J. Pain 2017, 18, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Edwards, R.R.; Fillingim, R.B. Effects of age on temporal summation and habituation of thermal pain: Clinical relevance in healthy older and younger adults. J. Pain 2001, 2, 307–317. [Google Scholar] [CrossRef]
- Greffrath, W.; Baumgärtner, U.; Treede, R.D. Peripheral and central components of habituation of heat pain perception and evoked potentials in humans. Pain 2007, 132, 301–311. [Google Scholar] [CrossRef]
- Jepma, M.; Jones, M.; Wager, T.D. The dynamics of pain: Evidence for simultaneous site-specific habituation and site-nonspecific sensitization in thermal pain. J. Pain 2014, 15, 734–746. [Google Scholar] [CrossRef] [Green Version]
- Hoofwijk, D.; Fiddelers, A.A.; Peters, M.L.; Stessel, B.; Kessels, A.G.; Joosten, E.A.; Gramke, H.-F.; Marcus, M.A. Prevalence and predictive factors of chronic postsurgical pain and poor global recovery 1 year after outpatient surgery. Clin. J. Pain 2015, 31, 1017–1025. [Google Scholar] [CrossRef]
- Rolke, R.; Baron, R.; Maier, C.A.; Tölle, T.; Treede, R.-D.; Beyer, A.; Binder, A.; Birbaumer, N.; Birklein, F.; Bötefür, I. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): Standardized protocol and reference values. Pain 2006, 123, 231–243. [Google Scholar] [CrossRef] [PubMed]
- Rolke, R.; Magerl, W.; Campbell, K.A.; Schalber, C.; Caspari, S.; Birklein, F.; Treede, R.D. Quantitative sensory testing: A comprehensive protocol for clinical trials. Eur. J. Pain 2006, 10, 77–88. [Google Scholar] [CrossRef] [PubMed]
- Vossen, C.J.; Vossen, H.G.; Marcus, M.A.; van Os, J.; Lousberg, R. Introducing the event related fixed interval area (ERFIA) multilevel technique: A method to analyze the complete epoch of event-related potentials at single trial level. PLoS ONE 2013, 8, e79905. [Google Scholar] [CrossRef]
- Coppola, G.; Pierelli, F.; Schoenen, J. Habituation and migraine. Neurobiol. Learn. Mem. 2009, 92, 249–259. [Google Scholar] [CrossRef]
- Flor, H.; Diers, M.; Birbaumer, N. Peripheral and electrocortical responses to painful and non-painful stimulation in chronic pain patients, tension headache patients and healthy controls. Neurosci. Lett. 2004, 361, 147–150. [Google Scholar] [CrossRef] [PubMed]





| Sample Size | Timescale | Type of Stimuli | Site | Nr of Stimuli for Habituation Analysis | Duration | ISI | Habituation Measurement | HabituationAnalysis | Main Habituation Result | |
|---|---|---|---|---|---|---|---|---|---|---|
| Arntz et al., 1991 [34] | CLBP = 22 C = 21 | Short-term | Electrical | Thumb of left hand | 20 | 1 s | 15–45 s | VAS: pretest, last trial of blocks, post-test | Trend over time | CLBP ↘ = C ↘ |
| Hüllemann et al., 2017 [36] | Painful radiculopathy = 27 C = 20 | Short-term | Heat (YAP laser) | Middle ventral thigh | 100 | 5 ms | 8–12 s | NRS: single trail EEG: N2–P2 amplitude | Trend over blocks | P ↘ = C ↘ P ↘ < C ↘ |
| Kersebaum et al., 2021 [38] | Painful radiculopathy n = 14 for twelve blocks and n = 18 for six blocks, controls n = 10 for twelve blocks and n = 14 for six blocks | Short-term | Heat (YAP laser) | Middle ventral thigh | 100 | 5 ms | 8–12 s | NRS: single trial EEG: N2–P2 amplitude | High-temporal-resolution analysis | NRS: over 12 blocks P ↘ C NA, over six blocks P → C → N2–P2: over 12 blocks P ↘ C NA, over six blocks P ↘ C → |
| May et al., 2012 [10] | CLBP = 21 C = 66 | Long-term (8 days) | Heat (thermode) | Left volar forearm | 480 | 6 s | – | VAS: average rating of last 6 stimuli | Trend over time | Within-session: CLBP ↗ = C ↗ Between-session: CLBP ↘ = C ↘ |
| Peters et al., 1989 [35] | CLBP = 20 C = 20 | Short-term | Pressure | Index finger of non-dominant hand | 6 | 70% of pain tolerance time | 4 min | VAS: single trials | Trend over time | CLBP → = C → |
| Rodriguez-Raecke et al., 2014 [11] | CLBP = 19 C = 21 | Long-term (8 days) | Heat (thermode) | Left volar forearm | 480 | 6 s | – | VAS: average rating of last 6 stimulifMRI: BOLD | Trend over time Whole-brain contrast | Within-session: CLBP ↗ = C ↗ Between-session: CLBP ↘ = C ↘ CLBP = C |
| Vossen et al., 2015 [37] | CLBP = 65 C = 76 | Short-term | Electrical | Left middle finger | 150 | 10 ms | 9–11 s | EEG: amplitude | Multilevel model with event-related fixed-interval areas | CLBP ↘ < C ↘ |
| Sample Size | Timescale | Type of Stimuli | Site | Nr of Stimuli for Habituation Analysis | Duration | ISI | Habituation Measurement | HabituationAnalysis | Main Habituation Result | |
|---|---|---|---|---|---|---|---|---|---|---|
| de Tommaso et al., 2011 [41] | F = 14 C = 13 | Short-term | Heat (CO2 laser) | Dorsum of the right hand, right supraorbital zone and knee | 20 | 25 ms | 10 s | VAS: average per block EEG: N1, N2, P2, and N2–P2 amplitude | Quotient between third and first block | VAS: F < C N1: F = C N2, P2, and N2–P2: F < C No differences between sites Self-reported depressive symptoms correlate with N2 habituation |
| de Tommaso et al., 2014 [42] | F combined = 199 F = 94 F with M = 70F with sensory deficits = 35 C = 109 | Short-term | Heat (CO2 laser) | Dorsum of the right hand, chest and knee | 10 | 30 ms | 10 s | EEG: N2–P2 amplitude | Quotient between third and first block | All sites: F combined < C F < C F with M < C F with sensory deficits < C F with M < F F with M < F with sensory deficits No correlation between habituation and self-reported depressive symptoms |
| de Tommaso et al., 2017 [43] | F = 50 C = 30 | Short-term | Heat (CO2 laser) | Dorsum of the right hand and foot | 30 | 30 ms | 10 s | EEG: N2–P2 amplitude | Percent amplitude change between third and first group of responses | Hand and foot: F < C |
| Hollins et al., 2011 [40] | F = 17 TMD = 29 C = 29 | Short-term | Heat (thermode) | Base of the thumb | 33 | 3 s | 12 s | VAS: single trial | Decrease over blocks | F = TMD = C |
| McLoughlin et al., 2011 [45] | F = 16 C = 18 | Short-term | Heat (thermode) | Left hand palm | 5 | 20 s | 20 s | VAS: single trial | Difference score | Self-reported activity correlated negatively with pain and unpleasantness difference scores in patients |
| Vecchio et al., 2020 [46] | F = 81 | Short-term | Heat (CO2 laser) | Dorsum of the right hand, in subgroups also thorax and dorsum of the foot | 30 | 30 ms | 10 s | EEG: N2–P2 amplitude | Ratio between third and first block | Thigh: habituation index of N2–P2 predicted intra-epidermal nerve fiber density |
| Vecchio et al., 2022 [44] | F = 41 (F with normal skin biopsy FMN = 18, F with proximal denervation FMP = 22, F with proximal and distal denervation FMD = 7) C = 15 | Short-term | Heat (CO2 laser) | Thigh and dorsum of the foot | 30 | 30 ms | 10 s | EEG: N2 and P2 amplitude | Change over time between third and first block | Thigh N2: F = C Thigh P2: F < C (all groups, FMN > FMP, FMD) Foot P2: F = C Patients with reduced intra-epidermal nerve fiber density showed less habituation of the P2 component |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van der Miesen, M.M.; Vossen, C.J.; Joosten, E.A. Habituation to Pain in Patients with Chronic Pain: Clinical Implications and Future Directions. J. Clin. Med. 2023, 12, 4305. https://doi.org/10.3390/jcm12134305
van der Miesen MM, Vossen CJ, Joosten EA. Habituation to Pain in Patients with Chronic Pain: Clinical Implications and Future Directions. Journal of Clinical Medicine. 2023; 12(13):4305. https://doi.org/10.3390/jcm12134305
Chicago/Turabian Stylevan der Miesen, Maite M., Catherine J. Vossen, and Elbert A. Joosten. 2023. "Habituation to Pain in Patients with Chronic Pain: Clinical Implications and Future Directions" Journal of Clinical Medicine 12, no. 13: 4305. https://doi.org/10.3390/jcm12134305