
Effect of a Targeted Ambulance Treatment Quality Improvement Programme on Outcomes from Out-of-Hospital Cardiac Arrest: A Metropolitan Citywide Intervention Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.3. Intervention
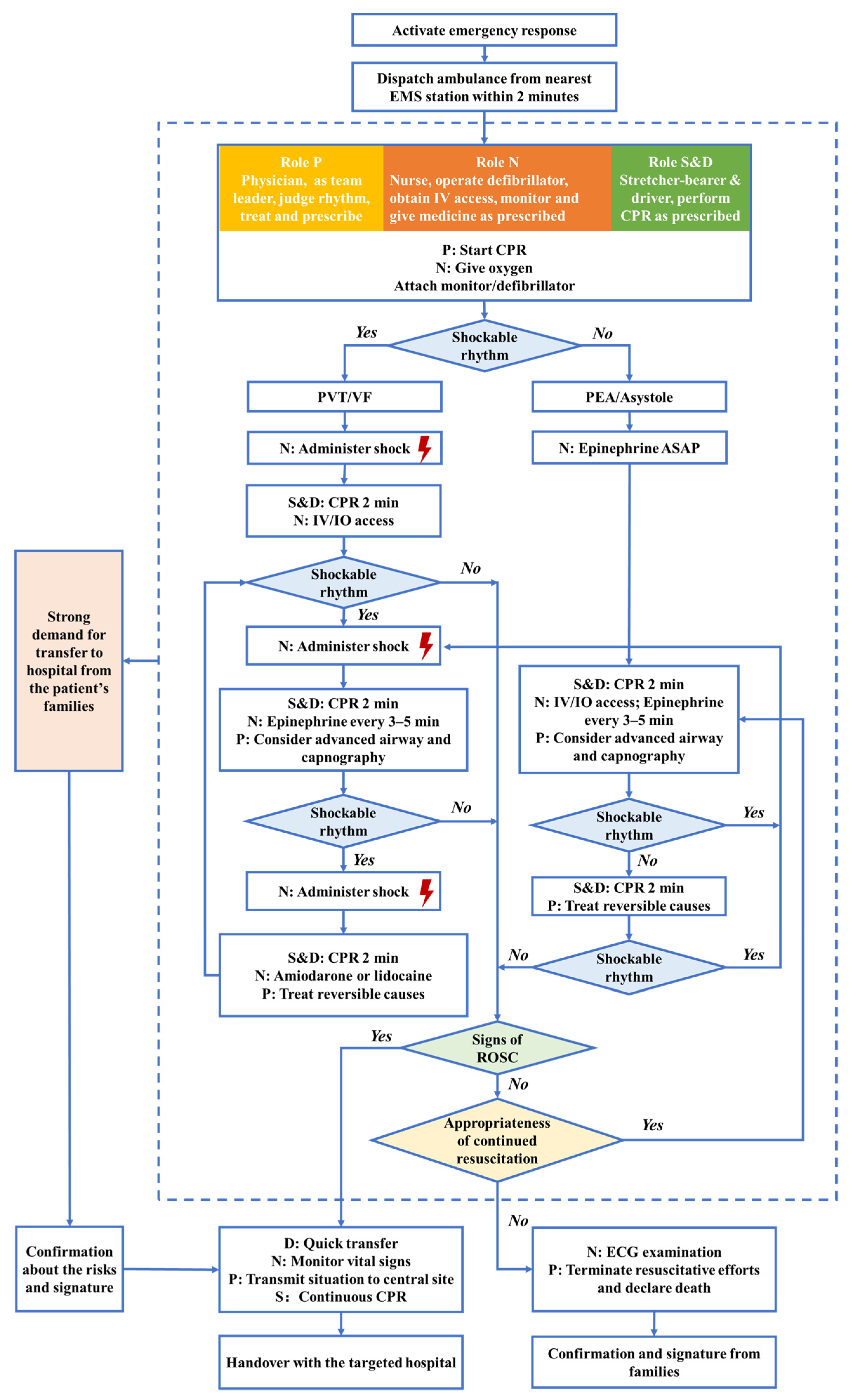
2.3.1. Standardized Ambulance Treatment Protocol Adopted
2.3.2. Ambulance Crew Targeted Training
2.3.3. Quality Monitoring, Feedback, and Post-Event Debriefing
2.4. Data Source
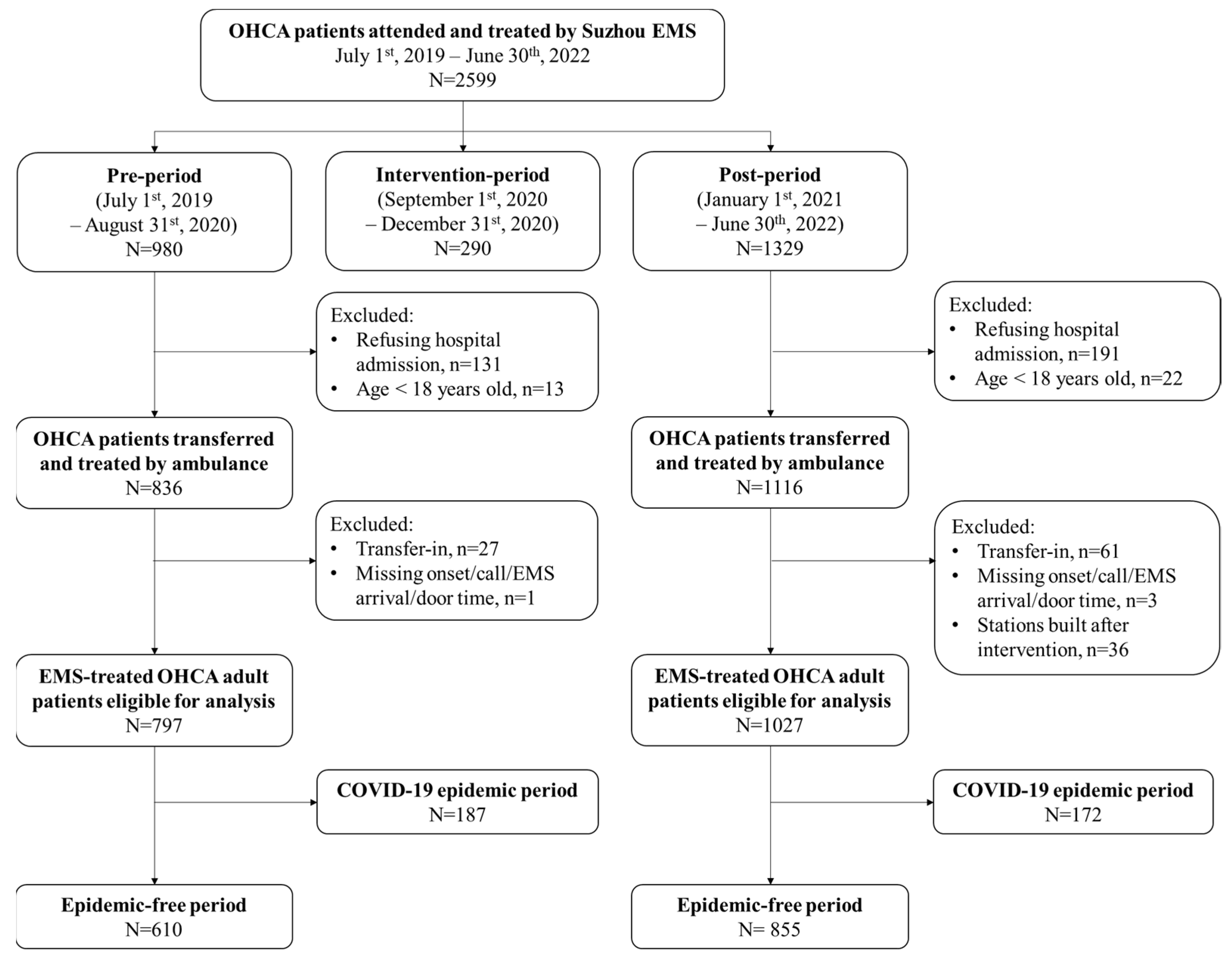
2.5. Study Population
2.6. Data Collection and Outcome Measures
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics
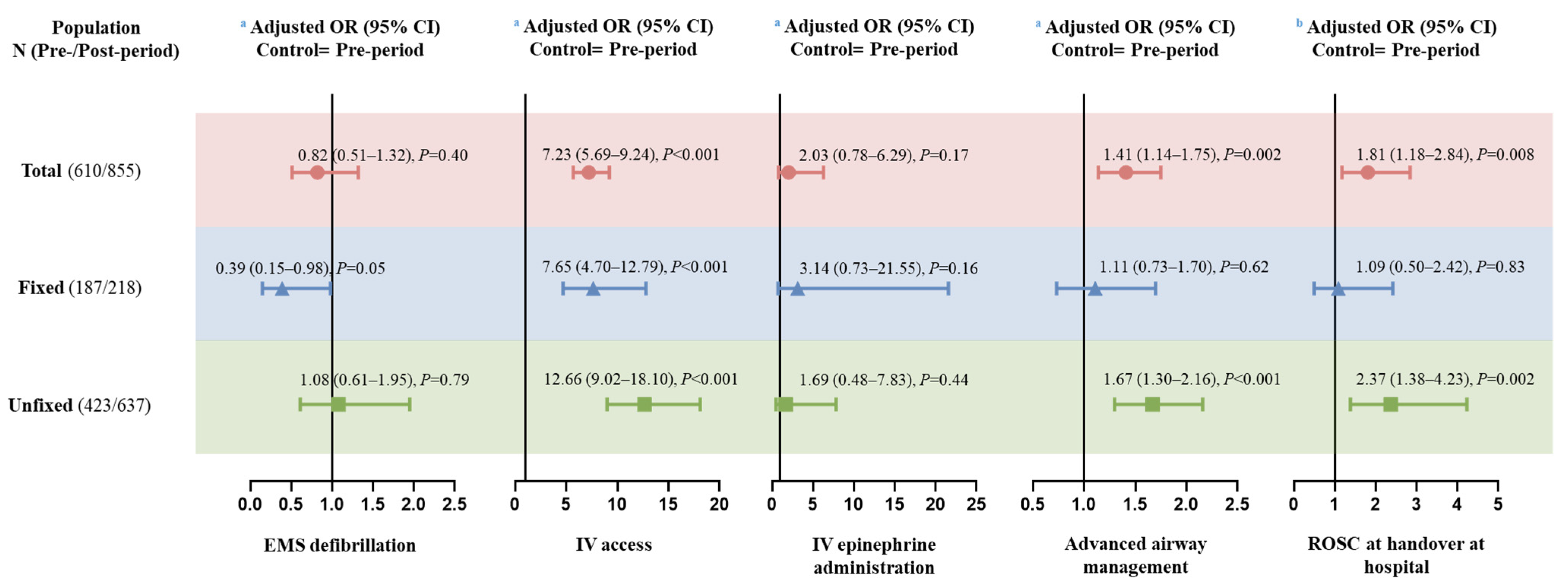
3.2. Main Analysis
3.3. Subgroup Analysis by Types of Ambulance Crew
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Kiguchi, T.; Okubo, M.; Nishiyama, C.; Maconochie, I.; Ong, M.E.H.; Kern, K.B.; Wyckoff, M.H.; McNally, B.; Christensen, E.F.; Tjelmeland, I.; et al. Out-of-hospital cardiac arrest across the world: First report from the international liaison committee on resuscitation (ilcor). Resuscitation 2020, 152, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Xu, F.; Zhang, Y.; Chen, Y. Cardiopulmonary resuscitation training in china: Current situation and future development. JAMA Cardiol. 2017, 2, 469–470. [Google Scholar] [CrossRef] [PubMed]
- Hou, L.; Wang, Y.; Wang, W. Optimization of the pre-hospital rescue system for out-of-hospital cardiac arrest in China. China CDC Wkly. 2022, 4, 52–55. [Google Scholar] [CrossRef] [PubMed]
- Ong, M.E.H.; Perkins, G.D.; Cariou, A. Out-of-hospital cardiac arrest: Prehospital management. Lancet 2018, 391, 980–988. [Google Scholar] [CrossRef] [Green Version]
- Berg, K.M.; Cheng, A.; Panchal, A.R.; Topjian, A.A.; Aziz, K.; Bhanji, F.; Bigham, B.L.; Hirsch, K.G.; Hoover, A.V.; Kurz, M.C.; et al. Part 7: Systems of care: 2020 american heart association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2020, 142, S580–S604. [Google Scholar] [CrossRef]
- Semeraro, F.; Greif, R.; Böttiger, B.; Burkart, R.; Cimpoesu, D.; Georgiou, M.; Yeung, J.; Lippert, F.; Lockey, A.S.; Olasveengen, T.; et al. European resuscitation council guidelines 2021: Systems saving lives. Resuscitation 2021, 161, 80–97. [Google Scholar] [CrossRef]
- Sporer, K.; Jacobs, M.; Derevin, L.; Duval, S.; Pointer, J. Continuous quality improvement efforts increase survival with favorable neurologic outcome after out-of-hospital cardiac arrest. Prehosp. Emerg. Care 2017, 21, 1–6. [Google Scholar] [CrossRef]
- Hwang, W.S.; Park, J.S.; Kim, S.J.; Hong, Y.S.; Moon, S.W.; Lee, S.W. A system-wide approach from the community to the hospital for improving neurologic outcomes in out-of-hospital cardiac arrest patients. Eur. J. Emerg. Med. 2017, 24, 87–95. [Google Scholar] [CrossRef]
- Chen, T.T.; Ma, M.H.; Chen, F.J.; Hu, F.C.; Lu, Y.C.; Chiang, W.C.; Ko, P.C. The relationship between survival after out-of-hospital cardiac arrest and process measures for emergency medical service ambulance team performance. Resuscitation 2015, 97, 55–60. [Google Scholar] [CrossRef]
- Hopkins, C.L.; Burk, C.; Moser, S.; Meersman, J.; Baldwin, C.; Youngquist, S.T. Implementation of pit crew approach and cardiopulmonary resuscitation metrics for out-of-hospital cardiac arrest improves patient survival and neurological outcome. J. Am. Heart Assoc. 2016, 5, e002892. [Google Scholar] [CrossRef]
- Pearson, D.A.; Nelson, R.D.; Monk, L.; Tyson, C.; Jollis, J.G.; Granger, C.B.; Corbett, C.; Garvey, L.; Runyon, M.S. Comparison of team-focused cpr vs standard cpr in resuscitation from out-of-hospital cardiac arrest: Results from a statewide quality improvement initiative. Resuscitation 2016, 105, 165–172. [Google Scholar] [CrossRef] [PubMed]
- GRA. Acting on the Call. 2018. Available online: https://www.globalresuscitationalliance.org/wp-content/pdf/acting_on_the_call.pdf (accessed on 16 August 2022).
- Park, S.Y.; Lim, D.; Kim, S.C.; Ryu, J.H.; Kim, Y.H.; Choi, B.; Kim, S.H. Effect of prehospital epinephrine use on survival from out-of-hospital cardiac arrest and on emergency medical services. J. Clin. Med. 2021, 11, 190. [Google Scholar] [CrossRef] [PubMed]
- Nehme, Z.; Ball, J.; Stephenson, M.; Walker, T.; Stub, D.; Smith, K. Effect of a resuscitation quality improvement programme on outcomes from out-of-hospital cardiac arrest. Resuscitation 2021, 162, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Fang, P.H.; Lin, Y.Y.; Lu, C.H.; Lee, C.C.; Lin, C.H. Impacts of emergency medical technician configurations on outcomes of patients with out-of-hospital cardiac arrest. Int. J. Environ. Res. Public Health 2020, 17, 1930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warren, S.A.; Prince, D.K.; Huszti, E.; Rea, T.D.; Fitzpatrick, A.L.; Andrusiek, D.L.; Darling, S.; Morrison, L.J.; Vilke, G.M.; Nichol, G. Volume versus outcome: More emergency medical services personnel on-scene and increased survival after out-of-hospital cardiac arrest. Resuscitation 2015, 94, 40–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.H.; Lee, S.Y.; Park, J.H.; Song, K.J.; Shin, S.D. Effects of a designated ambulance team response on prehospital return of spontaneous circulation and advanced cardiac life support of out-of-hospital cardiac arrest: A nationwide natural experimental study. Prehosp. Emerg. Care 2022, 26, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Bray, J.; Nehme, Z.; Nguyen, A.; Lockey, A.; Finn, J. A systematic review of the impact of emergency medical service practitioner experience and exposure to out of hospital cardiac arrest on patient outcomes. Resuscitation 2020, 155, 134–142. [Google Scholar] [CrossRef]
- Kim, K.H.; Ro, Y.S.; Park, J.H.; Kim, T.H.; Jeong, J.; Hong, K.J.; Song, K.J.; Shin, S.D. Association between case volume of ambulance stations and clinical outcomes of out-of-hospital cardiac arrest: A nationwide multilevel analysis. Resuscitation 2021, 163, 71–77. [Google Scholar] [CrossRef]
- Wilson, M.H.; Habig, K.; Wright, C.; Hughes, A.; Davies, G.; Imray, C.H. Pre-hospital emergency medicine. Lancet 2015, 386, 2526–2534. [Google Scholar] [CrossRef]
- Shao, F.; Li, H.; Ma, S.; Li, D.; Li, C. Outcomes of out-of-hospital cardiac arrest in beijing: A 5-year cross-sectional study. BMJ Open 2021, 11, e041917. [Google Scholar] [CrossRef]
- Zhang, L.; Luo, M.; Myklebust, H.; Pan, C.; Wang, L.; Zhou, Z.; Yang, Q.; Lin, Q.; Zheng, Z.J. When dispatcher assistance is not saving lives: Assessment of process compliance, barriers and outcomes in out-of-hospital cardiac arrest in a metropolitan city in china. Emerg. Med. J. 2021, 38, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Stroop, R.; Kerner, T.; Strickmann, B.; Hensel, M. Mobile phone-based alerting of cpr-trained volunteers simultaneously with the ambulance can reduce the resuscitation-free interval and improve outcome after out-of-hospital cardiac arrest: A german, population-based cohort study. Resuscitation 2020, 147, 57–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasegawa, M.; Abe, T.; Nagata, T.; Onozuka, D.; Hagihara, A. The number of prehospital defibrillation shocks and 1-month survival in patients with out-of-hospital cardiac arrest. Scand. J. Trauma Resusc. Emerg. Med. 2015, 23, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okubo, M.; Komukai, S.; Callaway, C.W.; Izawa, J. Association of timing of epinephrine administration with outcomes in adults with out-of-hospital cardiac arrest. JAMA Network Open 2021, 4, e2120176. [Google Scholar] [CrossRef]
- Bürger, A.; Wnent, J.; Bohn, A.; Jantzen, T.; Brenner, S.; Lefering, R.; Seewald, S.; Gräsner, J.T.; Fischer, M. The effect of ambulance response time on survival following out-of-hospital cardiac arrest. Dtsch. Arztebl. Int. 2018, 115, 541–548. [Google Scholar] [CrossRef]
- Beck, B.; Bray, J.E.; Smith, K.; Walker, T.; Grantham, H.; Hein, C.; Thorrowgood, M.; Smith, A.; Inoue, M.; Smith, T.; et al. Description of the ambulance services participating in the aus-roc australian and new zealand out-of-hospital cardiac arrest epistry. Emerg. Med. Australas 2016, 28, 673–683. [Google Scholar] [CrossRef]
- Lee, S.G.W.; Hong, K.J.; Kim, T.H.; Choi, S.; Shin, S.D.; Song, K.J.; Ro, Y.S.; Jeong, J.; Park, Y.J.; Park, J.H. Quality of chest compressions during prehospital resuscitation phase from scene arrival to ambulance transport in out-of-hospital cardiac arrest. Resuscitation 2022, 180, 1–7. [Google Scholar] [CrossRef]
- Izawa, J.; Iwami, T.; Gibo, K.; Okubo, M.; Kajino, K.; Kiyohara, K.; Nishiyama, C.; Nishiuchi, T.; Hayashi, Y.; Kiguchi, T.; et al. Timing of advanced airway management by emergency medical services personnel following out-of-hospital cardiac arrest: A population-based cohort study. Resuscitation 2018, 128, 16–23. [Google Scholar] [CrossRef]
- Hosomi, S.; Kitamura, T.; Sobue, T.; Zha, L.; Kiyohara, K.; Matsuyama, T.; Oda, J. Association between timing of epinephrine administration and outcomes of traumatic out-of-hospital cardiac arrest following traffic collisions. J. Clin. Med. 2022, 11, 3564. [Google Scholar] [CrossRef]
- Shibahashi, K.; Kato, T.; Hikone, M.; Sugiyama, K. Fifteen-year secular changes in the care and outcomes of patients with out-of-hospital cardiac arrest in japan: A nationwide, population-based study. Eur. Heart J. Qual. Care Clin. Outcomes 2022. ahead of print. [Google Scholar] [CrossRef]
- Weisfeldt, M.L.; Becker, L.B. Resuscitation after cardiac arrest: A 3-phase time-sensitive model. JAMA 2002, 288, 3035–3038. [Google Scholar] [CrossRef] [PubMed]
- Del Rios, M.; Weber, J.; Pugach, O.; Nguyen, H.; Campbell, T.; Islam, S.; Spencer, L.S.; Markul, E.; Bunney, E.B.; Vanden Hoek, T. Large urban center improves out-of-hospital cardiac arrest survival. Resuscitation 2019, 139, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Scapigliati, A.; Zace, D.; Matsuyama, T.; Pisapia, L.; Saviani, M.; Semeraro, F.; Ristagno, G.; Laurenti, P.; Bray, J.E.; Greif, R.; et al. Community initiatives to promote basic life support implementation-a scoping review. J. Clin. Med. 2021, 10, 5719. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total Cases (N = 1465) | Propensity Score-Matched Cases a (N = 1206) | ||||||
|---|---|---|---|---|---|---|---|
| Pre-Period (N = 610) | Post-Period (N = 855) | p | Pre-Period (N = 591) | Post-Period (N = 591) | p | SMD | |
| Gender = female, n (%) | 154 (25.2) | 221 (25.8) | 0.81 | 150 (25.4) | 148 (25.0) | 0.95 | 0.008 |
| Age, mean (SD) | 60.88 (17.85) | 62.31 (16.65) | 0.12 | 60.83 (17.88) | 60.72 (16.84) | 0.91 | 0.006 |
| Location = home, n (%) | 372 (61.0) | 530 (62.0) | 0.70 | 360 (60.9) | 358 (60.6) | 0.95 | 0.007 |
| Onset on weekend, n (%) | 190 (31.1) | 243 (28.4) | 0.27 | 183 (31.0) | 178 (30.1) | 0.80 | 0.018 |
| Call time of day, n (%) | 0.91 | 0.95 | 0.034 | ||||
| 0:00–5:59 | 84 (13.8) | 114 (13.3) | 82 (13.9) | 78 (13.2) | |||
| 6:00–11:59 | 198 (32.5) | 266 (31.1) | 189 (32.0) | 191 (32.3) | |||
| 12:00–17:59 | 176 (28.9) | 260 (30.4) | 174 (29.4) | 181 (30.6) | |||
| 18:00–23:59 | 152 (24.9) | 215 (25.1) | 146 (24.7) | 141 (23.9) | |||
| CVD history, n (%) | 190 (31.1) | 302 (35.3) | 0.10 | 188 (31.8) | 181 (30.6) | 0.71 | 0.026 |
| Presumed cardiac etiology, n (%) | 444 (72.8) | 655 (76.6) | 0.10 | 435 (73.6) | 432 (73.1) | 0.89 | 0.011 |
| Onset-to-call time, min, Median (IQR) | 15.0 (10.0, 20.0) | 15.0 (10.0, 20.0) | 0.35 | 15.0 (10.0, 20.0) | 15.00 (10.0, 20.0) | 0.26 | 0.046 |
| Response interval, min, Median (IQR) | 11.8 (9.1, 15.5) | 11.4 (8.6, 15.2) | 0.07 | 11.8 (9.0, 15.5) | 12.0 (8.8, 15.9) | 0.88 | 0.004 |
| Scene interval, min, Median (IQR) | 5.2 (2.6, 8.5) | 5.6 (3.0, 9.2) | 0.033 | 5.2 (2.7, 8.5) | 5.1 (2.8, 8.3) | 0.84 | 0.038 |
| Transport interval, min, Median (IQR) | 7.1 (4.4, 10.3) | 8.8 (5.3, 14.2) | <0.001 | 7.0 (4.4, 10.3) | 7.6 (4.6, 11.9) | 0.23 | 0.069 |
| Prehospital interval, min, Median (IQR) | 25.7 (20.8, 33.4) | 28.7 (22.0, 36.2) | <0.001 | 25.7 (20.8, 33.3) | 27.4 (20.9, 34.7) | 0.13 | 0.031 |
| Ambulance crew type, n (%) | 0.033 | 1 | 0.004 | ||||
| Fixed | 187 (30.7) | 218 (25.5) | 186 (31.5) | 185 (31.3) | |||
| Non-fixed | 423 (69.3) | 637 (74.5) | 405 (68.5) | 406 (68.7) | |||
| Treatment-EMS defibrillation, n (%) | 34 (5.6) | 42 (4.9) | 0.63 | 34 (5.8) | 18 (3.0) | 0.032 | / |
| Treatment-IV access, n (%) | 139 (22.8) | 580 (67.8) | <0.001 | 138 (23.4) | 403 (68.2) | <0.001 | / |
| Treatment-IV epinephrine use, n (%) | 5 (0.8) | 15 (1.8) | 0.17 | 5 (0.8) | 10 (1.7) | 0.29 | / |
| Treatment-airway, n (%) | 296 (48.5) | 492 (57.5) | 0.001 | 291 (49.2) | 337 (57.0) | 0.009 | / |
| ROSC at handover at hospital, n (%) | 32 (5.2) | 77 (9.0) | 0.008 | 32 (5.4) | 53 (9.0) | 0.024 | / |
| Pre-Period (N = 610) | Post-Period (N = 855) | |||||
|---|---|---|---|---|---|---|
| Fixed Crew (N = 187) | Non-Fixed Crew (N = 423) | p | Fixed Crew (N = 218) | Non-Fixed Crew (N = 637) | p | |
| Gender = female, n (%) | 47 (25.1) | 107 (25.3) | 1.0 | 53 (24.3) | 168 (26.4) | 0.59 |
| Age, mean (SD) | 61.19 (18.04) | 60.74 (17.79) | 0.78 | 64.18 (16.13) | 61.67 (16.79) | 0.06 |
| Location = home, n (%) | 114 (61.0) | 258 (61.0) | 1.0 | 136 (62.4) | 394 (61.9) | 0.94 |
| Onset on weekend, n (%) | 63 (33.7) | 127 (30.0) | 0.39 | 67 (30.7) | 176 (27.6) | 0.39 |
| Call time of day, n (%) | 0.45 | 0.66 | ||||
| 0:00–5:59 | 23 (12.3) | 61 (14.4) | 26 (11.9) | 88 (13.8) | ||
| 6:00–11:59 | 69 (36.9) | 129 (30.5) | 71 (32.6) | 195 (30.6) | ||
| 12:00–17:59 | 49 (26.2) | 127 (30.0) | 71 (32.6) | 189 (29.7) | ||
| 18:00–23:59 | 46 (24.6) | 106 (25.1) | 50 (22.9) | 165 (25.9) | ||
| CVD history, n (%) | 57 (30.5) | 133 (31.4) | 0.85 | 79 (36.2) | 223 (35.0) | 0.74 |
| Presumed cardiac etiology, n (%) | 144 (77.0) | 300 (70.9) | 0.14 | 179 (82.1) | 476 (74.7) | 0.026 |
| Onset-to-call time, min, Median (IQR) | 20.00 (10.00, 20.00) | 15.00 (10.00, 20.00) | 0.018 | 20.00 (10.00, 20.00) | 15.00 (10.00, 20.00) | 0.034 |
| Response interval, min, Median (IQR) | 11.03 (8.63, 13.96) | 12.45 (9.50, 16.21) | <0.001 | 11.80 (9.07, 15.21) | 11.28 (8.47, 15.18) | 0.49 |
| Scene interval, min, Median (IQR) | 5.27 (2.69, 7.74) | 5.08 (2.48, 8.79) | 0.93 | 4.94 (2.78, 7.82) | 5.82 (3.03, 9.60) | 0.024 |
| Transport interval, min, Median (IQR) | 7.60 (5.03, 10.38) | 6.73 (4.28, 10.25) | 0.049 | 9.47 (6.13, 13.37) | 8.58 (4.98, 14.72) | 0.27 |
| Prehospital interval, min, Median (IQR) | 24.80 (21.15, 32.27) | 26.18 (20.74, 34.51) | 0.25 | 28.55 (21.97, 35.14) | 28.76 (22.06, 36.96) | 0.33 |
| Treatment-EMS defibrillation, n (%) | 14 (7.5) | 20 (4.7) | 0.13 | 8 (3.7) | 34 (5.3) | 0.37 |
| Treatment-IV access, n (%) | 90 (48.1) | 49 (11.6) | <0.001 | 189 (86.7) | 391 (61.4) | <0.001 |
| Treatment-epinephrine use, n (%) | 2 (1.1) | 3 (0.7) | 0.65 | 7 (3.2) | 8 (1.3) | 0.07 |
| Treatment-airway, n (%) | 122 (65.2) | 174 (41.1) | <0.001 | 149 (68.3) | 343 (53.8) | <0.001 |
| ROSC at handover at hospital, n (%) | 14 (7.5) | 18 (4.3) | 0.12 | 17 (7.8) | 60 (9.4) | 0.58 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dong, X.; Wang, L.; Xu, H.; Ye, Y.; Zhou, Z.; Zhang, L. Effect of a Targeted Ambulance Treatment Quality Improvement Programme on Outcomes from Out-of-Hospital Cardiac Arrest: A Metropolitan Citywide Intervention Study. J. Clin. Med. 2023, 12, 163. https://doi.org/10.3390/jcm12010163
Dong X, Wang L, Xu H, Ye Y, Zhou Z, Zhang L. Effect of a Targeted Ambulance Treatment Quality Improvement Programme on Outcomes from Out-of-Hospital Cardiac Arrest: A Metropolitan Citywide Intervention Study. Journal of Clinical Medicine. 2023; 12(1):163. https://doi.org/10.3390/jcm12010163
Chicago/Turabian StyleDong, Xuejie, Liang Wang, Hanbing Xu, Yingfang Ye, Zhenxiang Zhou, and Lin Zhang. 2023. "Effect of a Targeted Ambulance Treatment Quality Improvement Programme on Outcomes from Out-of-Hospital Cardiac Arrest: A Metropolitan Citywide Intervention Study" Journal of Clinical Medicine 12, no. 1: 163. https://doi.org/10.3390/jcm12010163