
Influence of Coronal Flaring on the Shaping Ability of Two Heat-Treated Nickel-Titanium Endodontic Files: A Micro-Computed Tomographic Study

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Selection
2.2. Sample Preparation
- -
- HyFlex CM with coronal flaring: mesial canals were flared with One Flare, then instrumented with HyFlex CM (#25/0.04; #25/0.06);
- -
- HyFlex CM (without coronal flaring): mesial canals were instrumented with HyFlex CM without initial flaring;
- -
- 2Shape with coronal flaring: mesial canals were flared with One Flare (#25/0.09, Micro Mega, Besançon, France), then instrumented with 2Shape (#25/0.04 and #25/0.06);
- -
- 2Shape (without coronal flaring): mesial canals were instrumented with 2Shape without initial flaring.
2.3. Micro-CT Analysis
2.4. Root Canal Transportation
2.5. Root Canal Centralization
2.6. Statistical Analysis
3. Results
3.1. Root Canal Transportation
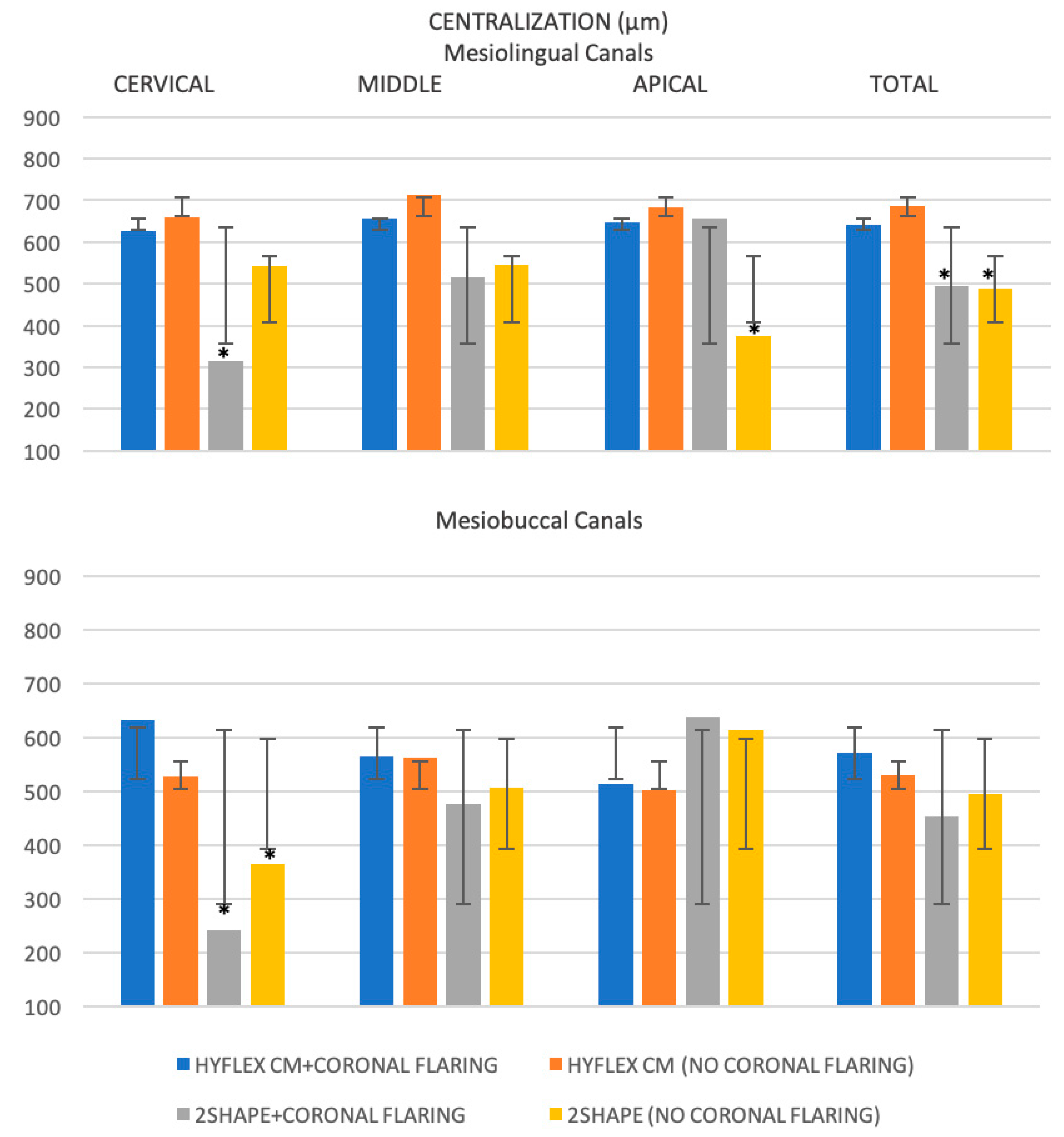
3.2. Root Canal Centralization
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tomson, P.L.; Simon, S.R. Contemporary Cleaning and Shaping of the Root Canal System. Prim. Dent. J. 2016, 5, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.F., Jr.; Pérez, A.R.; Marceliano-Alves, M.F.; Provenzano, J.C.; Silva, S.G.; Pires, F.R.; Vieira, G.C.S.; Rôças, I.N.; Alves, F.R.F. What happens to unprepared root canal walls: A correlative analysis using micro-computed tomography and histology/scanning electron microscopy. Int. Endod. J. 2018, 51, 501–508. [Google Scholar] [CrossRef]
- Taschieri, S.; Necchi, S.; Rosano, G.; Del Fabbro, M.; Weinstein, R.; Machtou, P. Avantages et limites des instruments en nickel-titane pour la préparation canalaire endodontique. Revue de la littérature récente [Advantages and limits of nickel-titanium instruments for root canal preparation. A review of the current literature]. Schweiz. Mon. Zahnmed. 2005, 115, 1000–1005. [Google Scholar]
- Lopes, D.S.; Pessoa, M.A.; Aguiar, C.M. Assessment of the Centralization of Root Canal Preparation with Rotary Systems. Acta Stomatol. Croat. 2016, 50, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Kum, K.Y.; Perinpanayagam, H.; Kim, C.; Kum, D.J.; Lim, S.M.; Chang, S.W.; Baek, S.H.; Zhu, Q.; Yoo, Y.J. Various heat-treated nickel-titanium rotary instruments evaluated in S-shaped simulated resin canals. J. Dent. Sci. 2017, 12, 14–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coltène Whaledent, Switzerland. 2022. Available online: https://nam.coltene.com/pim/DOC/BRO/docbro03464-h-en-hyflex-cm-8-5-x-11-0senaindv1.pdf (accessed on 23 December 2022).
- Micro Mega. 2022. Available online: https://micro-mega.com/wp-content/uploads/2018/03/60301807-C_Brochure-2Shape_EN_WEB.pdf (accessed on 23 December 2022).
- Siang Lin, G.S.; Singbal, K.P.; Abdul Ghani, N.R.N. A Comparative evaluation of the shaping ability, canal straightening, and preparation time of five different NiTi rotary files in simulated canals. J. Conserv. Dent. 2021, 24, 67–71. [Google Scholar] [PubMed]
- Faisal, I.; Saif, R.; Alsulaiman, M.; Natto, Z.S. Shaping ability of 2Shape and NeoNiTi rotary instruments in preparation of curved canals using micro-computed tomography. BMC Oral Health 2021, 21, 595. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, A.; Akbar, I.; AL-Omiri, M.K. An in vivo study to determine the effects of early preflaring on the working length in curved mesial canals of mandibular molars. J. Contemp. Dent. Pract. 2013, 14, 163–167. [Google Scholar]
- Plotino, G.; Nagendrababu, V.; Bukiet, F.; Grande, N.M.; Veettil, S.K.; De-Deus, G.; Aly Ahmed, H.M. Influence of Negotiation, Glide Path, and Preflaring Procedures on Root Canal Shaping-Terminology, Basic Concepts, and a Systematic Review. J. Endod. 2020, 46, 707–729. [Google Scholar] [CrossRef] [PubMed]
- Filho, E.; Rizzi, C.; Neto, J.; Queiroz, R.; Souza, E. Effect of different types of coronal flaring on the circularity and area of mandibular first molar mesial root canals. RGO-Rev. Gaúcha Odontol. 2013, 61, 193–197. [Google Scholar]
- Alqahtani, O.; AbuMostafa, A. Effect of Glide Path and Coronal Flaring on the Centering Ability and Transportation of Root Canals: Micro-CT In Vitro Study. J. Contemp. Dent. Pract. 2021, 22, 1471–1476. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.W. A comparison of canal preparations in straight and curved root canals. Oral Surg. Oral Med. Oral Pathol. 1971, 32, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Gambill, J.M.; Alder, M.; del Rio, C.E. Comparison of nickel-titanium and stainless steel hand-file instrumentation using computed tomography. J. Endod. 1996, 22, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, N.; Leonardi, D.P.; Baechtold, M.S.; Correr, G.M.; Gabardo, M.C.; Zielak, J.C.; Baratto-Filho, F. Influence of cervical preflaring on apical transportation in curved root canals instrumented by reciprocating file systems. BMC Oral Health 2015, 15, 149. [Google Scholar] [CrossRef] [Green Version]
- Ruddle, C. Endodontic Access Prep: Tools for Success. Dent. Prod. 2007, 26, 114–119. [Google Scholar]
- Hannig, C.; Krieger, E.; Dullin, C.; Merten, H.A.; Attin, T.; Grabbe, E.; Heidrich, G. Volumetry of human molars with flat panel-based volume CT in vitro. Clin. Oral Investig. 2006, 10, 253–257. [Google Scholar] [CrossRef]
- García, M.; Duran-Sindreu, F.; Mercadé, M.; Bueno, R.; Roig, M. A comparison of apical transportation between ProFile and RaCe rotary instruments. J. Endod. 2012, 38, 990–992. [Google Scholar] [CrossRef]
- Ba-Hattab, R.A.; Pahncke, D. Shaping Ability of Superelastic and Controlled Memory Nickel-Titanium File Systems: An In Vitro Study. Int. J. Dent. 2018, 2018, 6050234. [Google Scholar] [CrossRef] [Green Version]
- Kandaswamy, D.; Venkateshbabu, N.; Porkodi, I.; Pradeep, G. Canal-centering ability: An endodontic challenge. J. Conserv. Dent. 2009, 12, 3–9. [Google Scholar]
- Ataya, M.; Ha, J.H.; Kwak, S.W.; Abu-Tahun, I.H.; El Abed, R.; Kim, H.C. Mechanical Properties of Orifice Preflaring Nickel-titanium Rotary Instrument Heat Treated Using T-Wire Technology. J. Endod. 2018, 44, 1867–1871. [Google Scholar] [CrossRef]
- Nehme, W.; Araji, S.; Michetti, J.; Zogheib, C.; Naaman, A.; Khalil, I.; Pages, R.; Basarab, A.; Mallet, J.P.; Diemer, F. Assessment of root canal transportation of 2Shape and ProTaper gold in mandibular molar mesial canals: A micro-computed tomographic study. Microsc. Res. Tech. 2021, 84, 746–752. [Google Scholar] [CrossRef] [PubMed]
- Aoun, C.; Nehme, W.; Naaman, A.; Khalil, I. Review and classification of heat treatment procedures and their impact on mechanical behavior of endodontic. Int. J. Curr. Res. 2017, 9, 51300–51306. [Google Scholar]
- Goo, H.J.; Kwak, S.W.; Ha, J.H.; Pedullà, E.; Kim, H.C. Mechanical Properties of Various Heat-treated Nickel-titanium Rotary Instruments. J. Endod. 2017, 43, 1872–1877. [Google Scholar] [CrossRef] [PubMed]
- Bürklein, S.; Poschmann, T.; Schäfer, E. Shaping ability of different nickel-titanium systems in simulated S-shaped canals with and without glide path. J. Endod. 2014, 40, 1231–1234. [Google Scholar] [CrossRef] [PubMed]
- Kishore, A.; Gurtu, A.; Bansal, R.; Singhal, A.; Mohan, S.; Mehrotra, A. Comparison of canal transportation and centering ability of Twisted Files, HyFlex controlled memory, and Wave One using computed tomography scan: An in vitro study. J. Conserv. Dent. 2017, 20, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Chi, C.W.; Lai, E.H.; Liu, C.Y.; Lin, C.P.; Shin, C.S. Influence of heat treatment on cyclic fatigue and cutting efficiency of ProTaper Universal F2 instruments. J. Dent. Sci. 2017, 12, 21–26. [Google Scholar] [CrossRef]
- Sousa-Neto, M.D.; Silva-Sousa, Y.C.; Mazzi-Chaves, J.F.; Carvalho, K.K.T.; Barbosa, A.F.S.; Versiani, M.A.; Jacobs, R.; Leoni, G.B. Root canal preparation using micro-computed tomography analysis: A literature review. Braz. Oral Res. 2018, 32, e66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freire, L.G.; Gavini, G.; Branco-Barletta, F.; Sanches-Cunha, R.; dos Santos, M. Microscopic computerized tomographic evaluation of root canal transportation prepared with twisted or ground nickel-titanium rotary instruments. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 112, e143–e148. [Google Scholar] [CrossRef] [Green Version]
- Peters, O.A.; Laib, A.; Rüegsegger, P.; Barbakow, F. Three-dimensional analysis of root canal geometry by high-resolution computed tomography. J. Dent. Res. 2000, 79, 1405–1409. [Google Scholar] [CrossRef]
- De-Deus, G.; Rodrigues, E.A.; Belladonna, F.G.; Simões-Carvalho, M.; Cavalcante, D.M.; Oliveira, D.S.; Souza, E.M.; Giorgi, K.A.; Versiani, M.A.; Lopes, R.T.; et al. Anatomical danger zone reconsidered: A micro-CT study on dentine thickness in mandibular molars. Int. Endod. J. 2019, 52, 1501–1507. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Root Canal Transportation (mm) | ||||
|---|---|---|---|---|
| Root Canal Thirds | HyFlex CM+Coronal Flaring | HyFlex CM (No Coronal Flaring) | 2Shape+Coronal Flaring | 2Shape (No Coronal Flaring) |
| Cervical | 0.115 a ± 0.048 | 0.147 a ± 0.071 | 0.247 b,* ± 0.115 | 0.216 b,* ± 0.117 |
| Middle | 0.090 a ± 0.066 | 0.079 a ± 0.037 | 0.073 a ± 0.047 | 0.121 a ± 0.084 |
| Apical | 0.049 a,b ± 0.021 | 0.056 a,b ± 0.039 | 0.024 a ± 0.020 | 0.065 b ± 0.037 |
| Total | 0.084 a ± 0.045 | 0.031 a ± 0.049 | 0.114 a ± 0.060 | 0.134 a ± 0.079 |
| Root Canal Centralization (mm) | ||||
|---|---|---|---|---|
| Root Canal Thirds | HyFlex CM+Coronal Flaring | HyFlex CM (No Coronal Flaring) | 2Shape+Coronal Flaring | 2Shape (No Coronal Flaring) |
| Cervical | 0.629 a ± 0.117 | 0.594 a ± 0.137 | 0.278 b ± 0.246 | 0.455 b ± 0.170 |
| Middle | 0.612 a ± 0.104 | 0.639 a ± 0.185 | 0.496 a ± 0.192 | 0.527 a ± 0.184 |
| Apical | 0.580 a,b ± 0.112 | 0.593 a,b ± 0.178 | 0.647 a ± 0.199 | 0.495 b ± 0.162 |
| Total | 0.607 a ± 0.111 | 0.608 a ± 0.166 | 0.473 a ± 0.212 | 0.492 a ± 0.172 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hawi, N.; Pedullà, E.; La Rosa, G.R.M.; Conte, G.; Nehme, W.; Neelakantan, P. Influence of Coronal Flaring on the Shaping Ability of Two Heat-Treated Nickel-Titanium Endodontic Files: A Micro-Computed Tomographic Study. J. Clin. Med. 2023, 12, 357. https://doi.org/10.3390/jcm12010357
Hawi N, Pedullà E, La Rosa GRM, Conte G, Nehme W, Neelakantan P. Influence of Coronal Flaring on the Shaping Ability of Two Heat-Treated Nickel-Titanium Endodontic Files: A Micro-Computed Tomographic Study. Journal of Clinical Medicine. 2023; 12(1):357. https://doi.org/10.3390/jcm12010357
Chicago/Turabian StyleHawi, Nadine, Eugenio Pedullà, Giusy Rita Maria La Rosa, Gianluca Conte, Walid Nehme, and Prasanna Neelakantan. 2023. "Influence of Coronal Flaring on the Shaping Ability of Two Heat-Treated Nickel-Titanium Endodontic Files: A Micro-Computed Tomographic Study" Journal of Clinical Medicine 12, no. 1: 357. https://doi.org/10.3390/jcm12010357