
General versus Neuraxial Anesthesia on Clinical Outcomes in Patients Receiving Hip Fracture Surgery: An Analysis of the ACS NSQIP Database
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Population Selection and Clinical Characteristics
2.3. Study Outcomes
2.4. Statistical Analysis
3. Results
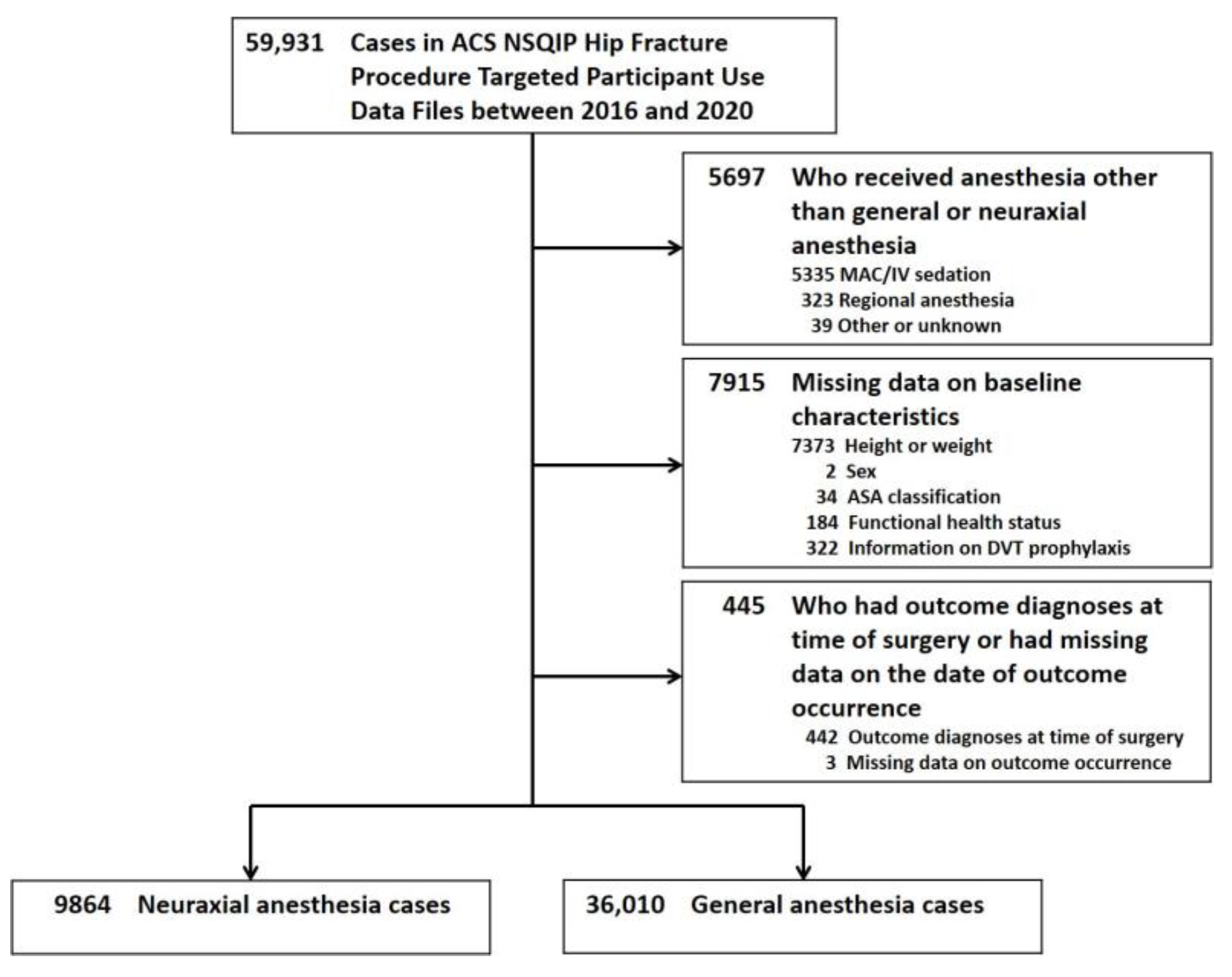
3.1. Study Sample Selection
3.2. Baseline Characteristics
3.3. Associations between General Anesthesia and Postoperative Adverse Events
3.3.1. Unweighted Multivariable Analysis
3.3.2. Multivariable Analysis after IPTW
3.3.3. Propensity Score-Matched Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cooper, C.; Cole, Z.A.; Holroyd, C.R.; Earl, S.C.; Harvey, N.C.; Dennison, E.M.; Melton, L.J.; Cummings, S.R.; Kanis, J.A.; IOF CSA Working Group on Fracture Epidemiology. Secular trends in the incidence of hip and other osteoporotic fractures. Osteoporos. Int. 2011, 22, 1277–1288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, S.D.; Rothbaum, R.R.; Kiel, D.P.; Lee, Y.; Mitchell, S.L. Association of clinical outcomes with surgical repair of hip fracture vs nonsurgical management in nursing home residents with advanced dementia. JAMA Intern. Med. 2018, 178, 774–780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhandari, M.; Swiontkowski, M. Management of acute hip fracture. N. Engl. J. Med. 2017, 377, 2053–2062. [Google Scholar] [CrossRef] [PubMed]
- Schattner, A. The burden of hip fractures-why aren’t we better at prevention? QJM 2018, 111, 765–767. [Google Scholar] [CrossRef] [PubMed]
- HIP ATTACK Investigators. Accelerated surgery versus standard care in hip fracture (HIP ATTACK): An international, randomised, controlled trial. Lancet 2020, 395, 698–708. [Google Scholar] [CrossRef] [PubMed]
- Reguant, F.; Arnau, A.; Lorente, J.V.; Maestro, L.; Bosch, J. Efficacy of a multidisciplinary approach on postoperative morbidity and mortality of elderly patients with hip fracture. J. Clin. Anesth. 2019, 53, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Neuman, M.D.; Feng, R.; Carson, J.L.; Gaskins, L.J.; Dillane, D.; Sessler, D.I.; Sieber, F.; Magaziner, J.; Marcantonio, E.R.; Mehta, S.; et al. Spinal anesthesia or general anesthesia for hip surgery in older adults. N. Engl. J. Med. 2021, 385, 2025–2035. [Google Scholar] [CrossRef]
- Chen, D.X.; Yang, L.; Ding, L.; Li, S.Y.; Qi, Y.N.; Li, Q. Perioperative outcomes in geriatric patients undergoing hip fracture surgery with different anesthesia techniques: A systematic review and meta-analysis. Medicine 2019, 98, e18220. [Google Scholar] [CrossRef] [Green Version]
- O’Donnell, C.M.; McLoughlin, L.; Patterson, C.C.; Clarke, M.; McCourt, K.C.; McBrien, M.E.; McAuley, D.F.; Shields, M.O. Perioperative outcomes in the context of mode of anaesthesia for patients undergoing hip fracture surgery: Systematic review and meta-analysis. Br. J. Anaesth. 2018, 120, 37–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American College of Surgeons. ACS National Surgical Quality Improvement Program. Available online: https://www.facs.org/quality-programs/acs-nsqip (accessed on 18 March 2023).
- Shiloach, M.; Frencher, S.K., Jr.; Steeger, J.E.; Rowell, K.S.; Bartzokis, K.; Tomeh, M.G.; Richards, K.E.; Ko, C.Y.; Hall, B.L. Toward robust information: Data quality and inter-rater reliability in the American College of Surgeons National Surgical Quality Improvement Program. J. Am. Coll. Surg. 2010, 210, 6–16. [Google Scholar] [CrossRef] [PubMed]
- Basques, B.A.; Bohl, D.D.; Golinvaux, N.S.; Samuel, A.M.; Grauer, J.G. General versus spinal anaesthesia for patients aged 70 years and older with a fracture of the hip. Bone Jt. J. 2015, 97, 689–695. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. The performance of different propensity-score methods for estimating differences in proportions (risk differences or absolute risk reductions) in observational studies. Stat. Med. 2010, 29, 2137–2148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Austin, P.C. An Introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, X.; Tan, Y.; Gao, Y.; Liu, Z. Comparative efficacy of neuraxial and general anesthesia for hip fracture surgery: A meta-analysis of randomized clinical trials. BMC Anesthesiol. 2020, 20, 162. [Google Scholar] [CrossRef]
- Durand, W.M.; Goodman, A.D.; Johnson, J.P.; Daniels, A.H. Assessment of 30-day mortality and complication rates associated with extended deep vein thrombosis prophylaxis following hip fracture surgery. Injury 2018, 49, 1141–1148. [Google Scholar] [CrossRef] [PubMed]
- Ahn, E.J.; Kim, H.J.; Kim, K.W.; Choi, H.R.; Kang, H.; Bang, S.R. Comparison of general anaesthesia and regional anaesthesia in terms of mortality and complications in elderly patients with hip fracture: A nationwide population-based study. BMJ Open 2019, 9, e029245. [Google Scholar] [CrossRef] [Green Version]
- Biboulet, P.; Jourdan, A.; Van Haevre, V.; Morau, D.; Bernard, N.; Bringuier, S.; Capdevila, X. Hemodynamic profile of target-controlled spinal anesthesia compared with 2 target-controlled general anesthesia techniques in elderly patients with cardiac comorbidities. Reg. Anesth. Pain Med. 2012, 37, 433–440. [Google Scholar] [CrossRef]
- Parker, M.J.; Griffiths, R. General versus regional anaesthesia for hip fractures. A pilot randomised controlled trial of 322 patients. Injury 2015, 46, 1562–1566. [Google Scholar] [CrossRef]
- O’Hara, D.A.; Duff, A.; Berlin, J.A.; Poses, R.M.; Lawrence, V.A.; Huber, E.C.; Noveck, H.; Strom, B.L.; Carson, J.L. The effect of anesthetic technique on postoperative outcomes in hip fracture repair. Anesthesiology 2000, 92, 947–957. [Google Scholar] [CrossRef]
- Neuman, M.D.; Rosenbaum, P.R.; Ludwig, J.M.; Zubizarreta, J.R.; Silber, J.H. Anesthesia technique, mortality, and length of stay after hip fracture surgery. JAMA 2014, 311, 2508–2517. [Google Scholar] [CrossRef]
- Seitz, D.P.; Gill, S.S.; Bell, C.M.; Austin, P.C.; Gruneir, A.; Anderson, G.M.; Rochon, P.A. Postoperative medical complications associated with anesthesia in older adults with dementia. J. Am. Geriatr. Soc. 2014, 62, 2102–2109. [Google Scholar] [CrossRef] [PubMed]
- Tung, Y.C.; Hsu, Y.H.; Chang, G.M. The effect of anesthetic type on outcomes of hip fracture surgery: A nationwide population-based study. Medicine 2016, 95, e3296. [Google Scholar] [CrossRef] [PubMed]
- Morgan, L.; McKeever, T.M.; Nightingale, J.; Deakin, D.E.; Moppett, I.K. Spinal or general anaesthesia for surgical repair of hip fracture and subsequent risk of mortality and morbidity: A database analysis using propensity score-matching. Anaesthesia 2020, 75, 1173–1179. [Google Scholar] [CrossRef] [PubMed]
- Neuman, M.D.; Silber, J.H.; Elkassabany, N.M.; Ludwig, J.M.; Fleisher, L.A. Comparative effectiveness of regional versus general anesthesia for hip fracture surgery in adults. Anesthesiology 2012, 117, 72–92. [Google Scholar] [CrossRef] [Green Version]
- Fields, A.C.; Dieterich, J.D.; Buterbaugh, K.; Moucha, C.S. Short-term complications in hip fracture surgery using spinal versus general anaesthesia. Injury 2015, 46, 719–723. [Google Scholar] [CrossRef]
- Chang, C.C.; Lin, H.C.; Lin, H.W.; Lin, H.C. Anesthetic management and surgical site infections in total hip or knee replacement: A population-based study. Anesthesiology 2010, 113, 279–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, K.; Zhang, J.; Li, J.; Meng, H.; Hou, Z.; Zhang, Y. Incidence of and risk factors for new-onset deep venous thrombosis after intertrochanteric fracture surgery. Sci. Rep. 2021, 11, 17319. [Google Scholar] [CrossRef] [PubMed]
- Davis, F.M.; Quince, M.; Laurenson, V.G. Deep vein thrombosis and anaesthetic technique in emergency hip surgery. Br. Med. J. 1980, 281, 1528–1529. [Google Scholar] [CrossRef] [Green Version]
- Guay, J.; Parker, M.J.; Gajendragadkar, P.R.; Kopp, S. Anaesthesia for hip fracture surgery in adults. Cochrane Database Syst. Rev. 2016, 2, CD000521. [Google Scholar] [CrossRef]


{kind=link}
| Unweighted Study Population | After IPTW | |||||
|---|---|---|---|---|---|---|
| Neuraxial Anesthesia | General Anesthesia | Neuraxial Anesthesia | General Anesthesia | |||
| (n = 9864) | (n = 36,010) | |||||
| Characteristics | Number (Percent of Patients) | SMD * | Percent of Patients | SMD * | ||
| Demographics | ||||||
| Age, years | ||||||
| <65 | 741 (7.5) | 4422 (12.3) | 0.160 | 12.3 | 11.3 | 0.033 |
| 65–74 | 1410 (14.3) | 6407 (17.8) | 0.095 | 16.8 | 17.0 | 0.007 |
| 75–84 | 3079 (31.2) | 10,725 (29.8) | 0.031 | 29.4 | 30.0 | 0.014 |
| ≥85 | 4634 (47.0) | 14,456 (40.1) | 0.138 | 41.6 | 41.7 | 0.002 |
| Sex | ||||||
| Female | 6974 (70.7) | 24,277 (67.4) | 0.071 | 68.1 | 68.1 | 0.002 |
| Male | 2890 (29.3) | 11,733 (32.6) | 0.071 | 32.0 | 31.9 | 0.002 |
| Race/ethnicity | ||||||
| White | 4807 (48.7) | 28,447 (79.0) | 0.664 | 72.7 | 72.5 | 0.003 |
| Other | 5057 (51.3) | 7563 (21.0) | 0.664 | 27.4 | 27.5 | 0.003 |
| Body mass index | ||||||
| Normal | 4938 (50.1) | 16,375 (45.5) | 0.092 | 46.7 | 46.5 | 0.005 |
| Underweight | 926 (9.4) | 2803 (7.8) | 0.057 | 8.1 | 8.1 | 0.001 |
| Overweight | 2667 (27.0) | 10,472 (29.1) | 0.045 | 28.4 | 28.6 | 0.004 |
| Obese | 1333 (13.5) | 6360 (17.7) | 0.115 | 16.8 | 16.8 | 0.001 |
| Functional health status | ||||||
| Independent | 7827 (79.4) | 28,302 (78.6) | 0.019 | 78.3 | 78.8 | 0.011 |
| Partially dependent | 1770 (17.9) | 6764 (18.8) | 0.022 | 19.1 | 18.6 | 0.012 |
| Totally dependent | 267 (2.7) | 944 (2.6) | 0.005 | 2.6 | 2.6 | 0.002 |
| Comorbidities | ||||||
| Smoking | 1074 (10.9) | 4585 (12.7) | 0.057 | 12.7 | 12.3 | 0.011 |
| Diabetes mellitus | 1652 (16.8) | 6986 (19.4) | 0.069 | 19.3 | 18.9 | 0.012 |
| Hypertension | 6166 (62.5) | 24,144 (67.1) | 0.095 | 66.6 | 66.2 | 0.009 |
| Congestive heart failure | 297 (3.0) | 1334 (3.7) | 0.039 | 3.4 | 3.6 | 0.007 |
| COPD | 1120 (11.4) | 3745 (10.4) | 0.031 | 10.8 | 10.6 | 0.007 |
| Dialysis | 130 (1.3) | 786 (2.2) | 0.066 | 2.4 | 2.0 | 0.028 |
| Dementia | 2741 (27.8) | 9501 (26.4) | 0.032 | 26.9 | 26.7 | 0.004 |
| Disseminated cancer | 279 (2.8) | 1306 (3.6) | 0.045 | 3.6 | 3.5 | 0.008 |
| Bleeding disorder | 684 (6.9) | 6884 (19.1) | 0.368 | 16.1 | 16.5 | 0.013 |
| Operative information | ||||||
| Type of fracture | ||||||
| Femoral neck fracture | 4075 (41.3) | 13,572 (37.7) | 0.074 | 38.0 | 38.4 | 0.008 |
| Intertrochanteric | 5009 (50.8) | 19,393 (53.9) | 0.062 | 53.5 | 53.3 | 0.005 |
| Subtrochanteric/other | 780 (7.9) | 3045 (8.5) | 0.020 | 8.5 | 8.3 | 0.005 |
| ASA classification | ||||||
| I or II | 1888 (19.1) | 6001 (16.7) | 0.065 | 18.0 | 17.3 | 0.017 |
| III | 5819 (59.0) | 22,964 (63.8) | 0.098 | 63.0 | 62.8 | 0.005 |
| IV or V † | 2157 (21.9) | 7045 (19.6) | 0.057 | 19.1 | 19.9 | 0.022 |
| Postoperative 30-Day Outcomes | Total Number of Patients | Number of Events (%) | Unweighted Adjusted HR (95% CI) * | After IPTW Adjusted HR (95% CI) * |
|---|---|---|---|---|
| Any adverse events | ||||
| Neuraxial anesthesia | 9864 | 1087 (11.0) | 1.00 (reference) | 1.00 (reference) |
| General anesthesia | 36,010 | 4635 (12.9) | 1.15 (1.07–1.23) | 1.14 (1.10–1.19) |
| Morbidity | ||||
| Neuraxial anesthesia | 9864 | 809 (8.2) | 1.00 (reference) | 1.00 (reference) |
| General anesthesia | 36,010 | 3463 (9.6) | 1.17 (1.08–1.27) | 1.19 (1.14–1.24) |
| Mortality | ||||
| Neuraxial anesthesia | 9864 | 437 (4.4) | 1.00 (reference) | 1.00 (reference) |
| General anesthesia | 36,010 | 1951 (5.4) | 1.13 (1.01–1.26) | 1.09 (1.03–1.16) |
| Postoperative 30-Day Outcomes | Total Number of Patients | Number of Events (%) | Unweighted Adjusted HR (95% CI) * | After IPTW Adjusted HR (95% CI) * |
|---|---|---|---|---|
| Myocardial infarction | ||||
| Neuraxial anesthesia | 9864 | 207 (2.1) | 1.00 (reference) | 1.00 (reference) |
| General anesthesia | 36,010 | 722 (2.0) | 0.98 (0.83–1.16) | 1.03 (0.94–1.13) |
| Cardiac arrest | ||||
| Neuraxial anesthesia | 9864 | 44 (0.5) | 1.00 (reference) | 1.00 (reference) |
| General anesthesia | 36,010 | 264 (0.7) | 1.39 (1.00–1.95) | 1.23 (1.04–1.45) |
| Stroke | ||||
| Neuraxial anesthesia | 9864 | 71 (0.7) | 1.00 (reference) | 1.00 (reference) |
| General anesthesia | 36,010 | 288 (0.8) | 1.06 (0.81–1.40) | 0.95 (0.83–1.10) |
| Pneumonia | ||||
| Neuraxial anesthesia | 9864 | 270 (2.7) | 1.00 (reference) | 1.00 (reference) |
| General anesthesia | 36,010 | 1075 (3.0) | 1.12 (0.97–1.29) | 1.18 (1.09–1.27) |
| Pulmonary embolism | ||||
| Neuraxial anesthesia | 9864 | 73 (0.7) | 1.00 (reference) | 1.00 (reference) |
| General anesthesia | 36,010 | 285 (0.8) | 1.11 (0.84–1.45) | 1.00 (0.86–1.16) |
| Ventilator support † | ||||
| Neuraxial anesthesia | 9864 | 22 (0.2) | 1.00 (reference) | 1.00 (reference) |
| General anesthesia | 36,010 | 202 (0.6) | 1.84 (1.17–2.91) | 1.42 (1.17–1.74) |
| Renal failure ‡ | ||||
| Neuraxial anesthesia | 9864 | 43 (0.4) | 1.00 (reference) | 1.00 (reference) |
| General anesthesia | 36,010 | 284 (0.8) | 1.49 (1.06–2.09) | 1.29 (1.10–1.51) |
| Surgical site infection | ||||
| Neuraxial anesthesia | 9864 | 89 (0.9) | 1.00 (reference) | 1.00 (reference) |
| General anesthesia | 36,010 | 410 (1.1) | 1.34 (1.05–1.71) | 1.37 (1.20–1.56) |
| Sepsis or septic shock | ||||
| Neuraxial anesthesia | 9864 | 104 (1.1) | 1.00 (reference) | 1.00 (reference) |
| General anesthesia | 36,010 | 556 (1.5) | 1.28 (1.03–1.60) | 1.32 (1.17–1.47) |
| DVT | ||||
| Neuraxial anesthesia | 9864 | 76 (0.8) | 1.00 (reference) | 1.00 (reference) |
| General anesthesia | 36,010 | 411 (1.1) | 1.38 (1.07–1.78) | 1.38 (1.21–1.57) |
| Neuraxial Anesthesia (n = 9864) | General Anesthesia (n = 9864) | ||
|---|---|---|---|
| Characteristics | Number (Percent of Patients) | SMD * | |
| Demographics | |||
| Age, years | |||
| <65 | 741 (7.5) | 722 (7.3) | 0.006 |
| 65–74 | 1410 (14.3) | 1439 (14.6) | 0.008 |
| 75–84 | 3079 (31.2) | 3034 (30.8) | 0.010 |
| ≥85 | 4634 (47.0) | 4669 (47.3) | 0.007 |
| Sex | |||
| Female | 6974 (70.7) | 6992 (70.9) | 0.004 |
| Male | 2890 (29.3) | 2872 (29.1) | 0.004 |
| Race/ethnicity | |||
| White | 4807 (48.7) | 4830 (49.0) | 0.005 |
| Other | 5057 (51.3) | 5034 (51.0) | 0.005 |
| Body mass index | |||
| Normal | 4938 (50.1) | 4948 (50.2) | 0.002 |
| Underweight | 926 (9.4) | 864 (8.8) | 0.022 |
| Overweight | 2667 (27.0) | 2706 (27.4) | 0.009 |
| Obese | 1333 (13.5) | 1346 (13.7) | 0.004 |
| Functional health status | |||
| Independent | 7827 (79.4) | 7840 (79.5) | 0.003 |
| Partially dependent | 1770 (17.9) | 1772 (18.0) | 0.001 |
| Totally dependent | 267 (2.7) | 252 (2.6) | 0.009 |
| Comorbidities | |||
| Smoking | 1074 (10.9) | 977 (9.9) | 0.030 |
| Diabetes mellitus | 1652 (16.8) | 1680 (17.0) | 0.007 |
| Hypertension | 6166 (62.5) | 6314 (64.0) | 0.031 |
| Congestive heart failure | 297 (3.0) | 275 (2.8) | 0.012 |
| COPD | 1120 (11.4) | 996 (10.1) | 0.040 |
| Dialysis | 130 (1.3) | 122 (1.2) | 0.006 |
| Dementia | 2741 (27.8) | 2848 (28.9) | 0.024 |
| Disseminated cancer | 279 (2.8) | 247 (2.5) | 0.018 |
| Bleeding disorder | 684 (6.9) | 665 (6.7) | 0.006 |
| Operative information | |||
| Type of fracture | |||
| Femoral neck fracture | 4075 (41.3) | 3993 (40.5) | 0.017 |
| Intertrochanteric | 5009 (50.8) | 5108 (51.8) | 0.020 |
| Subtrochanteric/other | 780 (7.9) | 763 (7.7) | 0.006 |
| ASA classification | |||
| I or II | 1888 (19.1) | 1943 (19.7) | 0.015 |
| III | 5819 (59.0) | 5930 (60.1) | 0.023 |
| IV or V | 2157 (21.9) | 1991 (20.2) | 0.042 |
| Postoperative 30-Day Outcomes | Total Number | Number of Events (%) | Unadjusted HR (95% CI) | Adjusted HR (95% CI) * |
|---|---|---|---|---|
| Any adverse events | ||||
| Neuraxial anesthesia | 9864 | 1087 (11.0) | 1.00 | 1.00 |
| General anesthesia | 9864 | 1254 (12.7) | 1.16 (1.07–1.26) | 1.25 (1.13–1.39) |
| Morbidity | ||||
| Neuraxial anesthesia | 9864 | 809 (8.2) | 1.00 | 1.00 |
| General anesthesia | 9864 | 939 (9.5) | 1.17 (1.06–1.28) | 1.30 (1.15–1.46) |
| Mortality | ||||
| Neuraxial anesthesia | 9864 | 437 (4.4) | 1.00 | 1.00 |
| General anesthesia | 9864 | 504 (5.1) | 1.16 (1.02–1.32) | 1.19 (1.00–1.42) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, M.-T.; Chang, C.-C.; Liu, C.-C.; Fan Chiang, Y.-H.; Shih, Y.-R.V.; Lee, Y.-W. General versus Neuraxial Anesthesia on Clinical Outcomes in Patients Receiving Hip Fracture Surgery: An Analysis of the ACS NSQIP Database. J. Clin. Med. 2023, 12, 3827. https://doi.org/10.3390/jcm12113827
Wang M-T, Chang C-C, Liu C-C, Fan Chiang Y-H, Shih Y-RV, Lee Y-W. General versus Neuraxial Anesthesia on Clinical Outcomes in Patients Receiving Hip Fracture Surgery: An Analysis of the ACS NSQIP Database. Journal of Clinical Medicine. 2023; 12(11):3827. https://doi.org/10.3390/jcm12113827
Chicago/Turabian StyleWang, Ming-Tse, Chuen-Chau Chang, Chih-Chung Liu, Yu-Hsuan Fan Chiang, Yu-Ru Vernon Shih, and Yuan-Wen Lee. 2023. "General versus Neuraxial Anesthesia on Clinical Outcomes in Patients Receiving Hip Fracture Surgery: An Analysis of the ACS NSQIP Database" Journal of Clinical Medicine 12, no. 11: 3827. https://doi.org/10.3390/jcm12113827