
Relationship of Different Anthropometric Indices with Vascular Ageing in an Adult Population without Cardiovascular Disease—EVA Study

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Variables and Measurement Instruments
2.3. Measurement of Arterial Stiffness
2.4. Vascular Ageing Measurement
2.5. Anthropometric Indices Measurement
- –
- Estimators of obesity and total body fat distribution:
- –
- Estimators of abdominal or visceral fat:
2.6. Ethical Considerations
2.7. Statistical Analysis
3. Results
3.1. Characteristics of the Participants and Vascular Ageing
3.2. Values of the Anthropometric Indices According to the Degree of Vascular Ageing
3.3. Relationship between the Anthropometric Parameters and cf-PWV: Multiple Regression Analysis
3.4. Association between the Anthropometric Parameters with Vascular Ageing: Multinomial Logistic Regression
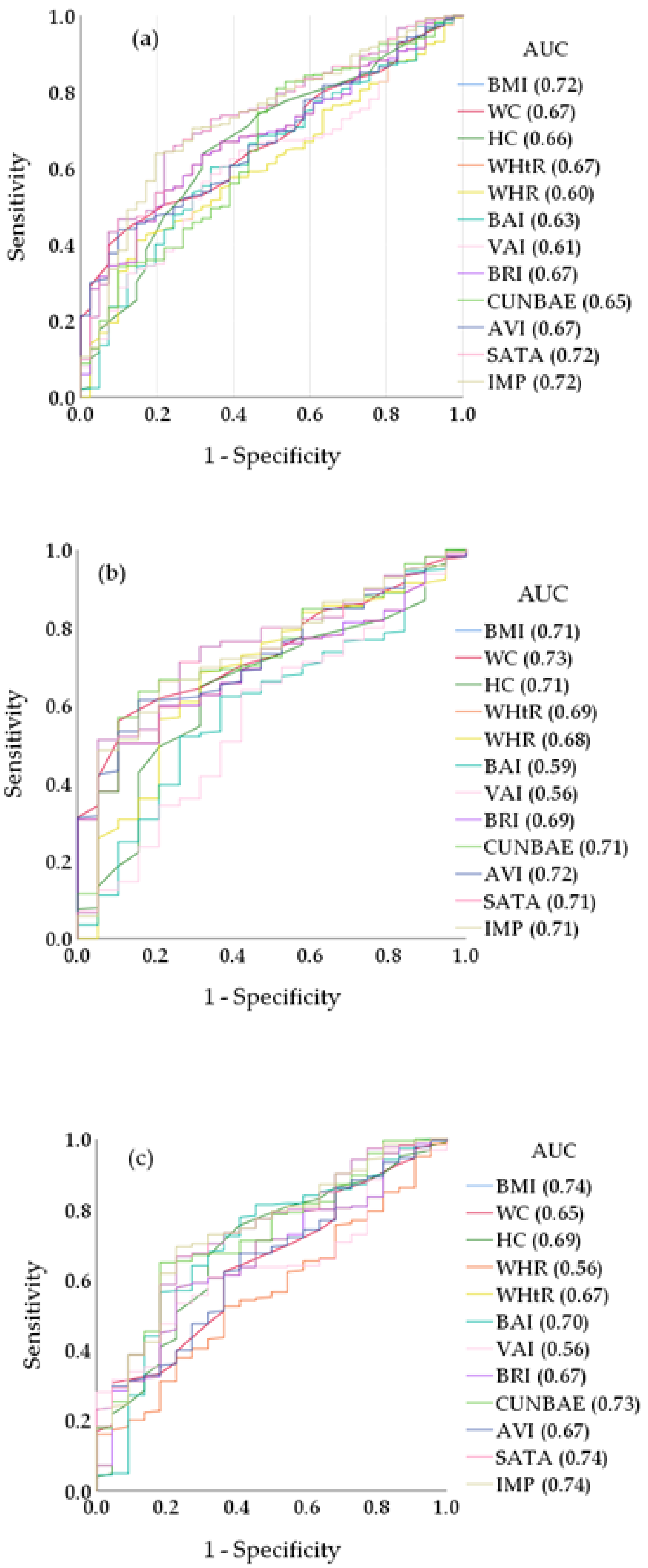
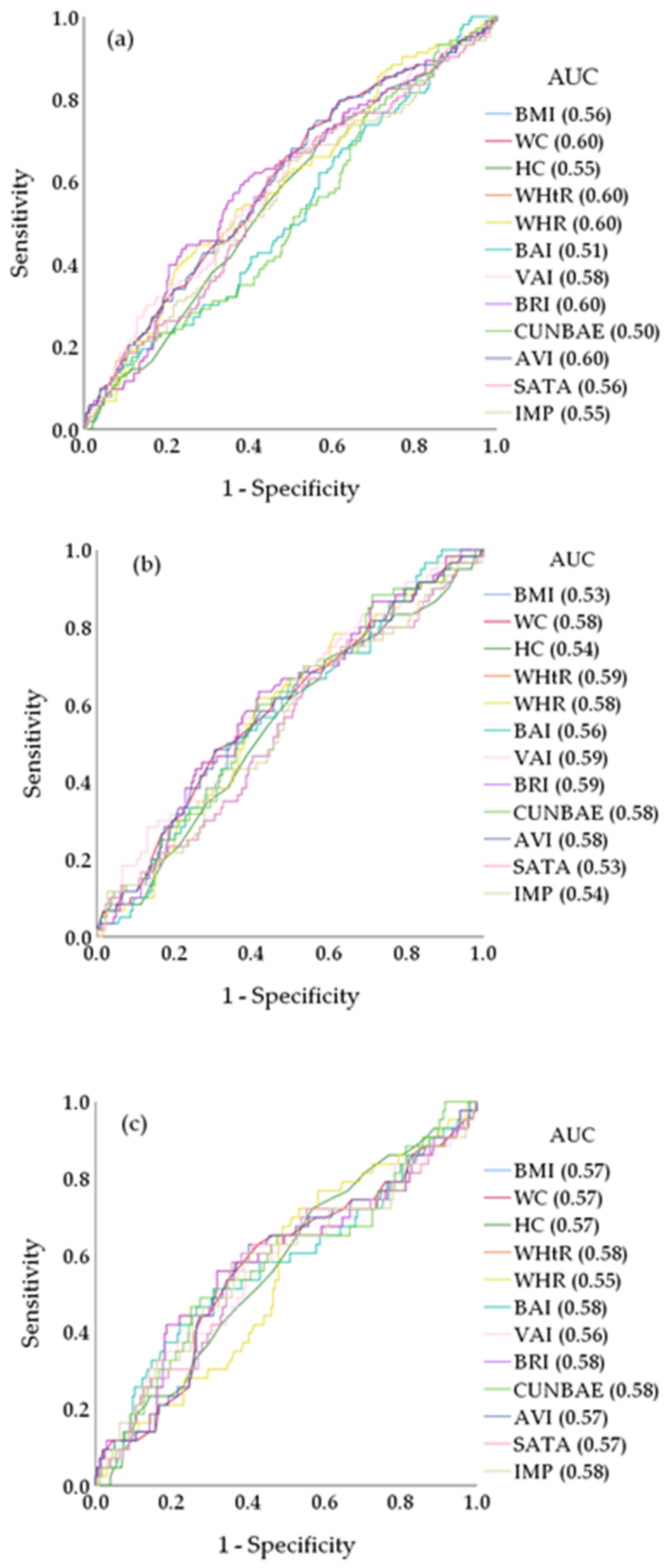
3.5. Comparison of the Anthropometric Indices for the Diagnosis of HVA and EVA
4. Discussion
5. Conclusions
6. Limits
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nevill, A.M.; Stewart, A.D.; Olds, T.; Holder, R. Relationship between adiposity and body size reveals limitations of BMI. Am. J. Phys. Anthropol. 2006, 129, 151–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, A.V.; Hildebrand, J.S.; Gapstur, S.M. Body mass index and all-cause mortality in a large prospective cohort of white and black U.S. Adults. PLoS ONE 2014, 9, e109153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishida, C.; Ko, G.T.; Kumanyika, S. Body fat distribution and noncommunicable diseases in populations: Overview of the 2008 WHO Expert Consultation on Waist Circumference and Waist-Hip Ratio. Eur. J. Clin. Nutr. 2010, 64, 2–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashwell, M.; Gunn, P.; Gibson, S. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: Systematic review and meta-analysis. Obes. Rev. 2012, 13, 275–286. [Google Scholar] [CrossRef]
- Bosello, O.; Donataccio, M.P.; Cuzzolaro, M. Obesity or obesities? Controversies on the association between body mass index and premature mortality. Eat Weight Disord. 2016, 21, 165–174. [Google Scholar] [CrossRef]
- Guerrero-Romero, F.; Rodríguez-Morán, M. Abdominal volume index. An anthropometry-based index for estimation of obesity is strongly related to impaired glucose tolerance and type 2 diabetes mellitus. Arch. Med. Res. 2003, 34, 428–432. [Google Scholar] [CrossRef]
- Brambilla, P.; Bedogni, G.; Moreno, L.A.; Goran, M.I.; Gutin, B.; Fox, K.R.; Peters, D.M.; Barbeau, P.; De Simone, M.; Pietrobelli, A. Crossvalidation of anthropometry against magnetic resonance imaging for the assessment of visceral and subcutaneous adipose tissue in children. Int. J. Obes. 2006, 30, 23–30. [Google Scholar] [CrossRef] [Green Version]
- Amato, M.C.; Giordano, C.; Galia, M.; Criscimanna, A.; Vitabile, S.; Midiri, M.; Galluzzo, A. Visceral Adiposity Index: A reliable indicator of visceral fat function associated with cardiometabolic risk. Diabetes Care 2010, 33, 920–922. [Google Scholar] [CrossRef] [Green Version]
- Bergman, R.N.; Stefanovski, D.; Buchanan, T.A.; Sumner, A.E.; Reynolds, J.C.; Sebring, N.G.; Xiang, A.H.; Watanabe, R.M. A better index of body adiposity. Obesity 2011, 19, 1083–1089. [Google Scholar] [CrossRef]
- Gómez-Ambrosi, J.; Silva, C.; Catalán, V.; Rodríguez, A.; Galofré, J.C.; Escalada, J.; Valentí, V.; Rotellar, F.; Romero, S.; Ramírez, B.; et al. Clinical usefulness of a new equation for estimating body fat. Diabetes Care 2012, 35, 383–388. [Google Scholar] [CrossRef] [Green Version]
- Krakauer, N.Y.; Krakauer, J.C. A new body shape index predicts mortality hazard independently of body mass index. PLoS ONE 2012, 7, e39504. [Google Scholar] [CrossRef]
- Thomas, D.M.; Bredlau, C.; Bosy-Westphal, A.; Mueller, M.; Shen, W.; Gallagher, D.; Maeda, Y.; McDougall, A.; Peterson, C.M.; Ravussin, E.; et al. Relationships between body roundness with body fat and visceral adipose tissue emerging from a new geometrical model. Obesity 2013, 21, 2264–2271. [Google Scholar] [CrossRef] [Green Version]
- Laurent, S.; Boutouyrie, P.; Cunha, P.G.; Lacolley, P.; Nilsson, P.M. Concept of Extremes in Vascular Aging. Hypertension 2019, 74, 218–228. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J. Hypertens. 2018, 36, 1953–2041. [Google Scholar] [CrossRef] [Green Version]
- Nowak, K.L.; Rossman, M.J.; Chonchol, M.; Seals, D.R. Strategies for Achieving Healthy Vascular Aging. Hypertension 2018, 71, 389–402. [Google Scholar] [CrossRef] [Green Version]
- Matjuda, E.N.; Engwa, G.A.; Anye, S.N.C.; Nkeh-Chungag, B.N.; Goswami, N. Cardiovascular Risk Factors and Their Relationship with Vascular Dysfunction in South African Children of African Ancestry. J. Clin. Med. 2021, 10, 354. [Google Scholar] [CrossRef]
- Nilsson, P.M.; Laurent, S.; Cunha, P.G.; Olsen, M.H.; Rietzschel, E.; Franco, O.H.; Ryliškytė, L.; Strazhesko, I.; Vlachopoulos, C.; Chen, C.H.; et al. Characteristics of healthy vascular ageing in pooled population-based cohort studies: The global Metabolic syndrome and Artery REsearch Consortium. J. Hypertens. 2018, 36, 2340–2349. [Google Scholar] [CrossRef]
- Ji, H.; Teliewubai, J.; Lu, Y.; Xiong, J.; Yu, S.; Chi, C.; Li, J.; Blacher, J.; Zhang, Y.; Xu, Y. Vascular aging and preclinical target organ damage in community-dwelling elderly: The Northern Shanghai Study. J. Hypertens. 2018, 36, 1391–1398. [Google Scholar] [CrossRef]
- Botto, F.; Obregon, S.; Rubinstein, F.; Scuteri, A.; Nilsson, P.M.; Kotliar, C. Frequency of early vascular aging and associated risk factors among an adult population in Latin America: The OPTIMO study. J. Hum. Hypertens. 2018, 32, 219–227. [Google Scholar] [CrossRef]
- Niiranen, T.J.; Lyass, A.; Larson, M.G.; Hamburg, N.M.; Benjamin, E.J.; Mitchell, G.F.; Vasan, R.S. Prevalence, Correlates, and Prognosis of Healthy Vascular Aging in a Western Community-Dwelling Cohort: The Framingham Heart Study. Hypertension 2017, 70, 267–274. [Google Scholar] [CrossRef]
- Cunha, P.G.; Cotter, J.; Oliveira, P.; Vila, I.; Boutouyrie, P.; Laurent, S.; Nilsson, P.M.; Scuteri, A.; Sousa, N. Pulse wave velocity distribution in a cohort study: From arterial stiffness to early vascular aging. J. Hypertens. 2015, 33, 1438–1445. [Google Scholar] [CrossRef] [Green Version]
- Gomez-Marcos, M.A.; Martinez-Salgado, C.; Gonzalez-Sarmiento, R.; Hernandez-Rivas, J.M.; Sanchez-Fernandez, P.L.; Recio-Rodriguez, J.I.; Rodriguez-Sanchez, E.; García-Ortiz, L. Association between different risk factors and vascular accelerated ageing (EVA study): Study protocol for a cross-sectional, descriptive observational study. BMJ Open 2016, 6, e011031. [Google Scholar] [CrossRef]
- Gómez-Sánchez, M.; Patino-Alonso, M.C.; Gómez-Sánchez, L.; Recio-Rodríguez, J.I.; Rodríguez-Sánchez, E.; Maderuelo-Fernández, J.A.; García-Ortiz, L.; Gómez-Marcos, M.A. Reference values of arterial stiffness parameters and their association with cardiovascular risk factors in the Spanish population. The EVA Study. Rev. Esp. Cardiol. 2020, 73, 43–52. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 Practice Guidelines for the management of arterial hypertension of the European Society of Hypertension and the European Society of Cardiology: ESH/ESC Task Force for the Management of Arterial Hypertension. J. Hypertens. 2018, 36, 2284–2309. [Google Scholar] [CrossRef] [Green Version]
- Van Bortel, L.M.; Laurent, S.; Boutouyrie, P.; Chowienczyk, P.; Cruickshank, J.K.; De Backer, T.; Filipovsky, J.; Huybrechts, S.; Mattace-Raso, F.U.; Protogerou, A.D.; et al. Expert consensus document on the measurement of aortic stiffness in daily practice using carotid-femoral pulse wave velocity. J. Hypertens. 2012, 30, 445–448. [Google Scholar] [CrossRef] [Green Version]
- Gomez-Sanchez, M.; Gomez-Sanchez, L.; Patino-Alonso, M.C.; Cunha, P.G.; Recio-Rodriguez, J.I.; Alonso-Dominguez, R.; Sanchez-Aguadero, N.; Rodriguez-Sanchez, E.; Maderuelo-Fernandez, J.A.; Garcia-Ortiz, L.; et al. Vascular aging and its relationship with lifestyles and other risk factors in the general Spanish population: Early Vascular Ageing Study. J. Hypertens. 2020, 38, 1110–1122. [Google Scholar] [CrossRef]
- Salas-Salvadó, J.; Rubio, M.A.; Barbany, M.; Moreno, B. [SEEDO 2007 Consensus for the evaluation of overweight and obesity and the establishment of therapeutic intervention criteria]. Med. Clin. 2007, 128, 184–196. [Google Scholar] [CrossRef]
- Cabañas Armesilla, M.D. Antropometría e Índices de Salud; Sociedad Española de Dietética y Ciencias de la Alimentación: Madrid, Spain, 2008; Available online: https://docplayer.es/2473040-Antropometria-e-indices-de-salud.html (accessed on 10 January 2022).
- World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [CrossRef] [Green Version]
- Merz, A.A.; Cheng, S. Sex differences in cardiovascular ageing. Heart 2016, 102, 825–831. [Google Scholar] [CrossRef]
- Coutinho, T. Arterial stiffness and its clinical implications in women. Can. J. Cardiol. 2014, 30, 756–764. [Google Scholar] [CrossRef]
- Anoop, S.; Misra, A.; Bhardwaj, S.; Gulati, S. High body fat and low muscle mass are associated with increased arterial stiffness in Asian Indians in North India. J. Diabetes Complicat. 2014, 6, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Q.; Hu, M.J.; Cui, Y.J.; Liang, L.; Zhou, M.M.; Yang, Y.W.; Huang, F. Carotid-Femoral Pulse Wave Velocity in the Prediction of Cardiovascular Events and Mortality: An Updated Systematic Review and Meta-Analysis. Angiology 2018, 69, 617–629. [Google Scholar] [CrossRef] [PubMed]
- Meani, P.; Maloberti, A.; Sormani, P.; Colombo, G.; Giupponi, L.; Stucchi, M.; Varrenti, M.; Vallerio, P.; Facchetti, R.; Grassi, G.; et al. Determinants of carotid-femoral pulse wave velocity progression in hypertensive patients over a 3.7 years follow-up. Blood Press 2018, 27, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Terentes-Printzios, D.; Vlachopoulos, C.; Xaplanteris, P.; Ioakeimidis, N.; Aznaouridis, K.; Baou, K.; Kardara, D.; Georgiopoulos, G.; Georgakopoulos, C.; Tousoulis, D. Cardiovascular Risk Factors Accelerate Progression of Vascular Aging in the General Population: Results From the CRAVE Study (Cardiovascular Risk Factors Affecting Vascular Age). Hypertension 2017, 70, 1057–1064. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
|
Total (n = 501) |
Men (n = 248) |
Women (n = 251) | p | ||||
|---|---|---|---|---|---|---|---|
| Age (years) | 55.90 | ±14.24 | 55.95 | ±14.31 | 55.85 | ±14.19 | 0.934 |
| Clinical variables, mean (SD) | |||||||
| Weight (kg) | 72.41 | ±13.61 | 79.22 | ±11.75 | 65.67 | ±11.87 | <0.001 |
| Height (cm) | 165.11 | ±9.68 | 171.60 | ±7.46 | 158.70 | ±6.98 | <0.001 |
| SBP (mmHg) | 120.69 | ±23.13 | 126.47 | ±19.52 | 114.99 | ±24.96 | <0.001 |
| DBP (mmHg) | 75.53 | ±10.10 | 77.40 | ±9.38 | 73.67 | ±10.46 | <0.001 |
| PP (mmHg) | 45.17 | ±19.81 | 49.06 | ±16.68 | 41.31 | 21.83 | <0.001 |
| Total cholesterol (mg/dL) | 194.76 | ±32.49 | 192.61 | ±32.26 | 196.88 | ±32.65 | 0.142 |
| LDL cholesterol (mg/dL) | 115.51 | ±29.37 | 117.43 | ±30.12 | 113.61 | ±28.54 | 0.148 |
| HDL cholesterol (mg/dL) | 58.88 | ±16.15 | 53.43 | ±14.23 | 64.27 | ±16.14 | <0.001 |
| Triglycerides (mg/dL) | 103.12 | ±53.11 | 112.27 | ±54.23 | 94.07 | ±50.48 | <0.001 |
| Fasting glucose (mg/dL) | 88.21 | ±17.37 | 90.14 | ±18.71 | 86.30 | ±15.73 | 0.013 |
| HbA1c (%) | 5.49 | ±0.56 | 5.54 | ±0.63 | 5.44 | ±0.47 | <0.001 |
| Smoker, (cigarettes day) | 14.23 | ±10.54 | 14.66 | ±11.00 | 13.83 | ±10.12 | 0.573 |
| cfPWV (m/s) | 8.17 | ±2.53 | 8.58 | ±2.74 | 7.77 | ±2.24 | 0.043 |
| Chronic diseases, n (%) | |||||||
| Hypertensive | 147 | (29.34) | 82 | (32.93) | 65 | (25.79) | 0.095 |
| Diabetes mellitus | 38 | (7.58) | 26 | (10.40) | 12 | (4.80) | 0.018 |
| Dyslipidemia | 191 | (38.12) | 95 | (38.10) | 96 | (38.20) | 0.989 |
| Obesity | 94 | (18.76) | 42 | (16.90) | 52 | (20.60) | 0.304 |
| Abdominal obesity | 193 | (38.52) | 78 | (31.30) | 115 | (45.80) | 0.001 |
| Smoker, n (%) | 90 | (17.96) | 49 | (9.80) | 41 | (8.20) | 0.353 |
| Medication, n (%) | |||||||
| Hypoglycaemic drugs | 35 | (7.00) | 23 | (9.20) | 12 | (4.80) | 0.055 |
| Antihypertensive drugs | 96 | (19.16) | 50 | (20.10) | 46 | (18.30) | 0.650 |
| Lipid-lowering drugs | 102 | (20.36) | 49 | (19.70) | 53 | (21.00) | 0.740 |
| Anthropometric parameters, mean (SD) | |||||||
| BMI (kg/m2) | 26.52 | ±4.23 | 26.90 | ±3.54 | 26.14 | ±4.79 | 0.044 |
| WC (cm) | 93.33 | ±12.00 | 98.76 | ±9.65 | 87.95 | ±11.68 | <0.001 |
| HC (cm) | 103.13 | ±9.24 | 102.71 | ±9.13 | 103.55 | ±9.34 | 0.313 |
| Ideal Weight (kg) | 65.11 | ±9.68 | 71.60 | ±7.46 | 58.70 | ±6.98 | <0.001 |
| WHtR | 0.57 | ±0.07 | 0.58 | ±0.06 | 0.56 | ±0.08 | 0.001 |
| WHR | 0.91 | ±0.12 | 0.97 | ±0.13 | 0.85 | ±0.07 | <0.001 |
| BAI (%) | 30.91 | ±6.01 | 27.80 | ±4.54 | 33.97 | ±5.71 | <0.001 |
| VAI (cm2) | 3.27 | ±2.44 | 3.31 | ±2.26 | 3.21 | ±2.61 | 0.656 |
| BRI | 4.79 | ±1.57 | 4.98 | ±1.36 | 4.59 | ±1.73 | 0.005 |
| CUNBAE | 33.20 | ±7.86 | 27.82 | ±5.07 | 38.50 | ±6.37 | <0.001 |
| AVI | 17.84 | ±4.44 | 19.76 | ±3.88 | 15.95 | ±4.13 | <0.001 |
| SATA | 286.24 | ±98.04 | 295.11 | ±82.06 | 277.48 | ±111.07 | 0.044 |
| IMP | 112.05 | ±18.83 | 111.11 | ±15.05 | 112.99 | ±21.92 | 0.264 |
| HVA | (n = 42) | NVA | (n = 353) | EVA | (n = 106) | p | |
|---|---|---|---|---|---|---|---|
| Total | |||||||
| BMI (kg/m2) *,‡ | 23.64 | ±3.37 | 26.67 | ±4.13 | 27.15 | ±4.44 | <0.001 |
| WC (cm) *,†,‡ | 87.05 | ±9.49 | 93.08 | ±11.83 | 96.59 | ±12.43 | <0.001 |
| HC (cm) *,‡ | 98.50 | ±10.76 | 103.36 | ±9.30 | 104.21 | ±7.84 | 0.002 |
| WHtR *,‡ | 0.53 | ±0.06 | 0.57 | ±0.07 | 0.58 | ±0.08 | <0.001 |
| WHR | 0.90 | ±0.19 | 0.90 | ±0.12 | 0.93 | ±0.09 | 0.224 |
| BAI (%) *,‡ | 28.41 | ±6.43 | 31.10 | ±6.02 | 31.25 | ±5.64 | 0.019 |
| VAI *,†,‡ | 2.41 | ±1.30 | 3.20 | ±2.39 | 3.77 | ±2.77 | <0.001 |
| BRI *,‡ | 3.93 | ±1.17 | 4.76 | ±1.54 | 5.19 | ±1.66 | <0.001 |
| CUNBAE *,‡ | 29.29 | ±7.03 | 33.63 | ±7.84 | 33.31 | ±7.85 | 0.000 |
| AVI (cm2) *,†,‡ | 15.51 | ±3.14 | 17.75 | ±4.37 | 19.06 | ±4.70 | 0.003 |
| SATA *,‡ | 219.53 | ±78.08 | 289.74 | ±95.76 | 300.91 | ±102.90 | <0.001 |
| IMP *,‡ | 110.03 | ±16.21 | 124.65 | ±19.86 | 127.34 | ±21.08 | <0.001 |
| Men | |||||||
| BMI (kg/m2) *,‡ | 24.72 | ±2.87 | 27.04 | ±3.44 | 27.23 | ±3.78 | 0.015 |
| WC (cm) *,‡ | 92.30 | ±5.80 | 98.75 | ±9.66 | 100.81 | ±9.79 | 0.002 |
| HC (cm) | 98.35 | ±13.40 | 102.80 | ±9.12 | 103.86 | ±7.11 | 0.061 |
| WHtR *,‡ | 0.54 | ±0.04 | 0.58 | ±0.06 | 0.59 | ±0.06 | 0.005 |
| WHR | 0.97 | ±0.26 | 0.97 | ±0.13 | 0.97 | ±0.06 | 0.984 |
| BAI (%) | 26.11 | ±6.55 | 27.71 | ±4.63 | 28.56 | ±3.30 | 0.098 |
| VAI | 2.79 | ±1.61 | 3.18 | ±2.23 | 3.76 | ±2.43 | 0.128 |
| BRI *,‡ | 4.17 | ±0.77 | 4.96 | ±1.38 | 5.29 | ±1.34 | 0.005 |
| CUNBAE *,‡ | 24.50 | ±4.52 | 27.85 | ±5.03 | 28.81 | ±4.98 | 0.004 |
| AVI (cm2) *,‡ | 17.25 | ±2.14 | 19.75 | ±3.87 | 20.55 | ±4.05 | 0.004 |
| SATA *,‡ | 244.58 | ±66.65 | 298.26 | ±79.82 | 302.76 | ±87.65 | 0.015 |
| IMP *,‡ | 114.50 | ±13.30 | 125.64 | ±16.38 | 127.07 | ±17.65 | 0.010 |
| Women | |||||||
| BMI (kg/m2) *,‡ | 22.66 | ±3.54 | 26.35 | ±4.64 | 27.03 | ±5.31 | 0.001 |
| WC (cm) *,‡ | 82.27 | ±9.75 | 88.08 | ±11.31 | 90.30 | ±13.35 | 0.030 |
| HC (cm) *,‡ | 98.64 | ±7.97 | 103.86 | ±9.46 | 104.72 | ±8.89 | 0.030 |
| WHtR *,‡ | 0.51 | ±0.07 | 0.56 | ±0.08 | 0.58 | ±0.09 | 0.012 |
| WHR | 0.83 | ±0.06 | 0.85 | ±0.07 | 0.86 | ±0.07 | 0.386 |
| BAI. (%) *,‡ | 30.51 | ±5.68 | 34.09 | ±5.50 | 35.238 | ±6.06 | 0.006 |
| VAI *,‡ | 2.06 | ±0.82 | 3.23 | ±2.52 | 3.80 | ±3.23 | 0.037 |
| BRI *,‡ | 3.70 | ±1.43 | 4.59 | ±1.65 | 5.05 | ±2.06 | 0.011 |
| CUNBAE *,‡ | 33.65 | ±6.01 | 38.73 | ±6.16 | 40.02 | ±6.42 | <0.001 |
| AVI (cm2) *,‡ | 13.93 | ±3.10 | 15.99 | ±4.02 | 16.84 | ±4.77 | 0.026 |
| SATA *,‡ | 196.75 | ±82.11 | 282.22 | ±107.55 | 298.15 | ±123.24 | <0.001 |
| IMP *,‡ | 105.97 | ±17.79 | 123.77 | ±22.49 | 127.73 | ±25.58 | <0.001 |
| Without FRC or IV | (n = 174) | With FRC or IV | (n = 327) | |
|---|---|---|---|---|
| Model 1 (Unadjusted) | Β (95% CI) | p-value | Β (95% CI) | p-value |
| BMI (kg/m2) | 0.113 (0.054–0.172) | <0.001 | 0.100 (0.029–0.171) | 0.006 |
| WC (cm) | 0.048 (0.027–0.069) | <0.001 | 0.071 (0.047–0.095) | <0.001 |
| HC (cm) | 0.008 (−0.020–0.035) | 0.578 | 0.025 (−0.007–0.057) | 0.121 |
| WHtR | 0.014 (0.012–0.017) | <0.001 | 0.100 (0.029–0.171) | 0.006 |
| WHR | 4.862 (2.876–6.847) | <0.001 | 4.818 (2.387–7.242) | <0.001 |
| BAI (%) | 0.031 (−0.012–0.075) | 0.155 | 0.051 (0.003–0.099) | 0.039 |
| VAI (cm2) | 0.104 (−0.139–0.347) | 0.400 | 0.095 (−0.015–0.205) | 0.090 |
| BRI | 0.459 (0.296–0.622) | <0.001 | 0.624 (0.442–0.805) | <0.001 |
| CUNBAE | 0.046 (0.014–0.078) | 0.005 | 0.042 (0.005–0.080) | 0.028 |
| AVI | 0.190 (0.126–0.254) | <0.001 | 0.142 (0.083–0.201) | <0.001 |
| SATA | 0.005 (0.002–0.007) | <0.001 | 0.004 (0.001–0.007) | 0.006 |
| IMP | 0.026 (0.013–0.040) | <0.001 | 0.023 (0.008–0.039) | 0.004 |
| Model 2 (Adjusted) | ||||
| BMI (kg/m2) | 0.061 (0.015–0.107) | 0.010 | 0.059 (0.003–0.116) | 0.040 |
| WC (cm) | 0.026 (0.007–0.045) | 0.007 | 0.037 (0.015–0.059) | 0.001 |
| HC (cm) | 0.014 (−0.006–0.034) | 0.016 | 0.031 (0.006–0.056) | 0.169 |
| WHtR | 0.004 (0.001–0.007) | 0.007 | 0.005 (0.001–0.008) | 0.008 |
| WHR | 1.975 (0.085–3.865) | 0.041 | 0.299 (−1.995–2.592) | 0.798 |
| BAI (%) | 0.027 (−0.010–0.064) | 0.150 | 0.029 (−0.020–0.077) | 0.251 |
| VAI (cm2) | 0.009 (−0.191–0.173) | 0.921 | 0.111 (0.024–0.197) | 0.012 |
| BRI | 0.206 (0.067–0.344) | 0.004 | 0.242 (0.079–0.406) | 0.004 |
| CUNBAE | 0.046 (0.009–0.082) | 0.015 | 0.046 (−0.001–0.093) | 0.056 |
| AVI | 0.077 (0.025–0.129) | 0.004 | 0.102 (0.043–0.161) | 0.001 |
| SATA | 0.003 (0.001–0.005) | 0.001 | 0.003 (0.001–0.005) | 0.040 |
| IMP | 0.014 (0.003–0.024) | 0.012 | 0.007 (−0.001–0.024) | 0.078 |
| Anthropometric Indices | OR | IC 95% | p-Value | OR | IC 95% | p-Value | |
|---|---|---|---|---|---|---|---|
| HVA (Reference) | Model 1 | Model 2 | |||||
| BMI (kg/m2) | 1.088 | 1.074–1.102 | <0.001 | 1.249 | 1.126–1385 | <0.001 | |
| WC (cm) | 1.024 | 1.020–1.027 | <0.001 | 1.063 | 1.025–1.102 | 0.001 | |
| HC, (cm) | 1.021 | 1.018–1.024 | <0.001 | 1.051 | 1.018–1.084 | 0.002 | |
| WHtR | 1.004 | 1.003–1.004 | <0.001 | 1.009 | 1.003–1.015 | 0.002 | |
| WHR | 1.038 | 1.007–1.482 | <0.001 | 1.017 | 0.035–29.822 | 0.992 | |
| NVA | BAI, (%) | 1.073 | 1.062–1.085 | <0.001 | 1.094 | 1.029–1.162 | 0.004 |
| VAI | 2.016 | 1.762–2.306 | <0.001 | 1.271 | 1.010–1.600 | 0.041 | |
| BRI | 1.600 | 1.483–1.727 | <0.001 | 1.578 | 1.187–2.097 | 0.002 | |
| CUNBAE | 1.069 | 1.058–1.081 | <0.001 | 1.181 | 1.095–1.275 | <0.001 | |
| AVI (cm2) | 1.132 | 1.110–1.155 | <0.001 | 1.200 | 1.078–1.336 | 0.001 | |
| SATA | 1.008 | 1.007–1.10 | <0.001 | 1.010 | 1.005–1.014 | <0.001 | |
| IMP | 1.020 | 1.017–1.023 | <0.001 | 1.050 | 1.025–1.074 | <0.001 | |
| BMI (kg/m2) | 1.042 | 1.027–1.056 | <0.001 | 1.263 | 1.130–1.412 | <0.001 | |
| WC (cm) | 1.011 | 1.007–1.015 | <0.001 | 1.065 | 1.033–1.119 | <0.001 | |
| HC, (cm) | 1.010 | 1.006–1.013 | <0.001 | 1.065 | 1.026–1.105 | 0.001 | |
| WHtR | 1.002 | 1.001–1.002 | <0.001 | 1.011 | 1.005–1.017 | 0.001 | |
| WHR | 1.029 | 1.010–1.043 | <0.001 | 0.617 | 0.015–25.897 | 0.800 | |
| EVA | BAI, (%) | 1.034 | 1.022–1.047 | <0.001 | 1.116 | 1.039–1.198 | 0.002 |
| VAI | 1.609 | 1.400–1.849 | <0.001 | 1.380 | 1.088–1.749 | 0.008 | |
| BRI | 1.295 | 1.194–1.406 | <0.001 | 1.714 | 1.259–2.334 | 0.001 | |
| CUNBAE | 1.033 | 1.021–1.045 | <0.001 | 1.193 | 1.097–1.298 | <0.001 | |
| AVI (cm2) | 1.067 | 1.045–1.090 | <0.001 | 1.237 | 1.102–1.389 | <0.001 | |
| SATA | 1.004 | 1.003–1.006 | <0.001 | 1.010 | 1.005–1.015 | <0.001 | |
| IMP | 1.010 | 1.006–1.013 | <0.001 | 1.052 | 1.026–1.079 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-Sánchez, L.; Gómez-Sánchez, M.; Rodríguez-Sánchez, E.; Patino-Alonso, C.; Alonso-Dominguez, R.; Sanchez-Aguadero, N.; Lugones-Sánchez, C.; Llamas-Ramos, I.; García-Ortiz, L.; Gómez-Marcos, M.A.; et al. Relationship of Different Anthropometric Indices with Vascular Ageing in an Adult Population without Cardiovascular Disease—EVA Study. J. Clin. Med. 2022, 11, 2671. https://doi.org/10.3390/jcm11092671
Gómez-Sánchez L, Gómez-Sánchez M, Rodríguez-Sánchez E, Patino-Alonso C, Alonso-Dominguez R, Sanchez-Aguadero N, Lugones-Sánchez C, Llamas-Ramos I, García-Ortiz L, Gómez-Marcos MA, et al. Relationship of Different Anthropometric Indices with Vascular Ageing in an Adult Population without Cardiovascular Disease—EVA Study. Journal of Clinical Medicine. 2022; 11(9):2671. https://doi.org/10.3390/jcm11092671
Chicago/Turabian StyleGómez-Sánchez, Leticia, Marta Gómez-Sánchez, Emiliano Rodríguez-Sánchez, Carmen Patino-Alonso, Rosario Alonso-Dominguez, Natalia Sanchez-Aguadero, Cristina Lugones-Sánchez, Ines Llamas-Ramos, Luis García-Ortiz, Manuel A. Gómez-Marcos, and et al. 2022. "Relationship of Different Anthropometric Indices with Vascular Ageing in an Adult Population without Cardiovascular Disease—EVA Study" Journal of Clinical Medicine 11, no. 9: 2671. https://doi.org/10.3390/jcm11092671