
Advanced and Invasive Cardiopulmonary Resuscitation (CPR) Techniques as an Adjunct to Advanced Cardiac Life Support


Abstract
:1. Introduction
2. Methods
3. Results and Discussion of Advanced and Invasive Techniques
3.1. Real-Time Audio or Audiovisual CPR Feedback Devices
3.2. Automated Mechanical CPR (mCPR)
3.2.1. Rationale
3.2.2. Significance of the Time Aspect

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Trial Abbreviation and Quotation | Design and Inclusion Criteria | Main Findings and Limitations |
|---|---|---|
| (a) RCTs on automated mCPR vs. conventional manual chest compression | ||
| ASPIRE [33] | mCPR (AutoPulse®) vs. conventional manual CPR; prospective cluster RCT, multi-center (Canada, USA); out-of-hospital; 2004–2005; 394 vs. 373 cases out of 1377 Inclusion criteria: age ≥ 18 and non-TCA | Stopped by DSMB, ±survival (after 4 h), ↓ discharge, ↓ CPC Limitations: design (allocation concealment and not powered for secondary analyses), selection bias (trial vehicles), performance bias (device implementation, noncompliance, quality monitoring), training effect, and COI (funding by manufacturer) |
| CIRC [34] | mCPR (AutoPulse®) vs. conventional manual CPR; prospective individually RCT, multi-center (USA, Austria, Netherlands); out-of-hospital; 2009–2011; 2099 vs. 2132 cases out of 4753 Inclusion criteria: age ≥ 18, presumed cardiac origin (non-TCA), and response time ≤ 16 min | ↓ “sustained” ROSC, ↓ survival (after 24 h), ±discharge, ±CPC Limitations: selection bias (response time), performance bias (guideline revision, quality monitoring), reporting bias (post-randomization exclusions), training effect, and COI (co-author is an employee of the manufacturer) |
| LINC [35] | mCPR (LUCAS®) with simultaneous defibrillation vs. conventional manual CPR with sequential defibrillation; prospective individually RCT, multi-center (Sweden, UK, Netherlands); out-of-hospital; 2008–2013; 1300 vs. 1289 cases out of 4998 Inclusion criteria: age ≥ 18, non-TCA, and no defibrillation before the device arrived on scene | ±ROSC, ±admission, ± survival (after 4 h and 1 and 6 months), ±discharge, ±CPC Limitations: performance bias (defibrillation simultaneous vs. sequential, guideline revision, quality monitoring, noncompliance), training effect, and COI (device developed by investigating university) |
| PARAMEDIC [36] | mCPR (LUCAS®) vs. conventional manual CPR; prospective cluster RCT, multi-center (UK); out-of-hospital; 2010–2013; 1652 vs. 2818 cases out of 4689 Inclusion criteria: trial vehicle first on the scene, age ≥ 18, and non-TCA | ±ROSC, ±admission, ±survival (after 1, 3 & 12 months), ↓ CPC Limitations: design (allocation concealment and the sample size was increased), selection bias (trial vehicles), performance bias (guideline revision, quality monitoring), and training effect |
| MECCA [37] | mCPR (LUCAS®) vs. conventional manual CPR; prospective cluster RCT, multi-center (Singapore); out-of-hospital; 2011–2012; 302 vs. 889 cases out of 1274 Inclusion criteria: age ≥ 21, presumed cardiac entity (non-TCA), and attended to by ambulance crew | ±ROSC, ±survival (after 24 h and 30 days), ±discharge; as-treated analysis: any outcome ↑ if mCPR device attached early Limitations: design (not powered for secondary analyses and allocation concealment), performance bias (quality monitoring and noncompliance), training effect, and COI not reported |
| (b) Non-RCTs on automated mCPR vs. conventional manual chest compression | ||
| German Resuscitation Registry [38,40] | mCPR (LUCAS®, AutoPulse®) vs. conventional manual CPR; retrospective registry analysis, multi-center (Germany); out-of-hospital; 2007–2014; 912 vs. 18,697 cases out of 35,593 Inclusion criteria: cases documented in the registry, age ≥ 18, and non-TCA | ↑ (AutoPulse®) or ± (LUCAS®) ROSC (if CPR duration considered, ±(AutoPulse®) or ↓ (LUCAS®) with general application) Limitations: design (retrospective), selection bias (voluntary participation in the registry), performance bias (registry data, quality of documentation, and voluntary), and loss of follow-up |
| LDB device for OHCA resuscitation [43] | mCPR (AutoPulse®) vs. conventional manual CPR; prospective phased longitudinal observational cohort study, single-center (USA); out-of-hospital; 2001–2005; 284 vs. 499 cases out of 2294 Inclusion criteria: age ≥ 18 and non-TCA | ↑ ROSC, ↑ admission, ↑ discharge, ±CPC, few survivors if response time > 8 min Limitations: design (observational), performance bias (hypothermia and device implementation), training effect, and COI (funding by manufacturer, co-author is an advisor for the manufacturer) |
3.2.3. Decision Criteria
3.2.4. Therapeutic Strategy
3.3. Extra-Corporeal Cardiopulmonary Resuscitation (eCPR)
3.3.1. Rationale
| Trial Abbreviation and Quotation | Design and Inclusion Criteria | Main Findings and Limitations |
|---|---|---|
| (a) RCTs on eCPR vs. conventional manual chest compression or automated mCPR | ||
| ARREST [70] | eCPR vs. conventional manual CPR or automated mCPR in patients with VF; prospective individualized RCT, single-center (USA); emergency department; 2019–2020; 15 vs. 15 patients out of 36 inclusion criteria: age 18–75, initially documented OHCA rhythm VF or pulseless ventricular tachycardia, no ROSC following three defibrillations, body morphology allows mCPR, and estimated transfer time < 30 min | Stopped by DSMB, superiority exceeded prespecified monitoring boundary; ↑ discharge, ↑ survival (after 3 and 6 months), ±CPC Limitations: design (single-center), performance bias (high eCPR expertise), low number of participants since stopped early, and training effect |
| (b) RCTs on a combined hyperinvasive approach vs. conventional manual chest compression | ||
| Prague OHCA study [7] | mCPR (LUCAS®), early intra-arrest transport, eCPR, invasive assessment and treatment vs. conventional manual CPR; prospective individually RCT, single-center (Czech Republic); out-of-hospital; 2013–2020; 124 vs. 132 cases out of 256 Inclusion criteria: age 18–65, witnessed collapse, presumed cardiac cause, ≥ 5 min ALS without sustained ROSC, unconsciousness (Glasgow Coma Score < 8), eCPR team, and ICU bed capacity available | Stopped by DSMB, possibly underpowered; ± “sustained” ROSC, ± “neurologic recovery” [survival with CPC 1–2] (↑ after 30 days, ± after 180 days), ± “cardiac recovery” Limitations: design (single-center, limited enrollment, power, and crossover), performance bias (high eCPR expertise and noncompliance), selection bias (high bystander CPR rates), and training effect |
| (c) retrospective cohort studies on mechanical circulatory support vs. mCPR | ||
| Survival and neurological outcome after OHCA treated with and without mechanical circulatory support [74] | eCPR (with or without Impella) vs. mCPR; retrospective cohort study, single-center (Denmark); emergency department; 2015–2019; 101 vs. 216 cases out of 1015 Inclusion criteria: age ≥ 18 and transport to the hospital with refractory OHCA | ↑ ICU admission, ↑ discharge, ↑ survival (after 30 days and 1 year), ↑ CPC Design (retrospective), selection bias (voluntary participation in the registry), performance bias (registry data, quality of documentation, and voluntarily), and loss of follow-up |
3.3.2. Decision Criteria
3.3.3. Cannulation
3.3.4. Therapeutic Strategy
3.4. Sonography
3.4.1. Optimisation of Chest Compressions
3.4.2. Detecting and Addressing Reversible Causes of Cardiac Arrest
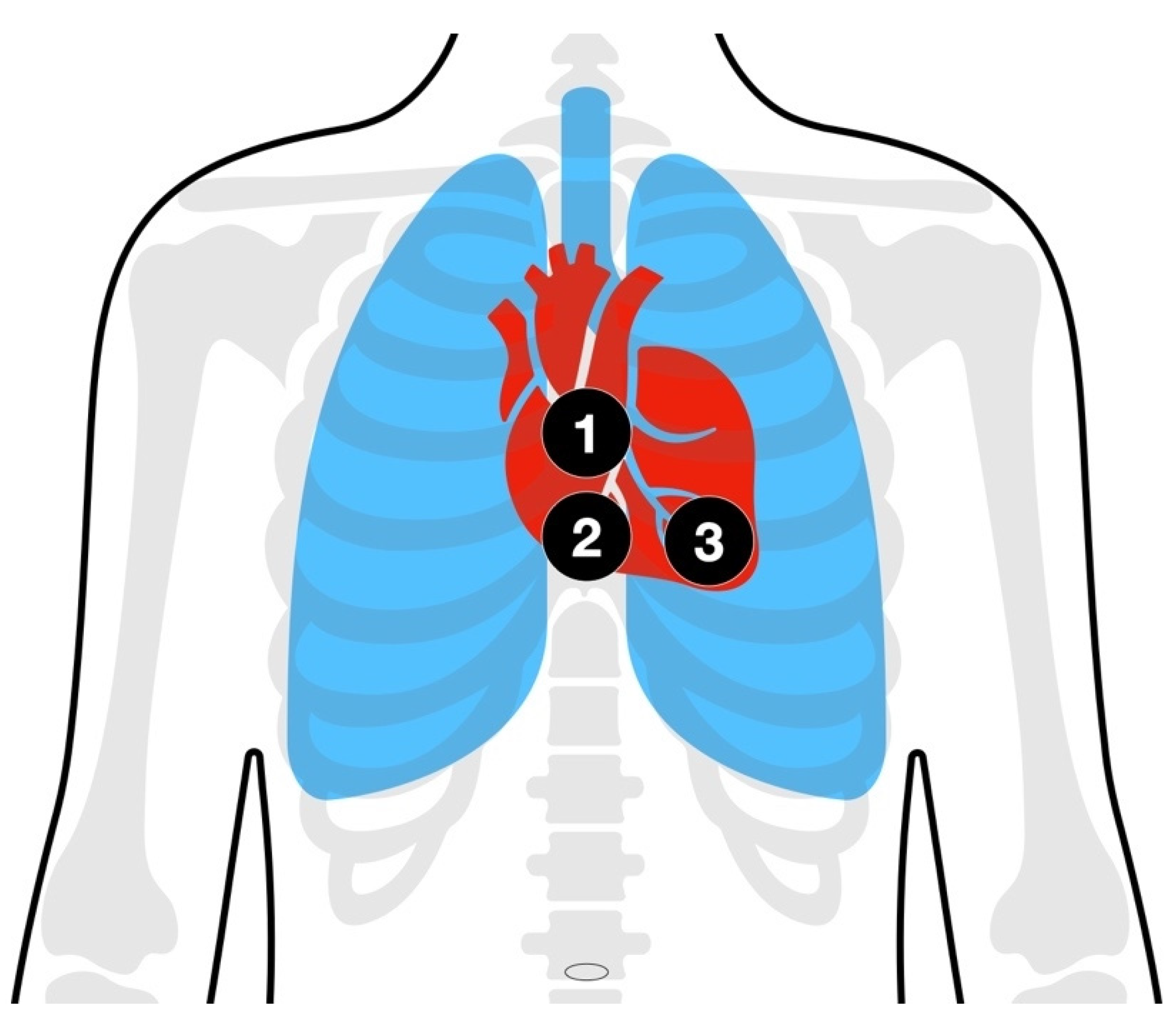
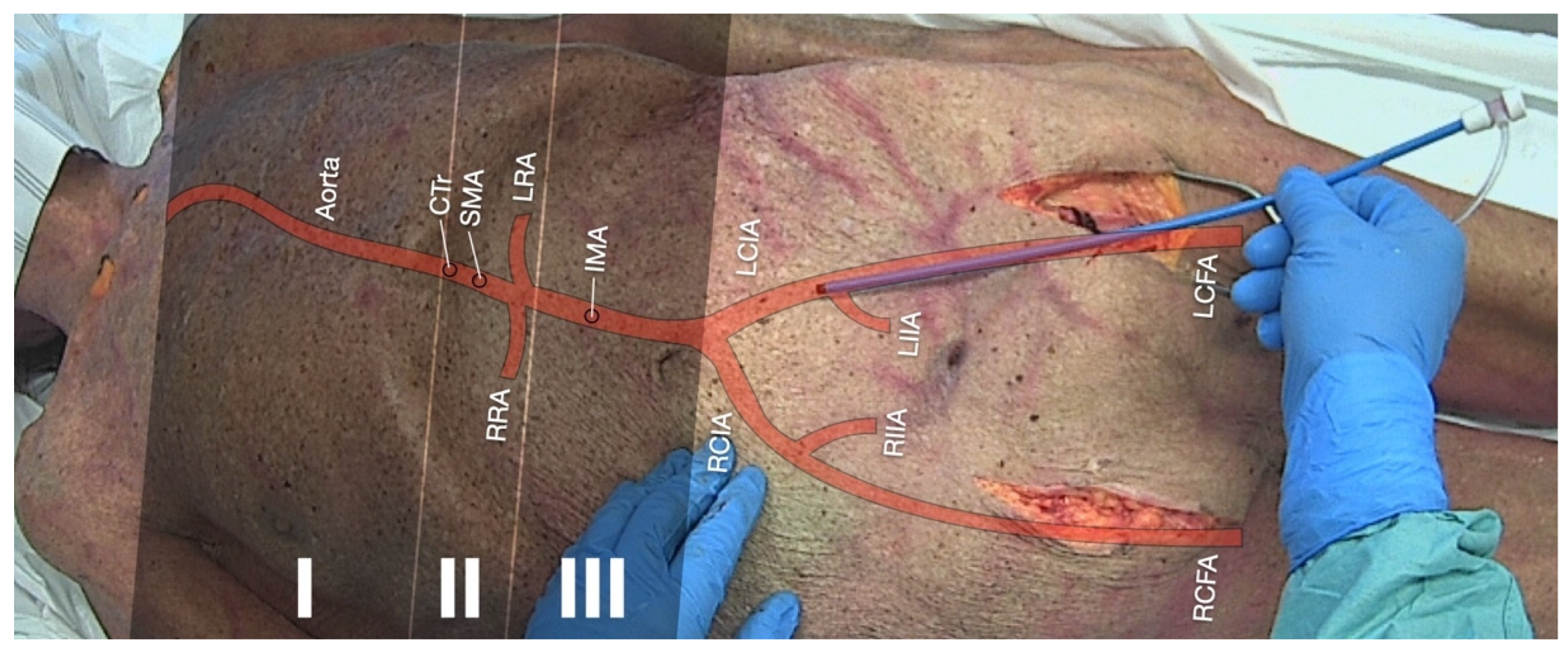
3.5. Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA)
- (1)
- The ascendant aorta with the aortic arch is occasionally referred to as “Zone 0”. Due to the branches of the carotid arteries supplying the brain with blood, balloon deployment is contraindicated in this zone.
- (2)
- Zone I: The left subclavian artery to the celiac trunk. This position is preferred in non-traumatic cardiac arrest to enhance coronary and cerebral perfusion. Among other scopes of application, there may be aortic dissection or uncontrollable thoracic or visceral bleeding.
- (3)
- Zone II: The coeliac trunk to the lowest renal artery supplying major intra- and retroperitoneal organs with blood. Balloon deployment is contraindicated in this zone.
- (4)
- Zone III: The lowest renal artery to the aortic bifurcation. This position is preferred in uncontrollable sub-/pelvic or groin bleeding.
3.5.1. Achieving Hemostasis in Severe Trauma and Traumatic Cardiac Arrest (TCA)
3.5.2. Improving Coronary Perfusion during CPR
3.6. Arterial Blood Gas (ABG) Analysis
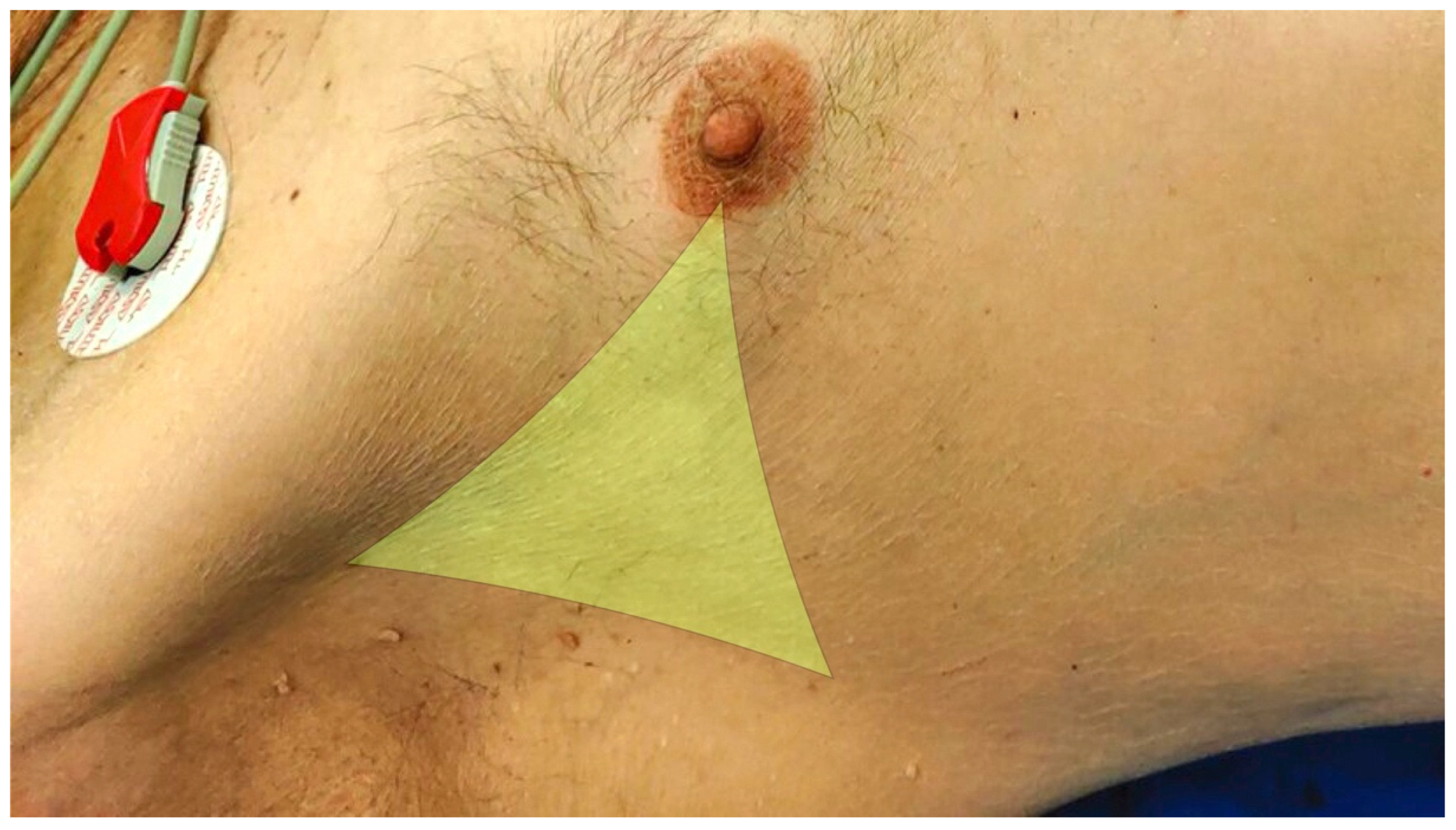
3.7. Thoracic Decompression
3.8. Pericardiocentesis
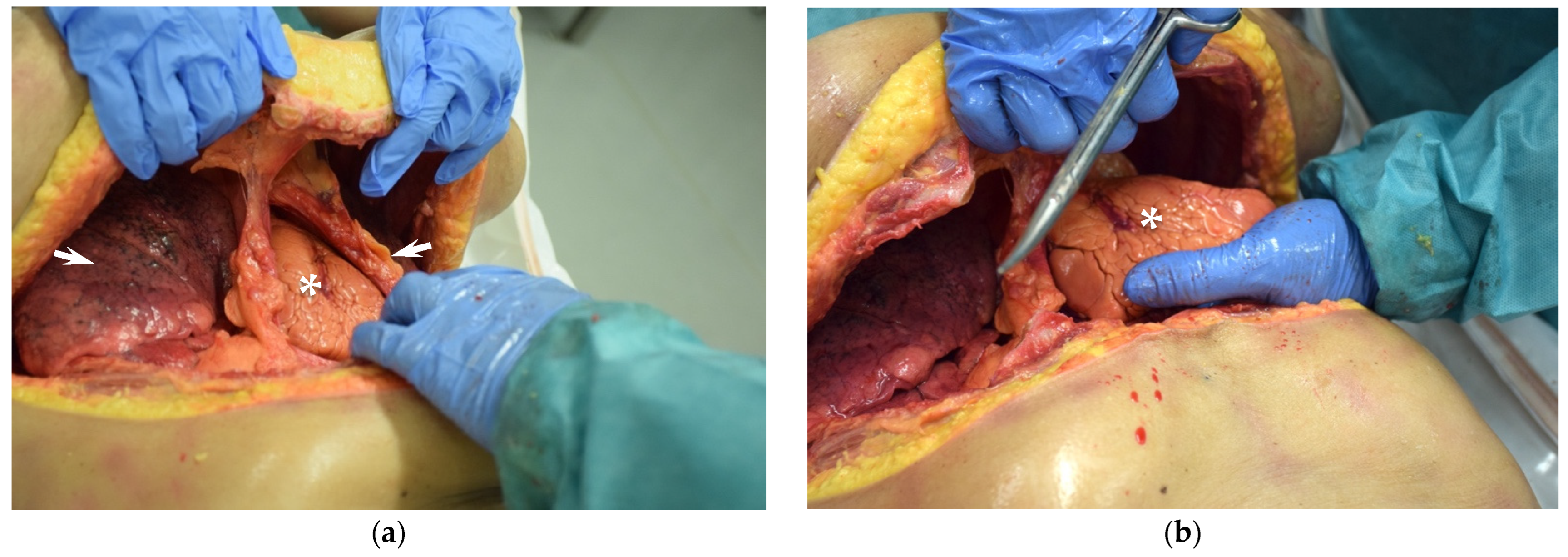
3.9. Resuscitative Thoracotomy
4. Discussion of Concepts and Strategies
4.1. Decision-Making and Timing
4.2. Emergency Response and Continuing Care Structures
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ABG | arterial blood gas |
| ALS | advanced life support |
| AMC | area of maximal compression |
| CAC | cardiac arrest center |
| CI | confidence interval |
| COI | conflict of interest |
| CPC | Glasgow–Pittsburgh cerebral performance category |
| CPR | cardiopulmonary resuscitation |
| CT | computed tomography |
| CTr | coeliac trunk |
| DSMB | data and safety monitoring board |
| DVT | deep vein thrombosis |
| ECLS | extracorporeal life support |
| ECMO | extracorporeal membrane oxygenation |
| eCPR | extracorporeal cardiopulmonary resuscitation (CPR) |
| eFAST | extended focused assessment with sonography for trauma |
| EMS | emergency medical service |
| etCO2 | end-tidal carbon dioxide partial pressure |
| FDA | US Food and Drug Administration |
| FEEL | focused echocardiographic evaluation in life support |
| ICU | intensive care unit |
| IHCA | in-hospital cardiac arrest |
| IMA | inferior mesenteric artery |
| IVC | inferior vena cava |
| LCFA | left common femoral artery |
| LCIA | left common iliac artery |
| LIIA | left internal iliac artery |
| LRA | left renal artery |
| LV | left ventricle |
| LVOT | left ventricular outflow tract |
| mCPR | (automated) mechanical cardiopulmonary resuscitation (CPR) |
| ME Bicaval | midoesophageal bicaval view |
| ME4CH | midoesophageal 4-chamber view |
| MELAX | midoesophageal long axis view |
| MIC | medical intervention car, a physician-staffed rapid response vehicle |
| mRS | modified Rankin Scale |
| OHCA | out-of-hospital cardiac arrest |
| OR | odds ratio |
| PCI | percutaneous coronary intervention |
| PE | pulmonary embolism |
| PEA | pulseless electrical activity |
| PLAX | parasternal long-axis view |
| POCT | point-of-care testing |
| POCUS | point-of-care ultrasound |
| RACA | return of spontaneous circulation (ROSC) after cardiac arrest |
| RCFA | right common femoral artery |
| RCIA | right common iliac artery |
| RCT | randomized controlled trial |
| REBOA | resuscitative endovascular balloon occlusion of the aorta |
| RIIA | right internal iliac artery |
| ROSC | return of spontaneous circulation |
| RRA | right renal artery |
| RV | right ventricle |
| S4CH | subcostal window 4-chamber view |
| SMA | superior mesenteric artery |
| SOP | standard operating procedure |
| TAVI | transcatheter aortic valve implantation |
| TCA | traumatic cardiac arrest |
| TGSAX | transgastric short axis view |
| TOE | trans-oesophageal echocardiography |
| TTE | trans-thoracic echocardiography |
| VF | ventricular fibrillation |
References
- Kouwenhoven, W.B.; Jude, J.R.; Knickerbocker, G.G. Closed-chest cardiac massage. JAMA 1960, 173, 1064–1067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Safar, P. Artificial Respitation. Anesthesiology 1960, 21, 570. [Google Scholar] [CrossRef]
- Gräsner, J.-T.; Herlitz, J.; Tjelmeland, I.B.M.; Wnent, J.; Masterson, S.; Lilja, G.; Bein, B.; Böttiger, B.W.; Rosell-Ortiz, F.; Nolan, J.P.; et al. European Resuscitation Council Guidelines 2021: Epidemiology of cardiac arrest in Europe. Resuscitation 2021, 161, 61–79. [Google Scholar] [CrossRef]
- Chamberlain, D. Never Quite There: A tale of Resuscitation Medicine. Resuscitation 2004, 60, 3–11. [Google Scholar] [CrossRef]
- Soar, J.; Bottiger, B.W.; Carli, P.; Couper, K.; Deakin, C.D.; Djarv, T.; Lott, C.; Olasveengen, T.; Paal, P.; Pellis, T.; et al. European Resuscitation Council Guidelines 2021: Adult advanced life support. Resuscitation 2021, 161, 115–151. [Google Scholar] [CrossRef]
- Rott, N.; Bottiger, B.W.; Lockey, A. The World Restart a Heart Initiative: How to save hundreds of thousands of lives worldwide. Curr. Opin. Crit. Care 2021, 27, 663–667. [Google Scholar] [CrossRef]
- Bělohlávek, J.; Smalcova, J.; Rob, D.; Franek, O.; Smid, O.; Pokorna, M.; Horak, J.; Mrazek, V.; Kovarnik, T.; Zemanek, D.; et al. Effect of Intra-arrest Transport, Extracorporeal Cardiopulmonary Resuscitation, and Immediate Invasive Assessment and Treatment on Functional Neurologic Outcome in Refractory Out-of-Hospital Cardiac Arrest: A Randomized Clinical Trial. JAMA 2022, 327, 737–747. [Google Scholar] [CrossRef]
- Bouhemad, B.; Brisson, H.; Le-Guen, M.; Arbelot, C.; Lu, Q.; Rouby, J.J. Bedside ultrasound assessment of positive end-expiratory pressure-induced lung recruitment. Am. J. Respir. Crit. Care Med. 2011, 183, 341–347. [Google Scholar] [CrossRef] [Green Version]
- O'Brien, C.E.; Santos, P.T.; Reyes, M.; Adams, S.; Hopkins, C.D.; Kulikowicz, E.; Hamrick, J.L.; Hamrick, J.T.; Lee, J.K.; Kudchadkar, S.R.; et al. Association of diastolic blood pressure with survival during paediatric cardiopulmonary resuscitation. Resuscitation 2019, 143, 50–56. [Google Scholar] [CrossRef]
- Brede, J.R. Aortic occlusion during cardiac arrest-mechanical adrenaline? Resuscitation 2022, 179, 94–96. [Google Scholar] [CrossRef]
- Olasveengen, T.M.; Semeraro, F.; Ristagno, G.; Castren, M.; Handley, A.; Kuzovlev, A.; Monsieurs, K.G.; Raffay, V.; Smyth, M.; Soar, J.; et al. European Resuscitation Council Guidelines 2021: Basic Life Support. Resuscitation 2021, 161, 98–114. [Google Scholar] [CrossRef] [PubMed]
- Nichol, G.; Thomas, E.; Callaway, C.W.; Hedges, J.; Powell, J.L.; Aufderheide, T.P.; Rea, T.; Lowe, R.; Brown, T.; Dreyer, J.; et al. Regional variation in out-of-hospital cardiac arrest incidence and outcome. JAMA 2008, 300, 1423–1431. [Google Scholar] [CrossRef] [Green Version]
- Valenzuela, T.D.; Kern, K.B.; Clark, L.L.; Berg, R.A.; Berg, M.D.; Berg, D.D.; Hilwig, R.W.; Otto, C.W.; Newburn, D.; Ewy, G.A. Interruptions of chest compressions during emergency medical systems resuscitation. Circulation 2005, 112, 1259–1265. [Google Scholar] [CrossRef] [PubMed]
- Ochoa, F.J.; Ramalle-Gomara, E.; Lisa, V.; Saralegui, I. The effect of rescuer fatigue on the quality of chest compressions. Resuscitation 1998, 37, 149–152. [Google Scholar] [CrossRef]
- Eftestol, T.; Sunde, K.; Steen, P.A. Effects of interrupting precordial compressions on the calculated probability of defibrillation success during out-of-hospital cardiac arrest. Circulation 2002, 105, 2270–2273. [Google Scholar] [CrossRef] [Green Version]
- Christenson, J.; Andrusiek, D.; Everson-Stewart, S.; Kudenchuk, P.; Hostler, D.; Powell, J.; Callaway, C.W.; Bishop, D.; Vaillancourt, C.; Davis, D.; et al. Chest compression fraction determines survival in patients with out-of-hospital ventricular fibrillation. Circulation 2009, 120, 1241–1247. [Google Scholar] [CrossRef] [Green Version]
- Paradis, N.A.; Martin, G.B.; Rivers, E.P.; Goetting, M.G.; Appleton, T.J.; Feingold, M.; Nowak, R.M. Coronary perfusion pressure and the return of spontaneous circulation in human cardiopulmonary resuscitation. JAMA 1990, 263, 1106–1113. [Google Scholar] [CrossRef]
- Rehn, M.; Davies, G.; Smith, P.; Lockey, D.J. Structure of Rapid Response Car Operations in an Urban Trauma Service. Air Med. J. 2016, 35, 143–147. [Google Scholar] [CrossRef]
- Obermaier, M.; Fiedler, M.O.; Göring, M.; Hochreiter, M.; Küßner, T.; Mohr, S.; Popp, E.; Schmitt, F.C.F.; Weigand, M.A.; Weilbacher, F.; et al. Medical Intervention Car: Projekt zur Verbesserung der außerklinischen Notfallversorgung. In Elsevier Emergency: Innovative Konzepte; Gollwitzer, J., Grusnick, H.-M., Klausmeier, M., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 18–24. [Google Scholar]
- Richardson, A.S.C.; Tonna, J.E.; Nanjayya, V.; Nixon, P.; Abrams, D.C.; Raman, L.; Bernard, S.; Finney, S.J.; Grunau, B.; Youngquist, S.T.; et al. Extracorporeal Cardiopulmonary Resuscitation in Adults. Interim Guideline Consensus Statement From the Extracorporeal Life Support Organization. Asaio J. 2021, 67, 221–228. [Google Scholar] [CrossRef]
- Bernhard, M.; Friedmann, C.; Aul, A.; Helm, M.; Mutzbauer, T.S.; Doll, S.; Völkl, A.; Gries, A. Praxisorientiertes Ausbildungskonzept für invasive Notfalltechniken. Notf. Rett. Med. 2010, 14, 475–482. [Google Scholar] [CrossRef]
- Schneider, N.R.E.; Küßner, T.; Weilbacher, F.; Göring, M.; Mohr, S.; Rudolph, M.; Popp, E. Invasive Notfalltechniken – INTECH Advanced. Notf. Rett. Med. 2018, 22, 87–99. [Google Scholar] [CrossRef]
- Trummer, G.; Muller, T.; Muellenbach, R.M.; Markewitz, A.; Pilarczyk, K.; Bittner, S.; Boeken, U.; Benk, C.; Baumgartel, M.; Bauer, A.; et al. Training module extracorporeal life support (ECLS): Consensus statement of the DIVI, DGTHG, DGfK, DGAI, DGIIN, DGF, GRC and DGK. Anaesthesist 2021, 70, 603–606. [Google Scholar] [CrossRef]
- Eismann, H.; Schild, S.; Neuhaus, C.; Baus, J.; Happel, O.; Heller, A.R.; Richter, T.; Weinert, M.; Sedlmayr, B.; Sedlmayr, M.; et al. Cognitive aids for crisis management in anaesthesiology: Principles and applications. Anästhesth. Intensivmed. 2020, 61, 239–247. [Google Scholar] [CrossRef]
- Lukas, R.P.; Gräsner, J.T.; Seewald, S.; Lefering, R.; Weber, T.P.; Van Aken, H.; Fischer, M.; Bohn, A. Chest compression quality management and return of spontaneous circulation: A matched-pair registry study. Resuscitation 2012, 83, 1212–1218. [Google Scholar] [CrossRef]
- Brouwer, T.F.; Walker, R.G.; Chapman, F.W.; Koster, R.W. Association Between Chest Compression Interruptions and Clinical Outcomes of Ventricular Fibrillation Out-of-Hospital Cardiac Arrest. Circulation 2015, 132, 1030–1037. [Google Scholar] [CrossRef] [Green Version]
- Gugelmin-Almeida, D.; Tobase, L.; Polastri, T.F.; Peres, H.H.C.; Timerman, S. Do automated real-time feedback devices improve CPR quality? A systematic review of literature. Resusc. Plus 2021, 6, 100108. [Google Scholar] [CrossRef]
- Wang, S.A.; Su, C.P.; Fan, H.Y.; Hou, W.H.; Chen, Y.C. Effects of real-time feedback on cardiopulmonary resuscitation quality on outcomes in adult patients with cardiac arrest: A systematic review and meta-analysis. Resuscitation 2020, 155, 82–90. [Google Scholar] [CrossRef]
- Goharani, R.; Vahedian-Azimi, A.; Farzanegan, B.; Bashar, F.R.; Hajiesmaeili, M.; Shojaei, S.; Madani, S.J.; Gohari-Moghaddam, K.; Hatamian, S.; Mosavinasab, S.M.M.; et al. Real-time compression feedback for patients with in-hospital cardiac arrest: A multi-center randomized controlled clinical trial. J. Intensive Care 2019, 7, 5. [Google Scholar] [CrossRef] [Green Version]
- Goharani, R.; Vahedian-Azimi, A.; Pourhoseingholi, M.A.; Amanpour, F.; Rosano, G.M.C.; Sahebkar, A. Survival to intensive care unit discharge among in-hospital cardiac arrest patients by applying audiovisual feedback device. ESC Heart Fail. 2021, 8, 4652–4660. [Google Scholar] [CrossRef]
- Hostler, D.; Everson-Stewart, S.; Rea, T.D.; Stiell, I.G.; Callaway, C.W.; Kudenchuk, P.J.; Sears, G.K.; Emerson, S.S.; Nichol, G.; Resuscitation Outcomes Consortium, I. Effect of real-time feedback during cardiopulmonary resuscitation outside hospital: Prospective, cluster-randomised trial. Br. Med. J. 2011, 342, d512. [Google Scholar] [CrossRef]
- Wyckoff, M.H.; Greif, R.; Morley, P.T.; Ng, K.C.; Olasveengen, T.M.; Singletary, E.M.; Soar, J.; Cheng, A.; Drennan, I.R.; Liley, H.G.; et al. 2022 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Resuscitation 2022. [Google Scholar] [CrossRef]
- Hallstrom, A.; Rea, T.D.; Sayre, M.R.; Christenson, J.; Anton, A.R.; Mosesso, V.N., Jr.; Van Ottingham, L.; Olsufka, M.; Pennington, S.; White, L.J.; et al. Manual chest compression vs use of an automated chest compression device during resuscitation following out-of-hospital cardiac arrest: A randomized trial. JAMA 2006, 295, 2620–2628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wik, L.; Olsen, J.A.; Persse, D.; Sterz, F.; Lozano, M., Jr.; Brouwer, M.A.; Westfall, M.; Souders, C.M.; Malzer, R.; van Grunsven, P.M.; et al. Manual vs. integrated automatic load-distributing band CPR with equal survival after out of hospital cardiac arrest. The randomized CIRC trial. Resuscitation 2014, 85, 741–748. [Google Scholar] [CrossRef] [PubMed]
- Rubertsson, S.; Lindgren, E.; Smekal, D.; Ostlund, O.; Silfverstolpe, J.; Lichtveld, R.A.; Boomars, R.; Ahlstedt, B.; Skoog, G.; Kastberg, R.; et al. Mechanical chest compressions and simultaneous defibrillation vs conventional cardiopulmonary resuscitation in out-of-hospital cardiac arrest: The LINC randomized trial. JAMA 2014, 311, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Perkins, G.D.; Lall, R.; Quinn, T.; Deakin, C.D.; Cooke, M.W.; Horton, J.; Lamb, S.E.; Slowther, A.M.; Woollard, M.; Carson, A.; et al. Mechanical versus manual chest compression for out-of-hospital cardiac arrest (PARAMEDIC): A pragmatic, cluster randomised controlled trial. Lancet 2015, 385, 947–955. [Google Scholar] [CrossRef] [Green Version]
- Anantharaman, V.; Ng, B.L.; Ang, S.H.; Lee, C.Y.; Leong, S.H.; Ong, M.E.; Chua, S.J.; Rabind, A.C.; Anjali, N.B.; Hao, Y. Prompt use of mechanical cardiopulmonary resuscitation in out-of-hospital cardiac arrest: The MECCA study report. Singapore Med. J. 2017, 58, 424–431. [Google Scholar] [CrossRef] [Green Version]
- Obermaier, M. Stellenwert von Kardiokompressionssystemen in der außer- und innerklinischen Reanimation: Eine retrospektive Registeranalyse und prospektive Metaanalyse. Ph.D. Thesis, Medizinische Fakultät, Universität Ulm, Open Access Repositorium of Ulm University (OPARU), Ulm, Germany, 2018. [Google Scholar]
- Wang, P.L.; Brooks, S.C. Mechanical versus manual chest compressions for cardiac arrest. Cochrane Database Syst. Rev. 2018, 8, CD007260. [Google Scholar] [CrossRef]
- Seewald, S.; Obermaier, M.; Lefering, R.; Bohn, A.; Georgieff, M.; Muth, C.-M.; Gräsner, J.-T.; Masterson, S.; Scholz, J.; Wnent, J. Application of mechanical cardiopulmonary resuscitation devices and their value in out-of-hospital cardiac arrest: A retrospective analysis of the German Resuscitation Registry. PLoS ONE 2019, 14, e0208113. [Google Scholar] [CrossRef]
- Obermaier, M.; Seewald, S.; Muth, C.-M.; Gräsner, J.-T. Präklinischer Einsatz von Kardiokompressionssystemen und deren Rolle in der präklinischen Reanimation: Eine retrospektive Analyse des Deutschen Reanimationsregisters. Anästhesiologie Intensivmed. 2014, 55, S13–S14. [Google Scholar]
- Wik, L.; Olsen, J.A.; Persse, D.; Sterz, F.; Lozano, M.; Brouwer, M.A.; Westfall, M.; Souders, C.M.; Malzer, R.; van Grunsven, P.M.; et al. Integrated autopulse CPR improves survival from out-of hospital cardiac arrests compared to manual CPR after controlling for EMS response times. Circulation 2013, 128, S1. [Google Scholar]
- Ong, M.E.H.; Ornato, J.P.; Edwards, D.P.; Dhindsa, H.S.; Best, A.M.; Ines, C.S.; Hickey, S.; Clark, B.; Williams, D.C.; Powell, R.G.; et al. Use of an automated, load-distributing band chest compression device for out-of-hospital cardiac arrest resuscitation. JAMA 2006, 295, 2629–2637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obermaier, M.; Zimmermann, J.B.; Popp, E.; Weigand, M.A.; Weiterer, S.; Dinse-Lambracht, A.; Muth, C.-M.; Nußbaum, B.L.; Gräsner, J.-T.; Seewald, S.; et al. Automated mechanical cardiopulmonary resuscitation devices versus manual chest compression in the treatment of cardiac arrest: Protocol of a systematic review and meta-analysis comparing machine to human. BMJ Open 2021, 11, e042062. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.Y.; Lim, K.C.; Lai, P.C.; Tsai, T.Y.; Huang, Y.T.; Tsai, M.J. Comparison between Prehospital Mechanical Cardiopulmonary Resuscitation (CPR) Devices and Manual CPR for Out-of-Hospital Cardiac Arrest: A Systematic Review, Meta-Analysis, and Trial Sequential Analysis. J. Clin. Med. 2022, 11, 1448. [Google Scholar] [CrossRef] [PubMed]
- Obermaier, M.; Schramm, C. LUCAS® leaving its footprints during cardiopulmonary resuscitation. Vis. J. Emerg. Med. 2019, 17, 100666. [Google Scholar] [CrossRef]
- Obermaier, M.; Do, T.D. Hemodynamically Relevant Intrathoracic Bleeding Following CPR: Case Report on Resuscitation-associated Injury to Intercostal Arteries with the Need for Transcatheter Arterial Embolization. Notarzt. 2022. [Google Scholar] [CrossRef]
- Ondruschka, B.; Baier, C.; Bayer, R.; Hammer, N.; Dressler, J.; Bernhard, M. Chest compression-associated injuries in cardiac arrest patients treated with manual chest compressions versus automated chest compression devices (LUCAS II) - a forensic autopsy-based comparison. Forensic Sci. Med. Pathol. 2018, 14, 515–525. [Google Scholar] [CrossRef]
- Ondruschka, B.; Baier, C.; Bernhard, M.; Buschmann, C.; Dressler, J.; Schlote, J.; Zwirner, J.; Hammer, N. Frequency and intensity of pulmonary bone marrow and fat embolism due to manual or automated chest compressions during cardiopulmonary resuscitation. Forensic Sci. Med. Pathol. 2019, 15, 48–55. [Google Scholar] [CrossRef]
- Risom, M.; Jorgensen, H.; Rasmussen, L.S.; Sorensen, A.M. Resuscitation, prolonged cardiac arrest, and an automated chest compression device. J. Emerg. Med. 2010, 38, 481–483. [Google Scholar] [CrossRef]
- Paal, P.; Brugger, H.; Boyd, J. Accidental hypothermia. N. Engl. J. Med. 2013, 368, 682. [Google Scholar] [CrossRef] [Green Version]
- Holmstrom, P.; Boyd, J.; Sorsa, M.; Kuisma, M. A case of hypothermic cardiac arrest treated with an external chest compression device (LUCAS) during transport to re-warming. Resuscitation 2005, 67, 139–141. [Google Scholar] [CrossRef]
- Wik, L.; Kiil, S. Use of an automatic mechanical chest compression device (LUCAS) as a bridge to establishing cardiopulmonary bypass for a patient with hypothermic cardiac arrest. Resuscitation 2005, 66, 391–394. [Google Scholar] [CrossRef] [PubMed]
- Lott, C.; Truhlar, A.; Alfonzo, A.; Barelli, A.; Gonzalez-Salvado, V.; Hinkelbein, J.; Nolan, J.P.; Paal, P.; Perkins, G.D.; Thies, K.C.; et al. European Resuscitation Council Guidelines 2021: Cardiac arrest in special circumstances. Resuscitation 2021, 161, 152–219. [Google Scholar] [CrossRef]
- Gässler, H.; Ventzke, M.M.; Lampl, L.; Helm, M. Transport with ongoing resuscitation: A comparison between manual and mechanical compression. Emerg. Med. J. 2013, 30, 589–592. [Google Scholar] [CrossRef] [PubMed]
- Ventzke, M.M.; Gassler, H.; Lampl, L.; Helm, M. Cardio pump reloaded: In-hospital resuscitation during transport. Intern Emerg. Med. 2013, 8, 621–626. [Google Scholar] [CrossRef]
- Gässler, H.; Kümmerle, S.; Ventzke, M.M.; Lampl, L.; Helm, M. Mechanical chest compression: An alternative in helicopter emergency medical services? Intern Emerg. Med. 2015, 10, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Bonnemeier, H.; Simonis, G.; Olivecrona, G.; Weidtmann, B.; Gotberg, M.; Weitz, G.; Gerling, I.; Strasser, R.; Frey, N. Continuous mechanical chest compression during in-hospital cardiopulmonary resuscitation of patients with pulseless electrical activity. Resuscitation 2011, 82, 155–159. [Google Scholar] [CrossRef]
- Wirth, S.; Korner, M.; Treitl, M.; Linsenmaier, U.; Leidel, B.A.; Jaschkowitz, T.; Reiser, M.F.; Kanz, K.G. Computed tomography during cardiopulmonary resuscitation using automated chest compression devices—An initial study. Eur. Radiol. 2009, 19, 1857–1866. [Google Scholar] [CrossRef]
- Schubert, E.C.; Kanz, K.G.; Linsenmaier, U.; Bogner, V.; Wirth, S.; Angstwurm, M. Use of computed tomography and mechanical CPR in cardiac arrest to confirm pulmonary embolism: A case study. CJEM 2016, 18, 66–69. [Google Scholar] [CrossRef] [Green Version]
- Agarwala, R.; Barber, R. A pitfall of Autopulse. Anaesthesia 2011, 66, 142–143. [Google Scholar] [CrossRef]
- Wagner, H.; Terkelsen, C.J.; Friberg, H.; Harnek, J.; Kern, K.; Lassen, J.F.; Olivecrona, G.K. Cardiac arrest in the catheterisation laboratory: A 5-year experience of using mechanical chest compressions to facilitate PCI during prolonged resuscitation efforts. Resuscitation 2010, 81, 383–387. [Google Scholar] [CrossRef]
- Weiss, A.; Frisch, C.; Hornung, R.; Baubin, M.; Lederer, W. A retrospective analysis of fibrinolytic and adjunctive antithrombotic treatment during cardiopulmonary resuscitation. Sci. Rep. 2021, 11, 24095. [Google Scholar] [CrossRef]
- Satler, L.F.; Pichard, A.D. The use of automated chest compression for arrest during TAVI. Catheter. Cardiovasc. Interv. 2013, 82, 849–850. [Google Scholar] [CrossRef]
- Vatsgar, T.T.; Ingebrigtsen, O.; Fjose, L.O.; Wikstrom, B.; Nilsen, J.E.; Wik, L. Cardiac arrest and resuscitation with an automatic mechanical chest compression device (LUCAS) due to anaphylaxis of a woman receiving caesarean section because of pre-eclampsia. Resuscitation 2006, 68, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Dumans-Nizard, V.; Fischler, M. Intraoperative use of an automated chest compression device. Anesthesiology 2011, 114, 1253–1255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wind, J.; Hoogland, E.R.; van Heurn, L.W. Preservation techniques for donors after cardiac death kidneys. Curr. Opin. Organ. Transplant. 2011, 16, 157–161. [Google Scholar] [CrossRef]
- Gräsner, J.-T.; Jantzen, T.; Cavus, E.; Gries, A.; Breckwoldt, J.; Böttiger, B.W.; Bein, B.; Dörges, V.; Fischer, M.; Messelken, M.; et al. Neuheiten aus Ausbildung und Lehre, Grundlagenforschung, klinischen Studien und Qualitätsmanagement. 4. Wissenschafttliche Arbeitstage Notfallmedizin 2008 in Kiel. Anästhesiologie Intensivmed. 2008, 49, 679. [Google Scholar]
- FDA. U.S. Food & Drug Administration Website. Available online: www.fda.gov (accessed on 27 July 2022).
- Yannopoulos, D.; Bartos, J.; Raveendran, G.; Walser, E.; Connett, J.; Murray, T.A.; Collins, G.; Zhang, L.; Kalra, R.; Kosmopoulos, M.; et al. Advanced reperfusion strategies for patients with out-of-hospital cardiac arrest and refractory ventricular fibrillation (ARREST): A phase 2, single centre, open-label, randomised controlled trial. Lancet 2020, 396, 1807–1816. [Google Scholar] [CrossRef]
- Rob, D.; Smalcova, J.; Smid, O.; Kral, A.; Kovarnik, T.; Zemanek, D.; Kavalkova, P.; Huptych, M.; Komarek, A.; Franek, O.; et al. Extracorporeal versus conventional cardiopulmonary resuscitation for refractory out-of-hospital cardiac arrest: A secondary analysis of the Prague OHCA trial. Crit. Care 2022, 26, 330. [Google Scholar] [CrossRef]
- Grasner, J.T.; Wnent, J.; Herlitz, J.; Perkins, G.D.; Lefering, R.; Tjelmeland, I.; Koster, R.W.; Masterson, S.; Rossell-Ortiz, F.; Maurer, H.; et al. Survival after out-of-hospital cardiac arrest in Europe - Results of the EuReCa TWO study. Resuscitation 2020, 148, 218–226. [Google Scholar] [CrossRef]
- Wengenmayer, T.; Rombach, S.; Ramshorn, F.; Biever, P.; Bode, C.; Duerschmied, D.; Staudacher, D.L. Influence of low-flow time on survival after extracorporeal cardiopulmonary resuscitation (eCPR). Crit. Care 2017, 21, 157. [Google Scholar] [CrossRef]
- Mørk, S.R.; Bøtker, M.T.; Christensen, S.; Tang, M.; Terkelsen, C.J. Survival and neurological outcome after out-of-hospital cardiac arrest treated with and without mechanical circulatory support. Resusc. Plus 2022, 10, 100230. [Google Scholar] [CrossRef]
- AWMF. S3-Leitlinie 011/021: Einsatz der extrakorporalen Zirkulation (ECLS/ECMO) bei Herz- und Kreislaufversagen; Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF): Berlin, Germany, 2020. [Google Scholar]
- Debaty, G.; Lamhaut, L.; Aubert, R.; Nicol, M.; Sanchez, C.; Chavanon, O.; Bouzat, P.; Durand, M.; Vanzetto, G.; Hutin, A.; et al. Prognostic value of signs of life throughout cardiopulmonary resuscitation for refractory out-of-hospital cardiac arrest. Resuscitation 2021, 162, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Kashiura, M.; Sugiyama, K.; Tanabe, T.; Akashi, A.; Hamabe, Y. Effect of ultrasonography and fluoroscopic guidance on the incidence of complications of cannulation in extracorporeal cardiopulmonary resuscitation in out-of-hospital cardiac arrest: A retrospective observational study. BMC Anesthesiol. 2017, 17, 4. [Google Scholar] [CrossRef] [PubMed]
- Lamhaut, L.; Hutin, A.; Dagron, C.; Baud, F.; An, K.; Carli, P. A new hybrid technique for extracorporeal cardiopulmonary resuscitation for use by nonsurgeons. Emergencias 2021, 33, 156–157. [Google Scholar]
- Danial, P.; Hajage, D.; Nguyen, L.S.; Mastroianni, C.; Demondion, P.; Schmidt, M.; Bougle, A.; Amour, J.; Leprince, P.; Combes, A.; et al. Percutaneous versus surgical femoro-femoral veno-arterial ECMO: A propensity score matched study. Intensive Care Med. 2018, 44, 2153–2161. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, A.W.; Sirois, M.; Laupland, K.B.; Liu, D.; Rowan, K.; Ball, C.G.; Hameed, S.M.; Brown, R.; Simons, R.; Dulchavsky, S.A.; et al. Hand-held thoracic sonography for detecting post-traumatic pneumothoraces: The Extended Focused Assessment with Sonography for Trauma (EFAST). J. Trauma 2004, 57, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Breitkreutz, R.; Price, S.; Steiger, H.V.; Seeger, F.H.; Ilper, H.; Ackermann, H.; Rudolph, M.; Uddin, S.; Weigand, M.A.; Muller, E.; et al. Focused echocardiographic evaluation in life support and peri-resuscitation of emergency patients: A prospective trial. Resuscitation 2010, 81, 1527–1533. [Google Scholar] [CrossRef]
- Nestaas, S.; Stensæth, K.H.; Rosseland, V.; Kramer-Johansen, J. Radiological assessment of chest compression point and achievable compression depth in cardiac patients. Scand. J. Trauma Resusc. Emerg. Med. 2016, 24, 54. [Google Scholar] [CrossRef] [Green Version]
- Pickard, A.; Darby, M.; Soar, J. Radiological assessment of the adult chest: Implications for chest compressions. Resuscitation 2006, 71, 387–390. [Google Scholar] [CrossRef]
- Shin, J.; Rhee, J.E.; Kim, K. Is the inter-nipple line the correct hand position for effective chest compression in adult cardiopulmonary resuscitation? Resuscitation 2007, 75, 305–310. [Google Scholar] [CrossRef]
- Blaivas, M. Transesophageal echocardiography during cardiopulmonary arrest in the emergency department. Resuscitation 2008, 78, 135–140. [Google Scholar] [CrossRef]
- Teran, F.; Dean, A.J.; Centeno, C.; Panebianco, N.L.; Zeidan, A.J.; Chan, W.; Abella, B.S. Evaluation of out-of-hospital cardiac arrest using transesophageal echocardiography in the emergency department. Resuscitation 2019, 137, 140–147. [Google Scholar] [CrossRef]
- Pruszczyk, P.; Goliszek, S.; Lichodziejewska, B.; Kostrubiec, M.; Ciurzynski, M.; Kurnicka, K.; Dzikowska-Diduch, O.; Palczewski, P.; Wyzgal, A. Prognostic value of echocardiography in normotensive patients with acute pulmonary embolism. JACC Cardiovasc. Imaging 2014, 7, 553–560. [Google Scholar] [CrossRef] [Green Version]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.J.; Harjola, V.P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jimenez, D.; et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Heart J. 2020, 41, 543–603. [Google Scholar] [CrossRef] [PubMed]
- Wardi, G.; Blanchard, D.; Dittrich, T.; Kaushal, K.; Sell, R. Right ventricle dysfunction and echocardiographic parameters in the first 24h following resuscitation in the post-cardiac arrest patient: A retrospective cohort study. Resuscitation 2016, 103, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Righini, M.; Le Gal, G.; Aujesky, D.; Roy, P.-M.; Sanchez, O.; Verschuren, F.; Rutschmann, O.; Nonent, M.; Cornuz, J.; Thys, F.; et al. Diagnosis of pulmonary embolism by multidetector CT alone or combined with venous ultrasonography of the leg: A randomised non-inferiority trial. Lancet 2008, 371, 1343–1352. [Google Scholar] [CrossRef] [PubMed]
- Alrajab, S.; Youssef, A.M.; Akkus, N.I.; Caldito, G. Pleural ultrasonography versus chest radiography for the diagnosis of pneumothorax: Review of the literature and meta-analysis. Crit. Care 2013, 17, R208. [Google Scholar] [CrossRef] [Green Version]
- Obermaier, M.; Katzenschlager, S.; Schneider, N.R.E. Diagnostik und invasive Maßnahmen beim Thoraxtrauma. AINS-Anästhesiologie Intensivmed. Notf. Schmerzther. 2020, 55, 620–633. [Google Scholar] [CrossRef]
- Hughes, C.W. Use of an intra-aortic balloon catheter tamponade for controlling intra-abdominal hemorrhage in man. Surgery 1954, 36, 65–68. [Google Scholar] [CrossRef]
- King, D.R. Initial Care of the Severely Injured Patient. N. Engl. J. Med. 2019, 380, 763–770. [Google Scholar] [CrossRef]
- Castellini, G.; Gianola, S.; Biffi, A.; Porcu, G.; Fabbri, A.; Ruggieri, M.P.; Coniglio, C.; Napoletano, A.; Coclite, D.; D'Angelo, D.; et al. Resuscitative endovascular balloon occlusion of the aorta (REBOA) in patients with major trauma and uncontrolled haemorrhagic shock: A systematic review with meta-analysis. World J. Emerg. Surg. 2021, 16, 41. [Google Scholar] [CrossRef] [PubMed]
- Hutin, A.; Levy, Y.; Lidouren, F.; Kohlhauer, M.; Carli, P.; Ghaleh, B.; Lamhaut, L.; Tissier, R. Resuscitative endovascular balloon occlusion of the aorta vs epinephrine in the treatment of non-traumatic cardiac arrest in swine. Ann. Intensive Care 2021, 11, 81. [Google Scholar] [CrossRef] [PubMed]
- Deakin, C.D.; Barron, D.J. Haemodynamic effects of descending aortic occlusion during cardiopulmonary resuscitation. Resuscitation 1996, 33, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Brede, J.R.; Lafrenz, T.; Klepstad, P.; Skjaerseth, E.A.; Nordseth, T.; Sovik, E.; Kruger, A.J. Feasibility of Pre-Hospital Resuscitative Endovascular Balloon Occlusion of the Aorta in Non-Traumatic Out-of-Hospital Cardiac Arrest. J. Am. Heart Assoc. 2019, 8, e014394. [Google Scholar] [CrossRef]
- McGreevy, D.; Dogan, E.; Toivola, A.; Bilos, L.; Pirouzran, A.; Nilsson, K.; Hörer, T. Endovascular resuscitation with aortic balloon occlusion in non-trauma cases: First use of ER-REBOA in Europe. J. Endovasc. Resusc. Trauma Manag. 2017, 1, 42–49. [Google Scholar] [CrossRef]
- Drumheller, B.C.; Pinizzotto, J.; Overberger, R.C.; Sabolick, E.E. Goal-directed cardiopulmonary resuscitation for refractory out-of-hospital cardiac arrest in the emergency Department: A feasibility study. Resusc. Plus 2021, 7, 100159. [Google Scholar] [CrossRef]
- Levis, A.; Greif, R.; Hautz, W.E.; Lehmann, L.E.; Hunziker, L.; Fehr, T.; Haenggi, M. Resuscitative endovascular balloon occlusion of the aorta (REBOA) during cardiopulmonary resuscitation: A pilot study. Resuscitation 2020, 156, 27–34. [Google Scholar] [CrossRef]
- Gamberini, L.; Coniglio, C.; Lupi, C.; Tartaglione, M.; Mazzoli, C.A.; Baldazzi, M.; Cecchi, A.; Ferri, E.; Chiarini, V.; Semeraro, F.; et al. Resuscitative endovascular occlusion of the aorta (REBOA) for refractory out of hospital cardiac arrest. An Utstein-based case series. Resuscitation 2021, 165, 161–169. [Google Scholar] [CrossRef]
- Brede, J.R.; Skjaerseth, E.; Klepstad, P.; Nordseth, T.; Kruger, A.J. Changes in peripheral arterial blood pressure after resuscitative endovascular balloon occlusion of the aorta (REBOA) in non-traumatic cardiac arrest patients. BMC Emerg. Med. 2021, 21, 157. [Google Scholar] [CrossRef]
- Jang, D.H.; Lee, D.K.; Jo, Y.H.; Park, S.M.; Oh, Y.T.; Im, C.W. Resuscitative endovascular occlusion of the aorta (REBOA) as a mechanical method for increasing the coronary perfusion pressure in non-traumatic out-of-hospital cardiac arrest patients. Resuscitation 2022. [Google Scholar] [CrossRef]
- Daley, J.; Buckley, R.; Kisken, K.C.; Barber, D.; Ayyagari, R.; Wira, C.; Aydin, A.; Latich, I.; Lozada, J.C.P.; Joseph, D.; et al. Emergency department initiated resuscitative endovascular balloon occlusion of the aorta (REBOA) for out-of-hospital cardiac arrest is feasible and associated with improvements in end-tidal carbon dioxide. J. Am. Coll. Emerg. Physicians Open 2022, 3, e12791. [Google Scholar] [CrossRef] [PubMed]
- Daley, J.; Morrison, J.J.; Sather, J.; Hile, L. The role of resuscitative endovascular balloon occlusion of the aorta (REBOA) as an adjunct to ACLS in non-traumatic cardiac arrest. Am. J. Emerg. Med. 2017, 35, 731–736. [Google Scholar] [CrossRef] [PubMed]
- Brede, J.R.; Skulberg, A.K.; Rehn, M.; Thorsen, K.; Klepstad, P.; Tylleskar, I.; Farbu, B.; Dale, J.; Nordseth, T.; Wiseth, R.; et al. REBOARREST, resuscitative endovascular balloon occlusion of the aorta in non-traumatic out-of-hospital cardiac arrest: A study protocol for a randomised, parallel group, clinical multicentre trial. Trials 2021, 22, 511. [Google Scholar] [CrossRef] [PubMed]
- Wildner, G.; Pauker, N.; Archan, S.; Gemes, G.; Rigaud, M.; Pocivalnik, M.; Prause, G. Arterial line in prehospital emergency settings - A feasibility study in four physician-staffed emergency medical systems. Resuscitation 2011, 82, 1198–1201. [Google Scholar] [CrossRef]
- Zwisler, S.T.; Zincuk, Y.; Bering, C.B.; Zincuk, A.; Nybo, M.; Mikkelsen, S. Diagnostic value of prehospital arterial blood gas measurements - a randomised controlled trial. Scand. J. Trauma Resusc. Emerg. Med. 2019, 27, 32. [Google Scholar] [CrossRef] [Green Version]
- Gilbert, H.C.; Vender, J.S. Arterial Blood Gas Monitoring. Crit. Care Clin. 1995, 11, 233–248. [Google Scholar] [CrossRef] [PubMed]
- Prause, G.; Ratzenhofer-Komenda, B.; Offner, A.; Lauda, P.; Voit, H.; Pojer, H. Prehospital point of care testing of blood gases and electrolytes - an evaluation of IRMA. Crit. Care 1997, 1, 79–83. [Google Scholar] [CrossRef] [Green Version]
- Spindelboeck, W.; Gemes, G.; Strasser, C.; Toescher, K.; Kores, B.; Metnitz, P.; Haas, J.; Prause, G. Arterial blood gases during and their dynamic changes after cardiopulmonary resuscitation: A prospective clinical study. Resuscitation 2016, 106, 24–29. [Google Scholar] [CrossRef]
- Spindelboeck, W.; Moser, A. Spontaneous tension pneumothorax and CO(2) narcosis in a near fatal episode of chronic obstructive pulmonary disease exacerbation. Am. J. Emerg. Med. 2012, 30, 1664.e3. [Google Scholar] [CrossRef]
- Kleber, C.; Giesecke, M.T.; Tsokos, M.; Haas, N.P.; Buschmann, C.T. Trauma-related preventable deaths in Berlin 2010: Need to change prehospital management strategies and trauma management education. World J. Surg. 2013, 37, 1154–1161. [Google Scholar] [CrossRef]
- Laan, D.V.; Vu, T.D.N.; Thiels, C.A.; Pandian, T.K.; Schiller, H.J.; Murad, M.H.; Aho, J.M. Chest wall thickness and decompression failure: A systematic review and meta-analysis comparing anatomic locations in needle thoracostomy. Injury 2016, 47, 797–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inaba, K.; Branco, B.C.; Eckstein, M.; Shatz, D.V.; Martin, M.J.; Green, D.J.; Noguchi, T.T.; Demetriades, D. Optimal positioning for emergent needle thoracostomy: A cadaver-based study. J. Trauma 2011, 71, 1099–1103. [Google Scholar] [CrossRef] [PubMed]
- Advanced Trauma Life Support. ATLS® 10th Edition Compendium of Change; American College of Surgeons: Chicago, IL, USA, 2018. [Google Scholar]
- Joint Trauma System’s (JTS) Committee on Tactical Combat Casualty Care (CoTCCC). Tactical Combat Casualty Care (TCCC) Guidelines for Medical Personnel. J. Spec. Oper. Med. 2022, 22, 11–17. [Google Scholar] [CrossRef]
- Martin, M.; Satterly, S.; Inaba, K.; Blair, K. Does needle thoracostomy provide adequate and effective decompression of tension pneumothorax? J. Trauma Acute Care Surg. 2012, 73, 1412–1417. [Google Scholar] [CrossRef] [PubMed]
- Garner, A.; Poynter, E.; Parsell, R.; Weatherall, A.; Morgan, M.; Lee, A. Association between three prehospital thoracic decompression techniques by physicians and complications: A retrospective, multicentre study in adults. Eur. J. Trauma Emerg. Surg. 2022. [Google Scholar] [CrossRef]
- Adler, Y.; Charron, P.; Imazio, M.; Badano, L.; Baron-Esquivias, G.; Bogaert, J.; Brucato, A.; Gueret, P.; Klingel, K.; Lionis, C.; et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2015, 36, 2921–2964. [Google Scholar] [CrossRef]
- Alerhand, S.; Carter, J.M. What echocardiographic findings suggest a pericardial effusion is causing tamponade? Am. J. Emerg. Med. 2019, 37, 321–326. [Google Scholar] [CrossRef]
- Alpert, E.A.; Amit, U.; Guranda, L.; Mahagna, R.; Grossman, S.A.; Bentancur, A. Emergency department point-of-care ultrasonography improves time to pericardiocentesis for clinically significant effusions. Clin. Exp. Emerg. Med. 2017, 4, 128–132. [Google Scholar] [CrossRef] [Green Version]
- Flaris, A.N.; Simms, E.R.; Prat, N.; Reynard, F.; Caillot, J.L.; Voiglio, E.J. Clamshell incision versus left anterolateral thoracotomy. Which one is faster when performing a resuscitative thoracotomy? The tortoise and the hare revisited. World J. Surg. 2015, 39, 1306–1311. [Google Scholar] [CrossRef]
- Davies, G.E.; Lockey, D.J. Thirteen survivors of prehospital thoracotomy for penetrating trauma: A prehospital physician-performed resuscitation procedure that can yield good results. J. Trauma 2011, 70, E75–E78. [Google Scholar] [CrossRef]
- Endo, A.; Shiraishi, A.; Otomo, Y.; Tomita, M.; Matsui, H.; Murata, K. Open-chest versus closed-chest cardiopulmonary resuscitation in blunt trauma: Analysis of a nationwide trauma registry. Crit. Care 2017, 21, 169. [Google Scholar] [CrossRef]
- Tonna, J.E.; Keenan, H.T.; Weir, C. A qualitative analysis of physician decision making in the use of extracorporeal cardiopulmonary resuscitation for refractory cardiac arrest. Resusc. Plus 2022, 11, 100278. [Google Scholar] [CrossRef]
- Tonna, J.E.; Becker, L.B.; Girotra, S.; Selzman, C.; Thiagarajan, R.R.; Presson, A.P.; Zhang, C.; Keenan, H.T. Resuscitation Using eCPR to Predict Survival After In-Hospital Cardiac Arrest (Rescue-IHCA Score) Survival Prediction Model--An Analysis of the American Heart Association Get With the Guidelines--Resuscitation Registry. Circulation 2019, 140, A205. [Google Scholar] [CrossRef]
- Otani, T.; Sawano, H.; Natsukawa, T.; Nakashima, T.; Oku, H.; Gon, C.; Takahagi, M.; Hayashi, Y. Low-flow time is associated with a favorable neurological outcome in out-of-hospital cardiac arrest patients resuscitated with extracorporeal cardiopulmonary resuscitation. J. Crit. Care 2018, 48, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Al-Azri, N.H. How to think like an emergency care provider: A conceptual mental model for decision making in emergency care. Int. J. Emerg. Med. 2020, 13, 17. [Google Scholar] [CrossRef]
- Alm-Kruse, K.; Sorensen, G.; Osbakk, S.A.; Sunde, K.; Bendz, B.; Andersen, G.O.; Fiane, A.; Hagen, O.A.; Kramer-Johansen, J. Outcome in refractory out-of-hospital cardiac arrest before and after implementation of an ECPR protocol. Resuscitation 2021, 162, 35–42. [Google Scholar] [CrossRef]
- Michels, G.; Wengenmayer, T.; Hagl, C.; Dohmen, C.; Bottiger, B.W.; Bauersachs, J.; Markewitz, A.; Bauer, A.; Grasner, J.T.; Pfister, R.; et al. Recommendations for extracorporeal cardiopulmonary resuscitation (eCPR): Consensus statement of DGIIN, DGK, DGTHG, DGfK, DGNI, DGAI, DIVI and GRC. Clin. Res. Cardiol. 2019, 108, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Lacerenza, C.N.; Marlow, S.L.; Tannenbaum, S.I.; Salas, E. Team development interventions: Evidence-based approaches for improving teamwork. Am. Psychol. 2018, 73, 517–531. [Google Scholar] [CrossRef]
- Couper, K.; Salman, B.; Soar, J.; Finn, J.; Perkins, G.D. Debriefing to improve outcomes from critical illness: A systematic review and meta-analysis. Intensive Care Med. 2013, 39, 1513–1523. [Google Scholar] [CrossRef]
- Rudolph, J.W.; Simon, R.; Raemer, D.B.; Eppich, W.J. Debriefing as formative assessment: Closing performance gaps in medical education. Acad. Emerg. Med. 2008, 15, 1010–1016. [Google Scholar] [CrossRef]
- Leong, K.; Hanskamp-Sebregts, M.; van der Wal, R.A.; Wolff, A.P. Effects of perioperative briefing and debriefing on patient safety: A prospective intervention study. BMJ Open 2017, 7, e018367. [Google Scholar] [CrossRef] [Green Version]
- Johnson, T.J.; Millinchamp, F.J.; Kelly, F.E. Use of a team immediate debrief tool to improve staff well-being after potentially traumatic events. Anaesthesia 2021, 76, 1001–1002. [Google Scholar] [CrossRef]
- Roehl, A.; Grottke, O. Prehospital administration of blood and plasma products. Curr. Opin. Anaesthesiol. 2021, 34, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Crombie, N.; Doughty, H.A.; Bishop, J.R.B.; Desai, A.; Dixon, E.F.; Hancox, J.M.; Herbert, M.J.; Leech, C.; Lewis, S.J.; Nash, M.R.; et al. Resuscitation with blood products in patients with trauma-related haemorrhagic shock receiving prehospital care (RePHILL): A multicentre, open-label, randomised, controlled, phase 3 trial. Lancet Haematol. 2022, 9, e250–e261. [Google Scholar] [CrossRef] [PubMed]
- Thiels, C.A.; Aho, J.M.; Fahy, A.S.; Parker, M.E.; Glasgow, A.E.; Berns, K.S.; Habermann, E.B.; Zietlow, S.P.; Zielinski, M.D. Prehospital Blood Transfusions in Non-Trauma Patients. World J. Surg. 2016, 40, 2297–2304. [Google Scholar] [CrossRef] [PubMed]
- Thies, K.C.; Truhlar, A.; Keene, D.; Hinkelbein, J.; Rutzler, K.; Brazzi, L.; Vivien, B. Pre-hospital blood transfusion—An ESA survey of European practice. Scand. J. Trauma Resusc. Emerg. Med. 2020, 28, 79. [Google Scholar] [CrossRef]






| Trial Abbreviation and Quotation | Design and Inclusion Criteria | Main Findings and Limitations |
|---|---|---|
| Compression Feedback for Patients with In-hospital Cardiac Arrest [29] | Cardio First Angel® vs. conventional manual CPR; prospective individualized RCT, multi-center (Iran); in-hospital; 2015; 450 vs. 450 cases out of 1454 Inclusion criteria: age ≥ 18 years, admitted to ICU, resuscitation status (full code), and informed consent | ↑ ROSC, ↑ ICU discharge, ↑ hospital discharge Limitations: selection bias (no primary cardiac entity), performance bias (quality monitoring), and training effect |
| Automated Real-time Feedback on CPR Study [31] | HeartStart-MRx® vs. conventional manual CPR; prospective cluster RCT, multi-center (USA, Canada); out-of-hospital; 2007–2009; 815 vs. 771 cases out of 1819 Inclusion criteria: age ≥ 20, defibrillation or chest compressions by study vehicle team and non-TCA | ↑ hands-on time, ↑ compression depth, ↑ complete release, ± ROSC, ± admission, ± discharge, ± CPC Limitations: design (allocation concealment and no regression analysis), selection bias (trial vehicle), and training effect |
| Trial Abbreviation and Quotation | Design and Inclusion Criteria | Main Findings and Limitations |
|---|---|---|
| (a) RCTs on REBOA in non-traumatic cardiac arrest | ||
| REBOARREST [107] | ALS an REBOA vs. standard ALS; RCT, multi-center (Norway); out-of-hospital; 2022-ongoing; calculated enrollment 200 patientsInclusion criteria: age 18–80, OHCA, non-TCA, witnessed or <10 min from the debut of arrest, and commenced ALS established and can be continued | Study currently recruiting |
| (b) observational trials on REBOA in non-traumatic cardiac arrest | ||
| Feasibility of Pre-Hospital REBOA [98] | ALS an REBOA vs. standard ALS; RCT, single-center (Norway); out-of-hospital, helicopter; 2018–2019; 10 patientsInclusion criteria: age 18–75, OHCA, non-TCA, and witnessed or <10 min from the debut of arrest | The attempt was 100% successful (80% first attempt), 60% ROSC, 30% admission to hospital, 10% survival (30 days), procedural time 11.7 ± 3.2 min, and etCO2 + 1.75 kPa after 1 minLimitations: feasibility study, a decision by study group, single-center, a small number of researchers and patients, and no autopsies (adverse effects) |
| NEURESCUE® Device as an Adjunct to Cardiac Arrest [NCT05146661] | REBOA device; interventional open-label single group study, single-center (Germany); in hospital emergency department; 2022-ongoing; calculated enrollment 10 patientsInclusion criteria: age 18–75, witnessed, CPR initiated ≤ 7 min of presumed arrest, not responding to standard ALS, and total CPR time ≤ 40 min at enrollment | Study currently recruiting |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Obermaier, M.; Katzenschlager, S.; Kofler, O.; Weilbacher, F.; Popp, E. Advanced and Invasive Cardiopulmonary Resuscitation (CPR) Techniques as an Adjunct to Advanced Cardiac Life Support. J. Clin. Med. 2022, 11, 7315. https://doi.org/10.3390/jcm11247315
Obermaier M, Katzenschlager S, Kofler O, Weilbacher F, Popp E. Advanced and Invasive Cardiopulmonary Resuscitation (CPR) Techniques as an Adjunct to Advanced Cardiac Life Support. Journal of Clinical Medicine. 2022; 11(24):7315. https://doi.org/10.3390/jcm11247315
Chicago/Turabian StyleObermaier, Manuel, Stephan Katzenschlager, Othmar Kofler, Frank Weilbacher, and Erik Popp. 2022. "Advanced and Invasive Cardiopulmonary Resuscitation (CPR) Techniques as an Adjunct to Advanced Cardiac Life Support" Journal of Clinical Medicine 11, no. 24: 7315. https://doi.org/10.3390/jcm11247315