
Manifestation of Headache Affecting Quality of Life in Long COVID Patients
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Methods
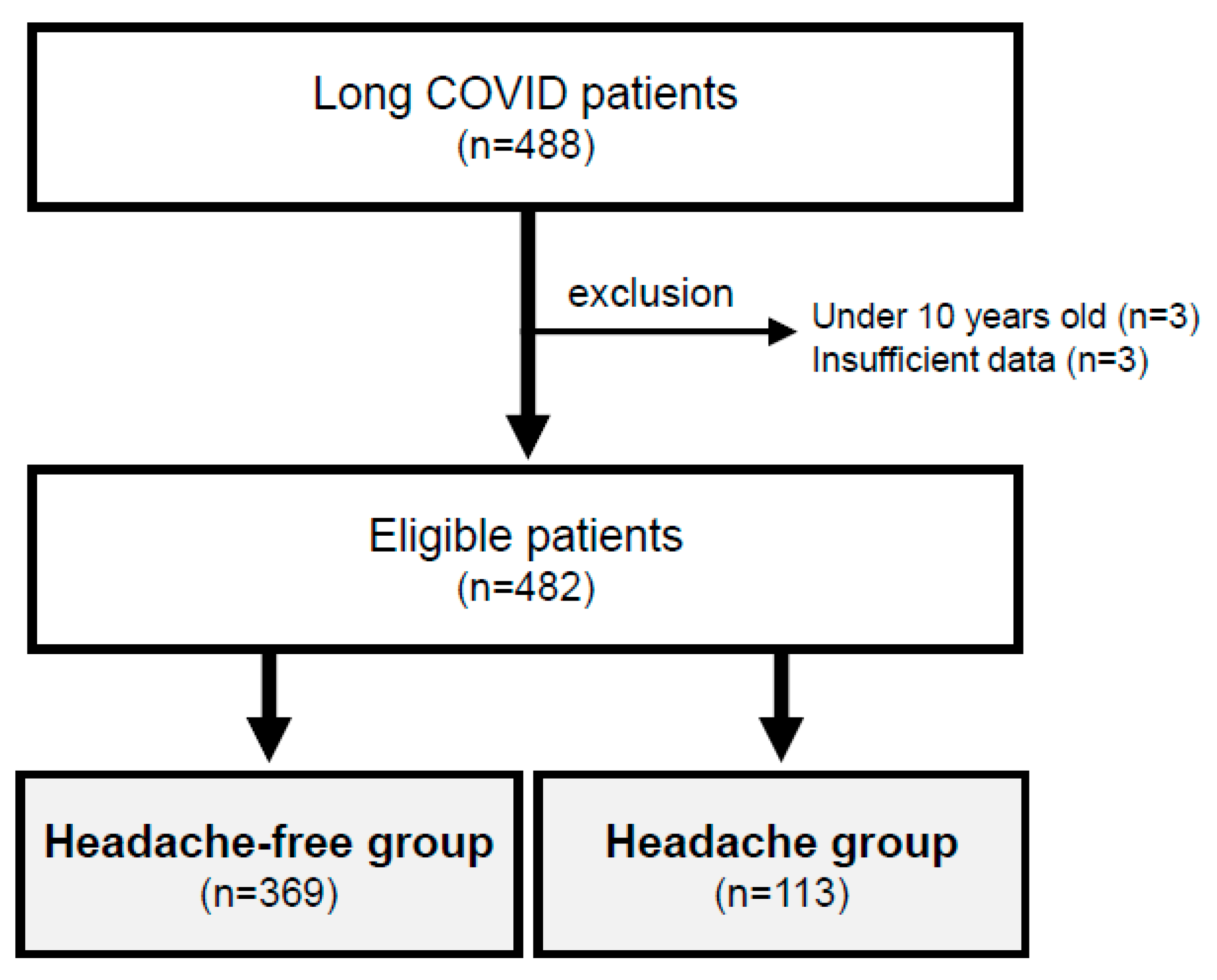
2.1. Study Design and Patients’ Characteristics
2.2. Blood Chemistry Examination
2.3. Definition of Self-Rating Scales
2.4. Statistical Analysis
2.5. Ethical Approval
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V.; on behalf of theWHO Clinical Case Definition Working Group on Post-COVID-19 Condition. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 2022, 22, e102–e107. [Google Scholar] [CrossRef]
- Ballering, A.V.; van Zon, S.K.R.; Olde Hartman, T.C.; Rosmalen, J.G.M. Persistence of somatic symptoms after COVID-19 in the Netherlands: An observational cohort study. Lancet 2022, 400, 452–461. [Google Scholar] [CrossRef] [PubMed]
- Sunada, N.; Honda, H.; Nakano, Y.; Yamamoto, K.; Tokumasu, K.; Sakurada, Y.; Matsuda, Y.; Hasegawa, T.; Otsuka, Y.; Obika, M.; et al. Hormonal trends in patients suffering from long COVID symptoms. Endocr. J. 2022, 69, 1173–1181. [Google Scholar] [CrossRef]
- Tokumasu, K.; Honda, H.; Sunada, N.; Sakurada, Y.; Matsuda, Y.; Yamamoto, K.; Nakano, Y.; Hasegawa, T.; Yamamoto, Y.; Otsuka, Y.; et al. Clinical Characteristics of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) Diagnosed in Patients with Long COVID. Medicina 2022, 58, 850. [Google Scholar] [CrossRef]
- Otsuka, Y.; Tokumasu, K.; Nakano, Y.; Honda, H.; Sakurada, Y.; Sunada, N.; Omura, D.; Hasegawa, K.; Hagiya, H.; Obika, M.; et al. Clinical Characteristics of Japanese Patients Who Visited a COVID-19 Aftercare Clinic for Post-Acute Sequelae of COVID-19/Long COVID. Cureus 2021, 13, e18568. [Google Scholar] [CrossRef]
- Sunada, N.; Nakano, Y.; Otsuka, Y.; Tokumasu, K.; Honda, H.; Sakurada, Y.; Matsuda, Y.; Hasegawa, T.; Omura, D.; Ochi, K.; et al. Characteristics of Sleep Disturbance in Patients with Long COVID: A Retrospective Observational Study in Japan. J. Clin. Med. 2022, 11, 7332. [Google Scholar] [CrossRef]
- Matsuda, Y.; Tokumasu, K.; Otsuka, Y.; Sunada, N.; Honda, H.; Sakurada, Y.; Nakano, Y.; Hasegawa, T.; Obika, M.; Ueda, K.; et al. Symptomatic Characteristics of Hypozincemia Detected in Long COVID Patients. J. Clin. Med. 2023, 12, 2062. [Google Scholar] [CrossRef]
- Nakano, Y.; Otsuka, Y.; Honda, H.; Sunada, N.; Tokumasu, K.; Sakurada, Y.; Matsuda, Y.; Hasegawa, T.; Ochi, K.; Hagiya, H.; et al. Transitional Changes in Fatigue-Related Symptoms Due to Long COVID: A Single-Center Retrospective Observational Study in Japan. Medicina 2022, 58, 1393. [Google Scholar] [CrossRef] [PubMed]
- Aparisi, A.; Ybarra-Falcon, C.; Iglesias-Echeverria, C.; Garcia-Gomez, M.; Marcos-Mangas, M.; Valle-Penacoba, G.; Carrasco-Moraleja, M.; Fernandez-de-Las-Penas, C.; Guerrero, A.L.; Garcia-Azorin, D. Cardio-Pulmonary Dysfunction Evaluation in Patients with Persistent Post-COVID-19 Headache. Int. J. Environ. Res. Public Health 2022, 19, 3961. [Google Scholar] [CrossRef]
- Sakurada, Y.; Otsuka, Y.; Tokumasu, K.; Sunada, N.; Honda, H.; Nakano, Y.; Matsuda, Y.; Hasegawa, T.; Ochi, K.; Hagiya, H.; et al. Trends in Long COVID Symptoms in Japanese Teenage Patients. Medicina 2023, 59, 261. [Google Scholar] [CrossRef] [PubMed]
- Tana, C.; Bentivegna, E.; Cho, S.J.; Harriott, A.M.; Garcia-Azorin, D.; Labastida-Ramirez, A.; Ornello, R.; Raffaelli, B.; Beltran, E.R.; Ruscheweyh, R.; et al. Long COVID headache. J. Headache Pain 2022, 23, 93. [Google Scholar] [CrossRef]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef] [PubMed]
- Mutiawati, E.; Kusuma, H.I.; Fahriani, M.; Harapan, H.; Syahrul, S.; Musadir, N. Headache in Post-COVID-19 Patients: Its Characteristics and Relationship with the Quality of Life. Medicina 2022, 58, 1500. [Google Scholar] [CrossRef] [PubMed]
- El-Tallawy, S.N.; Perglozzi, J.V.; Ahmed, R.S.; Kaki, A.M.; Nagiub, M.S.; LeQuang, J.K.; Hadarah, M.M. Pain Management in the Post-COVID Era-An Update: A Narrative Review. Pain Ther. 2023, 12, 423–448. [Google Scholar] [CrossRef]
- El-Tallawy, S.N.; Nalamasu, R.; Pergolizzi, J.V.; Gharibo, C. Pain Management During the COVID-19 Pandemic. Pain Ther. 2020, 9, 453–466. [Google Scholar] [CrossRef]
- Siso-Almirall, A.; Brito-Zeron, P.; Conangla Ferrin, L.; Kostov, B.; Moragas Moreno, A.; Mestres, J.; Sellares, J.; Galindo, G.; Morera, R.; Basora, J.; et al. Long Covid-19: Proposed Primary Care Clinical Guidelines for Diagnosis and Disease Management. Int. J. Environ. Res. Public Health 2021, 18, 4350. [Google Scholar] [CrossRef]
- Kato, Y. Case Management of COVID-19 (Secondary Version). JMA J. 2021, 4, 191–197. [Google Scholar] [CrossRef]
- Zung, W.W. A Self-Rating Depression Scale. Arch. Gen. Psychiatry 1965, 12, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Kusano, M.; Shimoyama, Y.; Sugimoto, S.; Kawamura, O.; Maeda, M.; Minashi, K.; Kuribayashi, S.; Higuchi, T.; Zai, H.; Ino, K.; et al. Development and evaluation of FSSG: Frequency scale for the symptoms of GERD. J. Gastroenterol. 2004, 39, 888–891. [Google Scholar] [CrossRef] [PubMed]
- De Vries, J.; Michielsen, H.; Van Heck, G.L.; Drent, M. Measuring fatigue in sarcoidosis: The Fatigue Assessment Scale (FAS). Br. J. Health Psychol. 2004, 9, 279–291. [Google Scholar] [CrossRef]
- Shiroiwa, T.; Ikeda, S.; Noto, S.; Igarashi, A.; Fukuda, T.; Saito, S.; Shimozuma, K. Comparison of Value Set Based on DCE and/or TTO Data: Scoring for EQ-5D-5L Health States in Japan. Value Health 2016, 19, 648–654. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, S.; Shiroiwa, T.; Igarashi, A.; Noto, S.; Fukuda, T.; Saito, S.; Shimozuma, K. Developing a Japanese version of the EQ-5D-5L value set. J. Natl. Inst. Public Health 2015, 64, 47–55. [Google Scholar]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef]
- Fernandez-de-Las-Penas, C.; Navarro-Santana, M.; Gomez-Mayordomo, V.; Cuadrado, M.L.; Garcia-Azorin, D.; Arendt-Nielsen, L.; Plaza-Manzano, G. Headache as an acute and post-COVID-19 symptom in COVID-19 survivors: A meta-analysis of the current literature. Eur. J. Neurol. 2021, 28, 3820–3825. [Google Scholar] [CrossRef]
- Martelletti, P.; Bentivegna, E.; Luciani, M.; Spuntarelli, V. Headache as a Prognostic Factor for COVID-19. Time to Re-evaluate. SN Compr. Clin. Med. 2020, 2, 2509–2510. [Google Scholar] [CrossRef] [PubMed]
- Pullen, M.F.; Skipper, C.P.; Hullsiek, K.H.; Bangdiwala, A.S.; Pastick, K.A.; Okafor, E.C.; Lofgren, S.M.; Rajasingham, R.; Engen, N.W.; Galdys, A.; et al. Symptoms of COVID-19 Outpatients in the United States. Open Forum. Infect. Dis. 2020, 7, ofaa271. [Google Scholar] [CrossRef] [PubMed]
- Al-Hashel, J.Y.; Abokalawa, F.; Alenzi, M.; Alroughani, R.; Ahmed, S.F. Coronavirus disease-19 and headache; impact on pre-existing and characteristics of de novo: A cross-sectional study. J. Headache Pain 2021, 22, 97. [Google Scholar] [CrossRef]
- Becker, W.J.; Findlay, T.; Moga, C.; Scott, N.A.; Harstall, C.; Taenzer, P. Guideline for primary care management of headache in adults. Can. Fam. Physician 2015, 61, 670–679. [Google Scholar]
- Dodick, D.W. Pearls: Headache. Semin. Neurol. 2010, 30, 74–81. [Google Scholar] [CrossRef]
- Mitsikostas, D.D.; Ashina, M.; Craven, A.; Diener, H.C.; Goadsby, P.J.; Ferrari, M.D.; Lampl, C.; Paemeleire, K.; Pascual, J.; Siva, A.; et al. European Headache Federation consensus on technical investigation for primary headache disorders. J. Headache Pain 2015, 17, 5. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Mattiuzzi, C.; Bovo, C.; Henry, B.M. Headache is an important symptom in patients with coronavirus disease 2019 (COVID-19). Diagnosis 2020, 7, 409–411. [Google Scholar] [CrossRef]
- Caronna, E.; Ballve, A.; Llaurado, A.; Gallardo, V.J.; Ariton, D.M.; Lallana, S.; Lopez Maza, S.; Olive Gadea, M.; Quibus, L.; Restrepo, J.L.; et al. Headache: A striking prodromal and persistent symptom, predictive of COVID-19 clinical evolution. Cephalalgia 2020, 40, 1410–1421. [Google Scholar] [CrossRef] [PubMed]
- Trigo, J.; Garcia-Azorin, D.; Planchuelo-Gomez, A.; Martinez-Pias, E.; Talavera, B.; Hernandez-Perez, I.; Valle-Penacoba, G.; Simon-Campo, P.; de Lera, M.; Chavarria-Miranda, A.; et al. Factors associated with the presence of headache in hospitalized COVID-19 patients and impact on prognosis: A retrospective cohort study. J. Headache Pain 2020, 21, 94. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Groups | Headache-Free Group (n = 369, 76.6%) | Headache Group (n = 113, 23.4%) | p Value |
|---|---|---|---|
| Age (years), median (IQR) | 42 (28–52) | 37 (22–45) | <0.01 ** |
| Height (cm), median (IQR) | 163.0 (155.8–170.4) | 163.7 (156.7–170.3) | 0.629 |
| Weight (kg), median (IQR) | 61.3 (52.5–72.2) | 61.8 (52.8–73.0) | 0.771 |
| BMI, median (IQR) | 22.6 (20.4–48.7) | 23.2 (20.5–26.5) | 0.619 |
| Gender | |||
| Female, n (%) | 199 (53.9%) | 63 (55.8%) | 0.816 |
| Male, n (%) | 170 (46.1%) | 50 (44.2%) | |
| Smoking habit, n (%) | 125 (33.9%) | 42 (37.2%) | 0.596 |
| Alcohol drinking habit, n (%) | 158 (42.8%) | 45 (39.8%) | 0.649 |
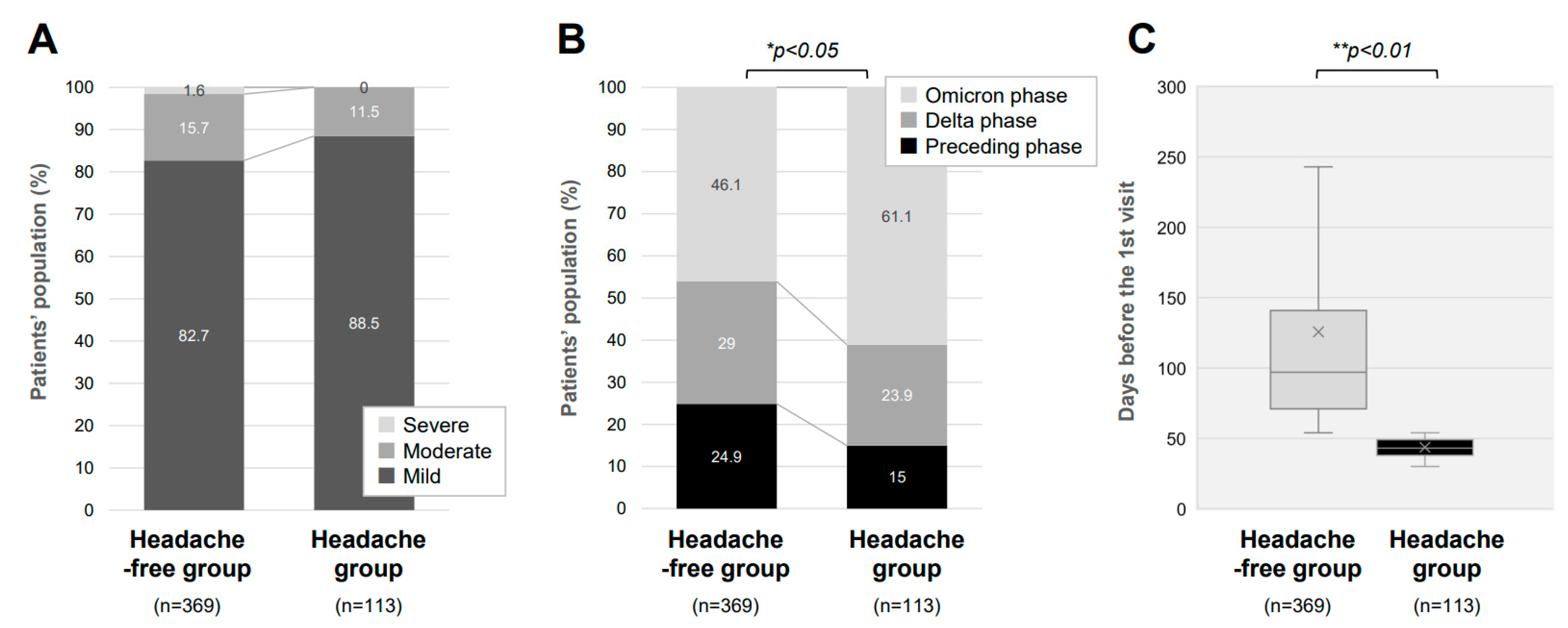
| Severity of COVID-19 | |||
| Mild, n (%) | 305 (82.7%) | 100 (88.5%) | 0.199 |
| Moderate, n (%) | 58 (15.7%) | 13 (11.5%) | |
| Severe, n (%) | 6 (1.6%) | 0 (0.0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fujita, K.; Otsuka, Y.; Sunada, N.; Honda, H.; Tokumasu, K.; Nakano, Y.; Sakurada, Y.; Obika, M.; Hagiya, H.; Otsuka, F. Manifestation of Headache Affecting Quality of Life in Long COVID Patients. J. Clin. Med. 2023, 12, 3533. https://doi.org/10.3390/jcm12103533
Fujita K, Otsuka Y, Sunada N, Honda H, Tokumasu K, Nakano Y, Sakurada Y, Obika M, Hagiya H, Otsuka F. Manifestation of Headache Affecting Quality of Life in Long COVID Patients. Journal of Clinical Medicine. 2023; 12(10):3533. https://doi.org/10.3390/jcm12103533
Chicago/Turabian StyleFujita, Kana, Yuki Otsuka, Naruhiko Sunada, Hiroyuki Honda, Kazuki Tokumasu, Yasuhiro Nakano, Yasue Sakurada, Mikako Obika, Hideharu Hagiya, and Fumio Otsuka. 2023. "Manifestation of Headache Affecting Quality of Life in Long COVID Patients" Journal of Clinical Medicine 12, no. 10: 3533. https://doi.org/10.3390/jcm12103533