
The Biology of Placebo and Nocebo Effects on Experimental and Chronic Pain: State of the Art

 , , ,
, , ,
Abstract
:1. Introduction
2. State of the Art
2.1. Experimental Approaches to Study Placebo and Nocebo Effects
2.2. Neurobiology
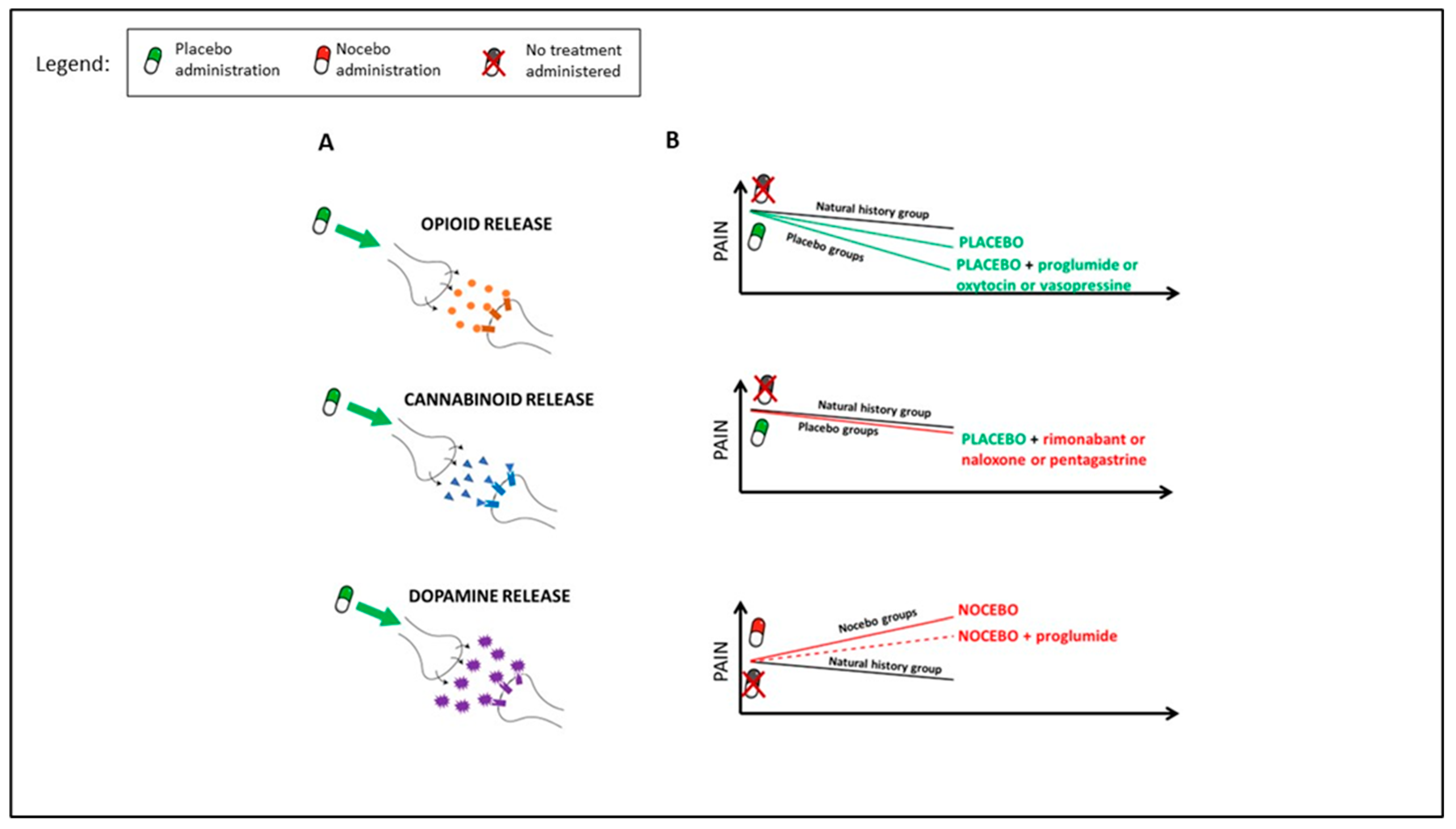
2.2.1. Pharmacological Evidence
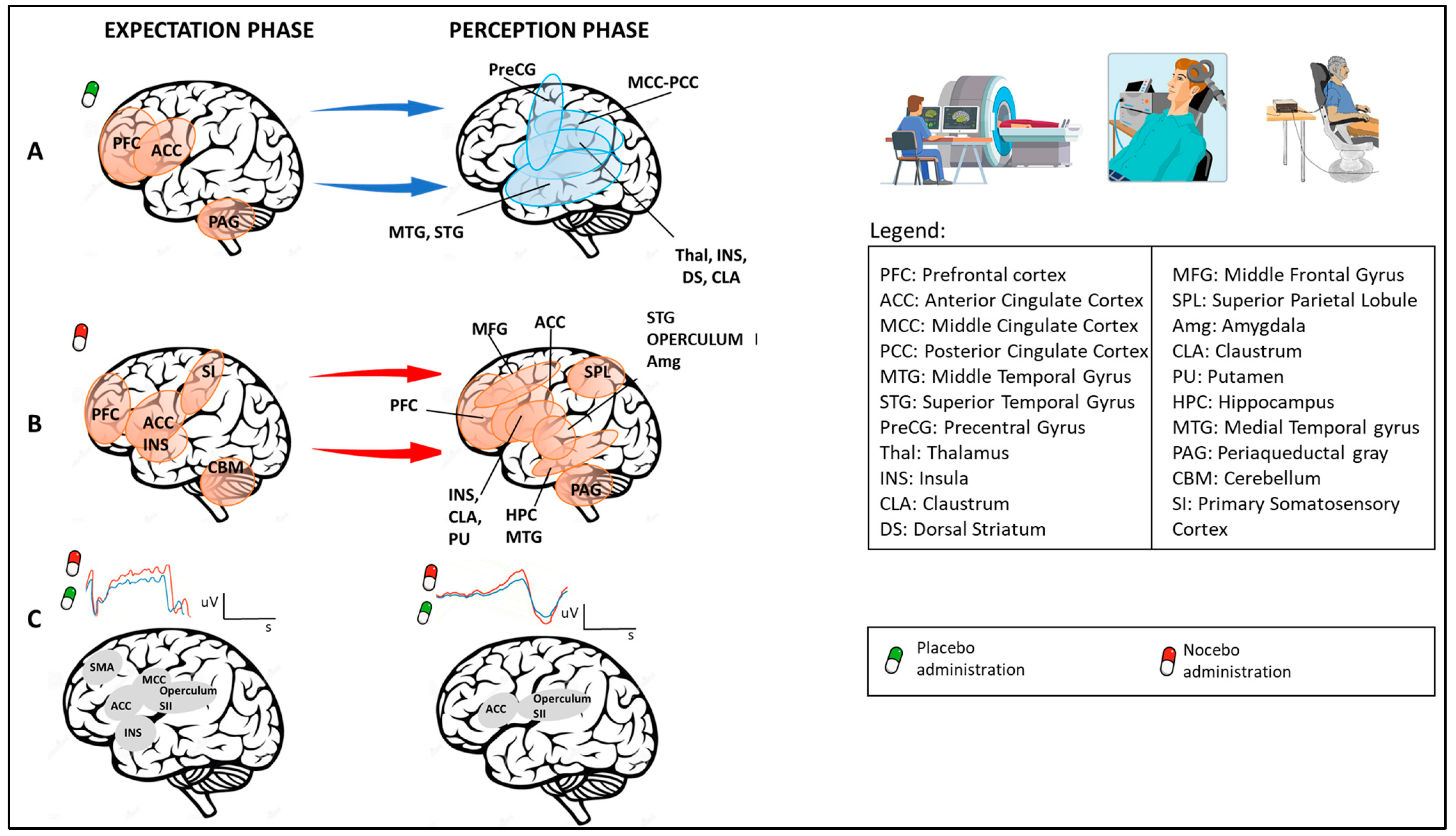
2.2.2. Neuroimaging Studies
Temporal Aspects
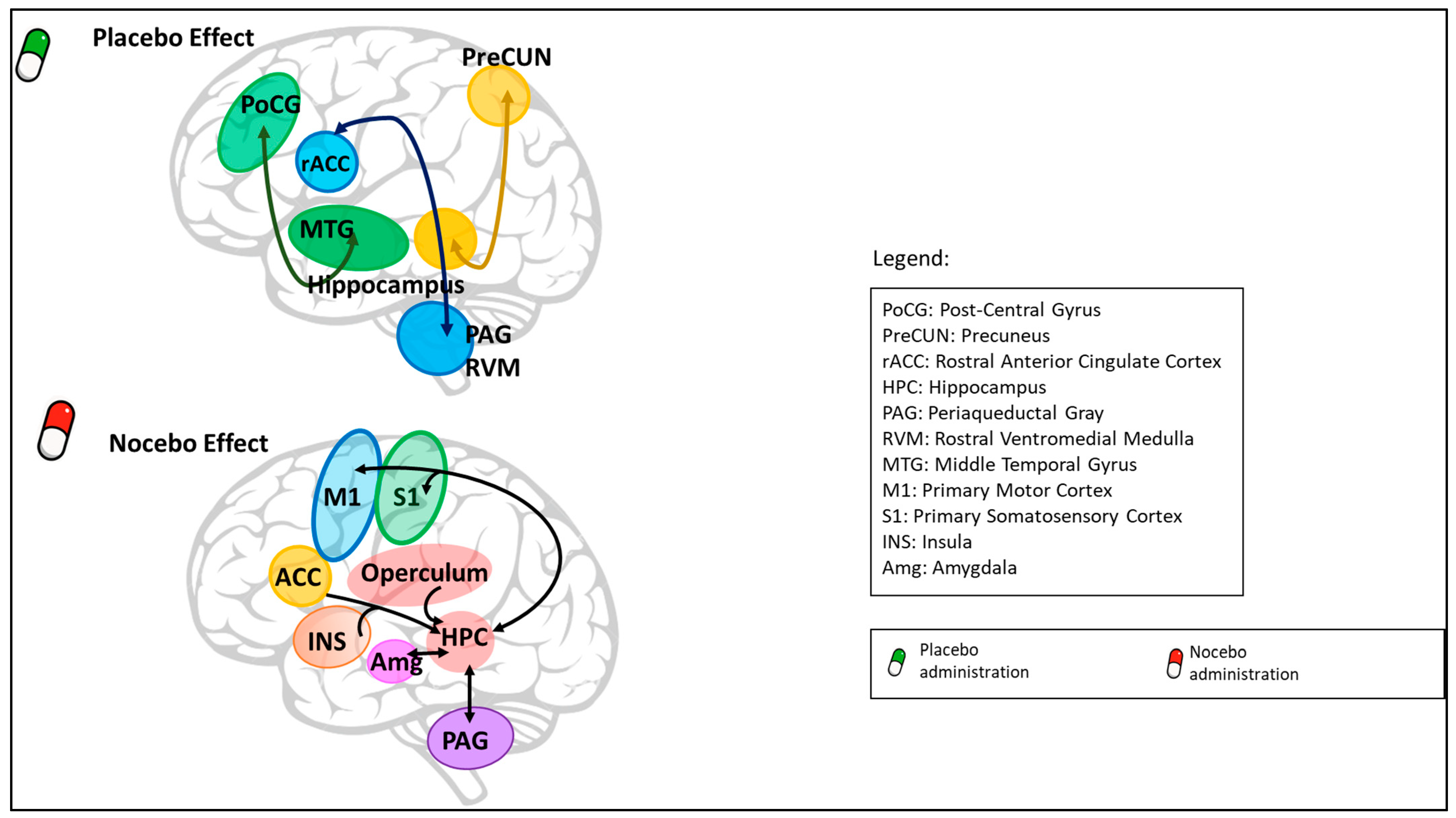
Central Nervous System
- High Central Nervous System Levels
- Low Central Nervous System Levels
2.3. Genetics
2.4. Placebo and Nocebo Effects in Chronic Pain
3. Future Directions for Clinical Practice
4. Future Directions for Research and Clinical Trials
5. Conclusions and Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| RCT | Randomized Controlled Trial |
| fMRI | functional Magnetic Resonance Imaging |
| PET | Positron Emission Tomography |
| EEG | electroencephalography |
| VAS | Visual Analogue Scale |
| NRS | Numerical Rating Scale |
| CI | Confidence Interval |
| rTMS | repetitive Transcranial Magnetic Stimulation |
| ROI | Regions of Interest |
| M | Male |
| F | Female |
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Paper ID | Sample Size (M, F, Not Analysed) * | Population Type | Pain Type/Pain Induction | Investigated Outcome | Outcome Measure | Level of Significance |
|---|---|---|---|---|---|---|
| Amanzio and Benedetti, 1999 [20] | 229 (132, 97) | Healthy subjects | Experimental ischemic pain | Behavioral (Pharmacological) | Pain tolerance (min) | p < 0.05 |
| Amanzio et al., 2001 [21] | 364 (278 patients; 86 healthy controls) | Patients (thoracic surgery) and healthy controls | Postoperative pain; experimental ischemic arm pain | Behavioral (Pharmacological) | NRS (0–10) | p < 0.05 |
| Benedetti et al., 1995 [40] | 93 (52, 41) | Patients (thoracotomy for lung surgery) | Post-surgery pain | Behavioral (Pharmacological) | NRS (0–10) | p < 0.02 |
| Benedetti et al., 1996 [39] | 340 (154, 186) | Healthy subjects | Experimental ischemic pain | Behavioral (Pharmacological) | NRS (0–10) | p < 0.05 |
| Benedetti et al., 1997 [38] | 180 (119, 61) | Patients (video-assisted thoracoscopy) | Post-surgery pain | Behavioral (Pharmacological) | NRS (0–10) | p < 0.05 |
| Benedetti et al., 2006 [42] | 49 (23, 26) | Healthy subjects | Experimental ischemic pain | Behavioral (Pharmacological) | NRS (0–10) | p < 0.05 |
| Benedetti et al., 2006 [86] | 44 (28 patients (11, 17), 16 controls) | Patients (Alzheimer’s disease) and healthy subjects | Burning pain after venipuncture | Electrophysiological (EEG) | NRS (0–10) | p < 0.05 |
| Benedetti et al., 2010 [41] | 40 (20, 20) | Healthy subjects | Experimental ischemic pain | Behavioral (Pharmacological) | Tolerance time | p < 0.05 |
| Benedetti et al., 2011 [36] | 82 (41, 41) | Healthy subjects | Experimental ischemic pain | Behavioral (Pharmacological) | Tolerance time | 95%CI |
| Benedetti et al., 2014 [54] | 74 (30, 44) | Healthy subjects | Hypobaric hypoxia headache | Behavioral (Pharmacological) | NRS (0–10) | 95%CI |
| Benedetti et al., 2022 [37] | 149 (82, 67) | Healthy subjects | Experimental ischemic pain | Behavioral (Pharmacological) | 0–10 rating scale | p < 0.05 |
| Bingel et al. 2011 [85] | 22 (15, 7) | Healthy subjects | Heat pain | Neuroimaging (fMRI) | VAS (0–100) | p < 0.05 |
| Bingel et al., 2022 [100] | 22 (15, 7) | Healthy subjects | Heat pain | Neuroimaging; functional connectivity (fMRI) | VAS (0–100) | p < 0.05 |
| Bush et al., 2021 [95] | 37 (12, 25) | Healthy subjects | Heat pain | Neuroimaging; functional connectivity (fMRI) | VAS (0–100) | p < 0.05 |
| Camerone et al., 2021 [16] | 166 (78, 88, 9) | Healthy subjects | Electrical stimuli | Behavioral | NRS (0–10) | p < 0.05 |
| Camerone et al., 2021 [17] | 77 (24, 24, 29) | Healthy subjects | Cold pressor test (CPT) | Behavioral | Numerical Pain Intensity (0–100) | p < 0.05 |
| Camerone et al., 2022 [18] | 51 (24, 27, 10) | Healthy subjects | Cold pressor test (CPT) | Behavioral | NRS (0–10) | p < 0.05 |
| Carlino et al., 2015 [73] | 34 (20, 14) | Healthy subjects | Laser stimulation | Electrophysiology (EEG) | NRS (0–10) | p < 0.05 |
| Carlino et al., 2016 [26] | 80 (34, 46) | Healthy subjects | Electrical stimuli | Behavioral | NRS (0–10) | p < 0.05 |
| Colloca et al., 2006 [24] | 30 (5, 25) | Healthy subjects | Electrical stimuli | Behavioral | NRS (0–10) | p < 0.05 |
| Colloca et al., 2008 [21] | 116 (0, 116) | Healthy subjects | Electrical stimuli | Behavioral | NRS (0–10) | p < 0.05 |
| Colloca et al., 2010 [25] | 46 (16, 30) | Healthy subjects | Electrical stimuli | Behavioral | VAS (0–10 | p < 0.05 |
| Colloca et al., 2016 [50] | 109 (55, 54, 1) | Healthy subjects | Electrical stimuli | Behavioral | VAS (0–10) | p < 0.05 |
| Colloca et al., 2019 [105] | 160 (58, 102) | Healthy subjects | Electrical and heat stimuli | DNA genotyping; epistasis | VAS (0–10) | p < 0.001 |
| Colloca et al., 2020 [121] | 763 (363 patients (85, 278); 400 healthy controls (162; 238) | Patients (chronic orofacial pain) and healthy subjects | Heat stimuli | Behavioral | VAS | p < 0.05 |
| Disley et al., 2021 [30] | 104 (10, 65, 29) | Healthy subjects | Cold pressor test (CPT) | Behavioral | VAS (0–100) | p = 0.05 |
| Eippert et al., 2009 [34] | 48 (48, -, 8) | Healthy subjects | Heat pain | Neuroimaging (fMRI) | VAS (0–100) | p ≤ 0.05 |
| Eippert et al., 2009 [92] | 15 (15, 0) | Healthy subjects | Heat pain | Neuroimaging (fMRI) | VAS (0–100) | p < 0.05 |
| Ellerbrock et al., 2015 [35] | 40 (20, 20, 1) | Healthy subjects | Heat pain | Neuroimaging; functional connectivity (fMRI) | VAS (0–100) | p < 0.05 |
| Fuentes et al., 2014 [164] | 117 | Patients (chronic low back pain) | - | Behavioral | NRS (0–10) | p < 0.05 |
| Hashmi et al., 2014 [91] | 42 | Patients (chronic knee osteoarthritis) | Heat pain | Neuroimaging (fMRI) | Gracely Sensory Scale (0–20) | p < 0.05 |
| Jarcho et al., 2016 [46] | 15 (0, 15) | Healthy subjects | Heat pain | Neuroimaging (PET; fMRI) | VAS (0–100) | p < 0.005 |
| Kaptchuk et al., 2008 [111] | 262 (63, 199) | Patients (irritable bowel syndrome) | - | Behavioral | Global improvement scale (range 1–7); adequate relief of symptoms; symptom severity | p < 0.01 |
| Kelley et al., 2009 [165] | 189 | Patients (irritable bowel syndrome) | - | Behavioral | Combined outcome (IBS Symptom Severity Scale; IBS Quality of Like Scale; IBS Global Improvement Scale; IBS Adequate Relief) | p < 0.05 |
| Kessner et al., 2013 [51] | 80 (80, 0) | Healthy subjects | Heat pain | Behavioral (Pharmacological) | Visual Analogue Scale (0–100) | p < 0.05 |
| Klinger et al., 2017 [112] | 48 (12, 36) | Patients (chronic back pain) | Electrical stimuli | Behavioral | NRS (0–10) | 95% CI |
| Kong et al., 2006 [57] | 24 (13, 11) | Healthy subjects | Heat pain | Neuroimaging (fMRI) | 0–20 Sensory Box Scale | p < 0.0001 for ROI p = 0.05 |
| Kong et al., 2008 [71] | 20 (5, 8, 7) | Healthy subjects | Heat pain | Neuroimaging (fMRI) | Gracely Sensory and Affective Scales | p < 0.05 |
| Koyama et al., 2005 [70] | 10 (8, 2) | Healthy subjects | Heat pain | Neuroimaging (fMRI) | VAS | p < 0.01 |
| Krummenacher et al., 2010 [87] | 40 (40, 0) | Healthy subjects | Heat pain | rTMS | VAS (0–10) | p ≤ 0.05 |
| Kube et al., 2020 [29] | 117 (48, 53, 16) | Healthy subjects | Heat pain | Behavioral | Pain tolerance | p < 0.05 |
| Lieberman et al., 2004 [58] | 52 (29 active drug; 23 placebo condition) | Patients (irritable bowel syndrome) | - | Neuroimaging (PET) | Symptom diary (4 weeks) | p < 0.005 |
| Malfiet et al., 2019 [79] | 83 | Patients (chronic neck pain) | - | Behavioral | VAS (0–100) | p = 0.05 |
| Martins et al., 2022 [125] | 56 | Patients (chronic knee osteoarthritis) | - | Neuroimaging; functional connectivity (fMRI) | VAS (0–10) | p < 0.05 |
| Morton et al., 2010 [74] | 67 (21, 35, 11) | Healthy subjects | Laser stimulation | Electrophysiological (EEG) | 0–10 scale | p = 0.05 |
| Müller et al., 2016 [118] | 50 (27, 32, 1) | Patients (chronic pain) | Pressure-pain stimuli | Behavioral | VAS (0–100) | p < 0.05 |
| Olson et al., 2021 [113] | 280 (65, 215) | Patients (chronic orofacial pain) | Heat pain | Behavioral | VAS (0–100) | p < 0.05 |
| Peciña et al., 2015 [106] | 50 (21, 29) | Healthy subjects | 5% hypertonic saline | DNA genotyping; Neuroimaging (PET) | VAS (0–100) | p < 0.05 |
| Petrovic et al., 2002 [60] | 9 | Healthy subjects | Heat stimuli | Neuroimaging (PET) | VAS (0–100) | p = 0.005 |
| Petrovic et al., 2010 [59] | 24 (9, 15) | Healthy subjects | Heat stimuli | Neuroimaging (PET; fMRI) | VAS (0–100) | p < 0.05 |
| Piedimonte et al., 2017 [23] | 34(16, 18, -) | Healthy subject | Electrical stimuli | Electrophysiological (EEG) | NRS (0–10) | p < 0.05 |
| Ploghaus et al., 1999 [67] | 12 (7, 5) | Healthy subjects | Heat stimuli | Neuroimaging (fMRI) | VAS (0–10) | p < 0.05 |
| Pollo et al., 2001 [81] | 38 | Patients (thoracotomized patients) | - | Behavioral | NRS (0–10) | p < 0.01 |
| Porro et al., 2002 [69] | 30 (10, 16, 4) | Healthy subjects | Acid solution injection | Neuroimaging (fMRI) | 0–100 scale rating | p < 0.05 |
| Price et al., 1999 [162] | 40 (16, 24) | Healthy subjects | Heat pain | Behavioral | VAS (0–10) | p < 0.05 |
| Price et al., 2007 [61] | 9 | Patients (irritable bowel syndrome) | Barostat balloon distension—pressure stimuli | Neuroimaging (fMRI) | 100-unit rating scale | p < 0.05 |
| Prossin et al., 2022 [55] | 37 (12, 25) | Healthy subjects | Hypertonic saline injection | Neuroimaging (PET, MRI) | VAS (0–100) | p < 0.05 |
| Rief et al., 2012 [168] | 144 (50, 904) | Healthy participants | Heat pain | Behavioral | Pain threshold change in °C | p < 0.05 |
| Ruscheweyh et al., 2014 [98] | 60 (30 patients, 30 controls) | Patients (cerebellum infarction) and healthy subjects | Heat; pressure; pinprick pain | Behavioral | NRS (0–10) | p < 0.05 |
| Sawamoto et al., 2000 [83] | 10 (10, 0) | Healthy subjects | Laser thermal stimulation | Neuroimaging (fMRI) | 0–100 scale | p < 0.05 |
| Schmid et al., 2015 [84] | 44 (22, 22) | Healthy subjects | Rectal distension | Neuroimaging (fMRI) | VAS (0–100) | p < 0.05 |
| Schwartz et al., 2022 [161] | 44 (18, 26) | Patients (chronic low back pain) | - | Behavioral | NRS (0–10) | p < 0.05 |
| Scott et al., 2007 [49] | 48 (30 Study1; 16 Study2; 18 Male controls) | Healthy subjects | 5% hypertonic saline injection | Neuroimaging (Study1—PET, fMRI Study2—fMRI) | VAS (0–100) | p < 0.05 |
| Scott et al., 2008 [43] | 20 (9, 11); 18 (18, 0) | Healthy subjects | Sustained muscle pain challenge | Neuroimaging (PET, MRI) | VAS (0–100) | p < 0.0001 for ROI p = 0.05 |
| Skyt et al., 2018 [47] | 19 (10, 9) | Patients (neuropathic pain) | Pinprick-evoked pain; wind-up-like pain | Behavioral | VAS (0–10; 0–100) | p < 0.05 |
| Tétreault et al., 2016 [89] | 98 (17 Study1; 39 Study2; 42 Study3) | Patients (chronic knee osteoarthritis pain) | - | Neuroimaging (fMRI) | VAS (0–10); Western Ontario and McMaster Universities Osteoarthritis Index | p < 0.05 |
| Tinnermann et al., 2017 [99] | 57 (27, 22, 8) | Healthy subjects | Heat stimuli | Neuroimaging (fMRI) | VAS (0–100) | p < 0.05 |
| Tu et al., 2021 [88] | 81 (44, 37) | Healthy subjects | Heat stimuli | Neuroimaging (fMRI); tDCS | Gracely Sensory Scale (0–20) | p < 0.05 |
| Vachon-Presseau et al., 2018 [90] | 129 (43 placebo group, 20 controls, 66 excluded) | Patients (chronic back pain) | Back pain intensity | Neuroimaging (MRI, fMRI) | VAS (0–10) | p < 0.05 |
| Vachon-Presseau et al., 2022 [144] | 181 (94 randomized to 3 arms, 87 excluded) | Patients (chronic low back pain) | Back pain intensity | Neuroimaging (fMRI) | Likert Scale (twice a day) | p < 0.05 |
| Van der Meulen et al., 2017 [72] | 30 (13, 17) | Healthy subjects | Heat stimuli | Neuroimaging (fMRI) | VAS (0–100) | p < 0.05 |
| Vase et al., 2003 [82] | 13 | Patients (irritable bowel syndrome) | Evoked rectal distension; heat pain | Behavioral | VAS (0–10) | p < 0.05 |
| Vase et al., 2005 [110] | 26 (0, 26) | Patients (irritable bowel syndrome) | Rectal distension | Behavioral (Pharmacological) | VAS (0–10) | p < 0.05 |
| Vecchio et al., 2021 [77] | 63 (31, 32) | Healthy subjects | Electrical stimuli | Electrophysiological (EEG) | 7 point Likert scale | p = 0.05 |
| Wager et al., 2004 [64] | 47 | Healthy subjects | Shock pain; heat pain | Neuroimaging (fMRI) | 10 point scale | p < 0.05 |
| Wager et al., 2007 [65] | 15 (15, 0) | Healthy subjects | Heat stimuli | Neuroimaging (PET) | VAS (0–10) | p < 0.05 |
| Wager et al., 2011 [63] | 47 | Healthy subjects | Shock pain; heat pain | Neuroimaging (fMRI) | 10 point scale | p < 0.001 |
| Wanigasekera et al., 2018 [96] | 16 | Patients (Post-traumatic neuropathic pain) | - | Neuroimaging (MRI) | NRS (0–10) | p = 0.05 |
| Weimer et al., 2019 [108] | 39 (25 monozygotic; 14 dizygotic twin pairs) | Healthy subjects | Heat pain | Behavioral | NRS (0–10) | p < 0.05 |
| Wrobel et al., 2014 [48] | 50 (28, 32, 12) | Healthy subjects | Heat pain | Neuroimaging (fMRI); Pharmacological | VAS (0–100) | p < 0.05 |
References
- Hohenschurz-Schmidt, D.; Thomson, O.P.; Rossettini, G.; Miciak, M.; Newell, D.; Roberts, L.; Vase, L.; Draper-Rodi, J. Avoiding nocebo and other undesirable effects in chiropractic, osteopathy and physiotherapy: An invitation to reflect. Musculoskelet. Sci. Pract. 2022, 62, 102677. [Google Scholar] [CrossRef] [PubMed]
- Palese, A.; Rossettini, G.; Colloca, L.; Testa, M. The impact of contextual factors on nursing outcomes and the role of placebo/nocebo effects: A discussion paper. Pain Rep. 2019, 4, e716. [Google Scholar] [CrossRef] [PubMed]
- Colloca, L. Placebo effects in pain. Int. Rev. Neurobiol. 2020, 153, 167–185. [Google Scholar] [CrossRef] [PubMed]
- Ongaro, G.; Kaptchuk, T.J. Symptom perception, placebo effects, and the Bayesian brain. Pain 2019, 160, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Benedetti, F.; Frisaldi, E.; Shaibani, A. Thirty Years of Neuroscientific Investigation of Placebo and Nocebo: The Interesting, the Good, and the Bad. Annu. Rev. Pharmacol. Toxicol. 2022, 62, 323–340. [Google Scholar] [CrossRef]
- Carlino, E.; Frisaldi, E.; Benedetti, F. Pain and the context. Nat. Rev. Rheumatol. 2014, 10, 348–355. [Google Scholar] [CrossRef]
- Carlino, E.; Benedetti, F. Different contexts, different pains, different experiences. Neuroscience 2016, 338, 19–26. [Google Scholar] [CrossRef]
- Benedetti, F. Placebo and the new physiology of the doctor-patient relationship. Physiol. Rev. 2013, 93, 1207–1246. [Google Scholar] [CrossRef]
- Colloca, L.; Lopiano, L.; Lanotte, M.; Benedetti, F. Overt versus covert treatment for pain, anxiety, and Parkinson’s disease. Lancet Neurol. 2004, 3, 679–684. [Google Scholar] [CrossRef]
- Gasparyan, A.Y.; Ayvazyan, L.; Blackmore, H.; Kitas, G.D. Writing a narrative biomedical review: Considerations for authors, peer reviewers, and editors. Rheumatol. Int. 2011, 31, 1409–1417. [Google Scholar] [CrossRef]
- Benedetti, F.; Piedimonte, A. The neurobiological underpinnings of placebo and nocebo effects. Semin. Arthritis Rheum. 2019, 49, S18–S21. [Google Scholar] [CrossRef]
- Carlino, E.; Piedimonte, A.; Benedetti, F. Chapter 48—Nature of the placebo and nocebo effect in relation to functional neurologic disorders. In Handbook of Clinical Neurology; Hallett, M., Stone, J., Carson, A., Eds.; Elsevier: Amsterdam, The Netherlands, 2016; Volume 139, pp. 597–606. [Google Scholar]
- Klinger, R.; Stuhlreyer, J.; Schwartz, M.; Schmitz, J.; Colloca, L. Clinical Use of Placebo Effects in Patients with Pain Disorders. Int. Rev. Neurobiol. 2018, 139, 107–128. [Google Scholar] [CrossRef]
- Morozov, A.; Bazarkin, A.; Babaevskaya, D.; Taratkin, M.; Kozlov, V.; Suvorov, A.; Spivak, L.; McFarland, J.; Russo, G.I.; Enikeev, D. A systematic review and meta-analysis of placebo effect in clinical trials on chronic prostatitis/chronic pelvic pain syndrome. Prostate 2022, 82, 633–656. [Google Scholar] [CrossRef]
- Colagiuri, B.; Schenk, L.A.; Kessler, M.D.; Dorsey, S.G.; Colloca, L. The placebo effect: From concepts to genes. Neuroscience 2015, 307, 171–190. [Google Scholar] [CrossRef] [Green Version]
- Camerone, E.M.; Piedimonte, A.; Testa, M.; Wiech, K.; Vase, L.; Zamfira, D.A.; Benedetti, F.; Carlino, E. The Effect of Temporal Information on Placebo Analgesia and Nocebo Hyperalgesia. Psychosom. Med. 2021, 83, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Camerone, E.M.; Wiech, K.; Benedetti, F.; Carlino, E.; Job, M.; Scafoglieri, A.; Testa, M. ‘External timing’ of placebo analgesia in an experimental model of sustained pain. Eur. J. Pain 2021, 25, 1303–1315. [Google Scholar] [CrossRef] [PubMed]
- Camerone, E.M.; Battista, S.; Benedetti, F.; Carlino, E.; Sansone, L.G.; Buzzatti, L.; Scafoglieri, A.; Testa, M. The Temporal Modulation of Nocebo Hyperalgesia in a Model of Sustained Pain. Front. Psychiatry 2022, 13, 807138. [Google Scholar] [CrossRef] [PubMed]
- Rosenkjær, S.; Lunde, S.J.; Kirsch, I.; Vase, L. Expectations: How and when do they contribute to placebo analgesia? Front. Psychiatry 2022, 13, 817179. [Google Scholar] [CrossRef]
- Amanzio, M.; Benedetti, F. Neuropharmacological dissection of placebo analgesia: Expectation-activated opioid systems versus conditioning-activated specific subsystems. J. Neurosci. 1999, 19, 484–494. [Google Scholar] [CrossRef] [Green Version]
- Colloca, L.; Sigaudo, M.; Benedetti, F. The role of learning in nocebo and placebo effects. PAIN® 2008, 136, 211–218. [Google Scholar] [CrossRef]
- Colloca, L.; Miller, F.G. How placebo responses are formed: A learning perspective. Philos. Trans. R. Soc. Lond. B. Biol. Sci. 2011, 366, 1859–1869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piedimonte, A.; Guerra, G.; Vighetti, S.; Carlino, E. Measuring expectation of pain: Contingent negative variation in placebo and nocebo effects. Eur. J. Pain 2017, 21, 874–885. [Google Scholar] [CrossRef] [PubMed]
- Colloca, L.; Benedetti, F. How prior experience shapes placebo analgesia. Pain 2006, 124, 126–133. [Google Scholar] [CrossRef]
- Colloca, L.; Petrovic, P.; Wager, T.D.; Ingvar, M.; Benedetti, F. How the number of learning trials affects placebo and nocebo responses. Pain 2010, 151, 430–439. [Google Scholar] [CrossRef] [Green Version]
- Carlino, E.; Guerra, G.; Piedimonte, A. Placebo effects: From pain to motor performance. Neurosci. Lett. 2016, 632, 224–230. [Google Scholar] [CrossRef]
- Benedetti, F.; Carlino, E.; Pollo, A. Hidden administration of drugs. Clin. Pharmacol. Ther. 2011, 90, 651–661. [Google Scholar] [CrossRef]
- Amanzio, M.; Pollo, A.; Maggi, G.; Benedetti, F. Response variability to analgesics: A role for non-specific activation of endogenous opioids. Pain 2001, 90, 205–215. [Google Scholar] [CrossRef]
- Kube, T.; Rief, W.; Vivell, M.B.; Schäfer, N.L.; Vermillion, T.; Körfer, K.; Glombiewski, J.A. Deceptive and Nondeceptive Placebos to Reduce Pain: An Experimental Study in Healthy Individuals. Clin. J. Pain 2020, 36, 68–79. [Google Scholar] [CrossRef]
- Disley, N.; Kola-Palmer, S.; Retzler, C. A comparison of open-label and deceptive placebo analgesia in a healthy sample. J. Psychosom. Res. 2021, 140, 110298. [Google Scholar] [CrossRef] [PubMed]
- Zunhammer, M.; Spisák, T.; Wager, T.D.; Bingel, U. Meta-analysis of neural systems underlying placebo analgesia from individual participant fMRI data. Nat. Commun. 2021, 12, 1391. [Google Scholar] [CrossRef] [PubMed]
- Frisaldi, E.; Shaibani, A.; Benedetti, F. Understanding the mechanisms of placebo and nocebo effects. Swiss Med. Wkly. 2020, 150, w20340. [Google Scholar] [CrossRef]
- Ortega, Á.; Salazar, J.; Galban, N.; Rojas, M.; Ariza, D.; Chávez-Castillo, M.; Nava, M.; Riaño-Garzón, M.E.; Díaz-Camargo, E.A.; Medina-Ortiz, O.; et al. Psycho-Neuro-Endocrine-Immunological Basis of the Placebo Effect: Potential Applications beyond Pain Therapy. Int. J. Mol. Sci. 2022, 23, 4196. [Google Scholar] [CrossRef]
- Eippert, F.; Bingel, U.; Schoell, E.D.; Yacubian, J.; Klinger, R.; Lorenz, J.; Büchel, C. Activation of the opioidergic descending pain control system underlies placebo analgesia. Neuron 2009, 63, 533–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellerbrock, I.; Wiehler, A.; Arndt, M.; May, A. Nocebo context modulates long-term habituation to heat pain and influences functional connectivity of the operculum. Pain 2015, 156, 2222–2233. [Google Scholar] [CrossRef]
- Benedetti, F.; Amanzio, M.; Rosato, R.; Blanchard, C. Nonopioid placebo analgesia is mediated by CB1 cannabinoid receptors. Nat. Med. 2011, 17, 1228–1230. [Google Scholar] [CrossRef]
- Benedetti, F.; Shaibani, A.; Arduino, C.; Thoen, W. Open-label nondeceptive placebo analgesia is blocked by the opioid antagonist naloxone. Pain 2022, 164, 984–990. [Google Scholar] [CrossRef]
- Benedetti, F.; Amanzio, M.; Casadio, C.; Oliaro, A.; Maggi, G. Blockade of nocebo hyperalgesia by the cholecystokinin antagonist proglumide. Pain 1997, 71, 135–140. [Google Scholar] [CrossRef]
- Benedetti, F. The opposite effects of the opiate antagonist naloxone and the cholecystokinin antagonist proglumide on placebo analgesia. Pain 1996, 64, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Benedetti, F.; Amanzio, M.; Maggi, G. Potentiation of placebo analgesia by proglumide. Lancet 1995, 346, 1231. [Google Scholar] [CrossRef] [PubMed]
- Benedetti, F.; Amanzio, M.; Thoen, W. Disruption of opioid-induced placebo responses by activation of cholecystokinin type-2 receptors. Psychopharmacology 2011, 213, 791–797. [Google Scholar] [CrossRef]
- Benedetti, F.; Amanzio, M.; Vighetti, S.; Asteggiano, G. The biochemical and neuroendocrine bases of the hyperalgesic nocebo effect. J. Neurosci. 2006, 26, 12014–12022. [Google Scholar] [CrossRef] [Green Version]
- Scott, D.J.; Stohler, C.S.; Egnatuk, C.M.; Wang, H.; Koeppe, R.A.; Zubieta, J.K. Placebo and nocebo effects are defined by opposite opioid and dopaminergic responses. Arch. Gen. Psychiatry 2008, 65, 220–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irizarry, K.J.; Licinio, J. An explanation for the placebo effect? Science 2005, 307, 1411–1412. [Google Scholar] [CrossRef] [PubMed]
- Peciña, M.; Zubieta, J.K. Molecular mechanisms of placebo responses in humans. Mol. Psychiatry 2015, 20, 416–423. [Google Scholar] [CrossRef] [Green Version]
- Jarcho, J.M.; Feier, N.A.; Labus, J.S.; Naliboff, B.; Smith, S.R.; Hong, J.Y.; Colloca, L.; Tillisch, K.; Mandelkern, M.A.; Mayer, E.A.; et al. Placebo analgesia: Self-report measures and preliminary evidence of cortical dopamine release associated with placebo response. NeuroImage Clin. 2016, 10, 107–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skyt, I.; Moslemi, K.; Baastrup, C.; Grosen, K.; Benedetti, F.; Petersen, G.L.; Price, D.D.; Hall, K.T.; Kaptchuk, T.J.; Svensson, P.; et al. Dopaminergic tone does not influence pain levels during placebo interventions in patients with chronic neuropathic pain. Pain 2018, 159, 261–272. [Google Scholar] [CrossRef]
- Wrobel, N.; Wiech, K.; Forkmann, K.; Ritter, C.; Bingel, U. Haloperidol blocks dorsal striatum activity but not analgesia in a placebo paradigm. Cortex 2014, 57, 60–73. [Google Scholar] [CrossRef]
- Scott, D.J.; Stohler, C.S.; Egnatuk, C.M.; Wang, H.; Koeppe, R.A.; Zubieta, J.K. Individual differences in reward responding explain placebo-induced expectations and effects. Neuron 2007, 55, 325–336. [Google Scholar] [CrossRef] [Green Version]
- Colloca, L.; Pine, D.S.; Ernst, M.; Miller, F.G.; Grillon, C. Vasopressin Boosts Placebo Analgesic Effects in Women: A Randomized Trial. Biol. Psychiatry 2016, 79, 794–802. [Google Scholar] [CrossRef]
- Kessner, S.; Sprenger, C.; Wrobel, N.; Wiech, K.; Bingel, U. Effect of oxytocin on placebo analgesia: A randomized study. JAMA 2013, 310, 1733–1735. [Google Scholar] [CrossRef] [PubMed]
- Feng, C.; Hackett, P.D.; DeMarco, A.C.; Chen, X.; Stair, S.; Haroon, E.; Ditzen, B.; Pagnoni, G.; Rilling, J.K. Oxytocin and vasopressin effects on the neural response to social cooperation are modulated by sex in humans. Brain Imaging Behav. 2015, 9, 754–764. [Google Scholar] [CrossRef]
- Thompson, R.; Gupta, S.; Miller, K.; Mills, S.; Orr, S. The effects of vasopressin on human facial responses related to social communication. Psychoneuroendocrinology 2004, 29, 35–48. [Google Scholar] [CrossRef] [PubMed]
- Benedetti, F.; Durando, J.; Vighetti, S. Nocebo and placebo modulation of hypobaric hypoxia headache involves the cyclooxygenase-prostaglandins pathway. Pain 2014, 155, 921–928. [Google Scholar] [CrossRef] [PubMed]
- Prossin, A.; Koch, A.; Campbell, P.; Laumet, G.; Stohler, C.S.; Dantzer, R.; Zubieta, J.K. Effects of placebo administration on immune mechanisms and relationships with central endogenous opioid neurotransmission. Mol. Psychiatry 2022, 27, 831–839. [Google Scholar] [CrossRef] [PubMed]
- Skyt, I.; Lunde, S.J.; Baastrup, C.; Svensson, P.; Jensen, T.S.; Vase, L. Neurotransmitter systems involved in placebo and nocebo effects in healthy participants and patients with chronic pain: A systematic review. Pain 2020, 161, 11–23. [Google Scholar] [CrossRef]
- Kong, J.; Gollub, R.L.; Rosman, I.S.; Webb, J.M.; Vangel, M.G.; Kirsch, I.; Kaptchuk, T.J. Brain activity associated with expectancy-enhanced placebo analgesia as measured by functional magnetic resonance imaging. J. Neurosci. 2006, 26, 381–388. [Google Scholar] [CrossRef] [Green Version]
- Lieberman, M.D.; Jarcho, J.M.; Berman, S.; Naliboff, B.D.; Suyenobu, B.Y.; Mandelkern, M.; Mayer, E.A. The neural correlates of placebo effects: A disruption account. NeuroImage 2004, 22, 447–455. [Google Scholar] [CrossRef] [Green Version]
- Petrovic, P.; Kalso, E.; Petersson, K.M.; Andersson, J.; Fransson, P.; Ingvar, M. A prefrontal non-opioid mechanism in placebo analgesia. Pain 2010, 150, 59–65. [Google Scholar] [CrossRef]
- Petrovic, P.; Kalso, E.; Petersson, K.M.; Ingvar, M. Placebo and opioid analgesia—Imaging a shared neuronal network. Science 2002, 295, 1737–1740. [Google Scholar] [CrossRef] [Green Version]
- Price, D.D.; Craggs, J.; Verne, G.N.; Perlstein, W.M.; Robinson, M.E. Placebo analgesia is accompanied by large reductions in pain-related brain activity in irritable bowel syndrome patients. Pain 2007, 127, 63–72. [Google Scholar] [CrossRef]
- Tracey, I. Getting the pain you expect: Mechanisms of placebo, nocebo and reappraisal effects in humans. Nat. Med. 2010, 16, 1277–1283. [Google Scholar] [CrossRef]
- Wager, T.D.; Atlas, L.Y.; Leotti, L.A.; Rilling, J.K. Predicting individual differences in placebo analgesia: Contributions of brain activity during anticipation and pain experience. J. Neurosci. 2011, 31, 439–452. [Google Scholar] [CrossRef] [Green Version]
- Wager, T.D.; Rilling, J.K.; Smith, E.E.; Sokolik, A.; Casey, K.L.; Davidson, R.J.; Kosslyn, S.M.; Rose, R.M.; Cohen, J.D. Placebo-induced changes in FMRI in the anticipation and experience of pain. Science 2004, 303, 1162–1167. [Google Scholar] [CrossRef]
- Wager, T.D.; Scott, D.J.; Zubieta, J.K. Placebo effects on human mu-opioid activity during pain. Proc. Natl. Acad. Sci. USA 2007, 104, 11056–11061. [Google Scholar] [CrossRef] [Green Version]
- Palermo, S.; Benedetti, F.; Costa, T.; Amanzio, M. Pain anticipation: An activation likelihood estimation meta-analysis of brain imaging studies. Hum. Brain Mapp. 2015, 36, 1648–1661. [Google Scholar] [CrossRef] [Green Version]
- Ploghaus, A.; Tracey, I.; Gati, J.S.; Clare, S.; Menon, R.S.; Matthews, P.M.; Rawlins, J.N. Dissociating pain from its anticipation in the human brain. Science 1999, 284, 1979–1981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koyama, T.; Tanaka, Y.Z.; Mikami, A. Nociceptive neurons in the macaque anterior cingulate activate during anticipation of pain. NeuroReport 1998, 9, 2663–2667. [Google Scholar] [CrossRef] [PubMed]
- Porro, C.A.; Baraldi, P.; Pagnoni, G.; Serafini, M.; Facchin, P.; Maieron, M.; Nichelli, P. Does anticipation of pain affect cortical nociceptive systems? J. Neurosci. 2002, 22, 3206–3214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koyama, T.; McHaffie, J.G.; Laurienti, P.J.; Coghill, R.C. The subjective experience of pain: Where expectations be come reality. Proc. Natl. Acad. Sci. USA 2005, 102, 12950–12955. [Google Scholar] [CrossRef] [Green Version]
- Kong, J.; Gollub, R.L.; Polich, G.; Kirsch, I.; Laviolette, P.; Vangel, M.; Rosen, B.; Kaptchuk, T.J. A functional magnetic resonance imaging study on the neural mechanisms of hyperalgesic nocebo effect. J. Neurosci. 2008, 28, 13354–13362. [Google Scholar] [CrossRef] [Green Version]
- Van der Meulen, M.; Kamping, S.; Anton, F. The role of cognitive reappraisal in placebo analgesia: An fMRI study. Soc. Cogn. Affect. Neurosci. 2017, 12, 1128–1137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlino, E.; Torta, D.M.; Piedimonte, A.; Frisaldi, E.; Vighetti, S.; Benedetti, F. Role of explicit verbal information in conditioned analgesia. Eur. J. Pain 2015, 19, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Morton, D.L.; Brown, C.A.; Watson, A.; El-Deredy, W.; Jones, A.K. Cognitive changes as a result of a single exposure to placebo. Neuropsychologia 2010, 48, 1958–1964. [Google Scholar] [CrossRef] [PubMed]
- Nagai, Y.; Critchley, H.D.; Featherstone, E.; Fenwick, P.B.; Trimble, M.R.; Dolan, R.J. Brain activity relating to the contingent negative variation: An fMRI investigation. NeuroImage 2004, 21, 1232–1241. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Larrea, L.; Frot, M.; Valeriani, M. Brain generators of laser-evoked potentials: From dipoles to functional significance. Neurophysiol. Clin. 2003, 33, 279–292. [Google Scholar] [CrossRef]
- Vecchio, A.; De Pascalis, V. ERP Indicators of Self-Pain and Other Pain Reductions due to Placebo Analgesia Responding: The Moderating Role of the Fight-Flight-Freeze System. Brain Sci. 2021, 11, 1192. [Google Scholar] [CrossRef]
- Linde, K.; Atmann, O.; Meissner, K.; Schneider, A.; Meister, R.; Kriston, L.; Werner, C. How often do general practitioners use placebos and non-specific interventions? Systematic review and meta-analysis of surveys. PLoS ONE 2018, 13, e0202211. [Google Scholar] [CrossRef] [Green Version]
- Malfliet, A.; Lluch Girbés, E.; Pecos-Martin, D.; Gallego-Izquierdo, T.; Valera-Calero, A. The Influence of Treatment Expectations on Clinical Outcomes and Cortisol Levels in Patients With Chronic Neck Pain: An Experimental Study. Pain Pract. 2019, 19, 370–381. [Google Scholar] [CrossRef]
- Pavlov, I.; Thompson, W. The Work of the Digestive Glands; C. Griffin: London, UK, 1902. [Google Scholar]
- Pollo, A.; Amanzio, M.; Arslanian, A.; Casadio, C.; Maggi, G.; Benedetti, F. Response expectancies in placebo analgesia and their clinical relevance. Pain 2001, 93, 77–84. [Google Scholar] [CrossRef]
- Vase, L.; Robinson, M.E.; Verne, G.N.; Price, D.D. The contributions of suggestion, desire, and expectation to placebo effects in irritable bowel syndrome patients. An empirical investigation. Pain 2003, 105, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Sawamoto, N.; Honda, M.; Okada, T.; Hanakawa, T.; Kanda, M.; Fukuyama, H.; Konishi, J.; Shibasaki, H. Expectation of pain enhances responses to nonpainful somatosensory stimulation in the anterior cingulate cortex and parietal operculum/posterior insula: An event-related functional magnetic resonance imaging study. J. Neurosci. 2000, 20, 7438–7445. [Google Scholar] [CrossRef] [Green Version]
- Schmid, J.; Bingel, U.; Ritter, C.; Benson, S.; Schedlowski, M.; Gramsch, C.; Forsting, M.; Elsenbruch, S. Neural underpinnings of nocebo hyperalgesia in visceral pain: A fMRI study in healthy volunteers. NeuroImage 2015, 120, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Bingel, U.; Wanigasekera, V.; Wiech, K.; Ni Mhuircheartaigh, R.; Lee, M.C.; Ploner, M.; Tracey, I. The effect of treatment expectation on drug efficacy: Imaging the analgesic benefit of the opioid remifentanil. Sci. Transl. Med. 2011, 3, 70ra14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benedetti, F.; Arduino, C.; Costa, S.; Vighetti, S.; Tarenzi, L.; Rainero, I.; Asteggiano, G. Loss of expectation-related mechanisms in Alzheimer’s disease makes analgesic therapies less effective. Pain 2006, 121, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Krummenacher, P.; Candia, V.; Folkers, G.; Schedlowski, M.; Schönbächler, G. Prefrontal cortex modulates placebo analgesia. Pain 2010, 148, 368–374. [Google Scholar] [CrossRef]
- Tu, Y.; Wilson, G.; Camprodon, J.; Dougherty, D.D.; Vangel, M.; Benedetti, F.; Kaptchuk, T.J.; Gollub, R.L.; Kong, J. Manipulating placebo analgesia and nocebo hyperalgesia by changing brain excitability. Proc. Natl. Acad. Sci. USA 2021, 118. [Google Scholar] [CrossRef]
- Tétreault, P.; Mansour, A.; Vachon-Presseau, E.; Schnitzer, T.J.; Apkarian, A.V.; Baliki, M.N. Brain Connectivity Predicts Placebo Response across Chronic Pain Clinical Trials. PLoS Biol. 2016, 14, e1002570. [Google Scholar] [CrossRef] [Green Version]
- Vachon-Presseau, E.; Berger, S.E.; Abdullah, T.B.; Huang, L.; Cecchi, G.A.; Griffith, J.W.; Schnitzer, T.J.; Apkarian, A.V. Brain and psychological determinants of placebo pill response in chronic pain patients. Nat. Commun. 2018, 9, 3397. [Google Scholar] [CrossRef] [Green Version]
- Hashmi, J.A.; Kong, J.; Spaeth, R.; Khan, S.; Kaptchuk, T.J.; Gollub, R.L. Functional network architecture predicts psychologically mediated analgesia related to treatment in chronic knee pain patients. J. Neurosci. 2014, 34, 3924–3936. [Google Scholar] [CrossRef] [Green Version]
- Eippert, F.; Finsterbusch, J.; Bingel, U.; Büchel, C. Direct evidence for spinal cord involvement in placebo analgesia. Science 2009, 326, 404. [Google Scholar] [CrossRef]
- Duerden, E.G.; Albanese, M.C. Localization of pain-related brain activation: A meta-analysis of neuroimaging data. Hum. Brain Mapp. 2013, 34, 109–149. [Google Scholar] [CrossRef]
- Segerdahl, A.R.; Mezue, M.; Okell, T.W.; Farrar, J.T.; Tracey, I. The dorsal posterior insula subserves a fundamental role in human pain. Nat. Neurosci. 2015, 18, 499–500. [Google Scholar] [CrossRef] [PubMed]
- Bush, N.; Robinson, M.; Bryan, M.; Staud, R.; Boissoneault, J. Task-dependent functional connectivity of pain-related brain regions is related to magnitude of placebo analgesia. J. Pain 2021, 22, 603. [Google Scholar] [CrossRef]
- Wanigasekera, V.; Wartolowska, K.; Huggins, J.P.; Duff, E.P.; Vennart, W.; Whitlock, M.; Massat, N.; Pauer, L.; Rogers, P.; Hoggart, B.; et al. Disambiguating pharmacological mechanisms from placebo in neuropathic pain using functional neuroimaging. Br. J. Anaesth. 2018, 120, 299–307. [Google Scholar] [CrossRef] [Green Version]
- Crawford, L.S.; Mills, E.P.; Hanson, T.; Macey, P.M.; Glarin, R.; Macefield, V.G.; Keay, K.A.; Henderson, L.A. Brainstem Mechanisms of Pain Modulation: A within-Subjects 7T fMRI Study of Placebo Analgesic and Nocebo Hyperalgesic Responses. J. Neurosci. 2021, 41, 9794–9806. [Google Scholar] [CrossRef]
- Ruscheweyh, R.; Kühnel, M.; Filippopulos, F.; Blum, B.; Eggert, T.; Straube, A. Altered experimental pain perception after cerebellar infarction. Pain 2014, 155, 1303–1312. [Google Scholar] [CrossRef]
- Tinnermann, A.; Geuter, S.; Sprenger, C.; Finsterbusch, J.; Büchel, C. Interactions between brain and spinal cord mediate value effects in nocebo hyperalgesia. Science 2017, 358, 105–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bingel, U.; Wiech, K.; Ritter, C.; Wanigasekera, V.; Ní Mhuircheartaigh, R.; Lee, M.C.; Ploner, M.; Tracey, I. Hippocampus mediates nocebo impairment of opioid analgesia through changes in functional connectivity. Eur. J. Neurosci. 2022, 56, 3967–3978. [Google Scholar] [CrossRef] [PubMed]
- Zunhammer, M.; Bingel, U.; Wager, T.D. Placebo Effects on the Neurologic Pain Signature: A Meta-analysis of Individual Participant Functional Magnetic Resonance Imaging Data. JAMA Neurol. 2018, 75, 1321–1330. [Google Scholar] [CrossRef] [Green Version]
- Cai, L.; He, L. Placebo effects and the molecular biological components involved. Gen. Psychiatry 2019, 32, e100089. [Google Scholar] [CrossRef]
- Hall, K.T.; Loscalzo, J.; Kaptchuk, T.J. Genetics and the placebo effect: The placebome. Trends Mol. Med. 2015, 21, 285–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, K.T.; Loscalzo, J.; Kaptchuk, T. Pharmacogenomics and the Placebo Response. ACS Chem. Neurosci. 2018, 9, 633–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colloca, L.; Wang, Y.; Martinez, P.E.; Chang, Y.C.; Ryan, K.A.; Hodgkinson, C.; Goldman, D.; Dorsey, S.G. OPRM1 rs1799971, COMT rs4680, and FAAH rs324420 genes interact with placebo procedures to induce hypoalgesia. Pain 2019, 160, 1824–1834. [Google Scholar] [CrossRef] [PubMed]
- Peciña, M.; Love, T.; Stohler, C.S.; Goldman, D.; Zubieta, J.K. Effects of the Mu opioid receptor polymorphism (OPRM1 A118G) on pain regulation, placebo effects and associated personality trait measures. Neuropsychopharmacology 2015, 40, 957–965. [Google Scholar] [CrossRef] [Green Version]
- Wang, R.S.; Hall, K.T.; Giulianini, F.; Passow, D.; Kaptchuk, T.J.; Loscalzo, J. Network analysis of the genomic basis of the placebo effect. JCI Insight 2017, 2, e93911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weimer, K.; Hahn, E.; Mönnikes, N.; Herr, A.K.; Stengel, A.; Enck, P. Are Individual Learning Experiences More Important Than Heritable Tendencies? A Pilot Twin Study on Placebo Analgesia. Front. Psychiatry 2019, 10, 679. [Google Scholar] [CrossRef]
- Raffaeli, W.; Tenti, M.; Corraro, A.; Malafoglia, V.; Ilari, S.; Balzani, E.; Bonci, A. Chronic Pain: What Does It Mean? A Review on the Use of the Term Chronic Pain in Clinical Practice. J. Pain Res. 2021, 14, 827–835. [Google Scholar] [CrossRef]
- Vase, L.; Robinson, M.E.; Verne, N.G.; Price, D.D. Increased placebo analgesia over time in irritable bowel syndrome (IBS) patients is associated with desire and expectation but not endogenous opioid mechanisms. Pain 2005, 115, 338–347. [Google Scholar] [CrossRef]
- Kaptchuk, T.J.; Kelley, J.M.; Conboy, L.A.; Davis, R.B.; Kerr, C.E.; Jacobson, E.E.; Kirsch, I.; Schyner, R.N.; Nam, B.H.; Nguyen, L.T.; et al. Components of placebo effect: Randomised controlled trial in patients with irritable bowel syndrome. BMJ 2008, 336, 999–1003. [Google Scholar] [CrossRef] [Green Version]
- Klinger, R.; Kothe, R.; Schmitz, J.; Kamping, S.; Flor, H. Placebo effects of a sham opioid solution: A randomized controlled study in patients with chronic low back pain. Pain 2017, 158, 1893–1902. [Google Scholar] [CrossRef]
- Olson, E.M.; Akintola, T.; Phillips, J.; Blasini, M.; Haycock, N.R.; Martinez, P.E.; Greenspan, J.D.; Dorsey, S.G.; Wang, Y.; Colloca, L. Effects of sex on placebo effects in chronic pain participants: A cross-sectional study. Pain 2021, 162, 531–542. [Google Scholar] [CrossRef]
- Machado, G.C.; Maher, C.G.; Ferreira, P.H.; Pinheiro, M.B.; Lin, C.W.; Day, R.O.; McLachlan, A.J.; Ferreira, M.L. Efficacy and safety of paracetamol for spinal pain and osteoarthritis: Systematic review and meta-analysis of randomised placebo controlled trials. BMJ 2015, 350, h1225. [Google Scholar] [CrossRef] [Green Version]
- Roelofs, P.D.; Deyo, R.A.; Koes, B.W.; Scholten, R.J.; van Tulder, M.W. Non-steroidal anti-inflammatory drugs for low back pain. Cochrane Database Syst. Rev. 2008, CD000396. [Google Scholar] [CrossRef] [PubMed]
- Chaparro, L.E.; Furlan, A.D.; Deshpande, A.; Mailis-Gagnon, A.; Atlas, S.; Turk, D.C. Opioids compared with placebo or other treatments for chronic low back pain: An update of the Cochrane Review. Spine 2014, 39, 556–563. [Google Scholar] [CrossRef] [PubMed]
- Henschke, N.; Kuijpers, T.; Rubinstein, S.M.; van Middelkoop, M.; Ostelo, R.; Verhagen, A.; Koes, B.W.; van Tulder, M.W. Injection therapy and denervation procedures for chronic low-back pain: A systematic review. Eur. Spine J. 2010, 19, 1425–1449. [Google Scholar] [CrossRef] [Green Version]
- Müller, M.; Kamping, S.; Benrath, J.; Skowronek, H.; Schmitz, J.; Klinger, R.; Flor, H. Treatment history and placebo responses to experimental and clinical pain in chronic pain patients. Eur. J. Pain 2016, 20, 1530–1541. [Google Scholar] [CrossRef] [PubMed]
- Constantino, M.J.; Arnkoff, D.B.; Glass, C.R.; Ametrano, R.M.; Smith, J.Z. Expectations. J. Clin. Psychol. 2011, 67, 184–192. [Google Scholar] [CrossRef]
- Peerdeman, K.J.; van Laarhoven, A.I.M.; Keij, S.M.; Vase, L.; Rovers, M.M.; Peters, M.L.; Evers, A.W.M. Relieving patients’ pain with expectation interventions: A meta-analysis. Pain 2016, 157, 1179–1191. [Google Scholar] [CrossRef]
- Colloca, L.; Akintola, T.; Haycock, N.R.; Blasini, M.; Thomas, S.; Phillips, J.; Corsi, N.; Schenk, L.A.; Wang, Y. Prior Therapeutic Experiences, Not Expectation Ratings, Predict Placebo Effects: An Experimental Study in Chronic Pain and Healthy Participants. Psychother. Psychosom. 2020, 89, 371–378. [Google Scholar] [CrossRef]
- Kupers, R.; Maeyaert, J.; Boly, M.; Faymonville, M.E.; Laureys, S. Naloxone-insensitive epidural placebo analgesia in a chronic pain patient. Anesthesiology 2007, 106, 1239–1242. [Google Scholar] [CrossRef] [Green Version]
- De Leon-Casasola, O.A. Opioids for chronic pain: New evidence, new strategies, safe prescribing. Am. J. Med. 2013, 126, S3–S11. [Google Scholar] [CrossRef] [PubMed]
- Meske, D.S.; Lawal, O.D.; Elder, H.; Langberg, V.; Paillard, F.; Katz, N. Efficacy of opioids versus placebo in chronic pain: A systematic review and meta-analysis of enriched enrollment randomized withdrawal trials. J. Pain Res. 2018, 11, 923–934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martins, D.; Veronese, M.; Turkheimer, F.E.; Howard, M.A.; Williams, S.C.R.; Dipasquale, O. A candidate neuroimaging biomarker for detection of neurotransmission-related functional alterations and prediction of pharmacological analgesic response in chronic pain. Brain Commun. 2022, 4, fcab302. [Google Scholar] [CrossRef] [PubMed]
- Ballantyne, J.C.; Shin, N.S. Efficacy of opioids for chronic pain: A review of the evidence. Clin. J. Pain 2008, 24, 469–478. [Google Scholar] [CrossRef]
- Thompson, S.J.; Pitcher, M.H.; Stone, L.S.; Tarum, F.; Niu, G.; Chen, X.; Kiesewetter, D.O.; Schweinhardt, P.; Bushnell, M.C. Chronic neuropathic pain reduces opioid receptor availability with associated anhedonia in rat. Pain 2018, 159, 1856–1866. [Google Scholar] [CrossRef]
- DaSilva, A.F.; Zubieta, J.K.; DosSantos, M.F. Positron emission tomography imaging of endogenous mu-opioid mechanisms during pain and migraine. Pain Rep. 2019, 4, e769. [Google Scholar] [CrossRef]
- Maarrawi, J.; Peyron, R.; Mertens, P.; Costes, N.; Magnin, M.; Sindou, M.; Laurent, B.; Garcia-Larrea, L. Differential brain opioid receptor availability in central and peripheral neuropathic pain. Pain 2007, 127, 183–194. [Google Scholar] [CrossRef]
- Harris, R.E.; Clauw, D.J.; Scott, D.J.; McLean, S.A.; Gracely, R.H.; Zubieta, J.K. Decreased central mu-opioid receptor availability in fibromyalgia. J. Neurosci. 2007, 27, 10000–10006. [Google Scholar] [CrossRef] [Green Version]
- Rossettini, G.; Colombi, A.; Carlino, E.; Manoni, M.; Mirandola, M.; Polli, A.; Camerone, E.M.; Testa, M. Unraveling Negative Expectations and Nocebo-Related Effects in Musculoskeletal Pain. Front. Psychol. 2022, 13, 789377. [Google Scholar] [CrossRef]
- Crombez, G.; Van Ryckeghem, D.M.L.; Eccleston, C.; Van Damme, S. Attentional bias to pain-related information: A meta-analysis. Pain 2013, 154, 497–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pincus, T.; Morley, S. Cognitive-processing bias in chronic pain: A review and integration. Psychol. Bull. 2001, 127, 599–617. [Google Scholar] [CrossRef]
- Schoth, D.E.; Liossi, C. Biased interpretation of ambiguous information in patients with chronic pain: A systematic review and meta-analysis of current studies. Health Psychol. 2016, 35, 944–956. [Google Scholar] [CrossRef]
- Rizvi, S.J.; Gandhi, W.; Salomons, T. Reward processing as a common diathesis for chronic pain and depression. Neurosci. Biobehav. Rev. 2021, 127, 749–760. [Google Scholar] [CrossRef]
- Apkarian, A.V.; Sosa, Y.; Krauss, B.R.; Thomas, P.S.; Fredrickson, B.E.; Levy, R.E.; Harden, R.N.; Chialvo, D.R. Chronic pain patients are impaired on an emotional decision-making task. Pain 2004, 108, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.; Kleinböhl, D.; Baus, D.; Hölzl, R. Operant learning of perceptual sensitization and habituation is impaired in fibromyalgia patients with and without irritable bowel syndrome. Pain 2011, 152, 1408–1417. [Google Scholar] [CrossRef] [PubMed]
- Verdejo-García, A.; López-Torrecillas, F.; Calandre, E.P.; Delgado-Rodríguez, A.; Bechara, A. Executive function and decision-making in women with fibromyalgia. Arch. Clin. Neuropsychol. 2009, 24, 113–122. [Google Scholar] [CrossRef] [Green Version]
- Walteros, C.; Sánchez-Navarro, J.P.; Muñoz, M.A.; Martínez-Selva, J.M.; Chialvo, D.; Montoya, P. Altered associative learning and emotional decision making in fibromyalgia. J. Psychosom. Res. 2011, 70, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Berger, S.E.; Baria, A.T.; Baliki, M.N.; Mansour, A.; Herrmann, K.M.; Torbey, S.; Huang, L.; Parks, E.L.; Schnizter, T.J.; Apkarian, A.V. Risky monetary behavior in chronic back pain is associated with altered modular connectivity of the nucleus accumbens. BMC Res. Notes 2014, 7, 739. [Google Scholar] [CrossRef] [Green Version]
- Finan, P.H.; Smith, M.T. The comorbidity of insomnia, chronic pain, and depression: Dopamine as a putative mechanism. Sleep Med. Rev. 2013, 17, 173–183. [Google Scholar] [CrossRef] [Green Version]
- Taylor, A.M.W.; Becker, S.; Schweinhardt, P.; Cahill, C. Mesolimbic dopamine signaling in acute and chronic pain: Implications for motivation, analgesia, and addiction. Pain 2016, 157, 1194–1198. [Google Scholar] [CrossRef] [Green Version]
- Borsook, D.; Erpelding, N.; Becerra, L. Losses and gains: Chronic pain and altered brain morphology. Expert Rev. Neurother. 2013, 13, 1221–1234. [Google Scholar] [CrossRef]
- Vachon-Presseau, E.; Abdullah, T.B.; Berger, S.E.; Huang, L.; Griffith, J.W.; Schnitzer, T.J.; Apkarian, A.V. Validating a biosignature-predicting placebo pill response in chronic pain in the settings of a randomized controlled trial. Pain 2022, 163, 910–922. [Google Scholar] [CrossRef]
- Carlino, E.; Vase, L. Can knowledge of Placebo and Nocebo Mechanisms Help Improve Randomized Clinical Trials? Int. Rev. Neurobiol. 2018, 138, 329–357. [Google Scholar] [CrossRef]
- Benedetti, F.; Carlino, E.; Piedimonte, A. Increasing uncertainty in CNS clinical trials: The role of placebo, nocebo, and Hawthorne effects. Lancet Neurol. 2016, 15, 736–747. [Google Scholar] [CrossRef]
- Vase, L.; Petersen, G.L.; Riley, J.L., 3rd; Price, D.D. Factors contributing to large analgesic effects in placebo mechanism studies conducted between 2002 and 2007. Pain 2009, 145, 36–44. [Google Scholar] [CrossRef]
- Petersen, G.L.; Finnerup, N.B.; Colloca, L.; Amanzio, M.; Price, D.D.; Jensen, T.S.; Vase, L. The magnitude of nocebo effects in pain: A meta-analysis. Pain 2014, 155, 1426–1434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsutsumi, Y.; Tsujimoto, Y.; Tajika, A.; Omae, K.; Fujii, T.; Onishi, A.; Kataoka, Y.; Katsura, M.; Noma, H.; Sahker, E.; et al. Proportion attributable to contextual effects in general medicine: A meta-epidemiological study based on Cochrane reviews. BMJ Evid. Based Med. 2023, 28, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Zou, K.; Wong, J.; Abdullah, N.; Chen, X.; Smith, T.; Doherty, M.; Zhang, W. Examination of overall treatment effect and the proportion attributable to contextual effect in osteoarthritis: Meta-analysis of randomised controlled trials. Ann. Rheum. Dis. 2016, 75, 1964–1970. [Google Scholar] [CrossRef] [PubMed]
- Jonas, W.B.; Crawford, C.; Colloca, L.; Kaptchuk, T.J.; Moseley, B.; Miller, F.G.; Kriston, L.; Linde, K.; Meissner, K. To what extent are surgery and invasive procedures effective beyond a placebo response? A systematic review with meta-analysis of randomised, sham controlled trials. BMJ Open 2015, 5, e009655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlsson, M.; Bergenheim, A.; Larsson, M.E.H.; Nordeman, L.; van Tulder, M.; Bernhardsson, S. Effects of exercise therapy in patients with acute low back pain: A systematic review of systematic reviews. Syst. Rev. 2020, 9, 182. [Google Scholar] [CrossRef]
- Artus, M.; van der Windt, D.A.; Jordan, K.P.; Hay, E.M. Low back pain symptoms show a similar pattern of improvement following a wide range of primary care treatments: A systematic review of randomized clinical trials. Rheumatology 2010, 49, 2346–2356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayden, J.A.; Wilson, M.N.; Riley, R.D.; Iles, R.; Pincus, T.; Ogilvie, R. Individual recovery expectations and prognosis of outcomes in non-specific low back pain: Prognostic factor review. Cochrane Database Syst. Rev. 2019, CD011284. [Google Scholar] [CrossRef] [PubMed]
- Mohamed Mohamed, W.J.; Joseph, L.; Canby, G.; Paungmali, A.; Sitilertpisan, P.; Pirunsan, U. Are patient expectations associated with treatment outcomes in individuals with chronic low back pain? A systematic review of randomised controlled trials. Int. J. Clin. Pract. 2020, 74, e13680. [Google Scholar] [CrossRef] [PubMed]
- Wassinger, C.A.; Edwards, D.C.; Bourassa, M.; Reagan, D.; Weyant, E.C.; Walden, R.R. The Role of Patient Recovery Expectations in the Outcomes of Physical Therapist Intervention: A Systematic Review. Phys. Ther. 2022, 102, pzac008. [Google Scholar] [CrossRef] [PubMed]
- Kinney, M.; Seider, J.; Beaty, A.F.; Coughlin, K.; Dyal, M.; Clewley, D. The impact of therapeutic alliance in physical therapy for chronic musculoskeletal pain: A systematic review of the literature. Physiother. Theory Pract. 2020, 36, 886–898. [Google Scholar] [CrossRef] [PubMed]
- Bajcar, E.A.; Bąbel, P. How Does Observational Learning Produce Placebo Effects? A Model Integrating Research Findings. Front. Psychol. 2018, 9, 2041. [Google Scholar] [CrossRef] [Green Version]
- Colloca, L. Placebo, nocebo, and learning mechanisms. Handb. Exp. Pharm. 2014, 225, 17–35. [Google Scholar] [CrossRef]
- Peerdeman, K.J.; van Laarhoven, A.I.; Peters, M.L.; Evers, A.W. An Integrative Review of the Influence of Expectancies on Pain. Front. Psychol. 2016, 7, 1270. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, M.; Fischer, L.M.; Bläute, C.; Stork, J.; Colloca, L.; Zöllner, C.; Klinger, R. Observing treatment outcomes in other patients can elicit augmented placebo effects on pain treatment: A double-blinded randomized clinical trial with patients with chronic low back pain. Pain 2022, 163, 1313–1323. [Google Scholar] [CrossRef]
- Price, D.D.; Milling, L.S.; Kirsch, I.; Duff, A.; Montgomery, G.H.; Nicholls, S.S. An analysis of factors that contribute to the magnitude of placebo analgesia in an experimental paradigm. Pain 1999, 83, 147–156. [Google Scholar] [CrossRef]
- Bordin, E.S. The generalizability of the psychoanalytic concept of the working alliance. Psychother. Theory Res. Pract. 1979, 16, 252–260. [Google Scholar] [CrossRef] [Green Version]
- Fuentes, J.; Armijo-Olivo, S.; Funabashi, M.; Miciak, M.; Dick, B.; Warren, S.; Rashiq, S.; Magee, D.J.; Gross, D.P. Enhanced therapeutic alliance modulates pain intensity and muscle pain sensitivity in patients with chronic low back pain: An experimental controlled study. Phys. Ther. 2014, 94, 477–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelley, J.M.; Lembo, A.J.; Ablon, J.S.; Villanueva, J.J.; Conboy, L.A.; Levy, R.; Marci, C.D.; Kerr, C.E.; Kirsch, I.; Jacobson, E.E.; et al. Patient and practitioner influences on the placebo effect in irritable bowel syndrome. Psychosom. Med. 2009, 71, 789–797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Blasi, Z.; Harkness, E.; Ernst, E.; Georgiou, A.; Kleijnen, J. Influence of context effects on health outcomes: A systematic review. Lancet 2001, 357, 757–762. [Google Scholar] [CrossRef] [PubMed]
- Wartolowska, K.A.; Hohenschurz-Schmidt, D.; Vase, L.; Aronson, J.K. The importance of using placebo controls in nonpharmacological randomised trials. Pain 2022, 164, 921–925. [Google Scholar] [CrossRef]
- Rief, W.; Glombiewski, J.A. The hidden effects of blinded, placebo-controlled randomized trials: An experimental investigation. Pain 2012, 153, 2473–2477. [Google Scholar] [CrossRef]
- Shah, E.; Triantafyllou, K.; Hana, A.A.; Pimentel, M. Adverse events appear to unblind clinical trials in irritable bowel syndrome. Neurogastroenterol. Motil. 2014, 26, 482–488. [Google Scholar] [CrossRef]
- Freed, B.; Williams, B.; Situ, X.; Landsman, V.; Kim, J.; Moroz, A.; Bang, H.; Park, J.J. Blinding, sham, and treatment effects in randomized controlled trials for back pain in 2000–2019: A review and meta-analytic approach. Clin. Trials 2021, 18, 361–370. [Google Scholar] [CrossRef]
- Frisaldi, E.; Shaibani, A.; Benedetti, F. Why We should Assess Patients’ Expectations in Clinical Trials. Pain Ther. 2017, 6, 107–110. [Google Scholar] [CrossRef] [Green Version]
- Zeppieri, G., Jr.; George, S.Z. Patient-defined desired outcome, success criteria, and expectation in outpatient physical therapy: A longitudinal assessment. Health Qual. Life Outcomes 2017, 15, 29. [Google Scholar] [CrossRef] [Green Version]
- Zeppieri, G., Jr.; Lentz, T.A.; Atchison, J.W.; Indelicato, P.A.; Moser, M.W.; Vincent, K.R.; George, S.Z. Preliminary results of patient-defined success criteria for individuals with musculoskeletal pain in outpatient physical therapy settings. Arch. Phys. Med. Rehabil. 2012, 93, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Rutherford, B.R.; Sneed, J.R.; Roose, S.P. Does study design influence outcome? The effects of placebo control and treatment duration in antidepressant trials. Psychother. Psychosom. 2009, 78, 172–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]



| Typology | Details |
|---|---|
| Sources accessed |
|
| Search terms |
|
| Limits |
|
| Studies included |
|
| Steps for writing |
|
| Area | Actions |
|---|---|
| Clinical Practice |
|
| Research |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossettini, G.; Campaci, F.; Bialosky, J.; Huysmans, E.; Vase, L.; Carlino, E. The Biology of Placebo and Nocebo Effects on Experimental and Chronic Pain: State of the Art. J. Clin. Med. 2023, 12, 4113. https://doi.org/10.3390/jcm12124113
Rossettini G, Campaci F, Bialosky J, Huysmans E, Vase L, Carlino E. The Biology of Placebo and Nocebo Effects on Experimental and Chronic Pain: State of the Art. Journal of Clinical Medicine. 2023; 12(12):4113. https://doi.org/10.3390/jcm12124113
Chicago/Turabian StyleRossettini, Giacomo, Francesco Campaci, Joel Bialosky, Eva Huysmans, Lene Vase, and Elisa Carlino. 2023. "The Biology of Placebo and Nocebo Effects on Experimental and Chronic Pain: State of the Art" Journal of Clinical Medicine 12, no. 12: 4113. https://doi.org/10.3390/jcm12124113