
Chronic Bronchitis Affects Outcomes in Smokers without Chronic Obstructive Pulmonary Disease (COPD)

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Statistical Analysis
3. Results
3.1. Smoking Habits and Prevalence of Chronic Bronchitis
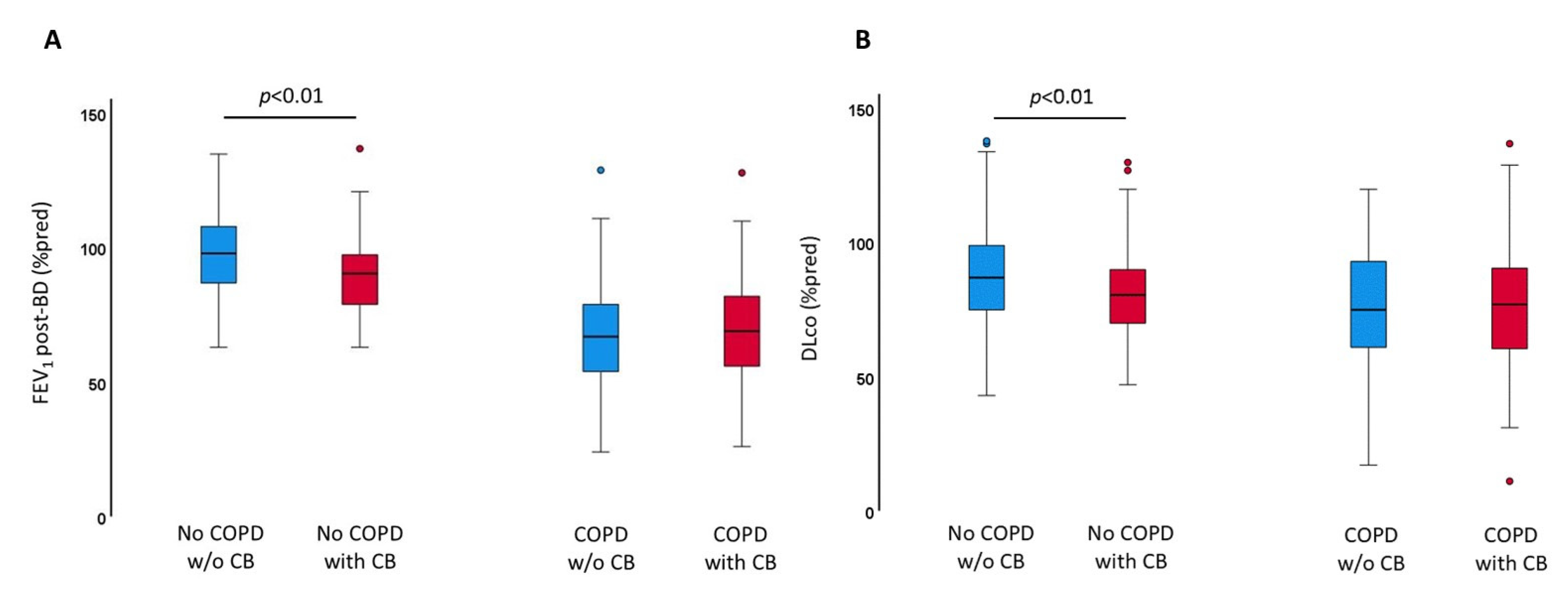
3.2. Impact of Chronic Bronchitis on Lung Function
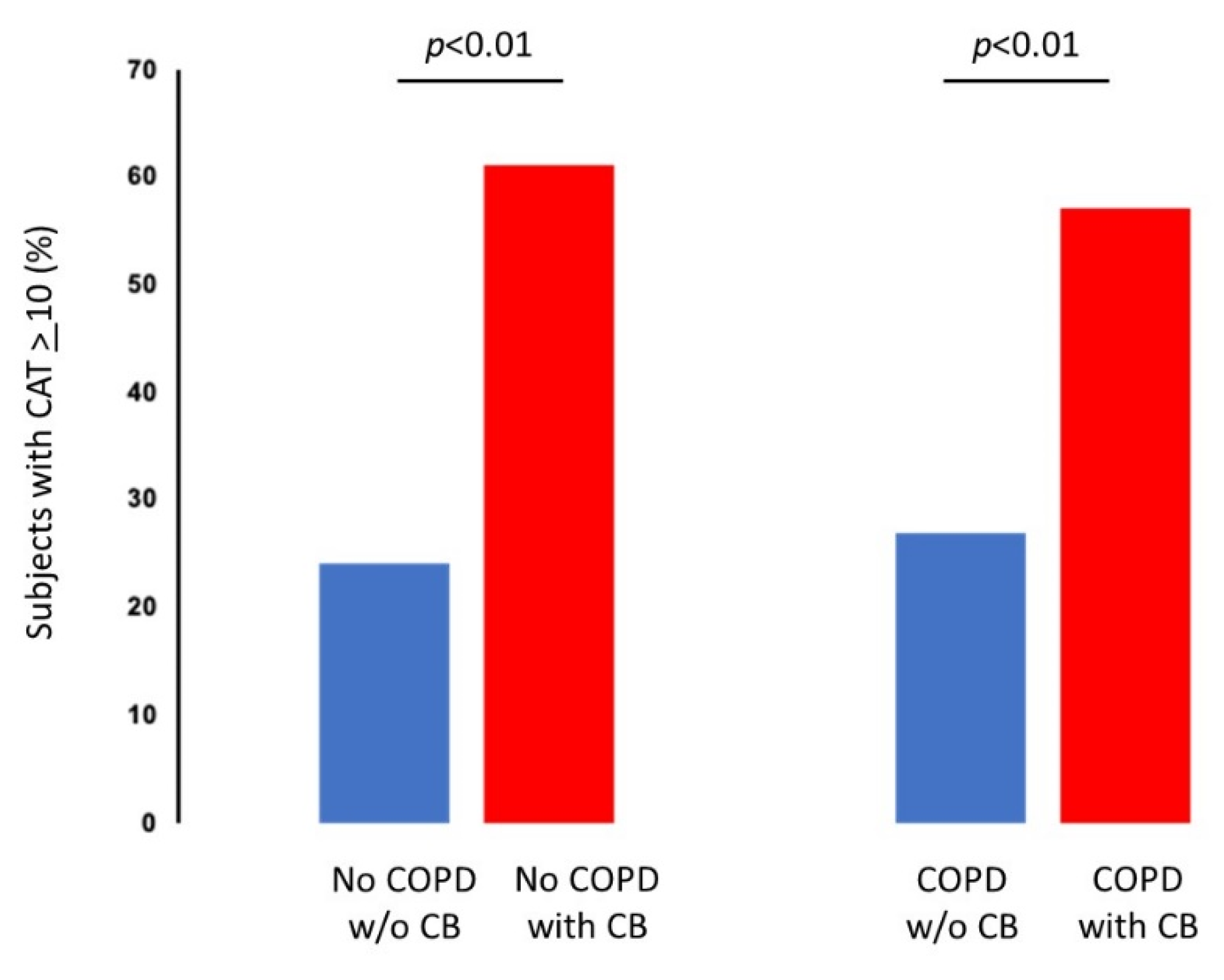
3.3. Impact of Chronic Bronchitis on Clinical Performance
3.4. Impact of Chronic Bronchitis on Exacerbations
3.5. Impact of Chronic Bronchitis on FEV1 Decline
3.6. Impact of Chronic Bronchitis on Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stuart-Harris, C.H.; Crofton, J. Definition and classification of chronic bronchitis for clinical and epidemiological purposes. A report to the Medical Research Council by their Committee on the Aetiology of Chronic Bronchitis. Lancet 1965, 1, 775–779. [Google Scholar]
- Fletcher, C.M. Chronic bronchitis. Its prevalence, nature, and pathogenesis. Am. Rev. Respir. Dis. 1959, 80, 483–494. [Google Scholar]
- Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease, Global Initiative for Chronic Obstructive Lung Disease (GOLD). 2021. Available online: https://goldcopd.org (accessed on 1 January 2021).
- Fletcher, F.E.; Peto, C.; Tinker, R. The Natural History of Chronic Bronchitis and Emphysema; Oxford University Press: Oxford, UK, 1976. [Google Scholar]
- Koo, H.-K.; Park, S.-W.; Park, J.-W.; Choi, H.S.; Kim, T.-H.; Yoon, H.K.; Yoo, K.H.; Jung, K.-S.; Kim, D.K. Chronic cough as a novel phenotype of chronic obstructive pulmonary disease. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 1793–1801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, W.J.; Yim, J.-J.; Kim, D.K.; Lee, M.G.; Fuhlbrigge, A.L.; Sliwinski, P.; Hawrylkiewicz, I.; Wan, E.S.; Cho, M.H.; Silverman, E.K. Severe COPD cases from Korea, Poland, and USA have substantial differences in respiratory symptoms and other respiratory illnesses. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 3415–3423. [Google Scholar] [CrossRef] [PubMed]
- Lu, M.; Yao, W.; Zhong, N.; Zhou, Y.; Wang, C.; Chen, P.; Kang, J.; Huang, S.; Chen, B.; Wang, C.; et al. Chronic obstructive pulmonary disease in the absence of chronic bronchitis in China. Respirology 2010, 15, 1072–1078. [Google Scholar] [CrossRef]
- Pelkonen, M.; Notkola, I.-L.; Nissinen, A.; Tukiainen, H.; Koskela, H. Thirty-Year Cumulative Incidence of Chronic Bronchitis and COPD in Relation to 30-Year Pulmonary Function and 40-Year Mortality. Chest 2006, 130, 1129–1137. [Google Scholar] [CrossRef]
- Kim, V.; Criner, G.J. Chronic Bronchitis and Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2013, 187, 228–237. [Google Scholar] [CrossRef] [Green Version]
- Mejza, F.; Gnatiuc, L.; Buist, A.S.; Vollmer, W.M.; Lamprecht, B.; Obaseki, D.O.; Nastalek, P.; Nizankowska-Mogilnicka, E.; Burney, P.G.J. BOLD collaborators; BOLD study collaborators. Prevalence and burden of chronic bronchitis symptoms: Results from the BOLD study. Eur. Respir. J. 2017, 50, 1700621. [Google Scholar] [CrossRef] [Green Version]
- Mejza, F.; Nastałek, P.; Doniec, Z.; Skucha, W. Symptoms of chronic bronchitis in individuals without chronic obstructive pulmonary disease: Prevalence, burden, and risk factors in southern Poland. Pol. Arch. Intern. Med. 2018, 128, 677–684. [Google Scholar] [CrossRef]
- Wang, G.; Hallberg, J.; Um Bergström, P.; Janson, C.; Pershagen, G.; Gruzieva, O.; van Hage, M.; Georgelis, A.; Bergström, A.; Kull, I.; et al. Assessment of chronic bronchitis and risk factors in young adults: Results from BAMSE. Eur. Respir. J. 2021, 57, 2002120. [Google Scholar] [CrossRef]
- de Oca, M.M.; Halbert, R.J.; Lopez, M.V.; Perez-Padilla, R.; Tálamo, C.; Moreno, D.; Muiño, A.; Jardim, J.R.; Valdivia, G.; Pertuzé, J.; et al. The chronic bronchitis phenotype in subjects with and without COPD: The PLATINO study. Eur. Respir. J. 2012, 40, 28–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vestbo, J.; Prescott, E.; Lange, P. Association of chronic mucus hypersecretion with FEV1 decline and chronic obstructive pulmonary disease morbidity. Am. J. Respir. Crit. Care Med. 1996, 153, 1530–1535. [Google Scholar] [CrossRef] [PubMed]
- de Marco, R.; Accordini, S.; Cerveri, I.; Corsico, A.; Antó, J.M.; Künzli, N.; Janson, C.; Sunyer, J.; Jarvis, D.; Chinn, S.; et al. Incidence of chronic obstructive pulmonary disease in a cohort of young adults according to the presence of chronic cough and phlegm. Am. J. Respir. Crit. Care Med. 2007, 175, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Communitè Europeenne du Carbon e de l’Acier. Aide-Memoire of Spirographic Practice for Examining Ventilatory Function, 2nd ed.; Industrial Health and Medicine: Luxemburg, 1971. [Google Scholar]
- Semenzato, U.; Biondini, D.; Bazzan, E.; Tiné, M.; Balestro, E.; Buldini, B.; Carizzo, S.J.; Cubero, P.; Marin-Oto, M.; Casara, A.; et al. Low-Blood Lymphocyte Number and Lymphocyte Decline as Key Factors in COPD Outcomes: A Longitudinal Cohort Study. Respiration 2021, 100, 618–630. [Google Scholar] [CrossRef] [PubMed]
- Bazzan, E.; Semenzato, U.; Turato, G.; Biondini, D.; Cubero, P.; Marin-Oto, M.; Forner, M.; Tinè, M.; Casara, A.; Baraldo, S.; et al. Symptomatic smokers without COPD have physiological changes heralding the development of COPD. ERJ Open Res. 2022, 8, 00202–2022. [Google Scholar] [CrossRef]
- Lindberg, A.; Sawalha, S.; Hedman, L.; Larsson, L.-G.; Lundbäck, B.; Rönmark, E. Subjects with COPD and productive cough have an increased risk for exacerbations and death. Respir. Med. 2015, 109, 88–95. [Google Scholar] [CrossRef] [Green Version]
- Sator, L.; Horner, A.; Studnicka, M.; Lamprecht, B.; Kaiser, B.; McBurnie, M.A.; Buist, A.S.; Gnatiuc, L.; Mannino, D.M.; Janson, C.; et al. BOLD Collaborative Research Group. Overdiagnosis of COPD in Subjects with Unobstructed Spirometry: A BOLD Analysis. Chest 2019, 156, 277–288. [Google Scholar] [CrossRef]
- Vestbo, J.; Lange, P. Can GOLD Stage 0 Provide Information of Prognostic Value in Chronic Obstructive Pulmonary Disease? Am. J. Respir. Crit. Care Med. 2002, 166, 329–332. [Google Scholar] [CrossRef]
- Martinez, C.H.; Kim, V.; Chen, Y.; Kazerooni, E.A.; Murray, S.; Criner, G.J.; Curtis, J.L.; Regan, E.A.; Wan, E.; Hersh, C.P.; et al. The clinical impact of non-obstructive chronic bronchitis in current and former smokers. Respir. Med. 2014, 108, 491–499. [Google Scholar] [CrossRef] [Green Version]
- Kim, V.; Han, M.K.; Vance, G.B.; Make, B.J.; Newell, J.D.; Hokanson, J.E.; Hersh, C.P.; Stinson, D.; Silverman, E.K.; Criner, G.J. COPDGene Investigators. The Chronic Bronchitic Phenotype of COPD: An Analysis of the COPDGene Study. Chest 2011, 140, 626–633. [Google Scholar] [CrossRef] [Green Version]
- Phillips, D.B.; Elbehairy, A.F.; James, M.D.; Vincent, S.G.; Milne, K.M.; De-Torres, J.P.; Neder, J.A.; Kirby, M.; Jensen, D.; Stickland, M.K.; et al. Impaired Ventilatory Efficiency, Dyspnea, and Exercise Intolerance in Chronic Obstructive Pulmonary Disease: Results from the CanCOLD Study. Am. J. Respir. Crit. Care Med. 2022, 205, 1391–1402. [Google Scholar] [CrossRef]
- Meek, P.M.; Petersen, H.; Washko, G.R.; Diaz, A.A.; Klm, V.; Sood, A.; Tesfaigzi, Y. Chronic Bronchitis Is Associated with Worse Symptoms and Quality of Life Than Chronic Airflow Obstruction. Chest 2015, 148, 408–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woodruff, P.G.; Barr, R.G.; Bleecker, E.; Christenson, S.A.; Couper, D.; Curtis, J.L.; Gouskova, N.A.; Hansel, N.N.; Hoffman, E.A.; Kanner, R.E.; et al. Spiromics Research Group. Clinical Significance of Symptoms in Smokers with Preserved Pulmonary Function. N. Engl. J. Med. 2016, 374, 1811–1821. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.C.; Bourbeau, J.; Hernandez, P.; Chapman, K.R.; Cowie, R.; FitzGerald, J.M.; Marciniuk, D.D.; Maltais, F.; Buist, A.S.; O’Donnell, D.E.; et al. CanCOLD Collaborative Research Group. Exacerbation-like respiratory symptoms in individuals without chronic obstructive pulmonary disease: Results from a population-based study. Thorax 2014, 69, 709–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chai, C.-S.; Liam, C.-K.; Pang, Y.-K.; Ng, D.L.-C.; Tan, S.-B.; Wong, T.-S.; Sia, J.-E. Clinical phenotypes of COPD and health-related quality of life: A cross-sectional study. Int. J. Chronic Obstr. Pulm. Dis. 2019, 14, 565–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agusti, A.; Calverley, P.M.; Celli, B.; Coxson, H.O.; Edwards, L.D.; Lomas, D.A.; MacNee, W.; Miller, B.E.; Rennard, S.; Silverman, E.K.; et al. Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) investigators. Characterisation of COPD heterogeneity in the ECLIPSE cohort. Respir. Res. 2010, 11, 122. [Google Scholar] [CrossRef] [PubMed]
- Burgel, P.-R.; Nesme-Meyer, P.; Chanez, P.; Caillaud, D.; Carré, P.; Perez, T.; Roche, N. Initiatives Bronchopneumopathie Chronique Obstructive (BPCO) Scientific Committee. Cough and Sputum Production Are Associated with Frequent Exacerbations and Hospitalizations in COPD Subjects. Chest 2009, 135, 975–982. [Google Scholar] [CrossRef]
- Lahousse, L.; Seys, L.J.M.; Joos, G.F.; Franco, O.H.; Stricker, B.H.; Brusselle, G.G. Epidemiology and impact of chronic bronchitis in chronic obstructive pulmonary disease. Eur. Respir. J. 2017, 50, 1602470. [Google Scholar] [CrossRef]
- Miravitlles, M.; Guerrero, T.; Mayordomo, C.; Sánchez-Agudo, L.; Nicolau, F.; Segú, J.L. The EOLO Study Group. Factors Associated with Increased Risk of Exacerbation and Hospital Admission in a Cohort of Ambulatory COPD Patients: A Multiple Logistic Regression Analysis. Respiration 2000, 67, 495–501. [Google Scholar] [CrossRef]
- Neder, J.A.; de-Torres, J.P.; O’Donnell, D.E. Exposing Pre-COPD: When Physiology Matters! Am. J. Respir. Crit. Care Med. 2021, 204, 110–111. [Google Scholar] [CrossRef]
- Button, B.; Goodell, H.P.; Atieh, E.; Chen, Y.-C.; Williams, R.; Shenoy, S.; Lackey, E.; Shenkute, N.T.; Cai, L.-H.; Dennis, R.G.; et al. Roles of mucus adhesion and cohesion in cough clearance. Proc. Natl. Acad. Sci. USA 2018, 115, 12501–12506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elbehairy, A.F.; Guenette, J.A.; Faisal, A.; Ciavaglia, C.E.; Webb, K.A.; Jensen, D.; Ramsook, A.H.; Neder, J.A.; O’Donnell, D.E. Canadian Respiratory Research Network. Mechanisms of exertional dyspnoea in symptomatic smokers without COPD. Eur. Respir. J. 2016, 48, 694–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbosa, G.W.; Neder, J.A.; Utida, K.; O’Donnell, D.E.; Müller, P.D.T. Impaired exercise ventilatory efficiency in smokers with low transfer factor but normal spirometry. Eur. Respir. J. 2017, 49, 1602511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arshad, S.H.; Kurukulaaratchy, R.; Zhang, H.; Hodgekiss, C.; Karmaus, W.; Holloway, J.W.; Roberts, G. Assessing small airway function for early detection of lung function impairment. Eur. Respir. J. 2020, 56, 2001946. [Google Scholar] [CrossRef]
- Guerra, S.; Sherrill, D.L.; Venker, C.; Ceccato, C.M.; Halonen, M.; Martinez, F.D. Chronic bronchitis before age 50 years predicts incident airflow limitation and mortality risk. Thorax 2009, 64, 894–900. [Google Scholar] [CrossRef] [Green Version]
- Allinson, J.P.; Hardy, R.; Donaldson, G.C.; Shaheen, S.O.; Kuh, D.; Wedzicha, J.A. The Presence of Chronic Mucus Hypersecretion across Adult Life in Relation to Chronic Obstructive Pulmonary Disease Development. Am. J. Respir. Crit. Care Med. 2016, 193, 662–672. [Google Scholar] [CrossRef] [Green Version]
- Fortis, S.; Shannon, Z.K.; Garcia, C.J.; Guillamet, R.V.; Aloe, A.M.; Schweizer, M.L.; Kim, V.; Nair, R. Association of Nonobstructive Chronic Bronchitis with All-Cause Mortality: A Systematic Literature Review and Meta-analysis. Chest 2022, 162, 92–100. [Google Scholar] [CrossRef]
- Balte, P.P.; Chaves, P.H.; Couper, D.J.; Enright, P.; Jacobs, D.R.; Kalhan, R.; Kronmal, R.A.; Loehr, L.R.; London, S.; Newman, A.B.; et al. Association of Nonobstructive Chronic Bronchitis with Respiratory Health Outcomes in Adults. JAMA Intern. Med. 2020, 180, 676–686. [Google Scholar] [CrossRef]
- Kim, V.; Zhao, H.; Boriek, A.M.; Anzueto, A.; Soler, X.; Bhatt, S.P.; Rennard, S.I.; Wise, R.; Comellas, A.; Ramsdell, J.W.; et al. Persistent and Newly Developed Chronic Bronchitis Are Associated with Worse Outcomes in Chronic Obstructive Pulmonary Disease. Ann. Am. Thorac. Soc. 2016, 13, 1016–1025. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NoCOPD all Population n = 209 | NoCOPD w/o CB n = 153 (73%) | NoCOPD with CB n = 56 (27%) | p | |
|---|---|---|---|---|
| Age (years) | 52 ± 11 | 51 ± 11 | 53 ± 12 | 0.43 |
| Males n (%) | 147 (70%) | 107 (70%) | 40 (71%) | 0.63 |
| Smoking history (pack years) | 35 ± 19 | 34 ± 18 | 38 ± 21 | 0.21 |
| Active smokers n (%) | 108 (51%) | 76 (49%) | 32 (57%) | 0.31 |
| FEV1 post-bd (%pred.) | 95 ± 15 | 97 ± 15 | 90 ± 14 | <0.01 |
| post-bd FEV1/FVC (%) | 78 ± 5 | 79 ± 5 | 78 ± 5 | 0.10 |
| Decline of FEV1 per year (ml/year) | 33 ± 37 | 32 ± 34 | 36 ± 44 | 0.47 |
| MEF 25–75 post-bd (% pred.) | 75 ± 21 | 77 ± 21 | 70 ± 21 | <0.01 |
| DLco (% pred) | 80 ± 21 | 87 ± 17 | 81 ± 28 | 0.01 |
| Subjects with mMRC ≥ 2, n (%) | 71 (34%) | 41 (27%) | 30 (54%) | <0.01 |
| Subjects with CAT ≥ 10, n (%) | 70 (33%) | 36 (24%) | 34 (61%) | <0.01 |
| Distance at 6-min walking test (m) | 481 ± 114 | 490 ± 111 | 452 ± 120 | 0.05 |
| Subjects with at least one exacerbation, n (%) | 73 (35%) | 46 (30%) | 27 (48%) | 0.01 |
| Number of total exacerbations/year | 0.49 ± 0.007 | 0.38 ± 0.002 | 0.79 ± 0.013 | 0.007 |
| Subjects who develop COPD at follow-up n (%) | 30 (14%) | 19 (12%) | 11 (20%) | 0.1 |
| COPD all Population n = 302 | COPD w/o CB n = 165 (55%) | COPD with CB n = 137 (45%) | p | |
|---|---|---|---|---|
| Age (years) | 62 ± 8 | 61 ± 8 | 63 ± 8 | 0.08 |
| Males n (%) | 276 (91%) | 150 (90%) | 126 (91%) | 0.53 |
| Smoking history (pack years) | 49 ± 25 | 50 ± 26 | 49 ± 25 | 0.79 |
| Active smokers n (%) | 103 (34%) | 53 (32%) | 50 (36%) | 0.4 |
| FEV1 post-bd (% pred.) | 68 ± 19 | 67 ± 19 | 69 ± 20 | 0.38 |
| post-bd FEV1/FVC (%) | 54 ± 11 | 54 ± 11 | 54 ± 12 | 0.73 |
| GOLD 1, n (%) | 81 (27%) | 41 (25%) | 40 (29%) | 0.65 |
| GOLD 2, n (%) | 169 (56%) | 96 (58%) | 73 (53%) | |
| GOLD 3–4, n (%) | 53 (17%) | 28 (17%) | 24 (18%) | |
| Decline of FEV1 per year (mL/year) | 31 ± 51 | 22 ± 53 | 41 ± 48 | <0.01 |
| MEF 25–75 post-bd (% pred.) | 27 ± 13 | 27 ± 13 | 28 ± 14 | 0.40 |
| DLco (% pred) | 80 ± 21 | 76 ± 21 | 77 ± 22 | 0.32 |
| Subjects with mMRC ≥ 2, n (%) | 144 (47%) | 68 (41%) | 76 (55%) | <0.01 |
| Subjects with CAT ≥ 10, n (%) | 123 (41%) | 45 (27%) | 78 (57%) | <0.01 |
| Distance at 6 min walking test (m) | 376 ± 109 | 383 ± 95 | 367 ± 123 | 0.55 |
| Subjects with at least one exacerbation, n (%) | 162 (53%) | 84 (51%) | 78 (57%) | 0.16 |
| Number of total exacerbations/year | 1.00 ± 0.007 | 0.84 ± 0.005 | 1.19 ± 0.008 | 0.09 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casara, A.; Turato, G.; Marin-Oto, M.; Semenzato, U.; Biondini, D.; Tinè, M.; Bernardinello, N.; Cocconcelli, E.; Cubero, P.; Balestro, E.; et al. Chronic Bronchitis Affects Outcomes in Smokers without Chronic Obstructive Pulmonary Disease (COPD). J. Clin. Med. 2022, 11, 4886. https://doi.org/10.3390/jcm11164886
Casara A, Turato G, Marin-Oto M, Semenzato U, Biondini D, Tinè M, Bernardinello N, Cocconcelli E, Cubero P, Balestro E, et al. Chronic Bronchitis Affects Outcomes in Smokers without Chronic Obstructive Pulmonary Disease (COPD). Journal of Clinical Medicine. 2022; 11(16):4886. https://doi.org/10.3390/jcm11164886
Chicago/Turabian StyleCasara, Alvise, Graziella Turato, Marta Marin-Oto, Umberto Semenzato, Davide Biondini, Mariaenrica Tinè, Nicol Bernardinello, Elisabetta Cocconcelli, Pablo Cubero, Elisabetta Balestro, and et al. 2022. "Chronic Bronchitis Affects Outcomes in Smokers without Chronic Obstructive Pulmonary Disease (COPD)" Journal of Clinical Medicine 11, no. 16: 4886. https://doi.org/10.3390/jcm11164886