
Worsened Anxiety and Loneliness Influenced Gaming and Gambling during the COVID-19 Pandemic
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
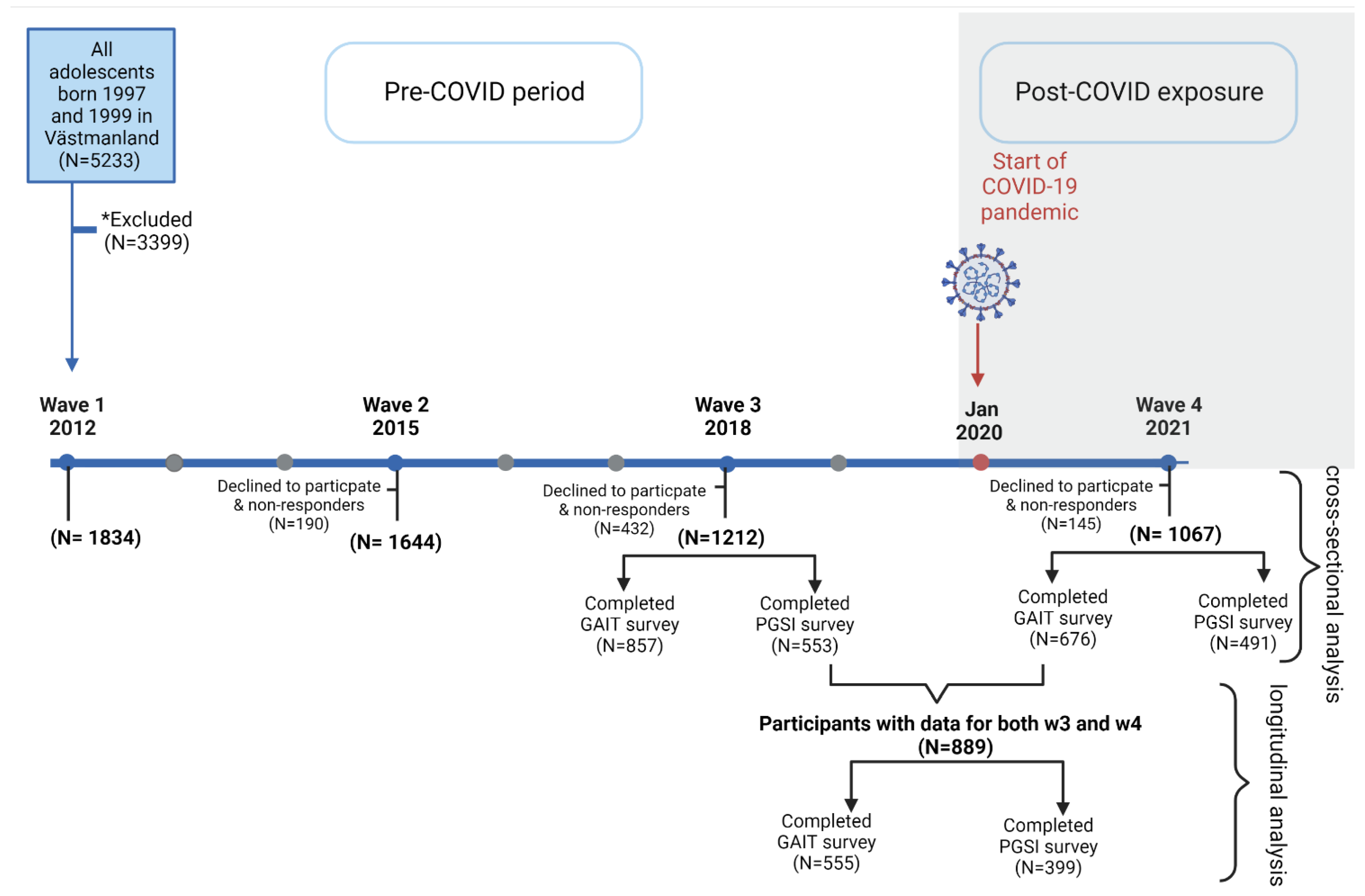
2.1. Participants
2.2. Measurements
2.3. Control Variables
2.4. Statistical Analysis
3. Results
3.1. Descriptive Attributes of w4 and w3 Participants
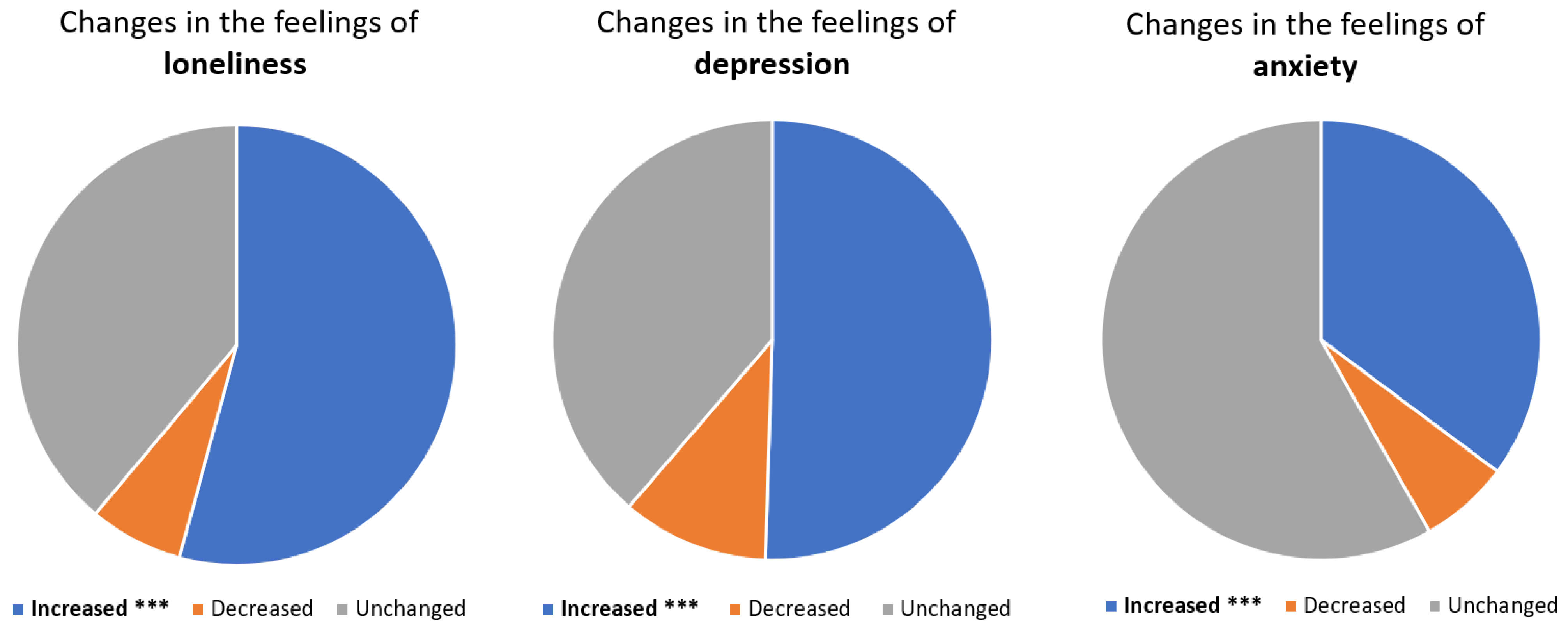
3.2. Changes in Gaming and Gambling Patterns during the COVID-19 Pandemic
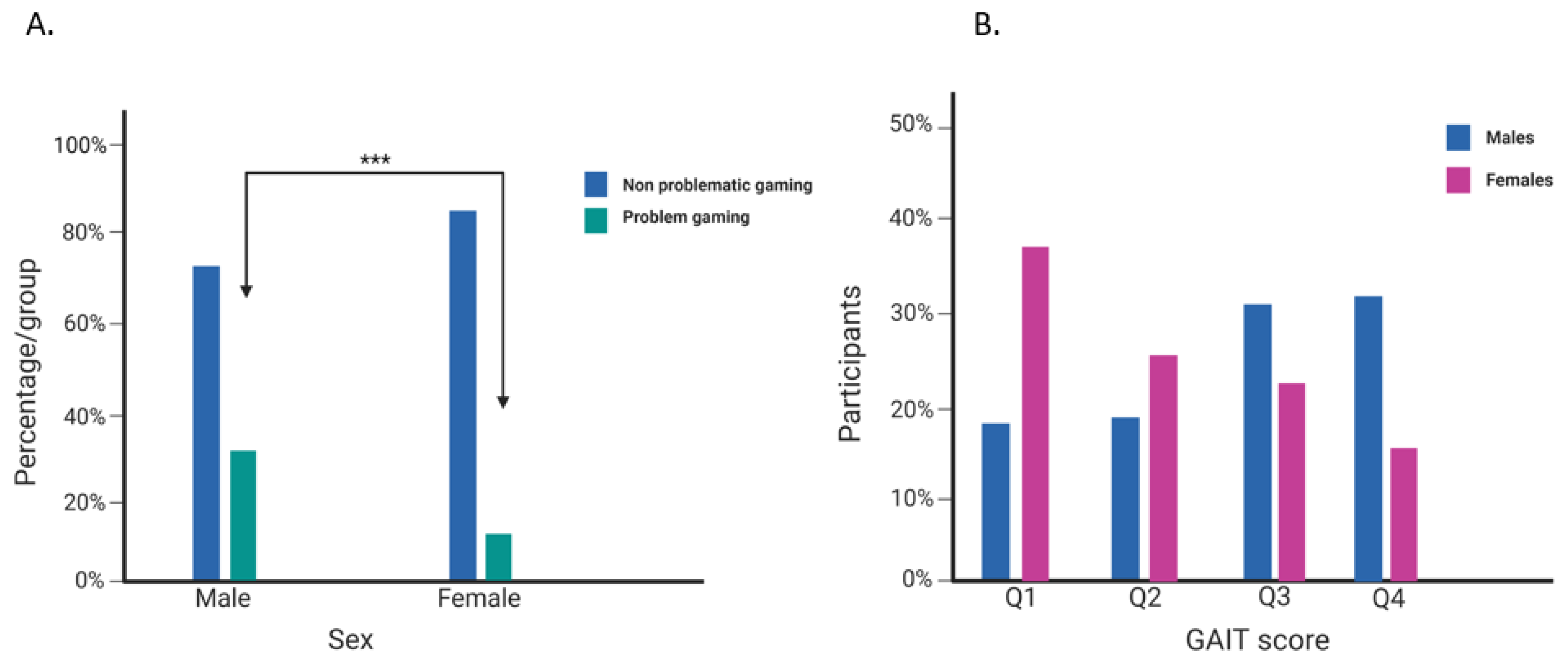
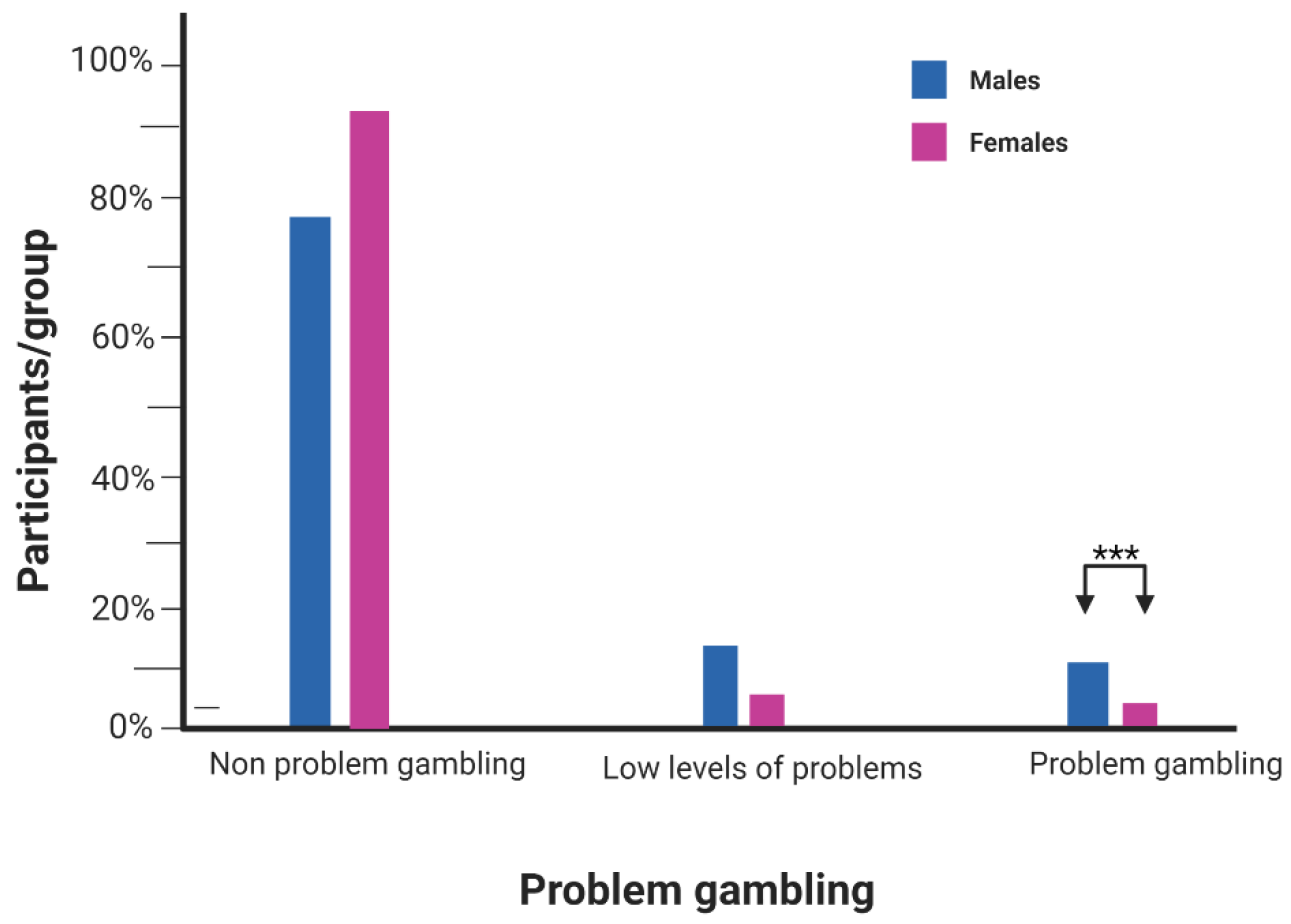
3.3. Cross-Sectional Association between Psychiatric Traits and Problematic Gaming and Gambling in SALVe Cohort at Wave 4
3.4. Longitudinal Association between Psychiatric Traits and Problematic Gaming and Gambling in SALVe Cohort at Wave 4
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Willoughby, T. A short-term longitudinal study of Internet and computer game use by adolescent boys and girls: Prevalence, frequency of use, and psychosocial predictors. Dev. Psychol. 2008, 44, 195–204. [Google Scholar] [CrossRef] [Green Version]
- Trepte, S.; Reinecke, L.; Juechems, K. The social side of gaming: How playing online computer games creates online and offline social support. Comput. Hum. Behav. 2012, 28, 832–839. [Google Scholar] [CrossRef]
- Schneider, L.A.; King, D.L.; Delfabbro, P.H. Maladaptive Coping Styles in Adolescents with Internet Gaming Disorder Symptoms. Int. J. Ment. Health Addict. 2018, 16, 905–916. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing, Inc.: Arlington, VA, USA, 2013; Volume 21, pp. 591–643. [Google Scholar] [CrossRef]
- International Classification of Diseases, Eleventh Revision (ICD-11), World Health Organization (WHO) 2019/2021. Available online: https://icd.who.int/en (accessed on 25 July 2022).
- Petry, N.M.; Rehbein, F.; Ko, C.-H.; O’Brien, C.P. Internet Gaming Disorder in the DSM-5. Curr. Psychiatry Rep. 2015, 17, 72. [Google Scholar] [CrossRef] [PubMed]
- Saunders, J.B.; Hao, W.; Long, J.; King, D.L.; Mann, K.; Fauth-Bühler, M.; Rumpf, H.-J.; Bowden-Jones, H.; Rahimi-Movaghar, A.; Chung, T.; et al. Gaming disorder: Its delineation as an important condition for diagnosis, management, and prevention. J. Behav. Addict. 2017, 6, 271–279. [Google Scholar] [CrossRef] [Green Version]
- Yau, Y.H.C.; Potenza, M.N. Gambling Disorder and Other Behavioral Addictions: Recognition and Treatment. Harv. Rev. Psychiatry 2015, 23, 134–146. [Google Scholar] [CrossRef]
- Lawn, S.; Oster, C.; Riley, B.; Smith, D.; Baigent, M.; Rahamathulla, M. A Literature Review and Gap Analysis of Emerging Technologies and New Trends in Gambling. Int. J. Environ. Res. Public. Health 2020, 17, 744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riley, B.J.; Oster, C.; Rahamathulla, M.; Lawn, S. Attitudes, Risk Factors, and Behaviours of Gambling among Adolescents and Young People: A Literature Review and Gap Analysis. Int. J. Environ. Res. Public. Health 2021, 18, 984. [Google Scholar] [CrossRef]
- Lorains, F.K.; Cowlishaw, S.; Thomas, S.A. Prevalence of comorbid disorders in problem and pathological gambling: Systematic review and meta-analysis of population surveys. Addiction 2011, 106, 490–498. [Google Scholar] [CrossRef]
- Mihara, S.; Higuchi, S. Cross-sectional and longitudinal epidemiological studies of Internet gaming disorder: A systematic review of the literature. Psychiatry Clin. Neurosci. 2017, 71, 425–444. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.-Y.; Wu, Y.-C.; Su, C.-H.; Lin, P.-C.; Ko, C.-H.; Yen, J.-Y. Association between Internet gaming disorder and generalized anxiety disorder. J. Behav. Addict. 2017, 6, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Sundqvist, K.; Wennberg, P. Problem gambling and anxiety disorders in the general swedish population—A case control study. J. Gambl. Stud. 2022, 38, 1257–1268. [Google Scholar] [CrossRef] [PubMed]
- Toneatto, T.; Pillai, S. Mood and Anxiety Disorders Are the Most Prevalent Psychiatric Disorders among Pathological and Recovered Gamblers. Int. J. Ment. Health Addict. 2016, 14, 217–227. [Google Scholar] [CrossRef]
- Rosendo-Rios, V.; Trott, S.; Shukla, P. Systematic literature review online gaming addiction among children and young adults: A framework and research agenda. Addict. Behav. 2022, 129, 107238. [Google Scholar] [CrossRef]
- Carras, M.C.; Shi, J.; Hard, G.; Saldanha, I.J. Evaluating the quality of evidence for gaming disorder: A summary of systematic reviews of associations between gaming disorder and depression or anxiety. PLoS ONE 2020, 15, e0240032. [Google Scholar]
- Boehm, M.A.; Lei, Q.M.; Lloyd, R.M.; Prichard, J.R. Depression, anxiety, and tobacco use: Overlapping impediments to sleep in a national sample of college students. J. Am. Coll. Health 2016, 64, 565–574. [Google Scholar] [CrossRef]
- Fazeli, S.; Mohammadi Zeidi, I.; Lin, C.-Y.; Namdar, P.; Griffiths, M.D.; Ahorsu, D.K.; Pakpour, A.H. Depression, anxiety, and stress mediate the associations between internet gaming disorder, insomnia, and quality of life during the COVID-19 outbreak. Addict. Behav. Rep. 2020, 12, 100307. [Google Scholar] [CrossRef]
- Mental Health and COVID-19: Early Evidence of the Pandemic’s Impact: Scientific Brief. 2 March 2022. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-Sci_Brief-Mental_health-2022.1 (accessed on 7 September 2022).
- COVID-19 Pandemic Triggers 25% Increase in Prevalence of Anxiety and Depression Worldwide. Available online: https://www.who.int/news/item/02-03-2022-covid-19-pandemic-triggers-25-increase-in-prevalence-of-anxiety-and-depression-worldwide (accessed on 8 July 2022).
- Brodeur, M.; Audette-Chapdelaine, S.; Savard, A.-C.; Kairouz, S. Gambling and the COVID-19 pandemic: A scoping review. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 111, 110389. [Google Scholar] [CrossRef]
- Ko, C.-H.; Yen, J.-Y. Impact of COVID-19 on gaming disorder: Monitoring and prevention. J. Behav. Addict. 2020, 9, 187–189. [Google Scholar] [CrossRef]
- Wei, H.-T.; Chen, M.-H.; Huang, P.-C.; Bai, Y.-M. The association between online gaming, social phobia, and depression: An internet survey. BMC Psychiatry 2012, 12, 92. [Google Scholar] [CrossRef]
- Sioni, S.R.; Burleson, M.H.; Bekerian, D.A. Internet gaming disorder: Social phobia and identifying with your virtual self. Comput. Hum. Behav. 2017, 71, 11–15. [Google Scholar] [CrossRef]
- Wang, J.-L.; Sheng, J.-R.; Wang, H.-Z. The Association Between Mobile Game Addiction and Depression, Social Anxiety, and Loneliness. Front. Public Health 2019, 7, 247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, C.-H.; Liu, T.-L.; Wu, H.-C.; Yeh, Y.-C.; Tsai, W.-X.; Yen, J.-Y. Psychiatric comorbidities and emotional intelligence in internet gaming disorder: Attention deficit hyperactivity disorder, major depressive disorder, generalized anxiety disorder, and social anxiety disorder. Psychiatry Clin. Neurosci. 2021, 75, 352–354. [Google Scholar] [CrossRef] [PubMed]
- Petry, N.M.; Stinson, F.S.; Grant, B.F. Comorbidity of DSM-IV pathological gambling and other psychiatric disorders: Results from the National Epidemiologic Survey on Alcohol and Related Conditions. J. Clin. Psychiatry 2005, 66, 564–574. [Google Scholar] [CrossRef]
- Vadlin, S.; Åslund, C.; Nilsson, K.W. Development and content validity of a screening instrument for gaming addiction in adolescents: The Gaming Addiction Identification Test (GAIT). Scand. J. Psychol. 2015, 56, 458–466. [Google Scholar] [CrossRef] [PubMed]
- Vadlin, S.; Åslund, C.; Nilsson, K.W. A longitudinal study of the individual- and group-level problematic gaming and associations with problem gambling among Swedish adolescents. Brain Behav. 2018, 8, e00949. [Google Scholar] [CrossRef]
- Spence, S.; Griffith University, Brisbane, QLD, Australia. The Adult Anxiety Scale-15 (AAS-15). Personal communication, 2017. [Google Scholar]
- Assanangkornchai, S.; McNeil, E.B.; Tantirangsee, N.; Kittirattanapaiboon, P. Gambling disorders, gambling type preferences, and psychiatric comorbidity among the Thai general population: Results of the 2013 National Mental Health Survey. J. Behav. Addict. 2016, 5, 410–418. [Google Scholar] [CrossRef] [Green Version]
- Blake, M.J.; Trinder, J.A.; Allen, N.B. Mechanisms underlying the association between insomnia, anxiety, and depression in adolescence: Implications for behavioral sleep interventions. Clin. Psychol. Rev. 2018, 63, 25–40. [Google Scholar] [CrossRef]
- Liu, L.; Yao, Y.-W.; Li, C.R.; Zhang, J.-T.; Xia, C.-C.; Lan, J.; Ma, S.-S.; Zhou, N.; Fang, X.-Y. The Comorbidity Between Internet Gaming Disorder and Depression: Interrelationship and Neural Mechanisms. Front. Psychiatry 2018, 9, 154. [Google Scholar] [CrossRef] [Green Version]
- Thorne, H.B.; Rockloff, M.J.; Ferguson, S.A.; Vincent, G.E.; Browne, M. Gambling Problems Are Associated with Alcohol Misuse and Insomnia: Results from a Representative National Telephone Survey. Int. J. Environ. Res. Public. Health 2021, 18, 6683. [Google Scholar] [CrossRef]
- Isaksson, J.; Vadlin, S.; Olofsdotter, S.; Åslund, C.; Nilsson, K.W. Psychotic-like experiences during early adolescence predict symptoms of depression, anxiety, and conduct problems three years later: A community-based study. Schizophr. Res. 2020, 215, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Nordin, M.; Åkerstedt, T.; Nordin, S. Psychometric evaluation and normative data for the Karolinska Sleep Questionnaire. Sleep Biol. Rhythm. 2013, 11, 216–226. [Google Scholar] [CrossRef]
- Claeson, M.; Hanson, S. COVID-19 and the Swedish enigma. Lancet 2021, 397, 259–261. [Google Scholar] [CrossRef]
- Tegnell, A. The Swedish public health response to COVID-19. APMIS 2021, 129, 320–323. [Google Scholar] [CrossRef]
- Pashakhanlou, A.H. Sweden’s coronavirus strategy: The Public Health Agency and the sites of controversy. World Med. Health Policy 2022, 14, 507–527. [Google Scholar] [CrossRef]
- Paterlini, M. What now for Sweden and covid-19? BMJ 2021, 375, n3081. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.M.; Badinlou, F.; Buhrman, M.; Brocki, K.C. Psychological impact of COVID-19 in the Swedish population: Depression, anxiety, and insomnia and their associations to risk and vulnerability factors. Eur. Psychiatry 2020, 63, e81. [Google Scholar] [CrossRef]
- Berman, A.H.; Bendtsen, M.; Molander, O.; Lindfors, P.; Lindner, P.; Granlund, L.; Topooco, N.; Engström, K.; Andersson, C. Compliance with recommendations limiting COVID-19 contagion among university students in Sweden: Associations with self-reported symptoms, mental health and academic self-efficacy. Scand. J. Public Health 2022, 50, 70–84. [Google Scholar] [CrossRef]
- Cudo, A.; Kopiś, N.; Zabielska-Mendyk, E. Personal distress as a mediator between self-esteem, self-efficacy, loneliness and problematic video gaming in female and male emerging adult gamers. PLoS ONE 2019, 14, e0226213. [Google Scholar] [CrossRef] [Green Version]
- Koban, K.; Biehl, J.; Bornemeier, J.; Ohler, P. Compensatory video gaming. Gaming behaviours and adverse outcomes and the moderating role of stress, social interaction anxiety, and loneliness. Behav. Inf. Technol. 2021, 41, 2727–2744. [Google Scholar] [CrossRef]
- Elhai, J.D.; McKay, D.; Yang, H.; Minaya, C.; Montag, C.; Asmundson, G.J.G. Health anxiety related to problematic smartphone use and gaming disorder severity during COVID-19: Fear of missing out as a mediator. Hum. Behav. Emerg. Technol. 2021, 3, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Oka, T.; Hamamura, T.; Miyake, Y.; Kobayashi, N.; Honjo, M.; Kawato, M.; Kubo, T.; Chiba, T. Prevalence and risk factors of internet gaming disorder and problematic internet use before and during the COVID-19 pandemic: A large online survey of Japanese adults. J. Psychiatr. Res. 2021, 142, 218–225. [Google Scholar] [CrossRef] [PubMed]
- Konkolÿ Thege, B.; Woodin, E.M.; Hodgins, D.C.; Williams, R.J. Natural course of behavioral addictions: A 5-year longitudinal study. BMC Psychiatry 2015, 15, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rothmund, T.; Klimmt, C.; Gollwitzer, M. Low Temporal Stability of Excessive Video Game Use in German Adolescents. J. Media Psychol. 2018, 30, 53–65. [Google Scholar] [CrossRef]
- Hodgins, D.C.; Stevens, R.M.G. The impact of COVID-19 on gambling and gambling disorder: Emerging data. Curr. Opin. Psychiatry 2021, 34, 332–343. [Google Scholar] [CrossRef]
- Welte, J.W.; Barnes, G.M.; Tidwell, M.-C.O.; Wieczorek, W.F. Predictors of Problem Gambling in the U.S. J. Gambl. Stud. 2017, 33, 327–342. [Google Scholar] [CrossRef]
- Wartberg, L.; Kriston, L.; Zieglmeier, M.; Lincoln, T.; Kammerl, R. A longitudinal study on psychosocial causes and consequences of Internet gaming disorder in adolescence. Psychol. Med. 2019, 49, 287–294. [Google Scholar] [CrossRef]
- Marmet, S.; Studer, J.; Wicki, M.; Khazaal, Y.; Gmel, G. Online Gambling’s Associations With Gambling Disorder and Related Problems in a Representative Sample of Young Swiss Men. Front. Psychiatry 2021, 12, 703118. [Google Scholar] [CrossRef]
- Li, W.; Mills, D.; Nower, L. The relationship of loot box purchases to problem video gaming and problem gambling. Addict. Behav. 2019, 97, 27–34. [Google Scholar] [CrossRef]
- Ohayon, M.M.; Roberts, L. Internet gaming disorder and comorbidities among campus-dwelling U.S. university students. Psychiatry Res. 2021, 302, 114043. [Google Scholar] [CrossRef]
- Van Rooij, A.J.; Schoenmakers, T.M.; Vermulst, A.A.; Van Den Eijnden, R.J.J.M.; Van De Mheen, D. Online video game addiction: Identification of addicted adolescent gamers. Addiction 2011, 106, 205–212. [Google Scholar] [CrossRef]
- González-Bueso, V.; Santamaría, J.J.; Fernández, D.; Merino, L.; Montero, E.; Ribas, J. Association between Internet Gaming Disorder or Pathological Video-Game Use and Comorbid Psychopathology: A Comprehensive Review. Int. J. Environ. Res. Public. Health 2018, 15, 668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marino, C.; Canale, N.; Vieno, A.; Caselli, G.; Scacchi, L.; Spada, M.M. Social anxiety and Internet gaming disorder: The role of motives and metacognitions. J. Behav. Addict. 2020, 9, 617–628. [Google Scholar] [CrossRef] [PubMed]
- Krossbakken, E.; Pallesen, S.; Mentzoni, R.A.; King, D.L.; Molde, H.; Finserås, T.R.; Torsheim, T. A Cross-Lagged Study of Developmental Trajectories of Video Game Engagement, Addiction, and Mental Health. Front. Psychol. 2018, 9, 2239. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Wave 3 (N = 1212) | Wave 4 (N = 1067) | * Longitudinal Analysis (N = 889) | |
|---|---|---|---|---|
| Scale Mean (SD) | ||||
| Age | 20.10 (1.09) | 22.9 (1.04) | 22.9 (1.04) | |
| Sleep/insomnia (KSQ) | 26.25 (14.25) | 26.64 (14.29) | 26.63 (14.34) | |
| Deprssion (DSRS) | 3.09 (2.84) | 3.36 (2.86) | 3.33 (2.83) | |
| Gaming (GAIT) | 5.76 (7.69) | 5.88 (7.80) | 5.70 (7.50) | |
| Average time spent in video game/day (hours) | 2.18(2.13) | 1.71(2.049) | 1.66 (2.01) | |
| Gambling (PGSI) | 0.51 (1.79) | 0.61 (2.57) | 0.36 (1.23) | |
| Categorical N (%) | ||||
| Sex | Male | 458 (37.8%) | 380 (35.6%) | 300 (33.7%) |
| Female | 754 (62.2%) | 687 (64.4%) | 589 (66.3%) | |
| Gaming (GAIT) | No problem | 647 (75.5%) | 519 (76.8%) | 430 (77.5%) |
| Problem gaming | 210 (24.5%) | 157 (23.2%) | 125 (22.5%) | |
| Gambling (PGSI) | No problem | 457 (82.6%) | 415 (84.5%) | 344 (86.2%) |
| Low level of problems | 65 (11.8%) | 44 (9%) | 35 (8.8%) | |
| Problem gambling | 31 (5.6%) | 32 (6.5%) | 20 (5.0%) | |
| Characteristic | Increased during the Pandemic N (%) | Decreased during the Pandemic N (%) | Unchanged N (%) | Never Played before nor after the Pandemic N (%) |
|---|---|---|---|---|
| Gaming | 131 (12.3%) | 118 (11.1%) | 408 (38.2%) | 410 (38.4%) |
| Gambling | 18 (1.7%) | 28 (2.6%) | 321 (30.1%) | 700 (65.6%) |
| Anxiety Trait | Model I * | Model II ** | Model III *** | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Odds Ratio | 95% Confidence Interval | p-Value | Odds Ratio | 95% Confidence Interval | p-Value | Odds Ratio | 95% Confidence Interval | p-Value | ||||
| Lower CI | Upper CI | Lower CI | Upper CI | Lower CI | Upper CI | |||||||
| Social anxiety | 1.26 | 1.18 | 1.33 | <0.001 | 1.20 | 1.13 | 1.28 | <0.001 | 1.19 | 1.12 | 1.27 | <0.001 |
| Generalized anxiety | 1.17 | 1.11 | 1.24 | <0.001 | 1.08 | 1.01 | 1.16 | <0.05 | 1.06 | 0.99 | 1.14 | 0.090 |
| Panic | 1.22 | 1.12 | 1.32 | <0.001 | 1.08 | 0.98 | 1.19 | 0.110 | 1.05 | 0.95 | 1.16 | 0.308 |
| Trait | Model I * | Model II ** | Model III *** | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Odds Ratio | 95% Confidence Interval | p-Value | Odds Ratio | 95% Confidence Interval | p-Value | Odds Ratio | 95% Confidence Interval | p-Value | ||||
| Lower CI | Upper CI | Lower CI | Upper CI | Lower CI | Upper CI | |||||||
| Social anxiety | 1.18 | 1.08 | 1.28 | <0.001 | 1.09 | 0.99 | 1.21 | 0.061 | 1.07 | 0.97 | 1.18 | 0.18 |
| Generalized anxiety | 1.22 | 1.11 | 1.33 | <0.001 | 1.13 | 1.02 | 1.26 | <0.05 | 1.08 | 0.97 | 1.22 | 0.17 |
| Panic | 1.36 | 1.22 | 1.51 | <0.001 | 1.29 | 1.14 | 1.45 | <0.001 | 1.23 | 1.08 | 1.39 | <0.01 |
| Problem gaming (GAIT) | 2.87 | 1.48 | 5.54 | <0.01 | 2.36 | 1.22 | 4.57 | <0.05 | 2.38 | 1.22 | 4.65 | <0.05 |
| Traits | Model I * | Model II ** | Model III *** | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Odds Ratio | 95% Confidence Interval | p-Value | Odds Ratio | 95% Confidence Interval | p-Value | Odds Ratio | 95% Confidence Interval | p-Value | ||||
| Lower CI | Upper CI | Lower CI | Upper CI | Lower CI | Upper CI | |||||||
| Social anxiety | 1.17 | 1.10 | 1.25 | <0.001 | 1.14 | 1.07 | 1.22 | <0.001 | 1.13 | 1.06 | 1.21 | <0.001 |
| Generalized anxiety | 1.10 | 1.04 | 1.17 | <0.01 | 1.05 | 0.98 | 1.13 | 0.18 | 1.03 | 0.96 | 1.11 | 0.45 |
| Panic | 1.19 | 1.08 | 1.32 | <0.001 | 1.11 | 0.99 | 1.24 | 0.07 | 1.08 | 0.96 | 1.21 | 0.21 |
| Problem gaming (GAIT) | 4.02 | 2.95 | 5.46 | <0.001 | 3.91 | 2.87 | 5.32 | <0.001 | 3.83 | 2.82 | 5.22 | <0.001 |
| Traits | Model I * | Model II ** | Model III *** | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Odds Ratio | 95% Confidence Interval | p-Value | Odds Ratio | 95% Confidence Interval | p-Value | Odds Ratio | 95% Confidence Interval | p-Value | ||||
| Lower CI | Upper CI | Lower CI | Upper CI | Lower CI | Upper CI | |||||||
| Social anxiety | 1.13 | 1.02 | 1.25 | 0.02 | 1.06 | 0.95 | 1.24 | 0.27 | 1.05 | 0.93 | 1.18 | 0.42 |
| Generalized anxiety | 1.09 | 0.98 | 1.21 | 0.10 | 0.97 | 0.86 | 1.10 | 0.71 | 0.95 | 0.83 | 1.08 | 0.43 |
| Panic | 1.27 | 1.18 | 1.48 | 0.001 | 1.15 | 0.96 | 1.37 | 0.13 | 1.12 | 0.93 | 1.35 | 0.24 |
| Problem gaming (GAIT) | 1.68 | 1.02 | 2.72 | 0.41 | 1.55 | 0.97 | 2.51 | 0.70 | 1.53 | 0.94 | 2.48 | 0.09 |
| Problem gambling (PGSI) | 6.92 | 3.07 | 15.61 | <0.001 | 5.94 | 2.58 | 13.66 | <0.001 | 6.05 | 2.61 | 14.06 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohamed, M.S.; Rukh, G.; Schiöth, H.B.; Vadlin, S.; Olofsdotter, S.; Åslund, C.; Nilsson, K.W. Worsened Anxiety and Loneliness Influenced Gaming and Gambling during the COVID-19 Pandemic. J. Clin. Med. 2023, 12, 249. https://doi.org/10.3390/jcm12010249
Mohamed MS, Rukh G, Schiöth HB, Vadlin S, Olofsdotter S, Åslund C, Nilsson KW. Worsened Anxiety and Loneliness Influenced Gaming and Gambling during the COVID-19 Pandemic. Journal of Clinical Medicine. 2023; 12(1):249. https://doi.org/10.3390/jcm12010249
Chicago/Turabian StyleMohamed, Mohamed S., Gull Rukh, Helgi B. Schiöth, Sofia Vadlin, Susanne Olofsdotter, Cecilia Åslund, and Kent W. Nilsson. 2023. "Worsened Anxiety and Loneliness Influenced Gaming and Gambling during the COVID-19 Pandemic" Journal of Clinical Medicine 12, no. 1: 249. https://doi.org/10.3390/jcm12010249