
Longitudinal Clinical Features of Post-COVID-19 Patients—Symptoms, Fatigue and Physical Function at 3- and 6-Month Follow-Up
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
- -
- ≥18 years old
- -
- infection with SARS-CoV-2 (PCR-tested) at least six weeks prior to the initial consultation
- -
- sufficient German language skills.
2.2. Study Population
2.3. Questionnaires
2.4. Tests and Examinations
2.5. Laboratory Parameters
2.6. Statistics
3. Results
3.1. Characteristics of Patients with PCS
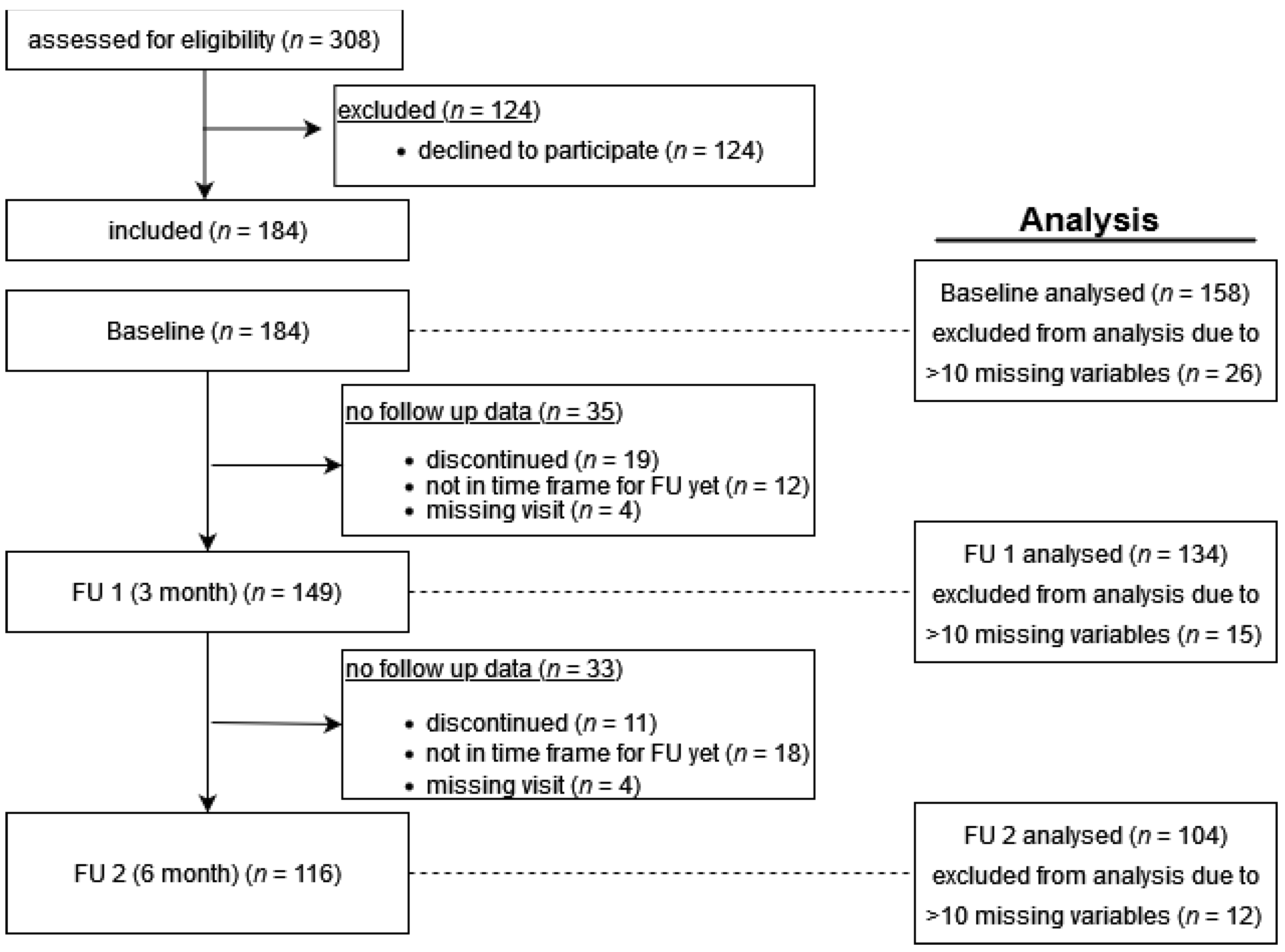
3.2. Baseline Characteristics and Follow-Up
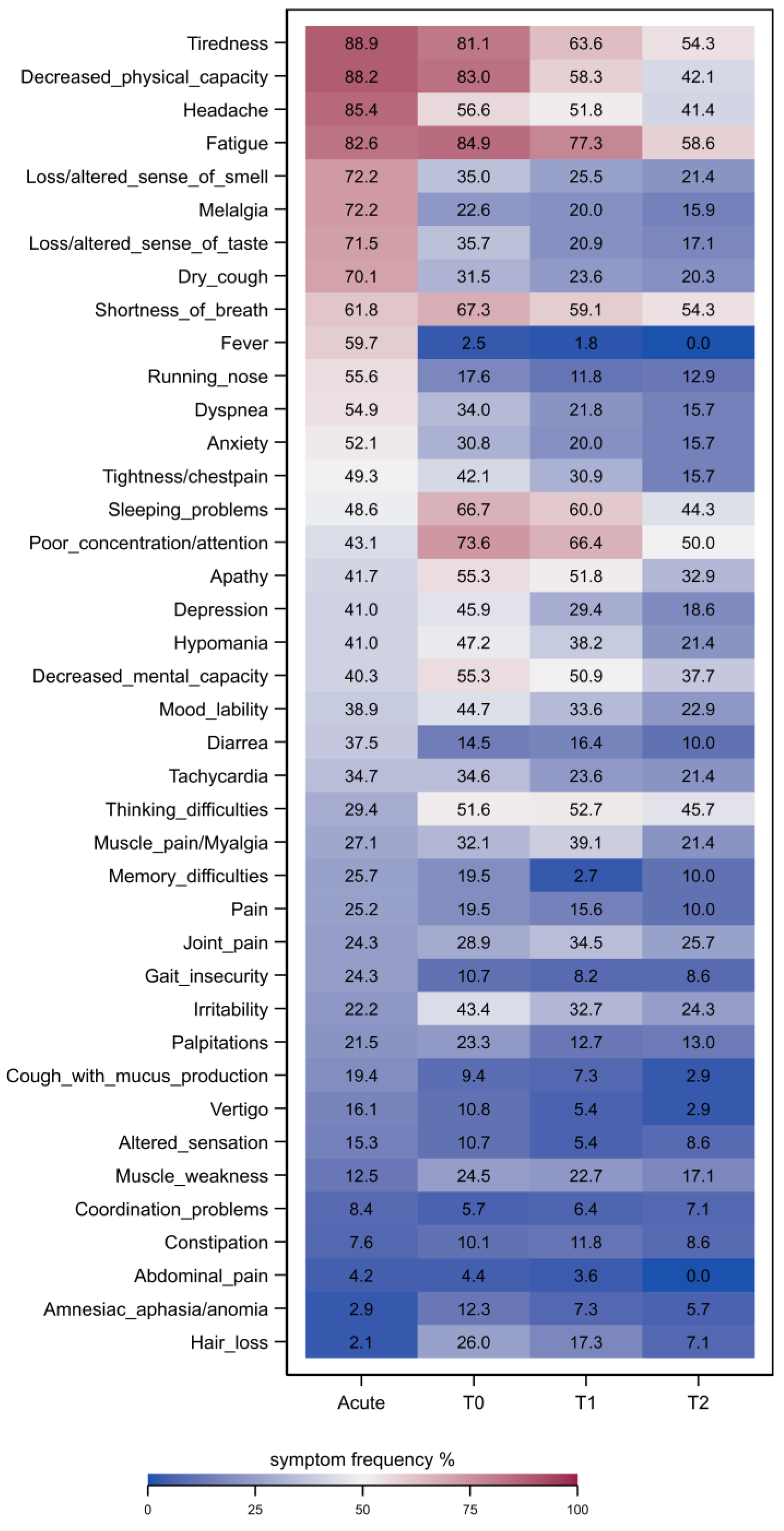
3.3. Symptoms and Scores over Time
3.4. Laboratory Tests
4. Discussion
4.1. Comparison with Other Studies
4.2. Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- The Lancet. Long COVID: 3 years in. Lancet 2023, 401, 795. [CrossRef]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef]
- Cervia, C.; Zurbuchen, Y.; Taeschler, P.; Ballouz, T.; Menges, D.; Hasler, S.; Adamo, S.; Raeber, M.E.; Bächli, E.; Rudiger, A.; et al. Immunoglobulin signature predicts risk of post-acute COVID-19 syndrome. Nat. Commun. 2022, 13, 446. [Google Scholar] [CrossRef] [PubMed]
- Bull-Otterson, L.; Baca, S.; Saydah, S.; Boehmer, T.K.; Adjei, S.; Gray, S.; Harris, A.M. Post–COVID Conditions Among Adult COVID-19 Survivors Aged 18–64 and ≥65 Years—United States, March 2020–November 2021. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 713–717. [Google Scholar] [CrossRef]
- Al-Aly, Z.; Bowe, B.; Xie, Y. Long COVID after breakthrough SARS-CoV-2 infection. Nat. Med. 2022, 28, 1461–1467. [Google Scholar] [CrossRef] [PubMed]
- Ayoubkhani, D.; Bosworth, M.L.; King, S.; Pouwels, K.B.; Glickman, M.; Nafilyan, V.; Zaccardi, F.; Khunti, K.; Alwan, N.A.; Walker, A.S. Risk of Long COVID in people infected with SARS-CoV-2 after two doses of a COVID-19 vaccine: Community-based, matched cohort study. Open Forum Infect. Dis. 2022, 9, ofac464. [Google Scholar] [CrossRef]
- Bowe, B.; Xie, Y.; Al-Aly, Z. Acute and postacute sequelae associated with SARS-CoV-2 reinfection. Nat. Med. 2022, 28, 2398–2405. [Google Scholar] [CrossRef]
- Tsampasian, V.; Elghazaly, H.; Chattopadhyay, R.; Debski, M.; Naing, T.K.P.; Garg, P.; Clark, A.; Ntatsaki, E.; Vassiliou, V.S. Risk Factors Associated with Post-COVID-19 Condition: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2023, 183, 566–580. [Google Scholar] [CrossRef]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef]
- Hayes, L.D.; Ingram, J.; Sculthorpe, N.F. More Than 100 Persistent Symptoms of SARS-CoV-2 (Long COVID): A Scoping Review. Front. Med. 2021, 8, 750378. [Google Scholar] [CrossRef]
- Seeßle, J.; Waterboer, T.; Hippchen, T.; Simon, J.; Kirchner, M.; Lim, A.; Müller, B.; Merle, U. Persistent Symptoms in Adult Patients 1 Year After Coronavirus Disease 2019 (COVID-19): A Prospective Cohort Study. Clin. Infect. Dis. 2022, 74, 1191–1198. [Google Scholar] [CrossRef]
- Peter, R.S.; Nieters, A.; Kräusslich, H.-G.; Brockmann, S.O.; Göpel, S.; Kindle, G.; Merle, U.; Steinacker, J.M.; Rothenbacher, D.; Kern, W.V. Post-acute sequelae of COVID-19 six to 12 months after infection: Population based study. BMJ 2022, 379, e071050. [Google Scholar] [CrossRef]
- DeVries, A.; Shambhu, S.; Sloop, S.; Overhage, J.M. One-Year Adverse Outcomes Among US Adults With Post-COVID-19 Condition vs Those Without COVID-19 in a Large Commercial Insurance Database. JAMA Health Forum 2023, 4, e230010. [Google Scholar] [CrossRef]
- Dennis, A.; Cuthbertson, D.J.; Wootton, D.; Crooks, M.; Gabbay, M.; Eichert, N.; Mouchti, S.; Pansini, M.; Roca-Fernandez, A.; Thomaides-Brears, H.; et al. Multi-organ impairment and long COVID: A 1-year prospective, longitudinal cohort study. J. R. Soc. Med. 2023, 116, 97–112. [Google Scholar] [CrossRef]
- Wahlgren, C.; Forsberg, G.; Divanoglou, A.; Östholm Balkhed, Å.; Niward, K.; Berg, S.; Levi, R. Two-year follow-up of patients with post-COVID-19 condition in Sweden: A prospective cohort study. Lancet Reg. Health Eur. 2023, 28, 100595. [Google Scholar] [CrossRef]
- Huang, L.; Li, X.; Gu, X.; Zhang, H.; Ren, L.; Guo, L.; Liu, M.; Wang, Y.; Cui, D.; Wang, Y.; et al. Health outcomes in people 2 years after surviving hospitalisation with COVID-19: A longitudinal cohort study. Lancet Respir. Med. 2022, 10, 863–876. [Google Scholar] [CrossRef]
- Alkodaymi, M.S.; Omrani, O.A.; Fawzy, N.A.; Shaar, B.A.; Almamlouk, R.; Riaz, M.; Obeidat, M.; Obeidat, Y.; Gerberi, D.; Taha, R.M.; et al. Prevalence of post-acute COVID-19 syndrome symptoms at different follow-up periods: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2022, 28, 657–666. [Google Scholar] [CrossRef]
- Crameri, G.A.G.; Bielecki, M.; Züst, R.; Buehrer, T.W.; Stanga, Z.; Deuel, J.W. Reduced maximal aerobic capacity after COVID-19 in young adult recruits, Switzerland, May 2020. Eurosurveillance 2020, 25, 2001542. [Google Scholar] [CrossRef]
- Steinestel, K.; Czech, A.; Hackenbroch, C.; Bloch, W.; Gagiannis, D. Klinische, radiologische und histopathologische Merkmale des pulmonalen Post-COVID-Syndroms: Eine Form der autoimmunvermittelten interstitiellen Lungenerkrankung? Pathologe 2021, 42, 160–164. [Google Scholar] [CrossRef]
- Ambardar, S.R.; Hightower, S.L.; Huprikar, N.A.; Chung, K.K.; Singhal, A.; Collen, J.F. Post-COVID-19 Pulmonary Fibrosis: Novel Sequelae of the Current Pandemic. J. Clin. Med. 2021, 10, 2452. [Google Scholar] [CrossRef]
- Trinkmann, F.; Müller, M.; Reif, A.; Kahn, N.; Kreuter, M.; Trudzinski, F.; Eichinger, M.; Heussel, C.-P.; Herth, F.J.F. Residual symptoms and lower lung function in patients recovering from SARS-CoV-2 infection. Eur. Respir. J. 2021, 57, 2003002. [Google Scholar] [CrossRef]
- Bouteleux, B.; Henrot, P.; Ernst, R.; Grassion, L.; Raherison-Semjen, C.; Beaufils, F.; Zysman, M.; Delorme, M. Respiratory rehabilitation for COVID-19 related persistent dyspnoea: A one-year experience. Respir. Med. 2021, 189, 106648. [Google Scholar] [CrossRef]
- Xiong, L.; Li, Q.; Cao, X.; Xiong, H.; Huang, M.; Yang, F.; Liu, Q.; Meng, D.; Zhou, M.; Wang, G.; et al. Dynamic changes of functional fitness, antibodies to SARS-CoV-2 and immunological indicators within 1 year after discharge in Chinese health care workers with severe COVID-19: A cohort study. BMC Med. 2021, 19, 163. [Google Scholar] [CrossRef]
- González, J.; Benítez, I.D.; Carmona, P.; Santisteve, S.; Monge, A.; Moncusí-Moix, A.; Gort-Paniello, C.; Pinilla, L.; Carratalá, A.; Zuil, M.; et al. Pulmonary Function and Radiologic Features in Survivors of Critical COVID-19: A 3-Month Prospective Cohort. Chest 2021, 160, 187–198. [Google Scholar] [CrossRef]
- Huang, L.; Yao, Q.; Gu, X.; Wang, Q.; Ren, L.; Wang, Y.; Hu, P.; Guo, L.; Liu, M.; Xu, J.; et al. 1-year outcomes in hospital survivors with COVID-19: A longitudinal cohort study. Lancet 2021, 398, 747–758. [Google Scholar] [CrossRef] [PubMed]
- Dennis, A.; Wamil, M.; Alberts, J.; Oben, J.; Cuthbertson, D.J.; Wootton, D.; Crooks, M.; Gabbay, M.; Brady, M.; Hishmeh, L.; et al. Multiorgan impairment in low-risk individuals with post-COVID-19 syndrome: A prospective, community-based study. BMJ Open 2021, 11, e048391. [Google Scholar] [CrossRef]
- Ceban, F.; Ling, S.; Lui, L.M.W.; Lee, Y.; Gill, H.; Teopiz, K.M.; Rodrigues, N.B.; Subramaniapillai, M.; Di Vincenzo, J.D.; Cao, B.; et al. Fatigue and cognitive impairment in Post-COVID-19 Syndrome: A systematic review and meta-analysis. Brain Behav. Immun. 2022, 101, 93–135. [Google Scholar] [CrossRef]
- Ferrucci, R.; Cuffaro, L.; Capozza, A.; Rosci, C.; Maiorana, N.; Groppo, E.; Reitano, M.R.; Poletti, B.; Ticozzi, N.; Tagliabue, L.; et al. Brain positron emission tomography (PET) and cognitive abnormalities one year after COVID-19. J. Neurol. 2023, 270, 1823–1834. [Google Scholar] [CrossRef]
- Hosp, J.A.; Dressing, A.; Blazhenets, G.; Bormann, T.; Rau, A.; Schwabenland, M.; Thurow, J.; Wagner, D.; Waller, C.; Niesen, W.D.; et al. Cognitive impairment and altered cerebral glucose metabolism in the subacute stage of COVID-19. Brain 2021, 144, 1263–1276. [Google Scholar] [CrossRef]
- Franke, C.; Boesl, F.; Goereci, Y.; Gerhard, A.; Schweitzer, F.; Schroeder, M.; Foverskov-Rasmussen, H.; Heine, J.; Quitschau, A.; Kandil, F.I.; et al. Association of cerebrospinal fluid brain-binding autoantibodies with cognitive impairment in post-COVID-19 syndrome. Brain Behav. Immun. 2023, 109, 139–143. [Google Scholar] [CrossRef]
- Moore, G.E.; Keller, B.A.; Stevens, J.; Mao, X.; Stevens, S.R.; Chia, J.K.; Levine, S.M.; Franconi, C.J.; Hanson, M.R. Recovery from Exercise in Persons with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Medicina 2023, 59, 571. [Google Scholar] [CrossRef]
- Office of the Chief Science Advisor of Canada. Post-COVID-19 Condition in Canada: What We Know, What We Don’t Know, and a Framework for Action; Office of the Chief Science Advisor of Canada: Ottawa, ON, Canada, 2022; Available online: https://science.gc.ca/site/science/sites/default/files/attachments/2023/Post-Covid-Condition_Report-2022.pdf (accessed on 1 April 2023).
- Kim, D. Who Gets Long COVID and Suffers its Mental Health and Socioeconomic Consequences in the United States? Preliminary Findings from a Large Nationwide Study. medRxiv 2023. medRxiv:06.23284199. [Google Scholar]
- Steinmetz, A.; Bahlmann, S.; Bergelt, C.; Bröker, B.M.; Ewert, R.; Felix, S.B.; Flöel, A.; Fleischmann, R.; Hoffmann, W.; Holtfreter, S.; et al. The Greifswald Post COVID Rehabilitation Study and Research (PoCoRe)–Study Design, Characteristics and Evaluation Tools. J. Clin. Med. 2023, 12, 624. [Google Scholar] [CrossRef] [PubMed]
- Winter, T.; Friedrich, N.; Lamp, S.; Schäfer, C.; Schattschneider, M.; Bollmann, S.; Brümmer, D.; Riemann, K.; Petersmann, A.; Nauck, M. The Integrated Research Biobank of the University Medicine Greifswald. Open J. Bioresour. 2020, 7, 2. [Google Scholar] [CrossRef] [Green Version]
- WHO. Living Guidance for Clinical Management of COVID-19. Available online: https://apps.who.int/iris/bitstream/handle/10665/349321/WHO-2019-nCoV-clinical-2021.2-eng.pdf (accessed on 17 April 2023).
- Craparo, G.; La Rosa, V.L.; Commodari, E.; Marino, G.; Vezzoli, M.; Faraci, P.; Vicario, C.M.; Cinà, G.S.; Colombi, M.; Arcoleo, G.; et al. What Is the Role of Psychological Factors in Long COVID Syndrome? Latent Class Analysis in a Sample of Patients Recovered from COVID-19. Int. J. Environ. Res. Public Health 2022, 20, 294. [Google Scholar] [CrossRef]
- Taquet, M.; Dercon, Q.; Luciano, S.; Geddes, J.R.; Husain, M.; Harrison, P.J. Incidence, co-occurrence, and evolution of long-COVID features: A 6-month retrospective cohort study of 273,618 survivors of COVID-19. PLoS Med. 2021, 18, e1003773. [Google Scholar] [CrossRef]
- Ballering, A.V.; van Zon, S.K.R.; Olde Hartman, T.C.; Rosmalen, J.G.M. Persistence of somatic symptoms after COVID-19 in the Netherlands: An observational cohort study. Lancet 2022, 400, 452–461. [Google Scholar] [CrossRef] [PubMed]
- Mejía-Zambrano, H. Radiological and functional pulmonary complications in patients recovered from COVID-19. MIC 2021, 1, e1217. [Google Scholar] [CrossRef]
- Daynes, E.; Gerlis, C.; Briggs-Price, S.; Jones, P.; Singh, S.J. COPD assessment test for the evaluation of COVID-19 symptoms. Thorax 2021, 76, 185–187. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Caro-Codón, J.; Rey, J.R.; Buño, A.; Iniesta, A.M.; Rosillo, S.O.; Castrejon-Castrejon, S.; Rodriguez-Sotelo, L.; Martinez, L.A.; Marco, I.; Merino, C.; et al. Characterization of NT-proBNP in a large cohort of COVID-19 patients. Eur. J. Heart Fail. 2021, 23, 456–464. [Google Scholar] [CrossRef]
- Grant, W.B.; Lahore, H.; McDonnell, S.L.; Baggerly, C.A.; French, C.B.; Aliano, J.L.; Bhattoa, H.P. Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths. Nutrients 2020, 12, 988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Filippo, L.; Frara, S.; Nannipieri, F.; Cotellessa, A.; Locatelli, M.; Rovere Querini, P.; Giustina, A. Low vitamin D levels are associated with Long COVID syndrome in COVID-19 survivors. J. Clin. Endocrinol. Metab. 2023, dgad207. [Google Scholar] [CrossRef]
- Townsend, L.; Dyer, A.H.; McCluskey, P.; O’Brien, K.; Dowds, J.; Laird, E.; Bannan, C.; Bourke, N.M.; Ní Cheallaigh, C.; Byrne, D.G.; et al. Investigating the Relationship between Vitamin D and Persistent Symptoms Following SARS-CoV-2 Infection. Nutrients 2021, 13, 2430. [Google Scholar] [CrossRef]
- Heightman, M.; Prashar, J.; Hillman, T.E.; Marks, M.; Livingston, R.; Ridsdale, H.A.; Bell, R.; Zandi, M.; McNamara, P.; Chauhan, A.; et al. Post-COVID-19 assessment in a specialist clinical service: A 12-month, single-centre, prospective study in 1325 individuals. BMJ Open Respir. Res. 2021, 8, e001041. [Google Scholar] [CrossRef]
- Boesl, F.; Audebert, H.; Endres, M.; Prüss, H.; Franke, C. A Neurological Outpatient Clinic for Patients With Post-COVID-19 Syndrome—A Report on the Clinical Presentations of the First 100 Patients. Front. Neurol. 2021, 12, 738405. [Google Scholar] [CrossRef] [PubMed]
- Rothman, K.J. No adjustments are needed for multiple comparisons. Epidemiology 1990, 1, 43–46. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Female (n = 124) | Male (n = 34) | Total (n = 158) | p-Value | |
|---|---|---|---|---|
| Age mean (SD) | 48.5 (13.8) | 47.1 (16.1) | 48.2 (14.3) | 0.669 |
| BMI mean (SD) | 28.7 (6.2) | 29.5 (5.6) | 28.9 (6.1) | 0.669 |
| Corona Waves n (%) | 0.479 | |||
| 1st Wave (incl. summer 2020) | 6 (4.8) | 1 (2.9) | 7 (4.4) | |
| 2nd Wave | 54 (43.6) | 18 (52.9) | 72 (45.6) | |
| 3rd Wave (VOC Alpha) incl. summer 2021 | 45 (36.3) | 8 (23.5) | 53 (33.5) | |
| 4th/5th Wave (VOC Delta/Omicron) | 19 (15.3) | 7 (20.6) | 27 (16.5) | |
| Preexisting comorbidities n (%) | ||||
| Diabetes | 10 (8.0) | 3 (8.8) | 13 (8.2) | 0.877 |
| Hypertension | 32 (25.6) | 13 (38.2) | 45 (28.5) | 0.155 |
| Respiratory diseases * | 13 (10.4) | 3 (8.2) | 16 (10.1) | 0.776 |
| Depression | 16 (12.9) | 3 (8.8) | 19 (12.0) | 0.517 |
| Rheumatoid arthritis | 31 (25.0) | 11 (32.3) | 42 (26.6) | 0.390 |
| Headache | 11 (8.9) | 1 (2.9) | 12 (7.6) | 0.248 |
| Smoking status n (%) | ||||
| Smoker | 14 (13.1) | 6 (20.7) | 20 (14.7) | 0.529 |
| Former smoker | 16 (15.0) | 3 (10.3) | 19 (14.0) |
| T0 | T1 | T2 | |
|---|---|---|---|
| 6-MWT distance | 459.8 (6.9) | 481.4 (7.4) *** | 499.8 (8.3) *** |
| HR before 6-MWT | 80.9 (1.1) | 75.2 (1.2) *** | 73.5 (1.4) *** |
| HR after 6-MWT | 101.7 (1.6) | 97.3 (1.8) * | 94.5 (2.1) ** |
| HR change 6-MWT | 21.1 (1.5) | 22.2 (1.7) | 20.8 (2.1) |
| BR before 6-MWT | 16.7 (0.3) | 16.1 (0.4) | 15.3 (0.4) *** |
| BR after 6-MWT | 22.9 (0.6) | 21.2 (0.7) * | 20.4 (0.8) ** |
| BR change 6-MWT | 6.2 (0.5) | 5.3 (0.6) | 5.0 (0.7) |
| Borg Scale 6-MWT (6–20) (a) pinteraction = 0.044 | |||
| wk05/20–wk08/21 | 13.3 (0.3) | 12.6 (0.3) ** | 12.8 (0.3) |
| wk09/21–wk30/21 | 12.8 (0.3) | 12.2 (0.3) * | 11.4 (0.4) *** |
| wk31/21–wk52/22 | 14.7 (0.5) | 13.9 (0.6) | 11.9 (0.9) ** |
| O2 saturation at rest | 98.1 (0.2) | 97.4 (0.2) ** | 97.8 (0.2) |
| O2 saturation after 6-MWT | 97.8 (0.1) | 97.6 (0.1) * | 97.7 (0.1) |
| BPsys | 129.4 (1.4) | 127.9 (1.5) | 123.0 (1.7) *** |
| BPdia | 82.0 (1.2) | 77.3 (1.4) ** | 80.1 (1.5) |
| FAS | 34.3 (0.7) | 30.9 (0.8) *** | 28.2 (0.9) *** |
| GAD-7 | 9.1 (0.4) | 7.8 (0.4) *** | 5.8 (0.5) *** |
| PHQ-9 | 11.4 (0.4) | 9.4 (0.5) *** | 7.9 (0.5) *** |
| MoCA | 25.5 (0.2) | 26.2 (0.3) * | 26.7 (0.4) ** |
| CAT | 17.1 (0.5) | 14.3 (0.6) *** | 12.1 (0.6) *** |
| MCRS | 14.4 (1.0) | 12.6 (1.1) | 7.5 (1.4) *** |
| VR-12 (MCS) | 23.5 (1.1) | 28.2 (1.2) *** | 33.5 (1.3) *** |
| VR-12 (PCS) (a) pinteraction = 0.007 | |||
| wk05/20–wk08/21 | 33.4 (1.4) | 37.8 (1.5) *** | 39.4 (1.5) *** |
| wk09/21–wk30/21 | 33.2 (1.8) | 38.6 (1.8) *** | 42.2 (1.9) *** |
| wk31/21–wk52/22 | 29.3 (2.6) | 30.8 (2.9) | 44.9 (3.5) *** |
| ITQ-1 | 10.7 (0.7) | 9.3 (0.8) * | 7.4 (0.9) *** |
| T0 | T1 | T2 | |
|---|---|---|---|
| FAS | |||
| No fatigue | 15 (9.6) | 19 (16.7) | 21 (27.3) |
| Fatigue | 64 (40.8) | 53 (46.5) | 39 (50.7) |
| Severe Fatigue | 78 (49.7) | 42 (36.8) | 17 (16.4) |
| GAD-7 | |||
| 0 minimal | 36 (23.7) | 32 (28.8) | 42 (53.9) |
| 1 mild | 47 (30.9) | 44 (39.6) | 21 (26.9) |
| 2 moderate | 40 (26.3) | 21 (18.9) | 13 (16.7) |
| 3 severe | 29 (19.1) | 14 (12.6) | 2 (2.6) |
| PHQ-9 | |||
| 0 minimal | 17 (11.1) | 22 (20.0) | 26 (33.3) |
| 1 mild | 48 (31.4) | 43 (39.1) | 28 (35.9) |
| 2 moderate | 43 (28.1) | 25 (22.7) | 17 (21.8) |
| 3 moderately severe | 33 (21.6) | 13 (11.8) | 7 (9.0) |
| 4 severe | 12 (7.8) | 7 (6.4) | 0 (0.0) |
| MoCA | |||
| <26 | 61 (38.9) | 35 (31.0) | 18 (25.0) |
| >26 | 96 (61.1) | 78 (69.0) | 54 (75.0) |
| PCFS | |||
| Grade 0 | 0 (0.0) | 5 (4.4) | 10 (13.0) |
| Grade 1 | 11 (7.0) | 18 (15.8) | 16 (20.8) |
| Grade 2 | 90 (57.0) | 65 (57.0) | 44 (57.1) |
| Grade 3 | 55 (34.8) | 24 (21.0) | 7 (9.1) |
| Grade 4 | 2 (1.3) | 2 (1.8) | 0 (0.0) |
| Laboratory Findings | Limits of Normal | T0 Mean (SD) | ||
|---|---|---|---|---|
| Hemoglobin | 7.4–10.0/8.6–11.2 | mmol/L | 8.88 (0.80) | mmol/L |
| Erythrocytes | 4.2–5.4/4.6–6.2 | Tpt/L | 4.82 (0.41) | Tpt/L |
| Leukocytes | 4.3–10.0 | Gpt/L | 6.96 1.98) | Gpt/L |
| Lymphocytes abs. | −5.0 | Gpt/L | 1.98 (0.61) | Gpt/L |
| Thrombocytes | 140–440 | Gpt/L | 271.14 (61.82) | Gpt/L |
| CRP | <5 | mg/L | 7.23 (4.14) | mg/L |
| Vit. D | >30 | µg/L | 29.57 (16.77) | µg/L |
| ALAT | <0.77 | µkatal/L | 0.54 (0.28) | µkatal/L |
| ASAT | <0.59 | µkatal/L | 0.36 (0.28) | µkatal/L |
| Bilirubin | <17 | µmol/L | 8.41 (4.08) | µmol/L |
| Calcium | 2.12–2.52 | mmol/L | 2.38 (0.09) | mmol/L |
| Cholesterol | <6.0 | mmol/L | 5.72 (1.27) | mmol/L |
| Creatine kinase | <7.9 | µkatal/L | 1.75 (0.75) | µkatal/L |
| GGT | <0.96 | µkatal/L | 0.52 (1.62) | µkatal/L |
| Glucose | 3.9–6.4 | mmol/L | 5.66 (0.78) | mmol/L |
| HDL Cholesterol | >1.03 | mmol/L | 1.56 (0.46) | mmol/L |
| Uric acid | 155–428 | µmol/L | 289.00 (93.47) | µmol/L |
| Urea | 2.5–6.4 | mmol/L | 5.01 (1.18) | mmol/L |
| Potassium | 3.5–4.6 | mmol/L | 4.02 (0.30) | mmol/L |
| Creatinine | 42–97 | µmol/L | 67.52 (14.88) | µmol/L |
| LDL Cholesterol | <3.34 | mmol/L | 3.52 (1.10) | mmol/L |
| Lipase | 1.59–6.36 | µkatal/L | 2.36 (0.85) | µkatal/L |
| Sodium | 135–145 | mmol/L | 142.42 (2.48) | mmol/L |
| NT-proBNP | <125 | pg/mL | 80.41 (129.82) | pg/mL |
| Phosphate | 0.6–1.6 | mmol/L | 0.99 (0.16) | mmol/L |
| Triglycerides | <1.9 | mmol/L | 1.56 (0.97) | mmol/L |
| Hs cTroponin I | <59 | ng/L | 7.46 (5.81) | ng/L |
| TSH | 0.49–3.29 | mU/L | 1.51 (0.76) | mU/L |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steinmetz, A.; Gross, S.; Lehnert, K.; Lücker, P.; Friedrich, N.; Nauck, M.; Bahlmann, S.; Fielitz, J.; Dörr, M. Longitudinal Clinical Features of Post-COVID-19 Patients—Symptoms, Fatigue and Physical Function at 3- and 6-Month Follow-Up. J. Clin. Med. 2023, 12, 3966. https://doi.org/10.3390/jcm12123966
Steinmetz A, Gross S, Lehnert K, Lücker P, Friedrich N, Nauck M, Bahlmann S, Fielitz J, Dörr M. Longitudinal Clinical Features of Post-COVID-19 Patients—Symptoms, Fatigue and Physical Function at 3- and 6-Month Follow-Up. Journal of Clinical Medicine. 2023; 12(12):3966. https://doi.org/10.3390/jcm12123966
Chicago/Turabian StyleSteinmetz, Anke, Stefan Gross, Kristin Lehnert, Petra Lücker, Nele Friedrich, Matthias Nauck, Susanne Bahlmann, Jens Fielitz, and Marcus Dörr. 2023. "Longitudinal Clinical Features of Post-COVID-19 Patients—Symptoms, Fatigue and Physical Function at 3- and 6-Month Follow-Up" Journal of Clinical Medicine 12, no. 12: 3966. https://doi.org/10.3390/jcm12123966