
Psychopathic Traits, Externalizing Problems, and Prosocial Behavior: The Role of Social Dominance Orientation
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.3. Statistical Analyses
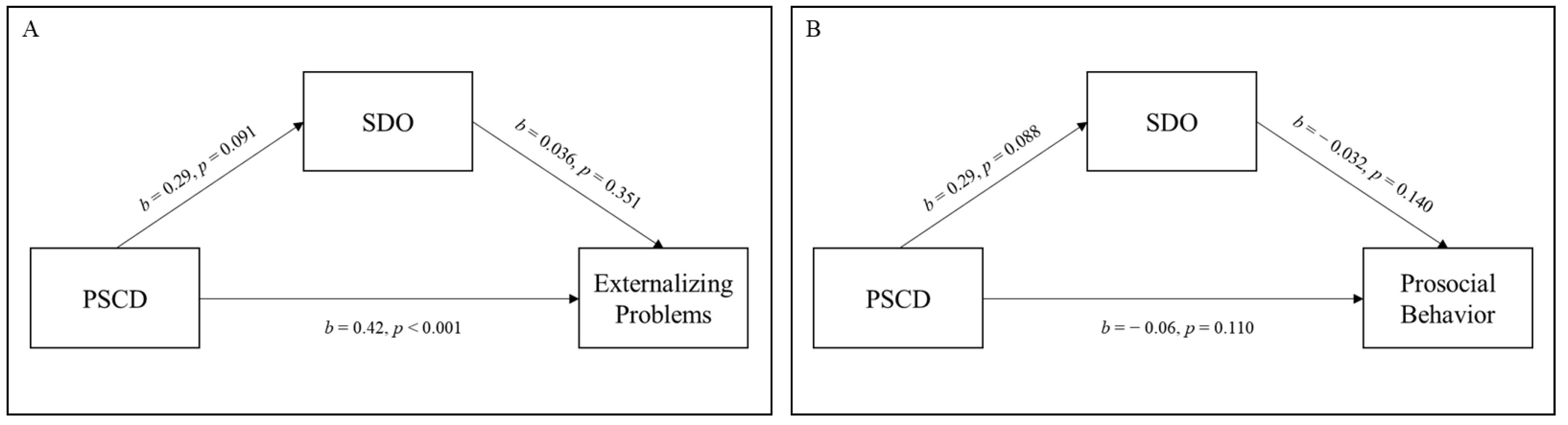
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hare, R.D.; Neumann, C.S. Psychopathy as a Clinical and Empirical Construct. Annu. Rev. Clin. Psychol. 2008, 4, 217–246. [Google Scholar] [CrossRef] [PubMed]
- Hare, R.D. Hare Psychopathy Checklist: Youth Version; Multi-Health Systems: Toronto, ON, Canada, 2003. [Google Scholar]
- Andershed, H. Stability and change of psychopathic traits: What do we know? In Handbook of Child Adolescent Psychopathy; Guilford Press: New York, NY, USA, 2010; pp. 233–250. ISBN 978-1-60623-682-6. [Google Scholar]
- Salekin, R.T. Research Review: What do we know about psychopathic traits in children? J. Child Psychol. Psychiatry Allied Discip. 2017, 58, 1180–1200. [Google Scholar] [CrossRef]
- Colins, O.F.; Andershed, H.; Frogner, L.; Lopez-Romero, L.; Veen, V.; Andershed, A.K. A new measure to assess psychopathic personality in children: The child problematic traits inventory. J. Psychopathol. Behav. Assess. 2014, 36, 4–21. [Google Scholar] [CrossRef] [PubMed]
- Salekin, R.T.; (Department of Psychology, University of North Texas, Denton, TX, USA); Hare, R.D.; (Psychology University of British Columbia, Vancouver, BC, Canada). The Proposed Specifiers for Conduct Disorder (PSCD) scale. Personal communication, 2016. Unpublished. [Google Scholar]
- Frick, P.J.; Kimonis, E.R.; Dandreaux, D.M.; Farell, J.M. The 4 Year Stability of Psychopathic Traits in Non-Referred Youth. Behav. Sci. Law 2003, 21, 713–736. [Google Scholar] [CrossRef] [PubMed]
- Lynam, D.R.; Caspi, A.; Moffitt, T.E.; Loeber, R.; Stouthamer-Loeber, M. Longitudinal evidence that psychopathy scores in early adolescence predict adult psychopathy. J. Abnorm. Psychol. 2007, 116, 155–165. [Google Scholar] [CrossRef]
- López-Romero, L.; Romero, E.; Colins, O.F.; Andershed, H.; Hare, R.D.; Salekin, R.T. Proposed Specifiers for Conduct Disorder (PSCD): Preliminary Validation of the Parent Version in a Spanish Sample of Preschoolers. Psychol. Assess. 2019, 31, 1357–1367. [Google Scholar] [CrossRef]
- Luo, J.; Wang, M.C.; Neumann, C.S.; Hare, R.D.; Salekin, R.T. Factor Structure and Construct Validity of the Proposed Specifiers for Conduct Disorder (PSCD) Scale in Chinese Adolescents. Assessment 2020, 28, 1765–1784. [Google Scholar] [CrossRef]
- Muratori, P.; Buonanno, C.; Gallani, A.; Grossi, G.; Levantini, V.; Milone, A.; Pisano, S.; Salekin, R.T.; Sesso, G.; Masi, G.; et al. Validation of the Proposed Specifiers for Conduct Disorder (PSCD) scale in a sample of Italian students. Children 2021, 8, 1020. [Google Scholar] [CrossRef]
- McCuish, E.C.; Corrado, R.R.; Hart, S.D.; DeLisi, M. The role of symptoms of psychopathy in persistent violence over the criminal career into full adulthood. J. Crim. Justice 2015, 43, 345–356. [Google Scholar] [CrossRef]
- Edens, J.F. Interpersonal Characteristics of Male Criminal Offenders: Personality, Psychopathological, and Behavioral Correlates. Psychol. Assess. 2009, 21, 89–98. [Google Scholar] [CrossRef]
- Kosson, D.S.; Forth, A.E.; Steuerwald, B.L.; Kirkhart, K.J. A new method for assessing the interpersonal behavior of psychopathic individuals: Preliminary validation studies. Psychol. Assess. 1997, 9, 89–101. [Google Scholar] [CrossRef]
- Johnson, S.; Leedom, L.; Muhtadie, L. The Dominance Behavioral System and Psychopathology: Evidence from Self-Report, Observational, and Biological Studies. Psychol. Bull. 2012, 138, 692–743. [Google Scholar] [CrossRef] [PubMed]
- Mayeux, L. Understanding popularity and relational aggression in adolescence: The role of social dominance orientation. Soc. Dev. 2014, 23, 502–517. [Google Scholar] [CrossRef]
- Gumpel, T.P.; Gotdiner, V. The use of Latent Pro fi le Analyses to examine social dominance orientation as a predictor of peer-to-peer aggression among adolescents. J. Interpers. Violence 2023, 38, 1424–1445. [Google Scholar] [CrossRef]
- Saucier, G. Isms and the structure of social attitudes. J. Pers. Soc. Psychol. 2000, 78, 366. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Li, W.; Sheldon, K.M.; Kou, Y. Chinese adolescents with higher social dominance orientation are less prosocial and less happy: A value-environment fit analysis. Int. J. Psychol. 2019, 54, 325–332. [Google Scholar] [CrossRef]
- Bai, B.Y.; Tan, X.Y.; Zhang, N.; Yang, Y. Social Dominance Orientation and Selfish Behaviors in Chinese Adolescents: The Mediating Role of Psychological Entitlement. Child Indic. Res. 2020, 13, 981–991. [Google Scholar] [CrossRef]
- Halkjelsvik, T.; Rise, J. Social dominance orientation, right-wing authoritarianism, and willingness to help addicted individuals: The role of responsibility judgments. Eur. J. Psychol. 2014, 10, 27–40. [Google Scholar] [CrossRef]
- Elhami Athar, M.; Kargari Padar, L.; Sharifi Nejad, A.; Karimi, S.; Ebrahimi, A.; Salekin, R.T.; Colins, O.F. Validation of the Proposed Specifiers for Conduct Disorder (PSCD) Self-Report Version in Iranian School-Attending Adolescents. J. Pers. Assess. 2022, 1–11. [Google Scholar] [CrossRef]
- Salekin, R.T.; Charles, N.E.; Barry, C.; Hare, R. Proposed Specifiers for Conduct Disorder (PSCD): Factor structure and psychometric properties in a residential school facility. Psychol. Assess. 2022, 34, 985–992. [Google Scholar] [CrossRef]
- Colins, O.F.; Bisback, A.; Reculé, C.; Batky, B.D.; López-Romero, L.; Hare, R.D.; Salekin, R.T. The Proposed Specifiers for Conduct Disorder (PSCD) Scale: Factor Structure and Validation of the Self-Report Version in a Forensic Sample of Belgian Youth. Assessment 2022, 30, 1302–1320. [Google Scholar] [CrossRef]
- López-Romero, L.; Cutrín, O.; Maneiro, L.; Salekin, R.T. Proposed Specifiers for Conduct Disorder-Short Version (PSCD-SV): Psychometric Properties, Concurrent Correlates and Parenting Predictors. Child Psychiatry Hum. Dev. 2022, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Bellamy, N.A.; Salekin, R.T.; Makol, B.A.; Augenstein, T.M.; De Los Reyes, A. The Proposed Specifiers for Conduct Disorder–Parent (PSCD-P): Convergent Validity, Incremental Validity, and Reactions to Unfamiliar Peer Confederates. Res. Child Adolesc. Psychopathol. 2023, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Andershed, H.; Colins, O.F.; Salekin, R.T.; Lordos, A.; Kyranides, M.N.; Fanti, K.A. Callous-Unemotional Traits Only Versus the Multidimensional Psychopathy Construct as Predictors of Various Antisocial Outcomes During Early Adolescence. J. Psychopathol. Behav. Assess. 2018, 40, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Bergstrøm, H.; Larmour, S.R.; Farrington, D.P. The usefulness of psychopathy in explaining and predicting violence: Discussing the utility of competing perspectives. Aggress. Violent Behav. 2018, 42, 84–95. [Google Scholar] [CrossRef]
- Frogner, L.; Gibson, C.L.; Andershed, A.-K.; Andershed, H. Childhood psychopathic personality and callous–unemotional traits in the prediction of conduct problems. Am. J. Orthopsychiatry 2018, 88, 211–225. [Google Scholar] [CrossRef]
- Fontaine, N.M.G.; Mccrory, E.J.P.; Boivin, M.; Moffitt, T.E. Predictors and Outcomes of Joint Trajectories of Callous-Unemotional Traits and Conduct Problems in Childhood. J. Abnorm. Psychol. 2011, 120, 730–742. [Google Scholar] [CrossRef]
- Frick, P.J.; Ray, J.V.; Thornton, L.C.; Kahn, R.E. Can Callous-Unemotional Traits Enhance the Understanding, Diagnosis, and Treatment of Serious Conduct Problems in Children and Adolescents? A comprehensive review. Psychol. Bull. 2013, 140, 1–57. [Google Scholar] [CrossRef]
- Milledge, S.V.; Cortese, S.; Thompson, M.; McEwan, F.; Rolt, M.; Meyer, B.; Sonuga-Barke, E.; Eisenbarth, H. Peer relationships and prosocial behaviour differences across disruptive behaviours. Eur. Child Adolesc. Psychiatry 2019, 28, 781–793. [Google Scholar] [CrossRef]
- Wendt, G.W.; Bartoli, A.J.; Arteche, A. Dimensions of youth psychopathy differentially predict concurrent pro- and antisocial behavior. Braz. J. Psychiatry 2017, 39, 267–270. [Google Scholar] [CrossRef]
- Viding, E.; McCrory, E. Towards understanding atypical social affiliation in psychopathy. Lancet Psychiatry 2019, 6, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Frick, P.J.; Ray, J.V. Evaluating Callous-Unemotional Traits as a Personality Construct. J. Pers. 2015, 83, 710–722. [Google Scholar] [CrossRef] [PubMed]
- Duckitt, J.; Sibley, C.G. Personality, ideology, prejudice, and politics: A dual-process motivational model. J. Pers. 2010, 78, 1861–1894. [Google Scholar] [CrossRef] [PubMed]
- Pratto, F.; Sidanius, J.; Stallworth, L.M.; Malle, B.F. Social dominance orientation: A personality variable predicting social and political attitudes. J. Pers. Soc. Psychol. 1994, 67, 741. [Google Scholar] [CrossRef]
- Sidanius, J.; Pratto, F. Social Dominance: An Intergroup Theory of Social Hierarchy and Oppression; Cambridge University Press: Cambridge, UK, 2001; ISBN 0521805406. [Google Scholar]
- Duckitt, J.; Wagner, C.; Du Plessis, I.; Birum, I. The psychological bases of ideology and prejudice: Testing a dual process model. J. Pers. Soc. Psychol. 2002, 83, 75. [Google Scholar] [CrossRef]
- Ekehammar, B.; Akrami, N.; Gylje, M.; Zakrisson, I. What matters most to prejudice: Big five personality, social dominance orientation, or right-wing authoritarianism? Eur. J. Pers. 2004, 18, 463–482. [Google Scholar] [CrossRef]
- Heaven, P.C.L.; Bucci, S. Right-wing authoritarianism, social dominance orientation and personality: An analysis using the IPIP measure. Eur. J. Pers. 2001, 15, 49–56. [Google Scholar] [CrossRef]
- Cillessen, A.H.N.; Marks, P.E.L. Conceptualizing and measuring popularity. Pop. Peer Syst. 2011, 1, 25–56. [Google Scholar]
- Volk, A.A.; Provenzano, D.A.; Farrell, A.H.; Dane, A.V.; Shulman, E.P. Personality and bullying: Pathways to adolescent social dominance. Curr. Psychol. 2021, 40, 2415–2426. [Google Scholar] [CrossRef]
- Kaufman, J.; Birmaher, B.; Brent, D.; Rao, U.; Flynn, C.; Moreci, P.; Williamson, D.; Ryan, N. Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL): Initial reliability and validity data. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 980–988. [Google Scholar] [CrossRef]
- Ribeiro da Silva, D.; Sousa, R.; Rijo, D.; Mendez, B.; Tsang, S.; Salekin, R.T. Proposed Specifiers for Conduct Disorder (PSCD): Factor Structure and Validation of the Self-Report Version in Community and Forensic Samples of Portuguese Youth. Assessment 2021, 30, 124–143. [Google Scholar] [CrossRef] [PubMed]
- Di Stefano, G.; Roccato, M. Una banca dati per misurare l’orientamento alla dominanza sociale in Italia. TPM. Test. PSICOMETRIA Metodol. 2005, 12, 5–20. [Google Scholar]
- Goodman, R. The strengths and difficulties questionnaire: A research note. J. Child Psychol. Psychiatry Allied Discip. 1997, 38, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Li, J.B.; Delvecchio, E.; Di Riso, D.; Lis, A.; Salcuni, S. Early Evidence of the Italian Parent-Report Strengths and Difficulties Questionnaire (SDQ-P). Child Psychiatry Hum. Dev. 2017, 48, 335–345. [Google Scholar] [CrossRef]
- Tobia, V.; Marzocchi, G.M. The Strengths and Difficulties Questionnaire-Parents for Italian School-Aged Children: Psychometric Properties and Norms. Child Psychiatry Hum. Dev. 2018, 49, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Goodman, A.; Lamping, D.L.; Ploubidis, G.B. When to Use Broader Internalising and Externalising Subscales Instead of the Hypothesised Five Subscales on the Strengths and Difficulties Questionnaire (SDQ): Data from British Parents, Teachers and Children. J. Abnorm. Child Psychol. 2010, 38, 1179–1191. [Google Scholar] [CrossRef] [PubMed]
- Preacher, K.J.; Hayes, A.F. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav. Res. Methods Instrum. Comput. 2004, 36, 717–731. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2017; ISBN 1462534651. [Google Scholar]
- Glenn, A.L.; Efferson, L.M.; Iyer, R.; Graham, J. Values, goals, and motivations associated with psychopathy. J. Soc. Clin. Psychol. 2017, 36, 108–125. [Google Scholar] [CrossRef]
- Schwartz, S.H. Universals in the content and structure of values: Theoretical advances and empirical tests in 20 countries. In Advances in Experimental Social Psychology; Elsevier: Amsterdam, The Netherlands, 1992; Volume 25, pp. 1–65. ISBN 0065-2601. [Google Scholar]
- Kasser, T.; Ryan, R.M. Further Examining the American Dream: Differential Correlates of Intrinsic and Extrinsic Goals. Personal. Soc. Psychol. Bull. 2016, 22, 280–287. [Google Scholar] [CrossRef]
- Sheldon, K.M.; Sheldon, M.S.; Osbaldiston, R. Prosocial values and group assortation: Within an N-person prisoner’s dilemma game. Hum. Nat. 2000, 11, 387–404. [Google Scholar] [CrossRef]
- Frick, P.J.; Ray, J.V.; Thornton, L.C.; Kahn, R.E. Annual research review: A developmental psychopathology approach to understanding callous-unemotional traits in children and adolescents with serious conduct problems. J. Child Psychol. Psychiatry Allied Discip. 2014, 55, 532–548. [Google Scholar] [CrossRef] [PubMed]
- Hawley, P.H. Prosocial and coercive configurations of resource control in early adolescence: A case for the well-adapted Machiavellian. Merrill-Palmer Q. 2003, 49, 279–309. [Google Scholar] [CrossRef]
- Pellegrini, A.D.; Bartini, M. Dominance in early adolescent boys: Affiliative and aggressive dimensions and possible functions. Merrill-Palmer Q. 2001, 47, 142–163. [Google Scholar] [CrossRef]
- Glenn, A.L.; Iyer, R.; Graham, J.; Koleva, S.; Haidt, J. Are all types of morality compromised in psychopathy? J. Pers. Disord. 2009, 23, 384–398. [Google Scholar] [CrossRef]
- Hare, R. Manual for the Revised Psychopathy Checklist; Multi-Health Systems: Toronto, ON, Canada, 2003. [Google Scholar]
- Levantini, V.; Muratori, P.; Calderoni, S.; Inguaggiato, E.; Masi, G.; Milone, A.; Tonacci, A.; Billeci, L. Psychopathic traits and emotion processing in a clinical sample of children with disruptive behavior disorder. Curr. Psychol. 2022, 1, 1–10. [Google Scholar] [CrossRef]
- Fantozzi, P.; Muratori, P.; Levantini, V.; Mammarella, I.; Masi, G.; Milone, A.; Petrucci, A.; Ricci, F.; Tacchi, A.; Cristofani, C. Callous–Unemotional Traits and Intelligence in Children with Externalizing Behavioral Problems. Children 2022, 9, 1768. [Google Scholar] [CrossRef]
- Yaros, A.; Lochman, J.E.; Rosenbaum, J.; Jimenez-Camargo, L.A. Real-time hostile attribution measurement and aggression in children. Aggress. Behav. 2014, 40, 409–420. [Google Scholar] [CrossRef]
- Muratori, P.; Paciello, M.; Buonanno, C.; Milone, A.; Ruglioni, L.; Lochman, J.E.; Masi, G. Moral disengagement and callous–unemotional traits: A longitudinal study of Italian adolescents with a disruptive behaviour disorder. Crim. Behav. Ment. Health 2017, 27, 514–524. [Google Scholar] [CrossRef]
- Paciello, M.; Ballarotto, G.; Cerniglia, L.; Muratori, P. Does the Interplay of Callous-Unemotional Traits and Moral Disengagement Underpin Disruptive Behavior? A Systematic Review. Adolesc. Health. Med. Ther. 2020, 11, 9–20. [Google Scholar] [CrossRef]
- Brummelman, E.; Thomaes, S.; Nelemans, S.A.; de Castro, B.O.; Bushman, B.J. My child is god’s gift to humanity: Development and validation of the parental overvaluation scale (POS). J. Pers. Soc. Psychol. 2015, 108, 665–679. [Google Scholar] [CrossRef]
- Borkovec, T.D.; Newman, M.G.; Pincus, A.L.; Lytle, R. A component analysis of cognitive-behavioral therapy for generalized anxiety disorder and the role of interpersonal problems. J. Consult. Clin. Psychol. 2002, 70, 288. [Google Scholar] [CrossRef] [PubMed]
- Everall, R.D.; Paulson, B.L. The therapeutic alliance: Adolescent perspectives. Couns. Psychother. Res. 2002, 2, 78–87. [Google Scholar] [CrossRef]
- Harris, G.T.; Rice, M.E. Treatment of Psychopathy: A Review of Empirical Findings. In Handbook of Psychopathy; Patrick, C.J., Ed.; The Guilford Press: New York, NY, USA, 2006; pp. 555–572. [Google Scholar]
- Salcido, C.G.; Ray, J.V.; Caudy, M.; Viglione, J.; Walter, R.J. Associations between Psychopathic Traits and Readiness for Change: An exploratory analysis. Pers. Individ. Dif. 2019, 141, 86–91. [Google Scholar] [CrossRef]
- Bisback, A.; Reculé, C.; Colins, O.F. Psychopathic Traits, Treatment Engagement, and Their Interrelation in Criminal Justice-Involved Boys: A Cross-Sectional Network Analysis. Res. Child Adolesc. Psychopathol. 2022, 50, 1589–1604. [Google Scholar] [CrossRef] [PubMed]
- Hawley, P.H. The Duality of Human Nature: Coercion and Prosociality in Youths’ Hierarchy Ascension and Social Success. Curr. Dir. Psychol. Sci. 2014, 23, 433–438. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Community Sample (N = 92) | Clinical Sample (N = 29) | ||||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | t | p | d | |
| PSCD total score | 8.58 | 4.42 | 14.00 | 4.04 | −5.97 | <0.001 | −1.25 |
| SDO | 19.68 | 6.60 | 22.96 | 7.58 | −2.22 | 0.028 | −0.48 |
| SDQ—Externalizing | 3.57 | 3.13 | 7.93 | 3.10 | −6.30 | <0.001 | −1.36 |
| SDQ—Prosocial | 8.23 | 1.64 | 6.39 | 1.77 | 5.09 | <0.001 | 1.10 |
| SDO | PSCD | Externalizing Problems | Prosocial Behavior | |
|---|---|---|---|---|
| SDO | - | 0.172 | 0.216 * | −0.239 * |
| PSCD | 0.752 *** | - | 0.609 *** | −0.200 |
| Externalizing Problems | 0.765 *** | 0.509 ** | - | −0.332 ** |
| Prosocial Behavior | −0.677 *** | −0.399 * | −0.750 *** | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grossi, G.; Strappini, F.; Iuliano, E.; Passiatore, Y.; Mancini, F.; Levantini, V.; Masi, G.; Milone, A.; Santaguida, E.; Salekin, R.T.; et al. Psychopathic Traits, Externalizing Problems, and Prosocial Behavior: The Role of Social Dominance Orientation. J. Clin. Med. 2023, 12, 3521. https://doi.org/10.3390/jcm12103521
Grossi G, Strappini F, Iuliano E, Passiatore Y, Mancini F, Levantini V, Masi G, Milone A, Santaguida E, Salekin RT, et al. Psychopathic Traits, Externalizing Problems, and Prosocial Behavior: The Role of Social Dominance Orientation. Journal of Clinical Medicine. 2023; 12(10):3521. https://doi.org/10.3390/jcm12103521
Chicago/Turabian StyleGrossi, Giuseppe, Francesca Strappini, Enrico Iuliano, Ylenia Passiatore, Francesco Mancini, Valentina Levantini, Gabriele Masi, Annarita Milone, Erica Santaguida, Randall T. Salekin, and et al. 2023. "Psychopathic Traits, Externalizing Problems, and Prosocial Behavior: The Role of Social Dominance Orientation" Journal of Clinical Medicine 12, no. 10: 3521. https://doi.org/10.3390/jcm12103521