
A Universal Bleeding Risk Score in Native and Allograft Kidney Biopsies: A French Nationwide Cohort Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Selection
2.3. Major Bleeding and Risk of Death after Biopsy
2.4. Collected Data
2.4.1. Demographic, Cardiovascular and Metabolic Conditions
2.4.2. Other Relevant Parameters
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Major Bleeding Rate in Transplant Kidney Biopsies
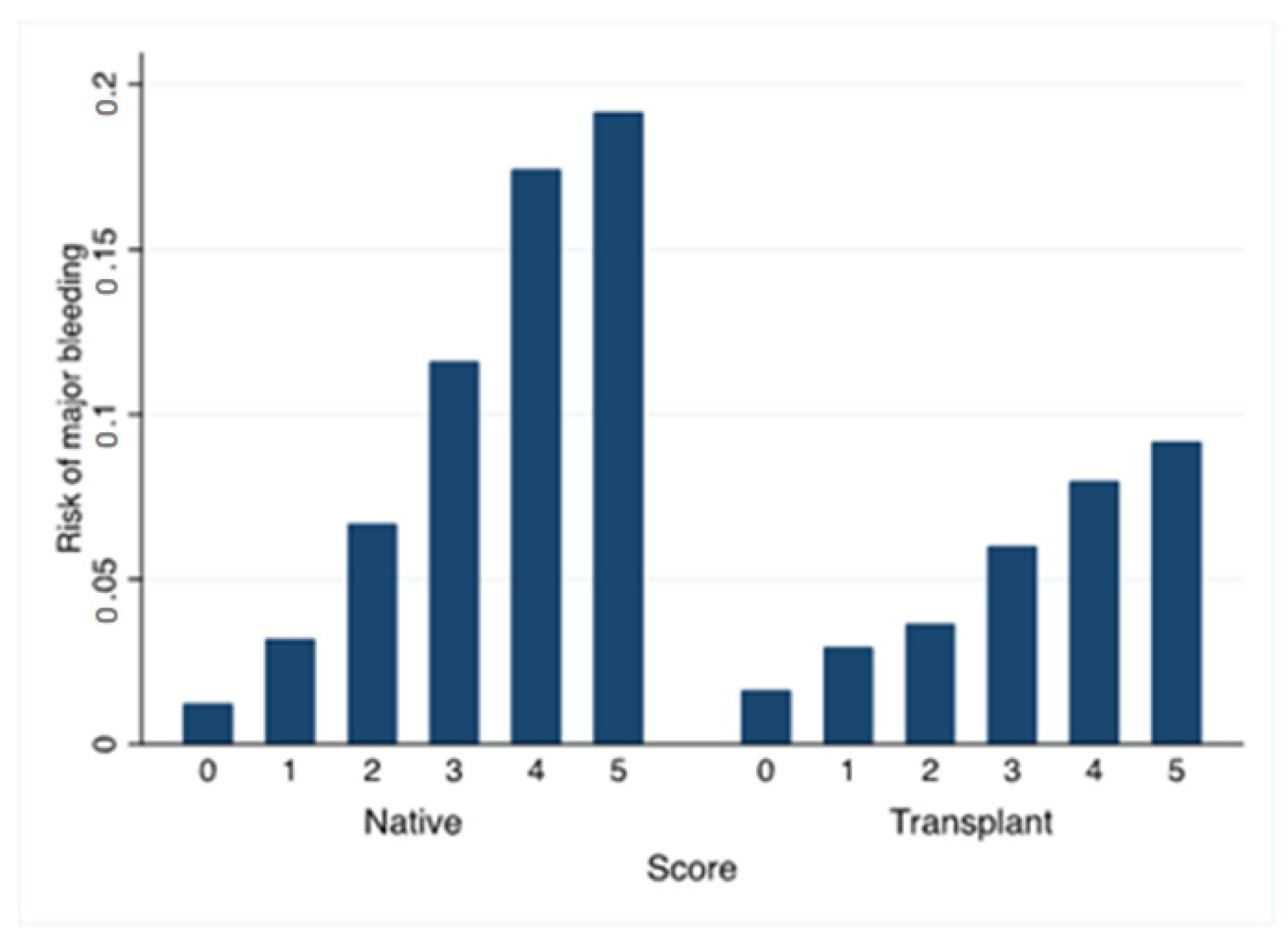
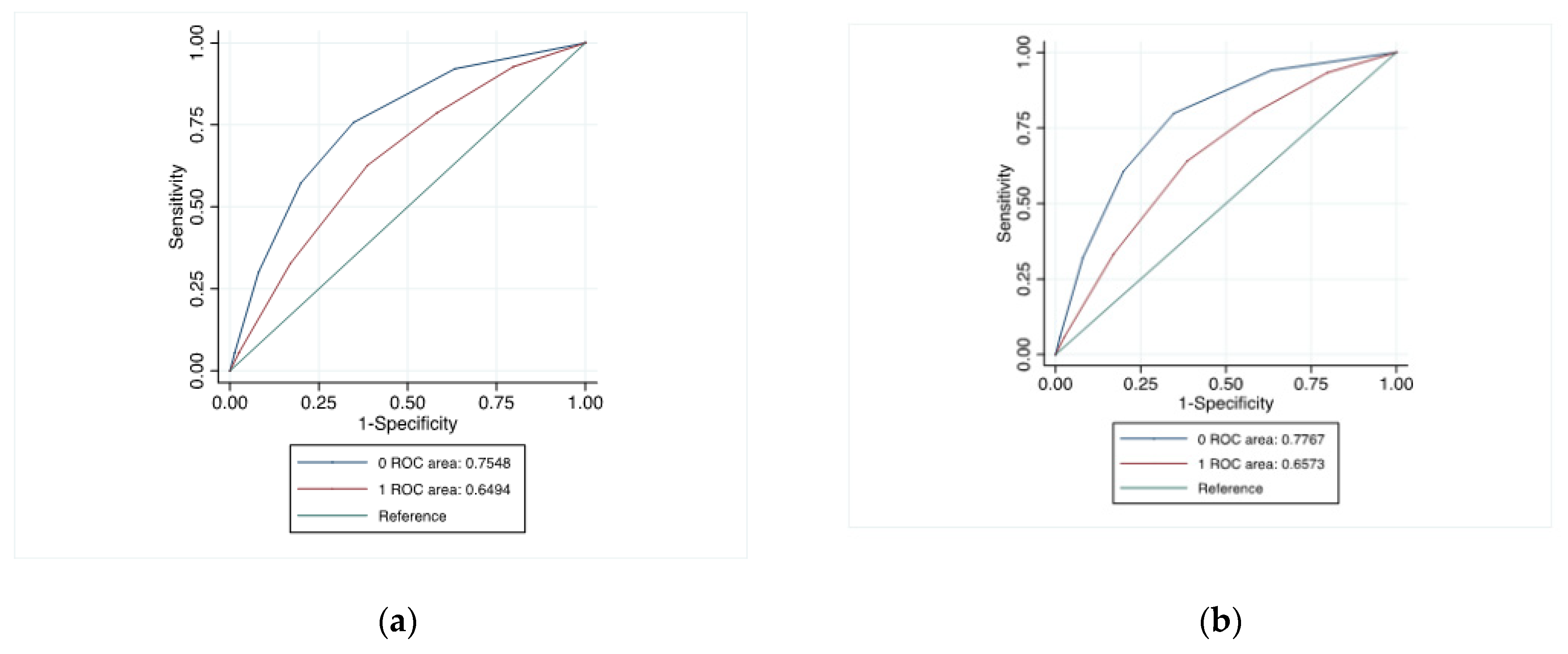
3.3. Risk Factors for Major Bleeding and Development of a New Score in This Population
3.4. Application of This New Score to Patients with Native Kidneys
3.5. Major Bleeding Risk: Center Effect in Kidney Transplant Recipients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Josephson, M.A. Monitoring and managing graft health in the kidney transplant recipient. Clin. J. Am. Soc. Nephrol. 2011, 6, 1774–1780. [Google Scholar] [CrossRef] [PubMed]
- Loupy, A.; Haas, M.; Roufosse, C.; Naesens, M.; Adam, B.; Afrouzian, M.; Akalin, E.; Alachkar, N.; Bagnasco, S.; Becker, J.U.; et al. The Banff 2019 Kidney Meeting Report (I): Updates on and clarification of criteria for T cell- and antibody-mediated rejection. Am. J. Transplant. 2020, 20, 2318–2331. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Lin, W.; Lee, C.; Yang, C.; Tsai, M. Two-year protocol biopsy after kidney transplantation in clinically stable recipients—A retrospective study. Transpl. Int. 2020, 34, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Kreis, H.; Noël, L.-H.; Legendre, C. The first transplant kidney biopsy ever performed. Am. J. Transplant. 2013, 13, 1367–1368. [Google Scholar] [CrossRef]
- Mahoney, M.C.; Racadio, J.M.; Merhar, G.L.; First, M.R. Safety and efficacy of kidney transplant biopsy: Tru-Cut needle vs sonographically guided Biopty gun. AJR Am. J. Roentgenol. 1993, 160, 325–326. [Google Scholar] [CrossRef]
- Nyman, R.S.; Cappelen-Smith, J.; Al Suhaibani, H.; Alfurayh, O.; Shakweer, W.; Akhtar, M. Yield and complications in percutaneous renal biopsy. A comparison between ultrasound-guided gun-biopsy and manual techniques in native and transplant kidneys. Acta Radiol. 1997, 38, 431–436. [Google Scholar]
- Kim, D.; Kim, H.; Shin, G.; Ku, S.; Ma, K.; Shin, S.; Gi, H.; Lee, E.; Yim, H. A randomized, prospective, comparative study of manual and automated renal biopsies. Am. J. Kidney Dis. 1998, 32, 426–431. [Google Scholar] [CrossRef]
- Nicholson, M.L.; Wheatley, T.J.; Doughman, T.M.; White, S.A.; Morgan, J.D.; Veitch, P.S.; Furness, P.N. A prospective randomized trial of three different sizes of core-cutting needle for renal transplant biopsy. Kidney Int. 2000, 58, 390–395. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [Updated March 2011]; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Schmid, A. Percutaneous renal transplant biopsy: Is the safety profile adequate for short-term postprocedure monitoring? Transpl. Int. 2016, 29, 165–166. [Google Scholar] [CrossRef]
- Aaltonen, S.; Finne, P.; Honkanen, E. Outpatient Kidney Biopsy: A Single Center Experience and Review of Literature. Nephron 2020, 144, 14–20. [Google Scholar] [CrossRef]
- Patel, I.J.; Davidson, J.C.; Nikolic, B.; Salazar, G.M.; Schwartzberg, M.S.; Walker, T.G.; Saad, W.A. Consensus guidelines for periprocedural management of coagulation status and hemostasis risk in percutaneous image-guided interventions. J. Vasc. Interv. Radiol. 2012, 23, 727–736. [Google Scholar] [CrossRef] [PubMed]
- Preda, A.; Van Dijk, L.C.; Van Oostaijen, J.A.; Pattynama, P.M. Complication rate and diagnostic yield of 515 consecutive ultrasound-guided biopsies of renal allografts and native kidneys using a 14-gauge Biopty gun. Eur. Radiol. 2003, 13, 527–530. [Google Scholar] [CrossRef] [PubMed]
- Redfield, R.R.; McCune, K.R.; Rao, A.; Sadowski, E.; Hanson, M.; Kolterman, A.J.; Robbins, J.; Guite, K.; Mohamed, M.; Parajuli, S.; et al. Nature, timing, and severity of complications from ultrasound-guided percutaneous renal transplant biopsy. Transpl. Int. 2016, 29, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Furness, P.N.; Philpott, C.M.; Chorbadjian, M.T.; Nicholson, M.L.; Bosmans, J.-L.; Corthouts, B.L.; Bogers, J.-J.; Schwarz, A.; Gwinner, W.; Haller, H.; et al. Protocol biopsy of the stable renal transplant: A multicenter study of methods and complication rates. Transplantation 2003, 76, 969–973. [Google Scholar] [CrossRef]
- Schwarz, A.; Gwinner, W.; Hiss, M.; Radermacher, J.; Mengel, M.; Haller, H. Safety and adequacy of renal transplant protocol biopsies. Am. J. Transplant. 2005, 5, 1992–1996. [Google Scholar] [CrossRef]
- Morgan, T.A.; Chandran, S.; Bürger, I.M.; Zhang, C.A.; Goldstein, R.B. Complications of Ultrasound-Guided Renal Transplant Biopsies. Am. J. Transplant. 2016, 16, 1298–1305. [Google Scholar] [CrossRef]
- Patel, A.G.; Kriegshauser, J.S.; Young, S.W.; Dahiya, N.; Patel, M.D. Detection of Bleeding Complications after Renal Transplant Biopsy. AJR Am. J. Roentgenol. 2021, 216, 428–435. [Google Scholar] [CrossRef]
- Tapia Canelas, C.; Tapia-Canelas, C.; Zometa, R.; López Oliva, M.O.; Jiménez, C.; Rivas, B.; Escuin, F.; Yébenes, L.; Selgas, R. Complications associated with renal graft biopsy in transplant patients. Nefrologia 2014, 34, 115–119. [Google Scholar]
- Riehl, J.; Maigatter, S.; Kierdorf, H.; Schmitt, H.; Maurin, N.; Sieberth, H.G. Percutaneous renal biopsy: Comparison of manual and automated puncture techniques with native and transplanted kidneys. Nephrol. Dial. Transplant. 1994, 9, 1568–1574. [Google Scholar]
- Atwell, T.D.; Spanbauer, J.C.; McMenomy, B.P.; Stockland, A.H.; Hesley, G.K.; Schleck, C.D.; Harmsen, W.S.; Welch, T.J. The Timing and Presentation of Major Hemorrhage after 18,947 Image-Guided Percutaneous Biopsies. Am. J. Roentgenol. 2015, 205, 190–195. [Google Scholar] [CrossRef]
- Charu, V.; O’Shaughnessy, M.M.; Chertow, G.M.; Kambham, N. Percutaneous Kidney Biopsy and the Utilization of Blood Transfusion and Renal Angiography Among Hospitalized Adults. Kidney Int. Rep. 2019, 4, 1435–1445. [Google Scholar] [CrossRef] [PubMed]
- Whittier, W.L.; Gashti, C.; Saltzberg, S.; Korbet, S. Comparison of native and transplant kidney biopsies: Diagnostic yield and complications. Clin. Kidney J. 2018, 11, 616–622. [Google Scholar] [CrossRef] [PubMed]
- Halimi, J.-M.; Gatault, P.; Longuet, H.; Barbet, C.; Bisson, A.; Sautenet, B.; Herbert, J.; Buchler, M.; Grammatico-Guillon, L.; Fauchier, L. Major bleeding and risk of death after percutaneous native kidney biopsies. A French nationwide cohort study. Clin. J. Am. Soc. Nephrol. 2020, 15, 1587–1594. [Google Scholar] [CrossRef] [PubMed]
- Ferrandiz, I.; Congy-Jolivet, N.; Del Bello, A.; Debiol, B.; Trébern-Launay, K.; Esposito, L.; Milongo, D.; Dörr, G.; Rostaing, L.; Kamar, N. Impact of Early Blood Transfusion after Kidney Transplantation on the Incidence of Donor-Specific Anti-HLA Antibodies. Am. J. Transplant. 2016, 16, 2661–2669. [Google Scholar] [CrossRef]
- Halimi, J.-M.; Gatault, P.; Longuet, H.; Barbet, C.; Goumard, A.; Gueguen, J.; Goin, N.; Sautenet, B.; Herbert, J.; Bisson, A.; et al. Major Bleeding of Transjugular Native Kidney Biopsies. A French Nationwide Cohort Study. Kidney Int. Rep. 2021, 6, 2594–2603. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Segal, J.B.; Chang, H.-Y.; Du, Y.; Walston, J.D.; Carlson, M.C.; Varadhan, R. Development of a Claims-based Frailty Indicator Anchored to a Well-established Frailty Phenotype. Med. Care 2017, 55, 716–722. [Google Scholar] [CrossRef]
- Lloyd-Jones, D.M.; Wang, T.J.; Leip, E.P.; Larson, M.G.; Levy, D.; Vasan, R.S.; D’Agostino, R.B.; Massaro, J.M.; Beiser, A.; Wolf, P.A.; et al. Lifetime risk for development of atrial fibrillation: The Framingham Heart Study. Circulation 2004, 110, 1042–1046. [Google Scholar] [CrossRef]
- Mehta, H.B.; Mehta, V.; Girman, C.J.; Adhikari, D.; Johnson, M.L. Regression coefficient-based scoring system should be used to assign weights to the risk index. J. Clin. Epidemiol. 2016, 79, 22–28. [Google Scholar] [CrossRef]
- Fereira, L.C.; Karras, A.; Martinez, F.; Thervet, E.; Legendre, C. Complications of protocol renal biopsy. Transplantation 2004, 77, 1475–1476. [Google Scholar] [CrossRef]
- Šimunov, B.; Gunjača, M.; Čingel, B.; Skegro, D.; Knotek, M. Safety of Outpatient Kidney Biopsies. Nephron 2018, 138, 275–279. [Google Scholar] [CrossRef] [PubMed]
- Beckingham, I.J.; Nicholson, M.L.; Bell, P.R. Analysis of factors associated with complications following renal transplant needle core biopsy. Br. J. Urol. 1994, 73, 13–15. [Google Scholar] [CrossRef] [PubMed]
- Tøndel, C.; Vikse, B.E.; Bostad, L.; Svarstad, E. Safety and complications of percutaneous kidney biopsies in 715 children and 8573 adults in Norway 1988–2010. Clin. J. Am. Soc. Nephrol. 2012, 7, 1591–1597. [Google Scholar] [CrossRef] [PubMed]
- Halimi, J.M. Complications after native kidney biopsy: Definitive data. Curr. Opin. Nephrol. Hypertens. 2021, 30, 555–558. [Google Scholar] [CrossRef] [PubMed]
- Corapi, K.M.; Chen, J.L.; Balk, E.M.; Gordon, C.E. Bleeding complications of native kidney biopsy: A systematic review and meta-analysis. Am. J. Kidney Dis. 2012, 60, 62–73. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Percutaneous Native Kidney Biopsy | Percutaneous Biopsy in Kidney Transplant | |
|---|---|---|
| (n = 55,026) | (n = 28,034) | |
| Age, years | 58.0 ± 17.4 | 51.6 ± 14.7 |
| Sex (male) | 33,523 (60.9) | 17,706 (63.2) |
| Charlson comorbidity index | 4.6 ± 2.8 | 4.8 ± 2.7 |
| Frailty index | 7.1 ± 7.7 | 8.6 ± 7.6 |
| Hypertension | 29,392 (53.4) | 20,971 (74.8) |
| Diabetes mellitus | 12,376 (22.5) | 7476 (26.7) |
| Obesity | 8626 (15.7) | 3863 (13.8) |
| Heart failure with congestion | 5827 (10.6) | 3825 (13.6) |
| Valve disease | 2454 (4.5) | 1189 (4.2) |
| Coronary artery disease | 5486 (10.0) | 4404 (15.7) |
| Vascular disease | 5889 (10.7) | 4081 (14.6) |
| Atrial fibrillation | 4839 (8.8) | 2090 (7.5) |
| Ischemic stroke | 1006 (1.8) | 362 (1.3) |
| Smoker | 5565 (10.1) | 2726 (9.7) |
| Dyslipidemia | 10,257 (18.6) | 6440 (23.0) |
| Poor nutrition | 4865 (8.8) | 2077 (7.4) |
| Alcohol related diagnoses | 3689 (6.7) | 939 (3.3) |
| Lung disease | 5749 (10.4) | 2070 (7.4) |
| Liver disease | 3345 (6.1) | 1493 (5.3) |
| Anaemia | 13,382 (24.3) | 14,484 (51.7) |
| Thrombocytopenia | 3854 (7.0) | 1733 (6.2) |
| Previous cancer | 13,264 (24.1) | 2562 (9.1) |
| Abnormal renal function | 17,566 (31.9) | 23,791 (84.9) |
| Percutaneous Biopsy in Kidney Transplant | Percutaneous Native Kidney Biopsy | |
|---|---|---|
| (n = 28,034) | (n = 55,026) | |
| Angiographic intervention | 56 (0.2) | 216 (0.4) |
| Nephrectomy | 7 (0.0) | 33 (0.1) |
| Blood transfusion | 1118 (4.0) | 2614 (4.8) |
| Hemorrhage/hematoma | 104 (0.4) | 273 (0.5) |
| Any of the bleeding events | 1238 (4.4) | 2991 (5.4) |
| Angiographic intervention or nephrectomy or transfusion | 1160 (4.1) | 2778 (5.0) |
| Death at day 30 | 32 (0.1) | 543 (1.0) |
| Univariate Analysis | Multivariable Analysis | |||
|---|---|---|---|---|
| HR, 95% CI | p | HR, 95% CI | p | |
| Age (quartile) | 0.980 (0.925–1.039) | 0.49 | 0.907 (0.848–0.970) | 0.004 |
| Charlson comorbidity index | 1.272 (1.206–1.341) | <0.0001 | 1.240 (1.155–1.333) | <0.0001 |
| Frailty index | 1.288 (1.219–1.361) | <0.0001 | 1.139 (1.072–1.211) | <0.0001 |
| Sex (male) | 0.797 (0.710–0.895) | <0.0001 | 0.853 (0.756–0.962) | 0.01 |
| Hypertension | 1.138 (0.994–1.302) | 0.06 | 0.844 (0.725–0.984) | 0.03 |
| Diabetes mellitus | 1.088 (0.959–1.235) | 0.19 | 0.848 (0.720–0.999) | 0.05 |
| Heart failure with congestion | 1.750 (1.520–2.015) | <0.0001 | 1.194 (1.018–1.401) | 0.03 |
| Valve disease | 1.397 (1.092–1.789) | 0.008 | 1.048 (0.807–1.362) | 0.72 |
| Coronary artery disease | 1.182 (1.018–1.371) | 0.03 | 1.035 (0.868–1.235) | 0.70 |
| Vascular disease | 1.074 (0.917–1.258) | 0.37 | 0.805 (0.671–0.965) | 0.02 |
| Atrial fibrillation | 1.473 (1.221–1.778) | <0.0001 | 1.170 (0.951–1.438) | 0.14 |
| Ischemic stroke | 1.339 (0.858–2.088) | 0.20 | 0.937 (0.594–1.478) | 0.78 |
| Smoker | 1.194 (0.997–1.430) | 0.06 | 0.993 (0.818–1.206) | 0.95 |
| Dyslipidemia | 1.032 (0.902–1.180) | 0.65 | 0.940 (0.807–1.096) | 0.43 |
| Obesity | 1.164 (0.994–1.362) | 0.06 | 1.035 (0.874–1.226) | 0.69 |
| Poor nutrition | 1.470 (1.217–1.775) | <0.0001 | 0.958 (0.785–1.169) | 0.67 |
| Alcohol related diagnoses | 1.335 (1.008–1.768) | 0.04 | 1.000 (0.739–1.352) | 1.00 |
| Abnormal renal function | 1.889 (1.548–2.306) | <0.0001 | 1.328 (1.070–1.648) | 0.01 |
| Lung disease | 1.275 (1.045–1.555) | 0.02 | 0.894 (0.725–1.103) | 0.30 |
| Liver disease | 1.510 (1.217–1.874) | <0.0001 | 1.016 (0.804–1.285) | 0.89 |
| Anaemia | 2.262 (1.998–2.560) | <0.0001 | 1.710 (1.490–1.963) | <0.0001 |
| Thrombocytopenia | 1.709 (1.408–2.074) | <0.0001 | 1.081 (0.879–1.329) | 0.46 |
| Previous cancer | 1.091 (0.901–1.322) | 0.37 | 0.855 (0.697–1.049) | 0.13 |
| Acute renal failure | 2.499 (2.209–2.827) | <0.0001 | 1.870 (1.640–2.132) | <0.0001 |
| Quartile of Center Volume | Mean Number of Biopsies by Center, 2010–1019 | Number of Patients with Percutaneous Biopsies, n | Number of Patients with Native Biopsy/Transplant | Major Bleeding Among Patients with Percutaneous Biopsy, n (%) | Major Bleeding among Patients with Native Percutaneous Biopsy, n (%) | Major Bleeding Among Patients with Transplant Percutaneous Biopsy, n (%) |
|---|---|---|---|---|---|---|
| 1 | 159 ± 86 | 20,827 | 17,936/2891 | 1081 (5.2) | 949 (5.3) | 132 (4.6) |
| 2 | 524 ± 121 | 21,661 | 15,835/5826 | 1268 (5.9) | 956 (6.0) | 312 (5.4) |
| 3 | 1035 ± 235 | 22,778 | 12,425/10,353 | 1063 (4.7) | 653 (5.3) | 410 (4.0) |
| 4 | 4473 ± 1121 | 17,794 | 8830/8964 | 817 (4.6) | 433 (4.9) | 384 (4.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaczmarek, M.; Halimi, J.-M.; de Fréminville, J.-B.; Gatault, P.; Gueguen, J.; Goin, N.; Longuet, H.; Barbet, C.; Bisson, A.; Sautenet, B.; et al. A Universal Bleeding Risk Score in Native and Allograft Kidney Biopsies: A French Nationwide Cohort Study. J. Clin. Med. 2023, 12, 3527. https://doi.org/10.3390/jcm12103527
Kaczmarek M, Halimi J-M, de Fréminville J-B, Gatault P, Gueguen J, Goin N, Longuet H, Barbet C, Bisson A, Sautenet B, et al. A Universal Bleeding Risk Score in Native and Allograft Kidney Biopsies: A French Nationwide Cohort Study. Journal of Clinical Medicine. 2023; 12(10):3527. https://doi.org/10.3390/jcm12103527
Chicago/Turabian StyleKaczmarek, Mathieu, Jean-Michel Halimi, Jean-Baptiste de Fréminville, Philippe Gatault, Juliette Gueguen, Nicolas Goin, Hélène Longuet, Christelle Barbet, Arnaud Bisson, Bénédicte Sautenet, and et al. 2023. "A Universal Bleeding Risk Score in Native and Allograft Kidney Biopsies: A French Nationwide Cohort Study" Journal of Clinical Medicine 12, no. 10: 3527. https://doi.org/10.3390/jcm12103527