
Anterior Quadratus Lumborum Block and Quadriceps Strength: A Prospective Cohort Study
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
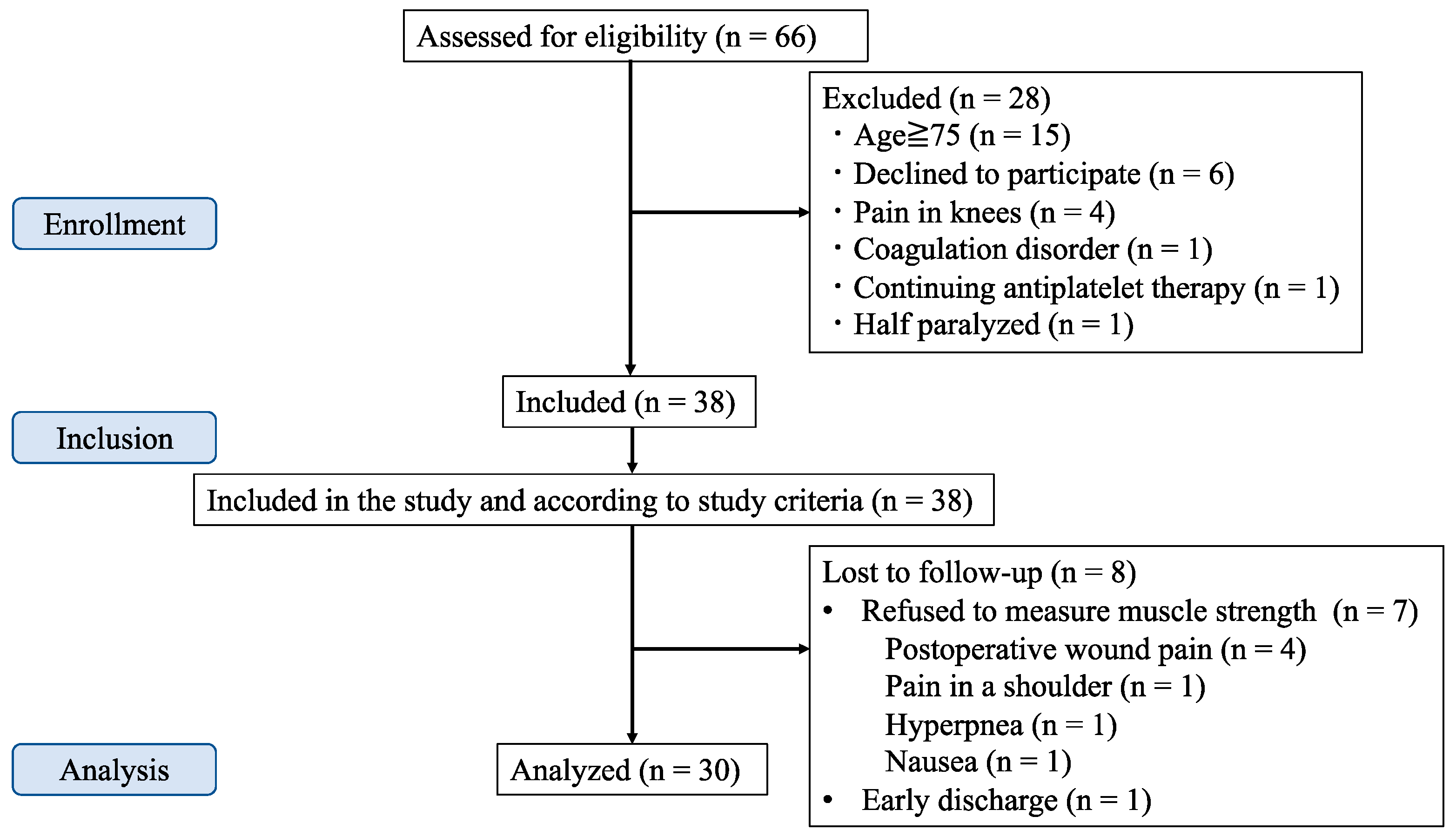
2.2. Participants
2.3. Intraoperative Management
2.4. Block Procedure
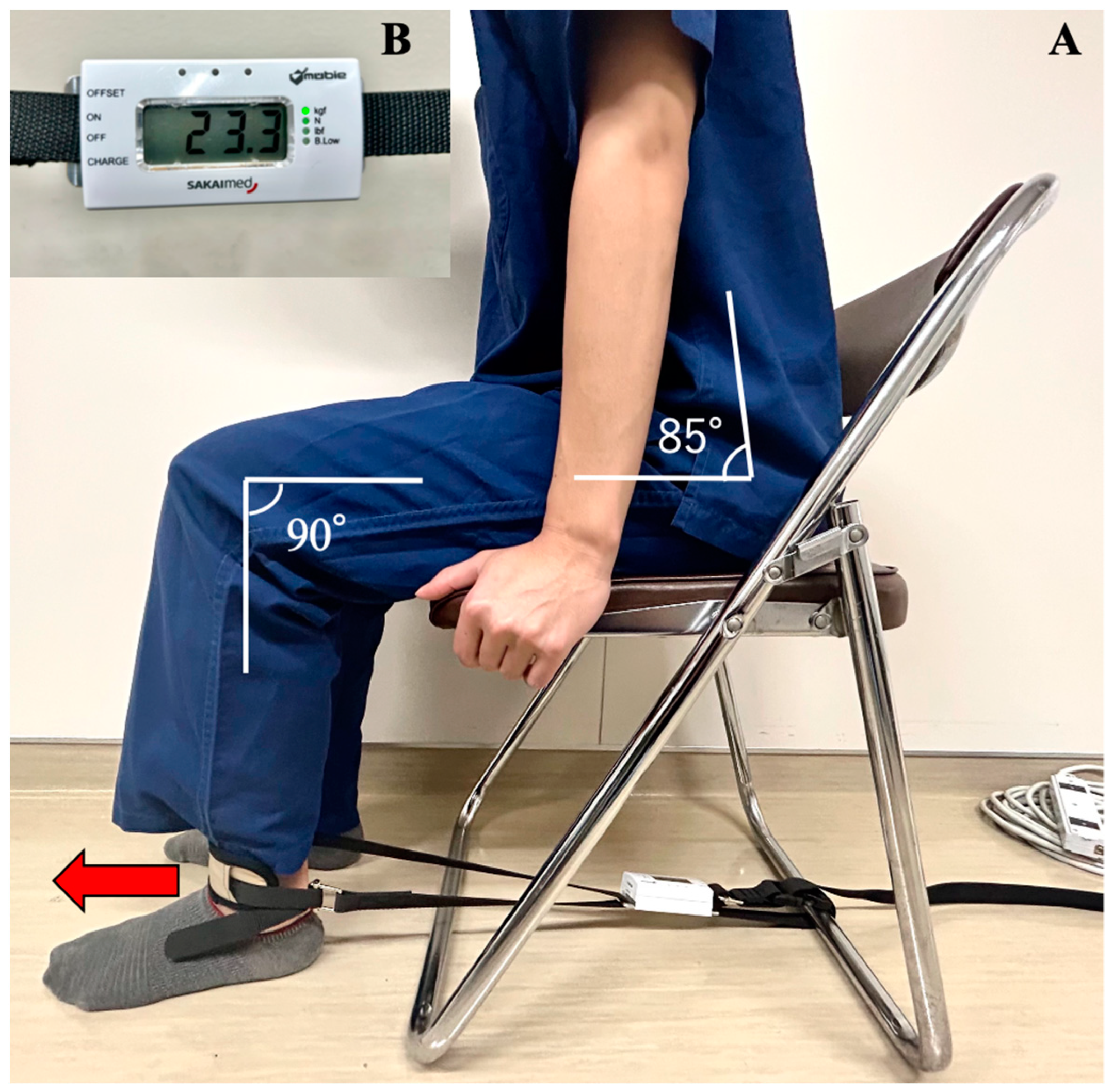
2.5. Measuring Muscle Strength
2.6. Sample Size Calculation
2.7. Statistical Methods
3. Results
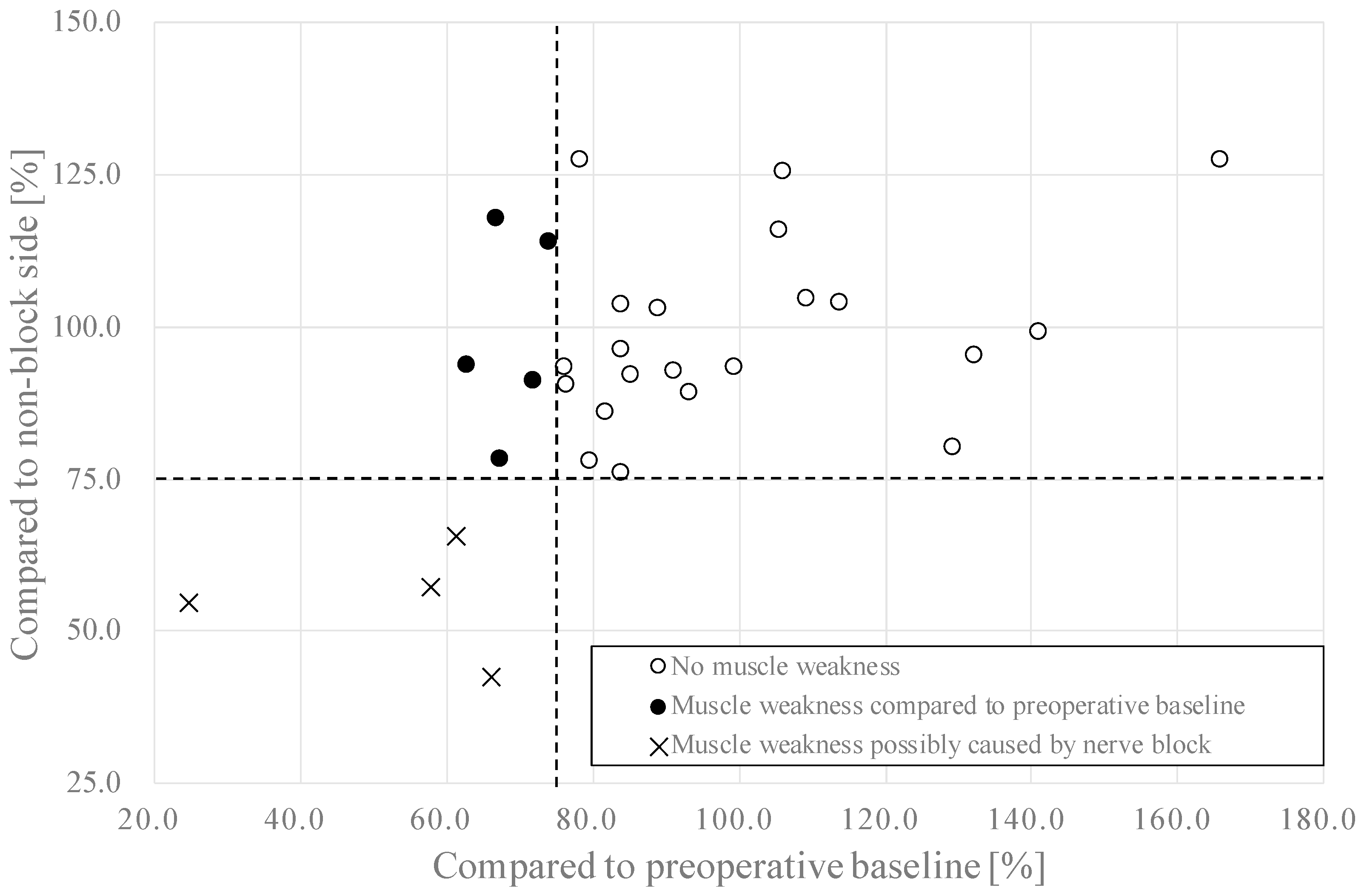
3.1. Muscle Strength
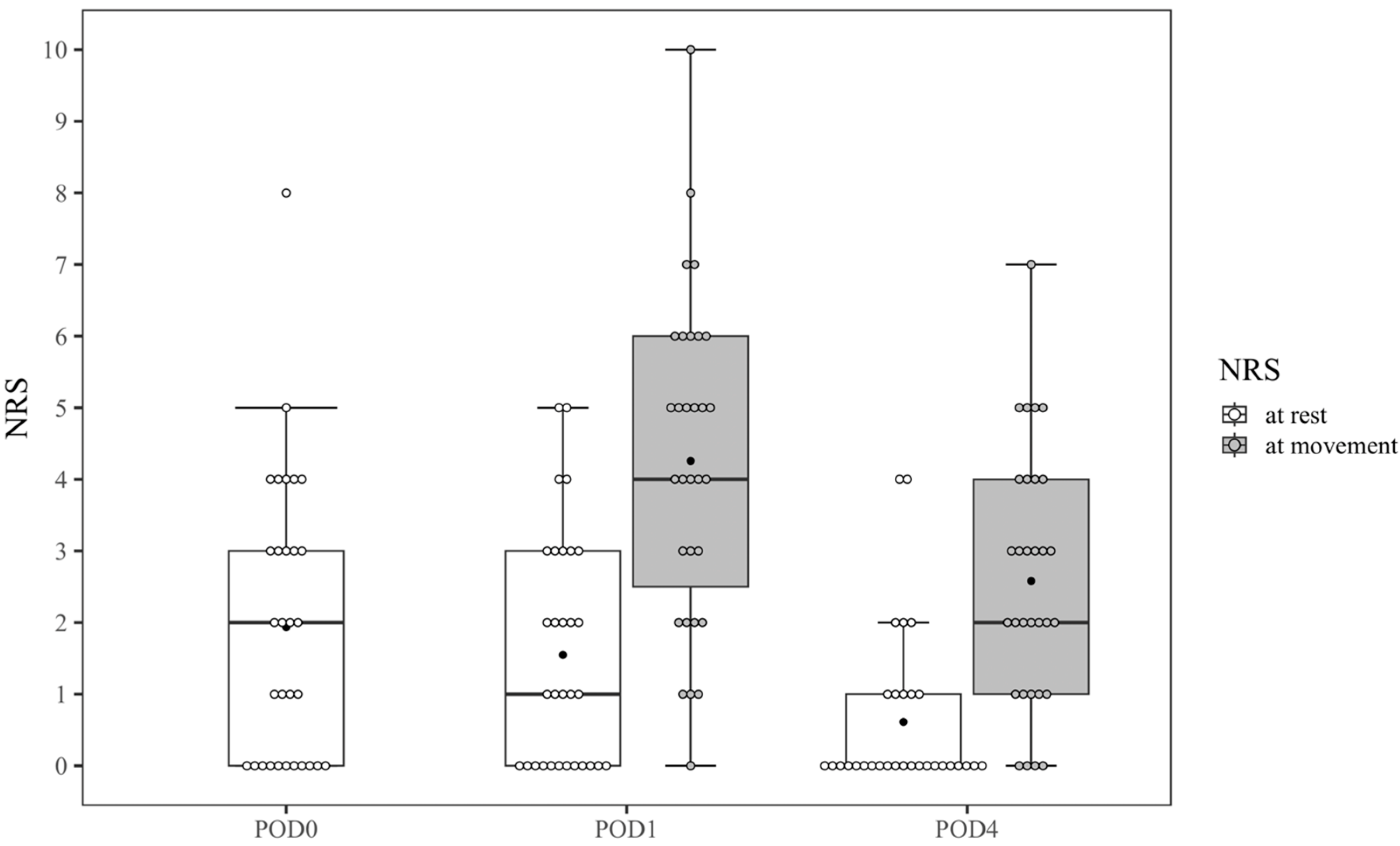
3.2. Postoperative Pain and Recovery
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alper, I.; Yüksel, E. Comparison of acute and chronic pain after open nephrectomy versus laparoscopic nephrectomy: A prospective clinical trial. Medicine 2016, 95, e3433. [Google Scholar] [CrossRef]
- Yuan, L.; Xu, C.; Zhang, Y.; Wang, G. Comparative efficacy analysis of ultrasound-guided quadratus lumborum block and lumbar plexus block in hip arthroscopy: A pilot prospective randomized controlled trial. J. Hip Preserv. Surg. 2022, 9, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-J.; Kim, H.-T.; Kim, H.-J.; Yoon, P.-W.; Park, J.-I.; Lee, S.-H.; Ro, Y.-J.; Koh, W.-U. Ultrasound-guided anterior quadratus lumborum block reduces postoperative opioid consumption and related side effects in patients undergoing total hip replacement arthroplasty: A propensity score-matched cohort study. J. Clin. Med. 2021, 10, 4632. [Google Scholar] [CrossRef]
- Ahmed, A.; Fawzy, M.; Nasr, M.A.R.; Hussam, A.M.; Fouad, E.; Aboeldahb, H.; Saad, D.; Osman, S.; Fahmy, R.S.; Farid, M.; et al. Ultrasound-guided quadratus lumborum block for postoperative pain control in patients undergoing unilateral inguinal hernia repair, a comparative study between two approaches. BMC Anesthesiol. 2019, 19, 184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, Y.; Zhang, J.; Xu, X.; Chen, W.; Zhang, S.; Zheng, H.; Xia, Y.; Papadimos, T.J.; Xu, X.; Chen, H. Sensory assessment and block duration of transmuscular quadratus lumborum block at L2 versus L4 in volunteers: A randomized controlled trial. Minerva Anestesiol. 2019, 85, 1273–1280. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Huang, M.; Zhong, Q.; Ni, H.; Yu, Z.; Zhang, X. Analgesic effect of ultrasound-guided anterior quadratus lumborum block at the L2 level in patients undergoing laparoscopic partial nephrectomy: A single-center, randomized controlled trial. Pain Res. Manag. 2022, 2022, 8958859. [Google Scholar] [CrossRef]
- Wikner, M. Unexpected motor weakness following quadratus lumborum block for gynaecological laparoscopy. Anaesthesia 2017, 72, 230–232. [Google Scholar] [CrossRef] [Green Version]
- Shi, R.; Li, H.; Wang, Y. Dermatomal coverage of single-injection ultrasound-guided parasagittal approach to anterior quadratus lumborum block at the lateral supra-arcuate ligament. J. Anesth. 2021, 35, 307–310. [Google Scholar] [CrossRef]
- Nassar, H.; Hasanin, A.; Sewilam, M.; Ahmed, H.; Abo-Elsoud, M.; Taalab, O.; Rady, A.; Zoheir, H.A. Transmuscular quadratus lumborum block versus suprainguinal fascia iliaca block for hip arthroplasty: A randomized, controlled pilot study. Local Reg. Anesth. 2021, 14, 67–74. [Google Scholar] [CrossRef]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13 (Suppl. 1), S31–S34. [Google Scholar] [CrossRef]
- Dam, M.; Moriggl, B.; Hansen, C.K.; Hoermann, R.; Bendtsen, T.F.; Børglum, J. The pathway of injectate spread with the transmuscular quadratus lumborum block: A cadaver study. Anesth. Analg. 2017, 125, 303–312. [Google Scholar] [CrossRef]
- Gerbershagen, H.J.; Rothaug, J.; Kalkman, C.J.; Meissner, W. Determination of moderate-to-severe postoperative pain on the numeric rating scale: A cut-off point analysis applying four different methods. Br. J. Anaesth. 2011, 107, 619–626. [Google Scholar] [CrossRef] [Green Version]
- Campfort, M.; Cayla, C.; Lasocki, S.; Rineau, E.; Léger, M. Early quality of recovery according to QoR-15 score is associated with one-month postoperative complications after elective surgery. J. Clin. Anesth. 2022, 78, 110638. [Google Scholar] [CrossRef]
- Nakatani, S.; Ida, M.; Tanaka, Y.; Okamoto, N.; Wang, X.; Nakatani, H.; Sato, M.; Naito, Y.; Kawaguchi, M. Translation and validation of the Japanese version of the Quality of Recovery-15 questionnaire. J. Anesth. 2021, 35, 426–433. [Google Scholar] [CrossRef]
- Henshaw, D.S.; Jaffe, J.D.; Reynolds, J.W.; Dobson, S.; Russell, G.B.; Weller, R.S. An evaluation of ultrasound-guided adductor canal blockade for postoperative analgesia after medial unicondylar knee arthroplasty. Anesth. Analg. 2016, 122, 1192–1201. [Google Scholar] [CrossRef]
- Blanco, R.; Ansari, T.; Girgis, E. Quadratus lumborum block for postoperative pain after caesarean section: A randomised controlled trial. Eur. J. Anaesthesiol. 2015, 32, 812–818. [Google Scholar] [CrossRef]
- Adhikary, S.D.; El-Boghdadly, K.; Nasralah, Z.; Sarwani, N.; Nixon, A.M.; Chin, K.J. A radiologic and anatomic assessment of injectate spread following transmuscular quadratus lumborum block in cadavers. Anaesthesia 2017, 72, 73–79. [Google Scholar] [CrossRef]
- Wardhan, R.; Auroux, A.-S.M.; Ben-David, B.; Chelly, J.E. Is L2 paravertebral block comparable to lumbar plexus block for postoperative analgesia after total hip arthroplasty? Clin. Orthop. Relat. Res. 2014, 472, 1475–1481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carline, L.; McLeod, G.A.; Lamb, C. A cadaver study comparing spread of dye and nerve involvement after three different quadratus lumborum blocks. Br. J. Anaesth. 2016, 117, 387–394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Menezes, T.C.; Bassi, D.; Cavalcanti, R.C.; Barros, J.E.S.L.; Granja, K.S.B.; Calles, A.C.D.N.; Exel, A.L. Comparisons and correlations of pain intensity and respiratory and peripheral muscle strength in the pre- and postoperative periods of cardiac surgery. Rev. Bras. Ter. Intensiv. 2018, 30, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Lachmann, G.; Mörgeli, R.; Kuenz, S.; Piper, S.K.; Spies, C.; Kurpanik, M.; Weber-Carstens, S.; Wollersheim, T. Perioperatively acquired weakness. Anesth. Analg. 2020, 130, 341–351. [Google Scholar] [CrossRef] [PubMed]
- Edwards, H. Postoperative deterioration in muscular function. Arch. Surg. 1982, 117, 899–901. [Google Scholar] [CrossRef]
- Zeiderman, M.R.; Welchew, E.A.; Clark, R.G. Changes in cardiorespiratory and muscle function associated with the development of postoperative fatigue. Br. J. Surg. 2005, 77, 576–580. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, A. Muscle power after surgery. Lancet 1980, 315, 420–421. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.; Thurairaja, R.; Johnson, C.D.; Primrose, J.N. Body composition, muscle function and psychological changes in patients undergoing operation for hepatic or pancreatic disease. Pancreatology 2001, 1, 90–95. [Google Scholar] [CrossRef]
- Jæger, P.; Zaric, D.; Fomsgaard, J.S.; Hilsted, K.L.; Bjerregaard, J.; Gyrn, J.; Mathiesen, O.; Larsen, T.K.; Dahl, J.B. Adductor canal block versus femoral nerve block for analgesia after total knee arthroplasty: A randomized, double-blind study. Reg. Anesth. Pain Med. 2013, 38, 526–532. [Google Scholar] [CrossRef] [Green Version]
- Murphy, G.S.; Szokol, J.W.; Marymont, J.H.; Greenberg, S.B.; Avram, M.J.; Vender, J.S. Residual neuromuscular blockade and critical respiratory events in the postanesthesia care unit. Anesth. Analg. 2008, 107, 130–137. [Google Scholar] [CrossRef]
- Krishnan, C.; Williams, G.N. Evoked tetanic torque and activation level explain strength differences by side. Eur. J. Appl. Physiol. 2009, 106, 769–774. [Google Scholar] [CrossRef] [Green Version]
- Dam, M.; Hansen, C.; Poulsen, T.D.; Azawi, N.H.; Laier, G.H.; Wolmarans, M.; Chan, V.; Bendtsen, T.F.; Børglum, J. Transmuscular quadratus lumborum block reduces opioid consumption and prolongs time to first opioid demand after laparoscopic nephrectomy. Reg. Anesth. Pain Med. 2021, 46, 18–24. [Google Scholar] [CrossRef]
- Guo, M.; Lei, B.; Li, H.; Gao, X.; Zhang, T.; Liang, Z.; Wang, Y.; Wang, L. Anterior quadratus lumborum block at the lateral supra-arcuate ligament versus transmuscular quadratus lumborum block for analgesia after elective cesarean section: A randomized controlled trial. J. Clin. Med. 2022, 11, 3827. [Google Scholar] [CrossRef]
- Blanco, R. Tap block under ultrasound guidance: The description of a ”non pops” technique. Reg. Anesth. Pain Med. 2007, 32, 130. [Google Scholar] [CrossRef]
- Kim, S.H.; Kim, H.J.; Kim, N.; Lee, B.; Song, J.; Choi, Y.S. Effectiveness of quadratus lumborum block for postoperative pain: A systematic review and meta-analysis. Minerva Anestesiol. 2020, 86, 554–564. [Google Scholar] [CrossRef] [PubMed]
- Shao, L.; Luo, X.; Ye, Y.; Liu, L.; Cai, Y.; Xia, Y.; Papadimos, T.J.; Wang, Q.; Pan, L. Anterior Quadratus Lumborum block area comparison in the three different volumes of Ropivacaine: A double-blind, randomized controlled trial in healthy volunteers. BMC Anesthesiol. 2022, 29, 365. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No-Muscle Weakness Group (n = 21) | Muscle Weakness Group (n = 9) | p-Value | |
|---|---|---|---|
| Sex | 0.10 | ||
| Male | 14 (66.7%) | 3 (33%) | |
| Female | 7 (33.3%) | 6 (67%) | |
| Age (years) | 64.0 [38, 75] | 67.0 [53, 74] | 0.70 |
| BMI (kg/m2) | 24.2 [18.4, 31.8] | 22.1 [21.6, 29.1] | 0.39 |
| ASA-PS | 0.08 | ||
| 1 | 0 (0%) | 2 (22%) | |
| 2 | 21 (100%) | 7 (78%) | |
| 3 | 0 (0%) | 0 (0%) | |
| 4 | 0 (0%) | 0 (0%) |
| No-Muscle Weakness Group (n = 21) | Muscle Weakness Group (n = 9) | p-Value | |
|---|---|---|---|
| Surgical approach | 1.00 | ||
| Posterior | 11 (52.3%) | 5 (56%) | |
| Anterior | 10 (47.6%) | 4 (44%) | |
| Ureteral catheter | 0.68 | ||
| With catheter | 14 (66.7%) | 7 (78%) | |
| No catheter | 7 (33.3%) | 2 (22%) | |
| Duration of surgery (min) | 196 [94, 301] | 229 [131, 269] | 0.39 |
| Muscle strength (kgf) | |||
| Block side | |||
| POD 0 | 17.8 [6.2, 36.8] | 16.7 [10.9–31.4] | 0.71 |
| POD 1 | 18.9 [8.4, 35.2] | 12.4 [3.0–21.2] | 0.03 |
| POD 4 | 19.1 [10.0, 42.5] | 14.5 [9.1–32.0] | 0.20 |
| Non-block side | |||
| POD 0 | 20.8 [6.0, 35.5] | 16.4 [10.6–33.2] | 0.59 |
| POD 1 | 20.3 [6.6, 38.6] | 15.6 [5.5–27.1] | 0.20 |
| POD 4 | 15 [9.1, 36.0] | 13.1 [10.2–27.0] | 0.39 |
| NRS scores at rest | |||
| 2 h after surgery | 1 [0, 4] | 3 [0, 8] | 0.02 |
| POD 1 | 1 [0, 5] | 2 [0, 4] | 0.80 |
| POD 4 | 0 [0, 4] | 0 [0, 4] | 0.42 |
| NRS scores at movement | |||
| POD1 | 4.5 [0, 10] | 5 [3, 6] | 0.73 |
| POD4 | 2 [0, 5] | 4 [0, 7] | 0.13 |
| QoR-15 | |||
| Preoperative | 148 [117, 150] | 147 [138, 150] | 0.20 |
| POD 1 | 120 [43, 150] | 109 [59, 137] | 0.22 |
| POD 4 | 138 [108, 149] | 138 [88, 143] | 0.44 |
| No-Muscle Weakness Group | Muscle Weakness Group | All (n = 30) | ||
|---|---|---|---|---|
| POD 1 | NRS ≥ 4 | 13 (65.0%) | 7 (35.0%) | 20 |
| NRS < 4 | 8 (80.0%) | 2 (20.0%) | 10 | |
| RR | 1.75 (0.44–6.93) | |||
| POD 4 | NRS ≥ 4 | 6 (66.7%) | 3 (33.3%) | 9 |
| NRS < 4 | 18 (85.7%) | 3 (14.2%) | 21 | |
| RR | 2.33 (0.58–9.43) | |||
| POD 1 | QoR-15 < 122 | 11 (61.1%) | 7 (38.8%) | 18 |
| QoR-15 ≥ 122 | 10 (83.3%) | 2 (16.7%) | 12 | |
| RR | 2.33 (0.58–9.38) | |||
| POD 4 | QoR-15 < 122 | 2 (50%) | 2 (50%) | 4 |
| QoR-15 ≥ 122 | 22 (84.6%) | 4 (66.7%) | 26 | |
| RR | 3.25 (0.86–12.31) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kadoya, Y.; Tanaka, N.; Suzuka, T.; Yamanaka, T.; Iwata, M.; Ozu, N.; Kawaguchi, M. Anterior Quadratus Lumborum Block and Quadriceps Strength: A Prospective Cohort Study. J. Clin. Med. 2023, 12, 3837. https://doi.org/10.3390/jcm12113837
Kadoya Y, Tanaka N, Suzuka T, Yamanaka T, Iwata M, Ozu N, Kawaguchi M. Anterior Quadratus Lumborum Block and Quadriceps Strength: A Prospective Cohort Study. Journal of Clinical Medicine. 2023; 12(11):3837. https://doi.org/10.3390/jcm12113837
Chicago/Turabian StyleKadoya, Yuma, Nobuhiro Tanaka, Takanori Suzuka, Takayuki Yamanaka, Masato Iwata, Naoki Ozu, and Masahiko Kawaguchi. 2023. "Anterior Quadratus Lumborum Block and Quadriceps Strength: A Prospective Cohort Study" Journal of Clinical Medicine 12, no. 11: 3837. https://doi.org/10.3390/jcm12113837