
COPD Exacerbation-Related Pathogens and Previous COPD Treatment
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Variables
2.3. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Park, Y.B.; Rhee, C.K.; Yoon, H.K.; Oh, Y.M.; Lim, S.Y.; Lee, J.H.; Yoo, K.H.; Ahn, J.H.; Committee of the Korean, C.G. Revised (2018) COPD Clinical Practice Guideline of the Korean Academy of Tuberculosis and Respiratory Disease: A Summary. Tuberc. Respir. Dis. 2018, 81, 261–273. [Google Scholar] [CrossRef] [PubMed]
- Raherison, C.; Girodet, P.O. Epidemiology of COPD. Eur. Respir. Rev. 2009, 18, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef] [PubMed]
- Sethi, S.; Murphy, T.F. Infection in the pathogenesis and course of chronic obstructive pulmonary disease. N. Engl. J. Med. 2008, 359, 2355–2365. [Google Scholar] [CrossRef]
- Rosell, A.; Monso, E.; Soler, N.; Torres, F.; Angrill, J.; Riise, G.; Zalacain, R.; Morera, J.; Torres, A. Microbiologic determinants of exacerbation in chronic obstructive pulmonary disease. Arch. Intern. Med. 2005, 165, 891–897. [Google Scholar] [CrossRef]
- Shimizu, K.; Yoshii, Y.; Morozumi, M.; Chiba, N.; Ubukata, K.; Uruga, H.; Hanada, S.; Saito, N.; Kadota, T.; Ito, S.; et al. Pathogens in COPD exacerbations identified by comprehensive real-time PCR plus older methods. Int. J. Chron. Obstruct. Pulmon. Dis. 2015, 10, 2009–2016. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.W.; Sim, Y.S.; Jung, J.Y.; Seo, H.; Park, J.W.; Min, K.H.; Lee, J.H.; Kim, B.K.; Lee, M.G.; Oh, Y.M.; et al. A Multicenter Study to Identify the Respiratory Pathogens Associated with Exacerbation of Chronic Obstructive Pulmonary Disease in Korea. Tuberc. Respir. Dis. 2022, 85, 37–46. [Google Scholar] [CrossRef]
- Seo, H.; Sim, Y.S.; Min, K.H.; Lee, J.H.; Kim, B.K.; Oh, Y.M.; Ra, S.W.; Kim, T.H.; Hwang, Y.I.; Park, J.W. The Relationship between Comorbidities and Microbiologic Findings in Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease. Int. J. Chron. Obstruct. Pulmon. Dis. 2022, 17, 855–867. [Google Scholar] [CrossRef]
- Singh, S.; Amin, A.V.; Loke, Y.K. Long-term use of inhaled corticosteroids and the risk of pneumonia in chronic obstructive pulmonary disease: A meta-analysis. Arch. Intern. Med. 2009, 169, 219–229. [Google Scholar] [CrossRef]
- Miravitlles, M.; Auladell-Rispau, A.; Monteagudo, M.; Vazquez-Niebla, J.C.; Mohammed, J.; Nunez, A.; Urrutia, G. Systematic review on long-term adverse effects of inhaled corticosteroids in the treatment of COPD. Eur. Respir. Rev. 2021, 30, 160. [Google Scholar] [CrossRef]
- Andrejak, C.; Nielsen, R.; Thomsen, V.O.; Duhaut, P.; Sorensen, H.T.; Thomsen, R.W. Chronic respiratory disease, inhaled corticosteroids and risk of non-tuberculous mycobacteriosis. Thorax 2013, 68, 256–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brode, S.K.; Campitelli, M.A.; Kwong, J.C.; Lu, H.; Marchand-Austin, A.; Gershon, A.S.; Jamieson, F.B.; Marras, T.K. The risk of mycobacterial infections associated with inhaled corticosteroid use. Eur. Respir. J. 2017, 50, 1700037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brassard, P.; Suissa, S.; Kezouh, A.; Ernst, P. Inhaled corticosteroids and risk of tuberculosis in patients with respiratory diseases. Am. J. Respir. Crit. Care Med. 2011, 183, 675–678. [Google Scholar] [CrossRef] [PubMed]
- Ernst, P.; Gonzalez, A.V.; Brassard, P.; Suissa, S. Inhaled corticosteroid use in chronic obstructive pulmonary disease and the risk of hospitalization for pneumonia. Am. J. Respir. Crit. Care Med. 2007, 176, 162–166. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Kim, K.; Hyun, M.K.; Jang, E.J.; Lee, N.R.; Yim, J.J. Use of inhaled corticosteroids and the risk of tuberculosis. Thorax 2013, 68, 1105–1113. [Google Scholar] [CrossRef] [Green Version]
- Suissa, S.; Patenaude, V.; Lapi, F.; Ernst, P. Inhaled corticosteroids in COPD and the risk of serious pneumonia. Thorax 2013, 68, 1029–1036. [Google Scholar] [CrossRef] [Green Version]
- Shafiek, H.; Verdu, J.; Iglesias, A.; Ramon-Clar, L.; Toledo-Pons, N.; Lopez-Causape, C.; Juan, C.; Fraile-Ribot, P.; Oliver, A.; Cosio, B.G. Inhaled corticosteroid dose is associated with Pseudomonas aeruginosa infection in severe COPD. BMJ Open Respir. Res. 2021, 8, e001067. [Google Scholar] [CrossRef]
- GOLD. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. Global Initiative for Chronic Obstructive Lung Disease. 2020. Available online: https://goldcopd.org/wp-content/uploads/2019/12/GOLD-2020-FINAL-ver1.2-03Dec19_WMV.pdf (accessed on 1 July 2022).
- Boixeda, R.; Rabella, N.; Sauca, G.; Delgado, M.; Martinez-Costa, X.; Mauri, M.; Vicente, V.; Palomera, E.; Serra-Prat, M.; Capdevila, J.A. Microbiological study of patients hospitalized for acute exacerbation of chronic obstructive pulmonary disease (AE-COPD) and the usefulness of analytical and clinical parameters in its identification (VIRAE study). Int. J. Chron. Obstruct. Pulmon. Dis. 2012, 7, 327–335. [Google Scholar] [CrossRef] [Green Version]
- Contoli, M.; Pauletti, A.; Rossi, M.R.; Spanevello, A.; Casolari, P.; Marcellini, A.; Forini, G.; Gnesini, G.; Marku, B.; Barnes, N.; et al. Long-term effects of inhaled corticosteroids on sputum bacterial and viral loads in COPD. Eur. Respir. J. 2017, 50, 1700451. [Google Scholar] [CrossRef] [Green Version]
- Eklof, J.; Ingebrigtsen, T.S.; Sorensen, R.; Saeed, M.I.; Alispahic, I.A.; Sivapalan, P.; Boel, J.B.; Bangsborg, J.; Ostergaard, C.; Dessau, R.B.; et al. Use of inhaled corticosteroids and risk of acquiring Pseudomonas aeruginosa in patients with chronic obstructive pulmonary disease. Thorax 2022, 77, 573–580. [Google Scholar] [CrossRef]
- Cheng, S.L.; Su, K.C.; Wang, H.C.; Perng, D.W.; Yang, P.C. Chronic obstructive pulmonary disease treated with inhaled medium- or high-dose corticosteroids: A prospective and randomized study focusing on clinical efficacy and the risk of pneumonia. Drug Des. Devel. Ther. 2014, 8, 601–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, C.; Goldmann, T.; Rohmann, K.; Rupp, J.; Marwitz, S.; Rotta Detto Loria, J.; Limmer, S.; Zabel, P.; Dalhoff, K.; Dromann, D. Budesonide Inhibits Intracellular Infection with Non-Typeable Haemophilus influenzae Despite Its Anti-Inflammatory Effects in Respiratory Cells and Human Lung Tissue: A Role for p38 MAP Kinase. Respiration 2015, 90, 416–425. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Vidal, C.; Almagro, P.; Romani, V.; Rodriguez-Carballeira, M.; Cuchi, E.; Canales, L.; Blasco, D.; Heredia, J.L.; Garau, J. Pseudomonas aeruginosa in patients hospitalised for COPD exacerbation: A prospective study. Eur. Respir. J. 2009, 34, 1072–1078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuwal, A.; Joshi, V.; Dutt, N.; Singh, S.; Agarwal, K.C.; Purohit, G. A Prospective Study of Bacteriological Etiology in Hospitalized Acute Exacerbation of COPD Patients: Relationship with Lung Function and Respiratory Failure. Turk. Thorac. J. 2018, 19, 19–27. [Google Scholar] [CrossRef] [Green Version]
- van de Garde, M.D.; Martinez, F.O.; Melgert, B.N.; Hylkema, M.N.; Jonkers, R.E.; Hamann, J. Chronic exposure to glucocorticoids shapes gene expression and modulates innate and adaptive activation pathways in macrophages with distinct changes in leukocyte attraction. J. Immunol. 2014, 192, 1196–1208. [Google Scholar] [CrossRef] [Green Version]
- Sethi, S.; Anzueto, A.; Miravitlles, M.; Arvis, P.; Alder, J.; Haverstock, D.; Trajanovic, M.; Wilson, R. Determinants of bacteriological outcomes in exacerbations of chronic obstructive pulmonary disease. Infection 2016, 44, 65–76. [Google Scholar] [CrossRef] [Green Version]
- Hurst, J.R.; Vestbo, J.; Anzueto, A.; Locantore, N.; Mullerova, H.; Tal-Singer, R.; Miller, B.; Lomas, D.A.; Agusti, A.; Macnee, W.; et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N. Engl. J. Med. 2010, 363, 1128–1138. [Google Scholar] [CrossRef] [Green Version]
- Eklof, J.; Sorensen, R.; Ingebrigtsen, T.S.; Sivapalan, P.; Achir, I.; Boel, J.B.; Bangsborg, J.; Ostergaard, C.; Dessau, R.B.; Jensen, U.S.; et al. Pseudomonas aeruginosa and risk of death and exacerbations in patients with chronic obstructive pulmonary disease: An observational cohort study of 22,053 patients. Clin. Microbiol. Infect. 2020, 26, 227–234. [Google Scholar] [CrossRef] [Green Version]
- Gunen, H.; Hacievliyagil, S.S.; Yetkin, O.; Gulbas, G.; Mutlu, L.C.; In, E. The role of nebulised budesonide in the treatment of exacerbations of COPD. Eur. Respir. J. 2007, 29, 660–667. [Google Scholar] [CrossRef] [Green Version]
- Diederen, B.M.; van der Valk, P.D.; Kluytmans, J.A.; Peeters, M.F.; Hendrix, R. The role of atypical respiratory pathogens in exacerbations of chronic obstructive pulmonary disease. Eur. Respir. J. 2007, 30, 240–244. [Google Scholar] [CrossRef]
- Messous, S.; Trabelsi, I.; Grissa, M.H.; Nouira, S.; Pozzetto, B.; Mastouri, M. Prevalence of Chlamydophila pneumoniae and Mycoplasma pneumoniae IgM and IgG antibodies in Tunisian patients presenting with exacerbation of chronic obstructive pulmonary disease. Med. Mal. Infect. 2017, 47, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, S.; Gonullu, N.; Yildiz, B.P.; Hattatoglu, D.G.; Kuskucu, M.; Midilli, K.; Aygun, G.; Mayda, P.Y.; Musellim, B. The role of typical and atypical pathogens in acute exacerbations of chronic obstructive pulmonary disease. Clin. Respir. J. 2021, 15, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Varma-Basil, M.; Dwivedi, S.K.D.; Kumar, K.; Pathak, R.; Rastogi, R.; Thukral, S.S.; Shariff, M.; Vijayan, V.K.; Chhabra, S.K.; Chaudhary, R. Role of Mycoplasma pneumoniae infection in acute exacerbations of chronic obstructive pulmonary disease. J. Med. Microbiol. 2009, 58, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.Y.; Choe, Y.H.; Lee, S.Y.; Kim, W.J.; Lee, J.D.; Ra, S.W.; Choi, E.G.; Lee, J.S.; Park, M.J.; Na, J.O. Use of serology and polymerase chain reaction to detect atypical respiratory pathogens during acute exacerbation of chronic obstructive pulmonary disease. Korean J. Intern. Med. 2018, 33, 941–951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foy, H.M.; Kenny, G.E.; Cooney, M.K.; Allan, I.D. Long-term epidemiology of infections with Mycoplasma pneumoniae. J. Infect. Dis. 1979, 139, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Walter, N.D.; Grant, G.B.; Bandy, U.; Alexander, N.E.; Winchell, J.M.; Jordan, H.T.; Sejvar, J.J.; Hicks, L.A.; Gifford, D.R.; Alexander, N.T.; et al. Community outbreak of Mycoplasma pneumoniae infection: School-based cluster of neurologic disease associated with household transmission of respiratory illness. J. Infect. Dis. 2008, 198, 1365–1374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, F.W.; Ip, M.; Chan, P.K.; Chan, M.C.; To, K.W.; Ng, S.S.; Chau, S.S.; Tang, J.W.; Hui, D.S. Viral etiology of acute exacerbations of COPD in Hong Kong. Chest 2007, 132, 900–908. [Google Scholar] [CrossRef]
- Tan, W.C.; Xiang, X.; Qiu, D.; Ng, T.P.; Lam, S.F.; Hegele, R.G. Epidemiology of respiratory viruses in patients hospitalized with near-fatal asthma, acute exacerbations of asthma, or chronic obstructive pulmonary disease. Am. J. Med. 2003, 115, 272–277. [Google Scholar] [CrossRef]
- Biancardi, E.; Fennell, M.; Rawlinson, W.; Thomas, P.S. Viruses are frequently present as the infecting agent in acute exacerbations of chronic obstructive pulmonary disease in patients presenting to hospital. Intern. Med. J. 2016, 46, 1160–1165. [Google Scholar] [CrossRef]
- Love, M.E.; Proud, D. Respiratory Viral and Bacterial Exacerbations of COPD-The Role of the Airway Epithelium. Cells 2022, 11, 1416. [Google Scholar] [CrossRef]
- Kan, O.K.; Washio, Y.; Fujimoto, T.; Shiroyama, N.; Nakano, T.; Wakamatsu, K.; Takata, S.; Yoshida, M.; Fujita, M.; Matsumoto, K. Differences in the spectrum of respiratory viruses and detection of human rhinovirus C in exacerbations of adult asthma and chronic obstructive pulmonary disease. Respir. Investig. 2022, 60, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Koul, P.A.; Mir, H.; Akram, S.; Potdar, V.; Chadha, M.S. Respiratory viruses in acute exacerbations of chronic obstructive pulmonary disease. Lung India 2017, 34, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.C.; Choi, S.H.; Huh, J.W.; Sung, H.; Hong, S.B.; Lim, C.M.; Koh, Y. Different pattern of viral infections and clinical outcomes in patient with acute exacerbation of chronic obstructive pulmonary disease and chronic obstructive pulmonary disease with pneumonia. J. Med. Virol. 2016, 88, 2092–2099. [Google Scholar] [CrossRef] [PubMed]
- Jang, J.G.; Ahn, J.H.; Jin, H.J. Incidence and Prognostic Factors of Respiratory Viral Infections in Severe Acute Exacerbation of Chronic Obstructive Pulmonary Disease. Int. J. Chron. Obstruct. Pulmon. Dis. 2021, 16, 1265–1273. [Google Scholar] [CrossRef]
- Thomas, B.J.; Porritt, R.A.; Hertzog, P.J.; Bardin, P.G.; Tate, M.D. Glucocorticosteroids enhance replication of respiratory viruses: Effect of adjuvant interferon. Sci. Rep. 2014, 4, 7176. [Google Scholar] [CrossRef] [Green Version]
- Yamaya, M.; Nishimura, H.; Nadine, L.; Kubo, H.; Nagatomi, R. Formoterol and budesonide inhibit rhinovirus infection and cytokine production in primary cultures of human tracheal epithelial cells. Respir. Investig. 2014, 52, 251–260. [Google Scholar] [CrossRef]
- Martinez-Garcia, M.A.; Faner, R.; Oscullo, G.; de la Rosa, D.; Soler-Cataluna, J.J.; Ballester, M.; Agusti, A. Inhaled Steroids, Circulating Eosinophils, Chronic Airway Infection, and Pneumonia Risk in Chronic Obstructive Pulmonary Disease. A Network Analysis. Am. J. Respir. Crit. Care Med. 2020, 201, 1078–1085. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 1177) | No Inhaler (n = 222) | SABA (n = 50) | ICS (n = 21) | LABA (n = 24) | LAMA (n = 126) | ICS/LABA (n = 143) | LABA/LAMA (n = 193) | ICS/LABA/LAMA (n = 399) | p-Value | |
|---|---|---|---|---|---|---|---|---|---|---|
| Sex, male | 974 (83%) | 188 (85%) | 44 (88%) | 17 (81%) | 19 (83%) | 102 (81%) | 112 (78%) | 157 (81%) | 335 (84%) | 0.718 |
| Age, years | 75 (69–80) | 75 (69–80) | 77 (71–81) | 80 (73–85) | 75 (62–82) | 77 (72–81) | 75 (67–81) | 74 (68–80) | 74 (68–79) | 0.023 |
| BMI, kg/m2 | 21.3 (18.8–23.9) | 21.5 (19.1–24.3) | 21.0 (18.7–23.7) | 20.2 (17.3–21.7) | 22.2 (17.5–24.9) | 21.1 (18.7–24.0) | 21.4 (18.7–24.0) | 21.3 (18.6–23.6) | 21.3 (18.8–23.9) | 0.773 |
| Disease duration | 6.0 (2.5–11.0) | 4.0 (1.0–8.0) | 4.5 (0.1–10.0) | 5.0 (2.5–10.0) | 4.0 (2.0–7.3) | 6.0 (2.0–10.0) | 5.0 (2.0–10.0) | 5.0 (2.0–10.0) | 8.3 (4.0–15.0) | <0.001 |
| Treatment duration | 5.0 (2.0–10.0) | 3.0 (1.0–7.0) | 4.0 (0.2–10.0) | 4.0 (2.5–7.0) | 4.0 (2.0–7.3) | 5.0 (2.0–10.0) | 5.0 (2.0–10.0) | 5.0 (2.0–10.0) | 8.0 (4.0–14.0) | <0.001 |
| Smoking history | 0.001 | |||||||||
| Never smoker | 312 (27%) | 69 (32%) | 12 (25%) | 10 (48%) | 8 (35%) | 43 (35%) | 39 (28%) | 48 (26%) | 83 (21%) | |
| Current smoker | 153 (13%) | 38 (17%) | 8 (16%) | 2 (10%) | 1 (4.3%) | 18 (15%) | 23 (16%) | 28 (15%) | 35 (15%) | |
| Ex-smoker | 686 (60%) | 112 (51%) | 29 (59%) | 9 (43%) | 14 (61%) | 61 (50%) | 80 (56%) | 110 (60%) | 271 (70%) | |
| Pack-years | 40.0 (21.5–50.0) | 36.5 (20.0–50.0) | 30.0 (20.0–50.0) | 30.0 (5.0–40.0) | 30.0 (20.0–44.0) | 40.0 (20.0–50.0) | 40.0 (18.8–50.0) | 40.0 (20.0–50.0) | 40.0 (25.0–50.0) | 0.081 |
| Previous respiratory disease | ||||||||||
| Tuberculosis | 375 (32%) | 69 (31%) | 15 (30%) | 6 (29%) | 12 (52%) | 44 (35%) | 37 (26%) | 72 (37%) | 120 (30%) | 0.150 |
| Bronchiectasis | 168 (14%) | 35 (16%) | 4 (8.0%) | 1 (4.8%) | 3 (13%) | 13 (10%) | 21 (15%) | 29 (15%) | 62 (16%) | 0.559 |
| Interstitial lung disease | 27 (2.3%) | 9 (4.1%) | 1 (2.0%) | 0 | 1 (4.3%) | 2 (1.6%) | 0 | 4 (2.1%) | 10 (2.5%) | 0.353 |
| Co-morbidities | ||||||||||
| Diabetes mellitus | 317 (26%) | 75 (34%) | 16 (32%) | 6 (29%) | 3 (13%) | 31 (25%) | 39 (27%) | 32 (25%) | 115 (29%) | 0.006 |
| Hypertension | 580 (49%) | 110 (49%) | 30 (60%) | 13 (62%) | 15 (65%) | 62 (49%) | 77 (54%) | 87 (45%) | 186 (47%) | 0.208 |
| Congestive heart disease | 166 (14%) | 36 (16%) | 7 (14%) | 3 (14%) | 4 (17%) | 19 (15%) | 19 (13%) | 11 (6%) | 67 (17%) | 0.038 |
| Chronic kidney disease | 75 (6.4%) | 22 (10%) | 2 (4.0%) | 2 (9.5%) | 6 (26%) | 5 (4.0%) | 10 (7.0%) | 12 (6.2%) | 16 (4.0%) | 0.001 |
| Cerebrovascular disease | 70 (5.9%) | 19 (8.6%) | 5 (10%) | 1 (4.8%) | 1 (4.3%) | 9 (7.1%) | 12 (8.4%) | 12 (6.2%) | 11 (2.8%) | 0.062 |
| Advanced cancer | 138 (12%) | 23 (10%) | 5 (10%) | 0 | 1 (4.3%) | 18 (14%) | 18 (13%) | 25 (13%) | 48 (12%) | 0.568 |
| Lung function (n = 898) | ||||||||||
| FEV1, L | 1.07 (0.77–1.50) | 1.20 (0.81–1.91) | 1.14 (0.59–1.50) | 1.34 (0.95–1.61) | 1.25 (1.03–1.65) | 1.18 (0.78–1.68) | 1.21 (0.86–1.57) | 1.17 (0.90–1.59) | 0.94 (0.71–1.32) | < 0.001 |
| FEV1, % predicted | 47 (33–63) | 53 (37–73) | 42 (28–59) | 53 (43–70) | 52 (38–72) | 56 (33–70) | 53 (36–68) | 49 (37–64) | 39 (29–54) | <0.001 |
| Bronchodilator response | 166 (14%) | 17 (8%) | 5 (10%) | 8 (40%) | 4 (19%) | 8 (7%) | 21 (15%) | 22 (11%) | 81 (21%) | <0.001 |
| GOLD group | <0.001 | |||||||||
| A | 63 (5.4%) | 16 (7.2%) | 0 | 0 | 2 (8.7%) | 11 (8.7%) | 6 (4.2%) | 17 (8.8%) | 11 (2.8%) | |
| B | 140 (12%) | 24 (11%) | 8 (16%) | 3 (14%) | 5 (22%) | 16 (13%) | 12 (8%) | 33 (17%) | 39 (10%) | |
| C | 40 (3.4%) | 2 (0.9%) | 0 | 2 (10%) | 0 | 0 | 10 (5.2%) | 10 (5.2%) | 16 (4.0%) | |
| D | 224 (19%) | 4 (1.8%) | 5 (10%) | 1 (4.8%) | 8 (35%) | 15 (12%) | 31 (22%) | 40 (21%) | 120 (30%) | |
| Leukotriene receptor antagonist | 216 (18%) | 12 (5.4%) | 2 (4.1%) | 4 (19%) | 4 (17%) | 12 (10%) | 31 (22%) | 29 (15%) | 122 (31%) | <0.001 |
| Xanthine derivative | 365 (31%) | 31 (14%) | 8 (16%) | 9 (43%) | 5 (22%) | 40 (32%) | 45 (32%) | 55 (29%) | 172 (43%) | <0.001 |
| Systemic steroid | 238 (20%) | 23 (10%) | 11 (22%) | 9 (43%) | 5 (22%) | 19 (15%) | 38 (27%) | 30 (16%) | 103 (26%) | <0.001 |
| Inhaled Corticosteroid | Systemic Steroid | |||||
|---|---|---|---|---|---|---|
| OR | CI | p-Value | OR | CI | p-Value | |
| Bacteria | ||||||
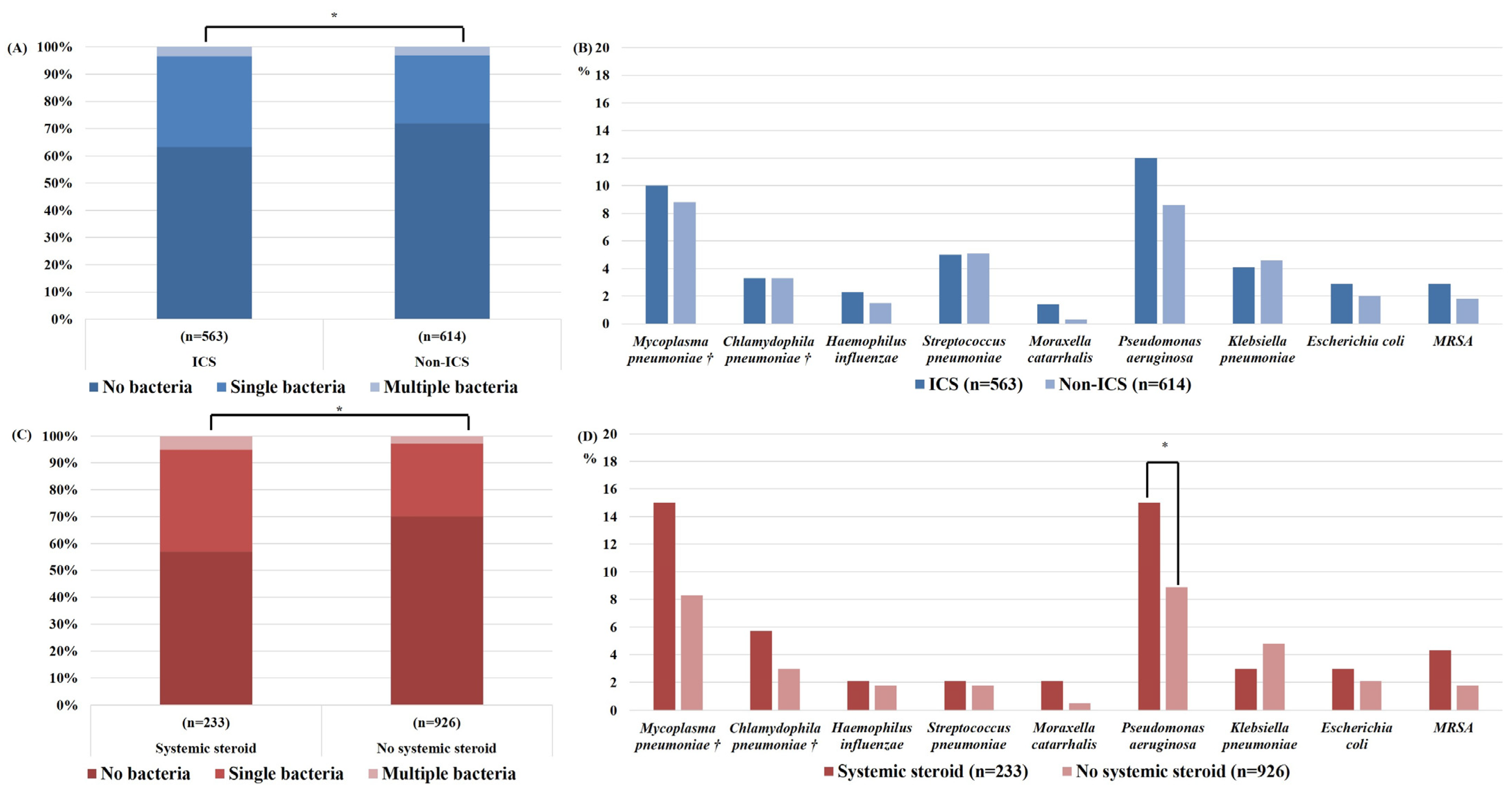
| Mycoplasma pneumoniae† | 1.134 | 0.624–2.061 | 0.680 | 1.876 | 0.952–3.700 | 0.069 |
| Chlamydophila pneumoniae† | 1.154 | 0.407–3.277 | 0.787 | 2.635 | 0.773–8.986 | 0.122 |
| Haemophilus influenzae | 1.395 | 0.563–3.458 | 0.472 | 1.097 | 0.387–3.105 | 0.962 |
| Streptococcus pneumoniae | 0.890 | 0.502–1.577 | 0.689 | 1.728 | 0.922–3.240 | 0.088 |
| Moraxella catarrhalis | 2.873 | 0.582–14.188 | 0.195 | 2.444 | 0.629–9.505 | 0.197 |
| Pseudomonas aeruginosa | 1.238 | 0.796–1.927 | 0.343 | 1.619 | 1.007–2.603 | 0.047 |
| Klebsiella pneumoniae | 0.843 | 0.459–1.550 | 0.583 | 0.698 | 0.303–1.610 | 0.399 |
| Escherichia coli | 1.792 | 0.747–4.302 | 0.192 | 1.420 | 0.567–3.552 | 0.454 |
| MRSA | 1.983 | 0.725–5.426 | 0.182 | 0.825 | 0.263–2.585 | 0.741 |
| Virus | ||||||
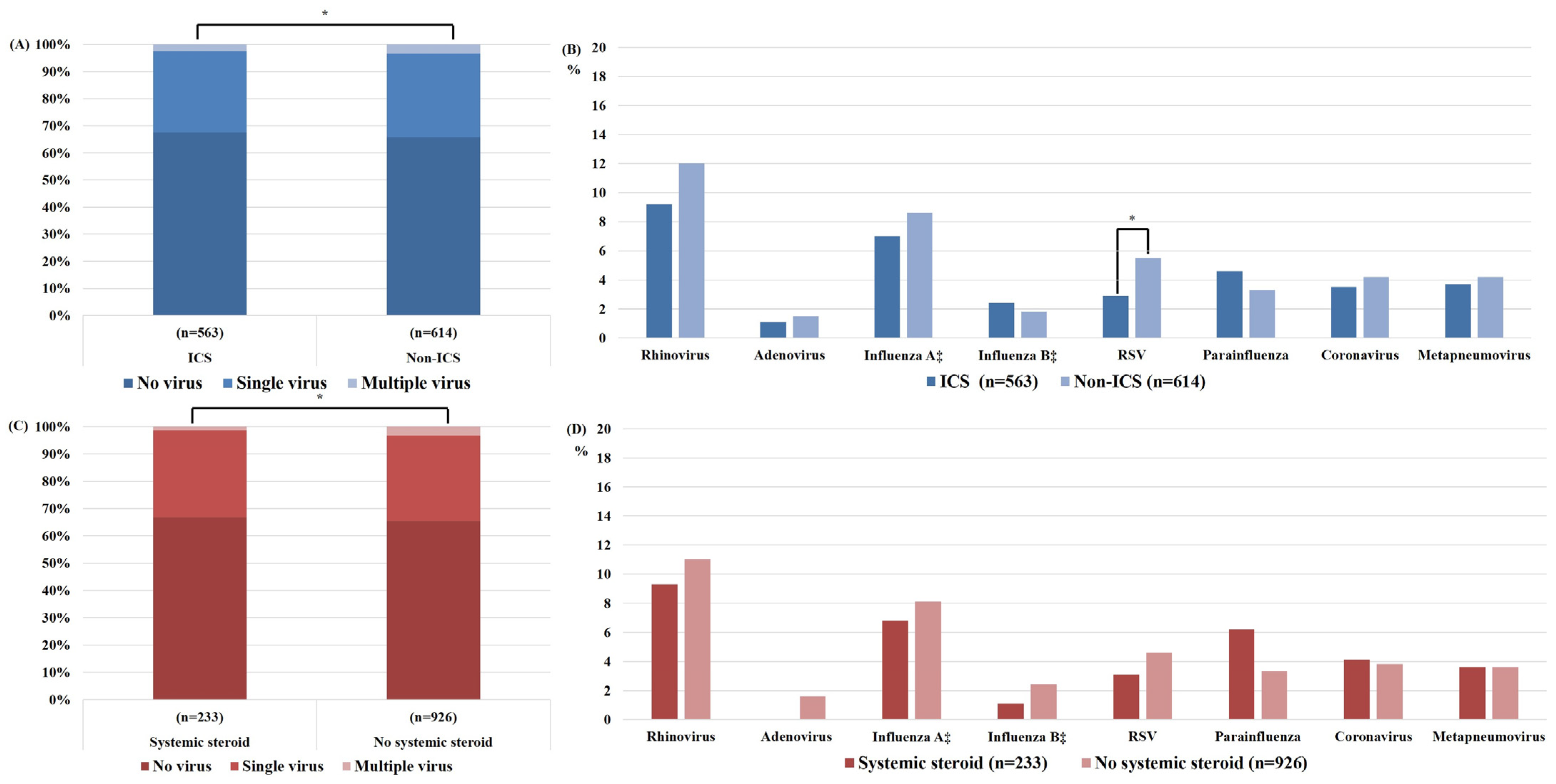
| Rhinovirus | 0.652 | 0.413–1.027 | 0.065 | 0.725 | 0.400–1.312 | 0.288 |
| Adenovirus | 0.616 | 0.191–1.985 | 0.417 | |||
| Influenza A ‡ | 0.855 | 0.483–1.513 | 0.591 | 0.940 | 0.463–1.907 | 0.864 |
| Influenza B ‡ | 1.197 | 0.400–3.579 | 0.748 | 0.625 | 0.135–2.911 | 0.511 |
| RSV | 0.492 | 0.244–0.988 | 0.045 | 0.670 | 0.271–1.655 | 0.386 |
| Parainfluenza | 1.068 | 0.528–2.159 | 0.854 | 1.848 | 0.865–3.948 | 0.113 |
| Coronavirus | 0.942 | 0.452–1.963 | 0.873 | 0.906 | 0.359–2.287 | 0.835 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sim, Y.S.; Lee, J.H.; Lee, E.G.; Choi, J.Y.; Lee, C.-H.; An, T.J.; Park, Y.; Yoon, Y.S.; Park, J.H.; Yoo, K.H. COPD Exacerbation-Related Pathogens and Previous COPD Treatment. J. Clin. Med. 2023, 12, 111. https://doi.org/10.3390/jcm12010111
Sim YS, Lee JH, Lee EG, Choi JY, Lee C-H, An TJ, Park Y, Yoon YS, Park JH, Yoo KH. COPD Exacerbation-Related Pathogens and Previous COPD Treatment. Journal of Clinical Medicine. 2023; 12(1):111. https://doi.org/10.3390/jcm12010111
Chicago/Turabian StyleSim, Yun Su, Jin Hwa Lee, Eung Gu Lee, Joon Young Choi, Chang-Hoon Lee, Tai Joon An, Yeonhee Park, Young Soon Yoon, Joo Hun Park, and Kwang Ha Yoo. 2023. "COPD Exacerbation-Related Pathogens and Previous COPD Treatment" Journal of Clinical Medicine 12, no. 1: 111. https://doi.org/10.3390/jcm12010111