
The Effect of Laparoscopic Sleeve Gastrectomy on the Course of Non-Alcoholic Fatty Liver Disease in Morbidly Obese Patients during One Year of Follow Up
 , ,
, ,
Abstract
:1. Introduction
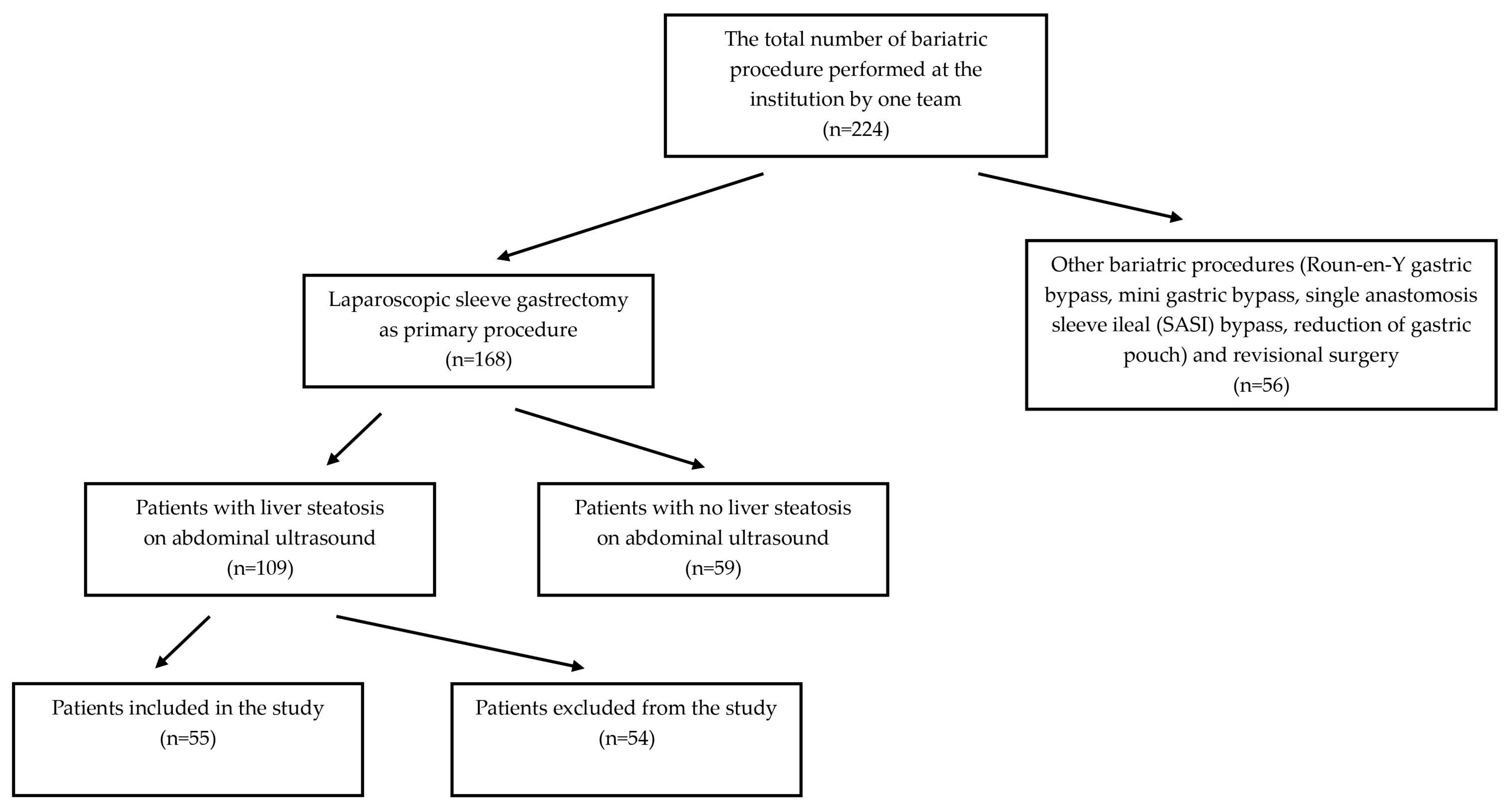
2. Materials and Methods
- -
- Percent total weight loss: %TWL = (initial weight-current weight)/(initial weight) × 100;
- -
- Percent excess BMI loss: %EBMIL = (initial BMI-postoperative BMI)/(initial BMI-25) × 100;
- -
- Percent excess weight loss: %EWL = (initial weight-postoperative weight)/(initial weight-ideal weight) × 100, where ideal weight is defined by the weight corresponding to a BMI of 25 kg/m2.
- Score 0 (absent)—normal echotexture of the liver;
- Score 1 (mild)—a slight and diffuse increase in liver echogenicity with normal visualization of the diaphragm and of the portal vein wall;
- Score 2 (moderate)—a moderate increase in liver echogenicity with slightly impaired appearance of the portal vein wall and the diaphragm;
- Score 3 (severe)—marked increase in liver echogenicity with poor or no visualization of portal vein wall, diaphragm and posterior part of the right liver lobe.
2.1. Surgical Technique
2.2. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chauhan, M.; Singh, K.; Thuluvath, P.J. Bariatric Surgery in NAFLD. Dig. Dis. Sci. 2022, 67, 408–422. [Google Scholar] [CrossRef] [PubMed]
- Fazel, Y.; Koenig, A.B.; Sayiner, M.; Goodman, Z.D.; Younossi, Z.M. Epidemiology and natural history of nonalcoholic fatty liver disease. Metabolism 2016, 65, 1017–1025. [Google Scholar] [CrossRef] [Green Version]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, M.E.; Cusi, K.; Charlton, M.; Sanyal, J.A. The diagnosis and management of non-alcoholic fatty liver disease: Practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology. Gastroenterology 2012, 142, 1592–1609. [Google Scholar]
- Younossi, Z.; Stepanova, M.; Ong, J.P.; Jacobson, I.M.; Bugianesi, E.; Duseja, A.; Eguchi, Y.; Wong, V.W.; Negro, F.; Yilmaz, Y.; et al. Nonalcoholic steatohepatitis is the fastest growing cause of hepatocellular carcinoma in liver transplant candidates. Clin. Gastroenterol. Hepatol. 2019, 17, 748–755.e3. [Google Scholar] [CrossRef] [Green Version]
- Kwong, A.; Kim, W.R.; Lake, J.R.; Smith, J.M.; Schladt, D.P.; Skeans, M.A.; Noreen, S.M.; Foutz, J.; Miller, E.; Snyder, J.J.; et al. OPTN/SRTR 2018 annual data report: Liver. Am. J. Transpl. 2020, 20, 193–299. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology 2012, 55, 2005–2023. [Google Scholar] [CrossRef]
- Vilar-Gomez, E.; Martinez-Perez, Y.; Calzadilla-Bertot, L.; Torres-Gonzalez, A.; Gra-Oramas, B.; Gonzalez-Fabian, L.; Friedman, S.L.; Diago, M.; Romero-Gomez, M. Weight loss through lifestyle modification significantly reduces features of nonalcoholic steatohepatitis. Gastroenterology 2015, 149, 367–378.e15. [Google Scholar] [CrossRef] [PubMed]
- Diemieszczyk, I.; Woźniewska, P.; Gołaszewski, P.; Drygalski, K.; Nadolny, K.; Ładny, J.R.; Hady, H.R. Does weight loss after laparoscopic sleeve gastrectomy contribute to reduction in blood pressure? Pol. Arch. Intern. Med. 2021, 131, 693–700. [Google Scholar] [CrossRef]
- Doumouras, A.G.; Wong, J.A.; Paterson, J.M.; Lee, Y.; Sivapathasundaram, B.; Tarride, J.E.; Thabane, L.; Hong, D.; Yusuf, S.; Anvari, M. Bariatric Surgery and Cardiovascular Outcomes in Patients with Obesity and Cardiovascular Disease: A Population-Based Retrospective Cohort Study. Circulation 2021, 143, 1468–1480. [Google Scholar] [CrossRef]
- Welbourn, R.; Hollyman, M.; Kinsman, R.; Dixon, J.; Liem, R.; Ottosson, J.; Ramos, A.; Våge, V.; Al-Sabah, S.; Brown, W.; et al. Bariatric Surgery Worldwide: Baseline Demographic Description and One-Year Outcomes from the Fourth IFSO Global Registry Report 2018. Obes. Surg. 2019, 29, 782–795. [Google Scholar]
- Ali, M.; Khan, S.A.; Mushtaq, M.; Haider, S.A. Comparison of Laparoscopic Sleeve Gastrectomy (LSG) with Laparoscopic Gastric Bypass (LRYGB) in Bariatric Surgery. Cureus 2021, 13, e14022. [Google Scholar] [CrossRef]
- Wang, Y.; Guo, X.; Lu, X.; Mattar, S.; Kassab, G. Mechanisms of Weight Loss After Sleeve Gastrectomy and Adjustable Gastric Banding: Far More Than Just Restriction. Obesity 2019, 27, 1776–1783. [Google Scholar] [CrossRef]
- Budzyński, A.; Major, P. Polskie rekomendacje w zakresie chirurgii bariatrycznej i metabolicznej. Med. Prakt.–Chir. 2016, 6, 13–25. [Google Scholar]
- Schmitz, S.M.; Kroh, A.; Ulmer, T.F.; Andruszkow, J.; Luedde, T.; Brozat, J.F.; Neumann, U.P.; Alizai, P.H. Evaluation of NAFLD and fibrosis in obese patients—A comparison of histological and clinical scoring systems. BMC Gastroenterol. 2020, 20, 254. [Google Scholar] [CrossRef]
- Głuszyńska, P.; Lemancewicz, D.; Dzięcioł, J.B.; Razak Hady, H. Non-Alcoholic Fatty Liver Disease (NAFLD) and Bariatric/Metabolic Surgery as Its Treatment Option: A Review. J. Clin. Med. 2021, 10, 5721. [Google Scholar] [CrossRef] [PubMed]
- Kargulewicz, A.; Stankowiak-Kulpa, H.; Grzymisławski, M. Dietary recommendations for patients with nonalcoholic fatty liver disease. Prz. Gastroenterol. 2014, 9, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Murshid, K.R.; Alsisi, G.H.; Almansouri, F.A.; Zahid, M.M.; Boghdadi, A.A.; Mahmoud, E.H. Laparoscopic sleeve gastrectomy for weight loss and treatment of type 2 diabetes mellitus. J. Taibah Univ. Med. Sci. 2021, 16, 387–394. [Google Scholar] [CrossRef]
- Diamantis, T.; Apostolou, K.G.; Alexandrou, A.; Griniatsos, J.; Felekouras, E.; Tsigris, C. Review of long-term weight loss results after laparoscopic sleeve gastrectomy. Surg. Obes. Relat. Dis. 2014, 10, 177–183. [Google Scholar] [CrossRef]
- Hirth, D.A.; Jones, E.L.; Rothchild, K.B.; Mitchell, B.C.; Schoen, J.A. Laparoscopic sleeve gastrectomy: Long-term weight loss outcomes. Surg. Obes. Relat. Dis. 2015, 11, 1004–1007. [Google Scholar] [CrossRef]
- Kraljević, M.; Cordasco, V.; Schneider, R.; Peters, T.; Slawik, M.; Wölnerhanssen, B.; Peterli, R. Long-term Effects of Laparoscopic Sleeve Gastrectomy: What Are the Results Beyond 10 Years? Obes. Surg. 2021, 31, 3427–3433. [Google Scholar] [CrossRef]
- Algooneh, A.; Almazeedi, S.; Al-Sabah, S.; Ahmed, M.; Othman, F. Non-alcoholic fatty liver disease resolution following sleeve gastrectomy. Surg. Endosc. 2016, 30, 1983–1987. [Google Scholar] [CrossRef] [PubMed]
- Mattar, S.G.; Velcu, L.M.; Rabinovitz, M.; Demetris, A.J.; Krasinskas, A.M.; Barinas-Mitchell, E.; Eid, G.M.; Ramanathan, R.; Taylor, D.S.; Schauer, P.R. Surgically-induced weight loss significantly improves nonalcoholic fatty liver disease and the metabolic syndrome. Ann. Surg. 2005, 242, 610–617. [Google Scholar] [CrossRef]
- Fakhry, T.K.; Mhaskar, R.; Schwitalla, T.; Muradova, E.; Gonzalvo, J.P.; Murr, M.M. Bariatric surgery improves nonalcoholic fatty liver disease: A contemporary systematic review and meta-analysis. Surg. Obes. Relat. Dis. 2019, 15, 502–511. [Google Scholar] [CrossRef]
- Bower, G.; Toma, T.; Harling, L.; Jiao, L.R.; Efthimiou, E.; Darzi, A.; Athanasiou, T.; Ashrafian, H. Bariatric Surgery and Non-Alcoholic Fatty Liver Dis-ease: A Systematic Review of Liver Biochemistry and Histology. Obes. Surg. 2015, 25, 2280–2289. [Google Scholar] [CrossRef]
- Lee, Y.; Doumouras, A.G.; Yu, J.; Brar, K.; Banfield, L.; Gmora, S.; Anvari, M.; Hong, D. Complete Resolution of Nonalcoholic Fatty Liver Disease After Bariatric Surgery: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2019, 17, 1040–1060.e11. [Google Scholar] [CrossRef] [Green Version]
- Moretto, M.; Kupski, C.; da Silva, V.D.; Padoin, A.V.; Mottin, C.C. Effect of bariatric surgery on liver fibrosis. Obes. Surg. 2012, 22, 1044–1049. [Google Scholar] [CrossRef] [PubMed]
- Gasteyger, C.; Larsen, T.M.; Vercruysse, F.; Astrup, A. Effect of a dietary-induced weight loss on liver enzymes in obese subjects. Am. J. Clin. Nutr. 2008, 87, 1141–1147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathurin, P.; Hollebecque, A.; Arnalsteen, L.; Buob, D.; Leteurtre, E.; Caiazzo, R.; Pigeyre, M.; Verkindt, H.; Dharancy, S.; Louvet, A.; et al. Prospective study of the long-term effects of bariatric surgery on liver injury in patients without advanced disease. Gastroenterology 2009, 137, 532–540. [Google Scholar] [CrossRef] [PubMed]
- Mottin, C.C.; Moretto, M.; Padoin, A.V.; Kupski, C.; Swarowsky, A.M.; Glock, L.; Duval, V.; Braga da Silva, J. Histological behavior of hepatic steatosis in morbidly obese patients after weight loss induced by bariatric surgery. Obes. Surg. 2005, 15, 788–793. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Tovar, J.; Alsina, M.E.; Alpera, M.R.; OBELCHE Group. Improvement of nonalcoholic fatty liver disease in morbidly obese patients after sleeve gastrectomy: Association of ultrasonographic findings with lipid profile and liver enzymes. Acta Chir. Belg. 2017, 117, 363–369. [Google Scholar] [CrossRef]
- Elyasinia, F.; Jalali, S.M.; Zarini, S.; Sadeghian, E.; Sorush, A.; Pirouz, A. The Effect of Laparoscopic Sleeve Gastrectomy and Gastric Bypass Surgery on Non-Alcoholic Steatohepatitis in Iranian Patients with Obesity. Middle East J. Dig. Dis. 2021, 13, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, K.; Paull-Forney, B.; Okut, H.; Schwasinger-Schmidt, T. Bariatric Metabolic Surgery Reduced Liver Enzyme Levels in Patients with Non-Alcohol Fatty Liver Disease. Kans. J. Med. 2021, 14, 209–214. [Google Scholar] [CrossRef]
- Groth, D.; Woźniewska, P.; Olszewska, M.; Zabielski, P.; Ładny, J.R.; Dadan, J.; Zalewska, A.; Błachnio-Zabielska, A.; Diemieszczyk, I.; Krętowski, A.; et al. Gender-related metabolic outcomes of laparoscopic sleeve gastrectomy in 6-month follow-up. Wideochir. Inne Tech. Maloinwazyjne 2020, 15, 148–156. [Google Scholar] [CrossRef]
- Lee, H.; Shin, D.W.; Lee, T.H.; Yang, H.K.; Ahn, E.; Yoon, J.M.; Lee, H.K.; Suh, B.; Son, K.Y.; Kim, J.S.; et al. Association Between Change in Serum Aminotransferase and Mortality: A Nationwide Cohort Study in Korea. Medicine 2016, 95, e3158. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, T.M.; Alves-Júnior, A.; Nunes, M.A.; de Freitas, T.R.; da Silva, M.A.; Alves, M.R. Comparison of hepatic profile in pre and postoperative of bariatric surgery: Private vs. public network. Arq. Bras. Cir. Dig. 2015, 28, 274–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, A.; Nguyen, M.; Ju, I.; Brancatisano, A.; Ryan, B.; van der Poorten, D. Utility of Fibroscan XL to assess the severity of non-alcoholic fatty liver disease in patients undergoing bariatric surgery. Sci. Rep. 2021, 11, 14006. [Google Scholar] [CrossRef] [PubMed]
- Sandvik, E.C.S.; Aasarød, K.M.; Johnsen, G.; Hoff, D.A.L.; Kulseng, B.; Hyldmo, Å.A.; Græslie, H.; Nymo, S.; Sandvik, J.; Fossmark, R. The Effect of Roux-en-Y Gastric Bypass on Non-Alcoholic Fatty Liver Disease Fibrosis Assessed by FIB-4 and NFS Scores-An 11.6-Year Follow-Up Study. J. Clin. Med. 2022, 11, 4910. [Google Scholar] [CrossRef] [PubMed]
- Salman, M.A.; Mikhail, H.M.S.; Nafea, M.A.; Sultan, A.A.E.A.; Elshafey, H.E.; Tourky, M.; Awad, A.; Abouelregal, T.E.; Ahmed, R.A.; Ashoush, O.; et al. Impact of laparoscopic sleeve gastrectomy on fibrosis stage in patients with child-A NASH-related cirrhosis. Surg. Endosc. 2021, 35, 1269–1277. [Google Scholar] [CrossRef] [PubMed]
- Murakami, E.; Nakahara, T.; Hiramatsu, A.; Morio, K.; Fujino, H.; Yamauchi, M.; Kawaoka, T.; Tsuge, M.; Imamura, M.; Aikata, H.; et al. Therapeutic effects of sleeve gastrectomy for non-alcoholic steatohepatitis estimated by paired liver biopsy in morbidly obese Japanese patients. Medicine 2021, 100, e26436. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Follow Up | 0 | 6 Months | 12 Months | |
|---|---|---|---|---|
| Liver Steatosis Status | ||||
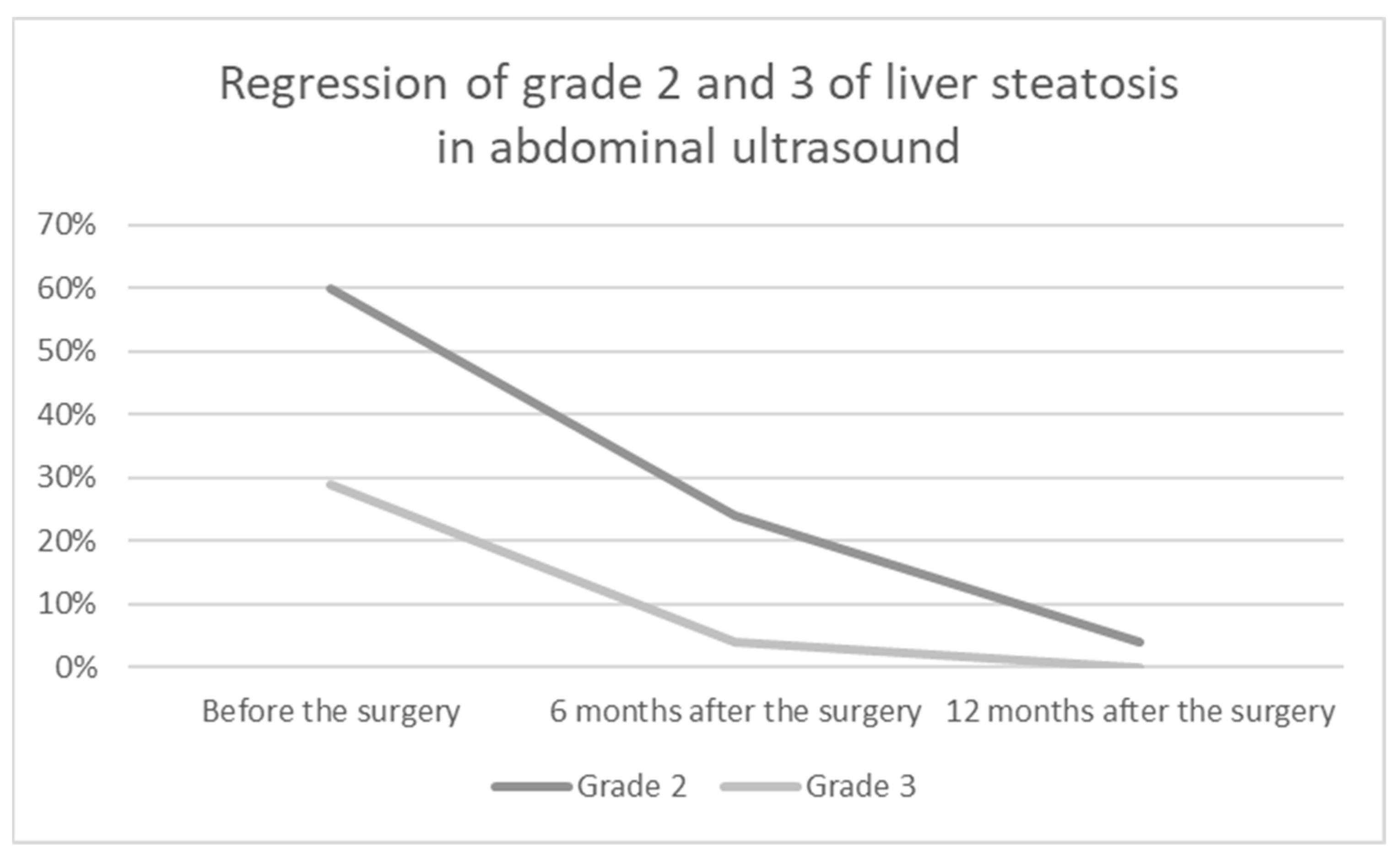
| Steatosis | Grade 0 | N/A | 20 (37%) | 34 (62%) |
| Grade 1 | 6 (11%) | 20 (37%) | 19 (35%) | |
| Grade 2 | 33 (60%) | 13 (24%) | 2 (4%) | |
| Grade 3 | 16 (29%) | 2 (4%) | 0 | |
| Partial remission | N/A | 27 (49%) | 16 (29%) | |
| Total remission | N/A | 20 (37%) | 34 (62%) | |
| Variables | 0 | 6 Months | 12 Months | p-Value |
|---|---|---|---|---|
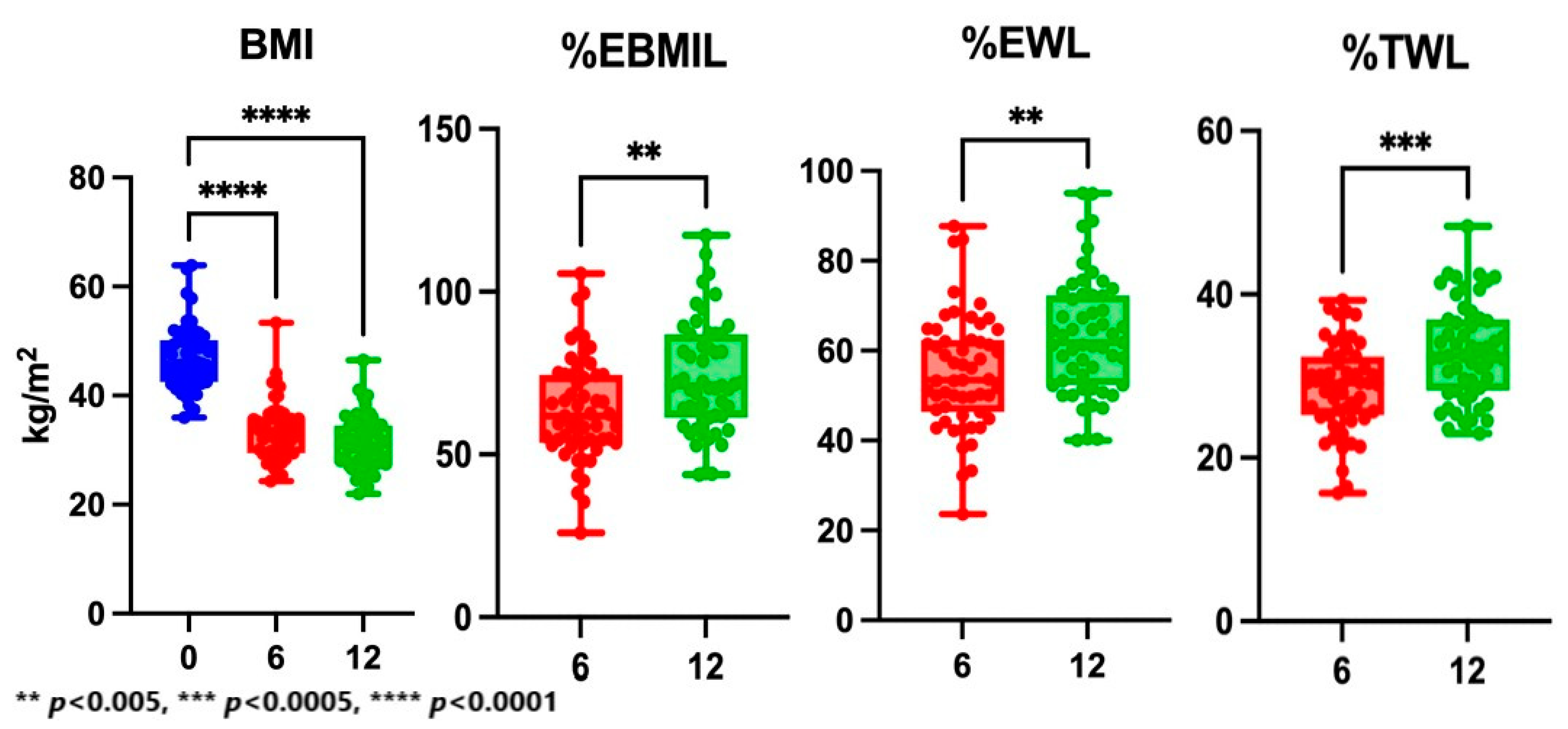
| BMI (kg/m2) | 45.6 (42.5–50.2) | 33.5 (29.4–35.8) | 31.0 (27.5–34.5) | <0.0001 |
| %TWL | N/A | 29.2 (25.2–32.4) | 32.5 (28.2–36.9) | 0.0003 |
| %EWL | N/A | 53.5 (46.3–62.4) | 61.8 (52.4–72.3) | 0.0013 |
| %EBMIL | N/A | 61.8 (53.6–74.4) | 71.0 (61.3–86.9) | 0.0036 |
| Variables | 0 | 6 Months | 12 Months | p-Value |
|---|---|---|---|---|
| ALB (g/dL) | 3.8 (3.7–3.9) | 4.0 (3.9–4.2) | 4.0 (3.9–4.1) | <0.0001 |
| PLT (×109/L) | 234.0 (20.5–274.0) | 218.0 (190.0–276.0) | 233.0 (200.0–268.0) | 0.5600 |
| FPG (mg/dL) | 110.0 (94.0–130.0) | 94.0 (89.0–99.0) | 89.0 (83.0–96.0) | <0.0001 |
| Bilirubin (mg/dL) | 0.6 (0.4–0.7) | 0.8(0.5–0.9) | 0.9 (0.6–1.1) | 0.0002 |
| GGT (IU/L) | 28.5 (21.6–56.5) | 18.0 (12.5–27.0) | 18.0 (13.7–35.0) | 0.0003 |
| LDH (IU/L) | 235.0 (186.0–271.0) | 179.0 (154.0–203.0) | 176.0 (152.0–184.0) | <0.0001 |
| ALT (IU/L) | 41.1 (21.0–53.9) | 21.0 (14.7–26.0) | 19.0 (16.0–24.0) | <0.0001 |
| AST (IU/L) | 25.5 (19.0–37.0) | 18.1 (14.0–24.0) | 20.0 (17.0–26.0) | 0.0002 |
| Total cholesterol (mg/dL) | 178.0 (148.0–193.0) | 178.0 (144.0–201.0) | 180.0 (153.0–180.0) | 0.8285 |
| LDL (mg/dL) | 114.4 (96.3–129.0) | 106.4 (82.0–133.0) | 113.5 (76.0–132.6) | 0.6769 |
| HDL (mg/dL) | 45.8 (37.1–50.4) | 47.5 (39.8–57.6) | 54.0 (46.8–65.0) | <0.0001 |
| TG (mg/dL) | 156.1 (112.0–215.0) | 109.0 (76.0–139.0) | 86.0 (61.0–134.0) | <0.0001 |
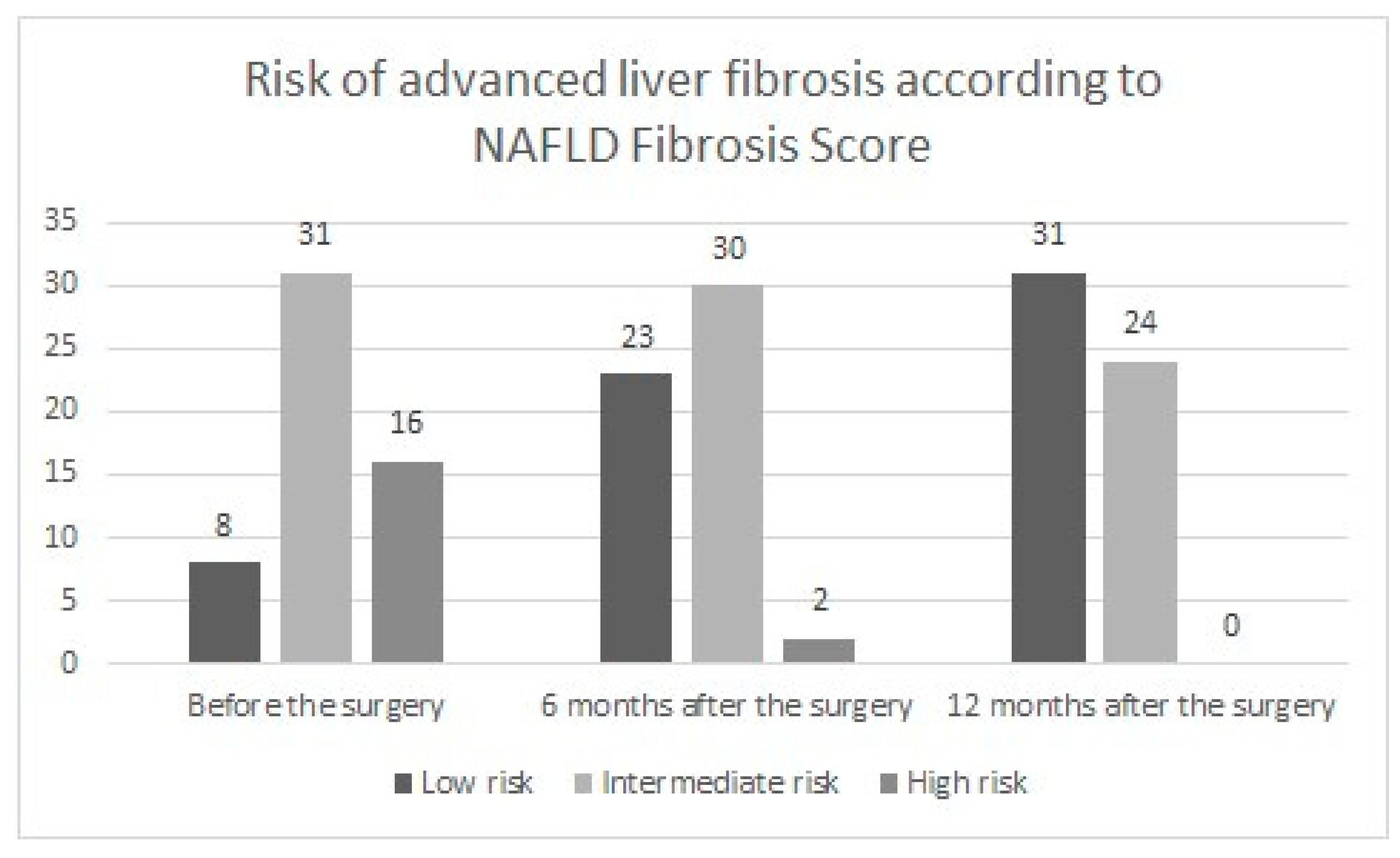
| NAFLD Fibrosis Score | 0.2 (−0.8–1.0) | −1.1 (−2.3–−0.2) | −1.6 (−2.4–−0.4) | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Głuszyńska, P.; Łukaszewicz, A.; Diemieszczyk, I.; Chilmończyk, J.; Reszeć, J.; Citko, A.; Szczerbiński, Ł.; Krętowski, A.; Razak Hady, H. The Effect of Laparoscopic Sleeve Gastrectomy on the Course of Non-Alcoholic Fatty Liver Disease in Morbidly Obese Patients during One Year of Follow Up. J. Clin. Med. 2023, 12, 4122. https://doi.org/10.3390/jcm12124122
Głuszyńska P, Łukaszewicz A, Diemieszczyk I, Chilmończyk J, Reszeć J, Citko A, Szczerbiński Ł, Krętowski A, Razak Hady H. The Effect of Laparoscopic Sleeve Gastrectomy on the Course of Non-Alcoholic Fatty Liver Disease in Morbidly Obese Patients during One Year of Follow Up. Journal of Clinical Medicine. 2023; 12(12):4122. https://doi.org/10.3390/jcm12124122
Chicago/Turabian StyleGłuszyńska, Paulina, Aleksander Łukaszewicz, Inna Diemieszczyk, Jan Chilmończyk, Joanna Reszeć, Anna Citko, Łukasz Szczerbiński, Adam Krętowski, and Hady Razak Hady. 2023. "The Effect of Laparoscopic Sleeve Gastrectomy on the Course of Non-Alcoholic Fatty Liver Disease in Morbidly Obese Patients during One Year of Follow Up" Journal of Clinical Medicine 12, no. 12: 4122. https://doi.org/10.3390/jcm12124122