
Positivity Trends of Bacterial Cultures from Cases of Acute and Chronic Periprosthetic Joint Infections

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
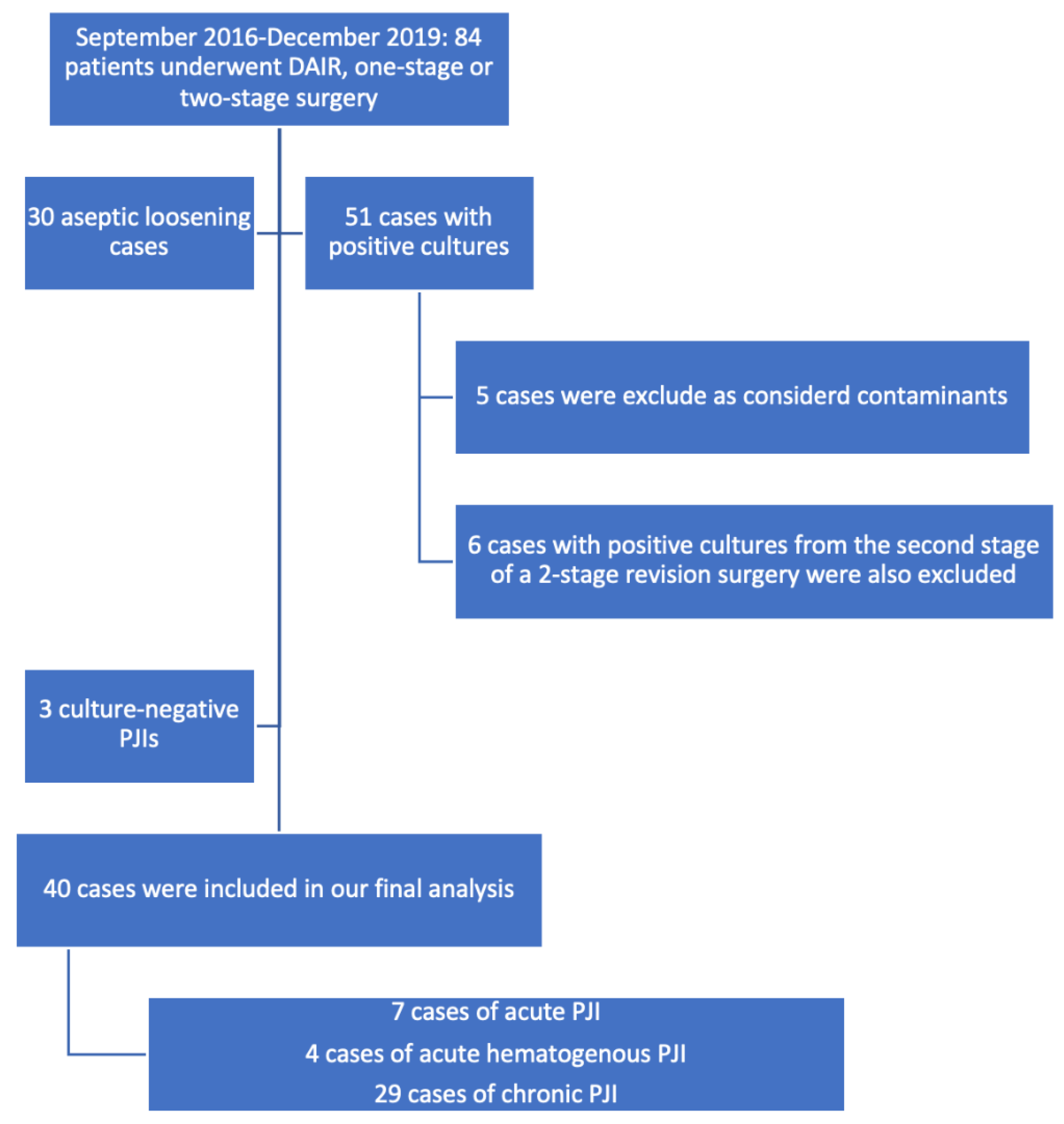
2.2. Study Population
2.3. Laboratory Studies
2.4. Study Definitions and Classification
2.5. Statistical Analysis
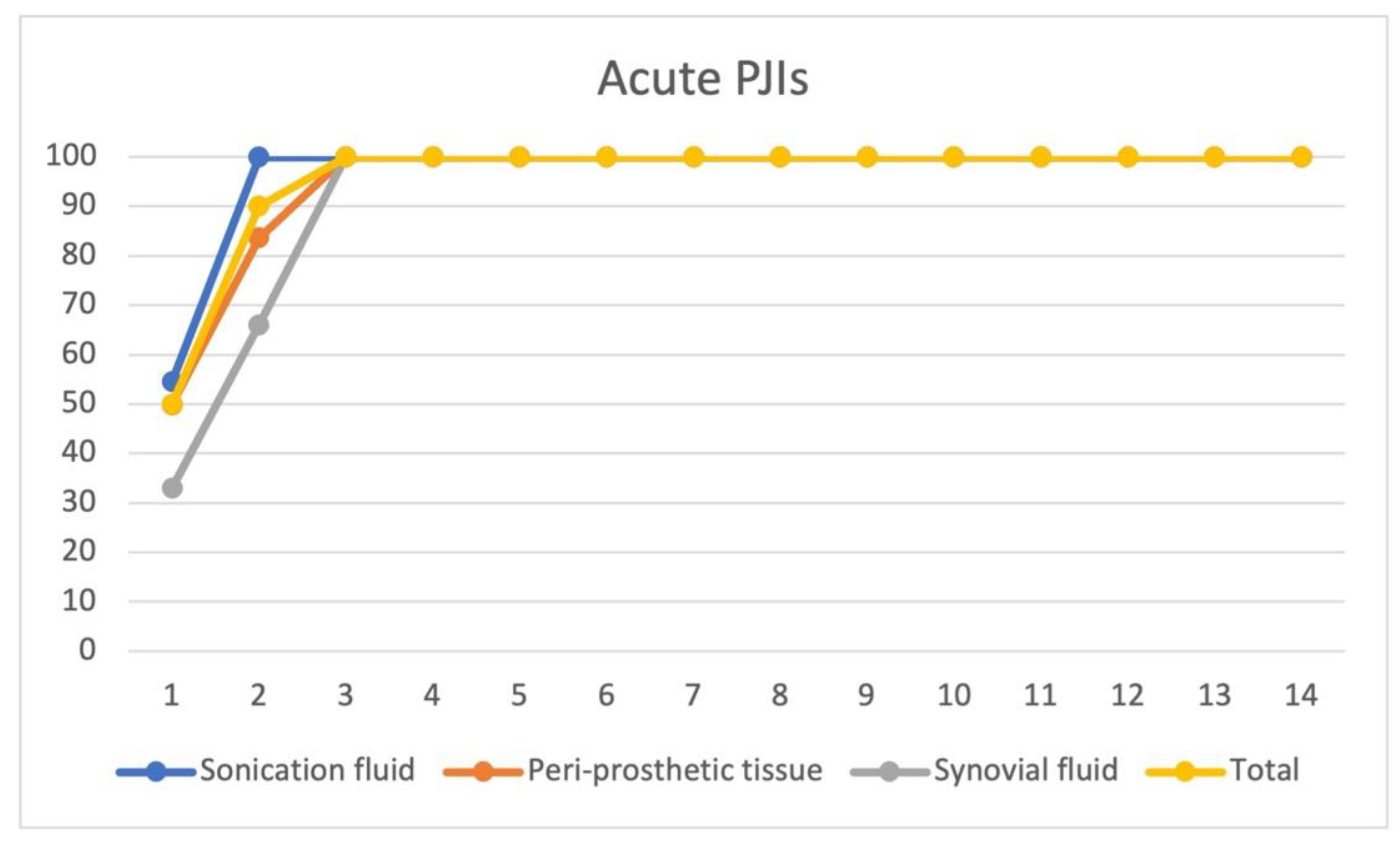
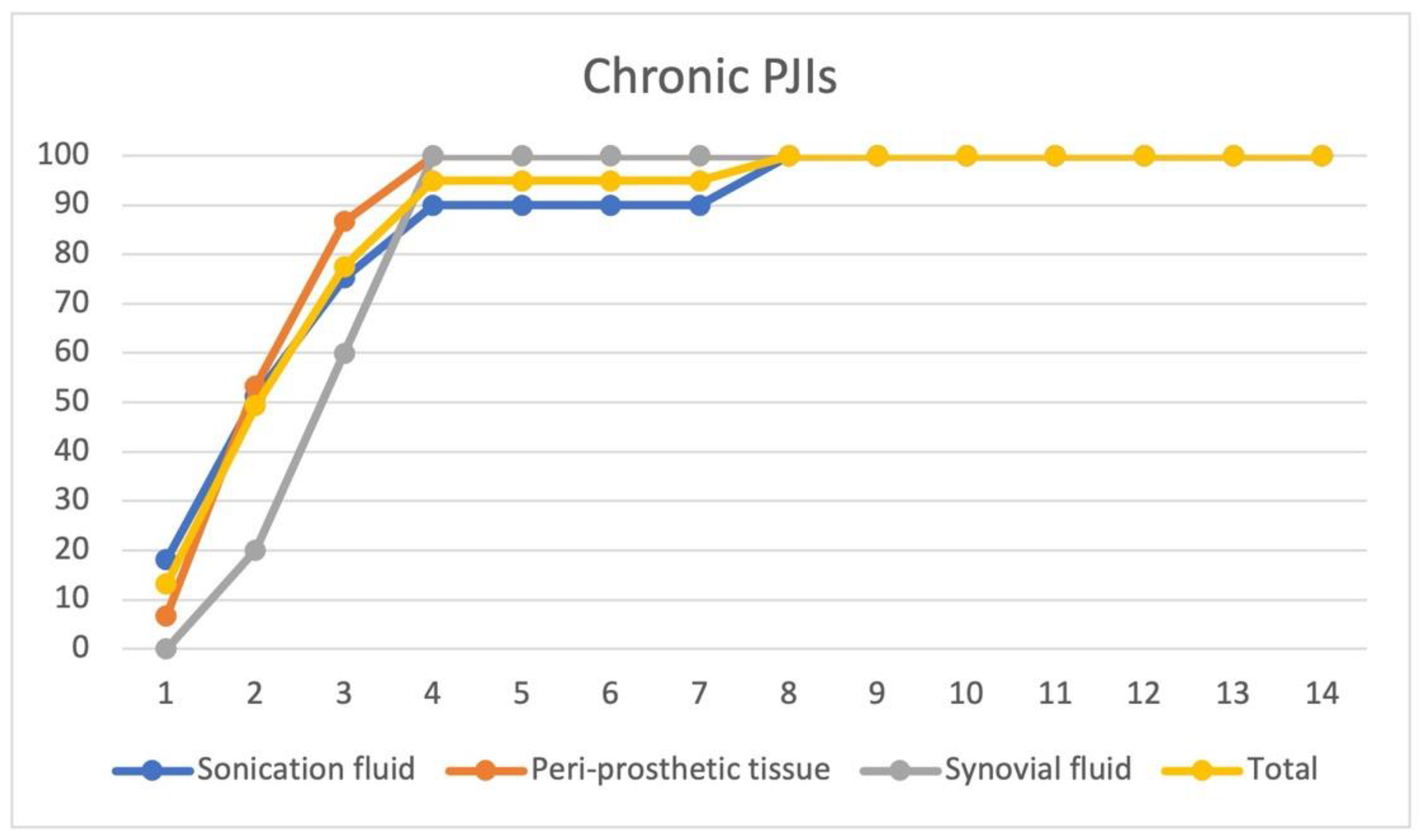
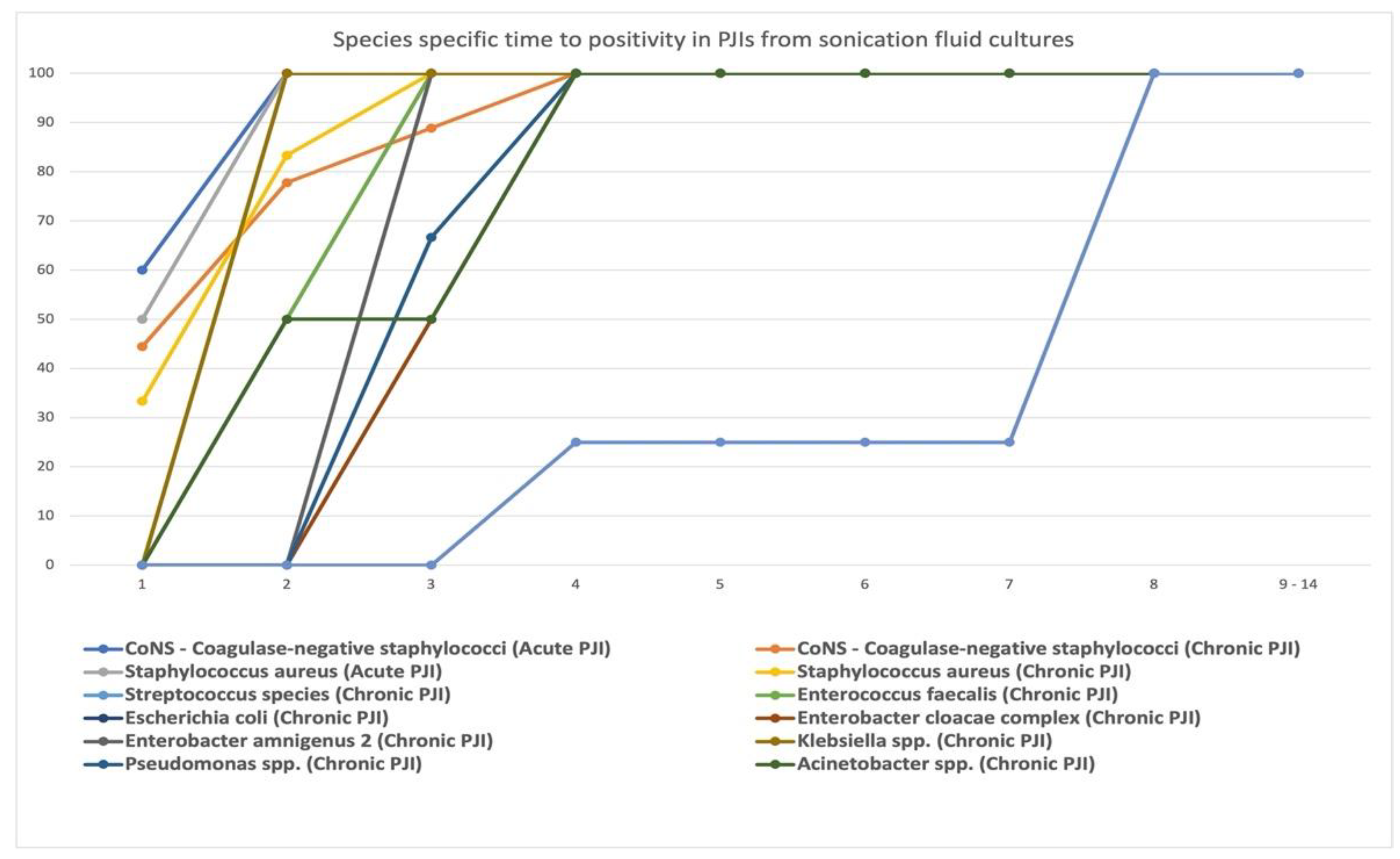
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Birlutiu, V.; Birlutiu, R.M. Endocarditis due to Abiotrophia defectiva, a biofilm-related infection associated with the presence of fixed braces: A case report. Medicine 2017, 96, e8756. [Google Scholar] [CrossRef] [PubMed]
- Birlutiu, V.; Birlutiu, R.M.; Costache, V.S. Viridans streptococcal infective endocarditis associated with fixed orthodontic appliance managed surgically by mitral valve plasty: A case report. Medicine 2018, 97, e11260. [Google Scholar] [CrossRef] [PubMed]
- Birlutiu, R.M.; Birlutiu, V.; Mihalache, M.; Mihalache, C.; Cismasiu, R.S. Diagnosis and management of orthopedic implant-associated infection: A comprehensive review of the literature. Biomed. Res. 2017, 28, 5063–5073. [Google Scholar]
- Klement, M.R.; Cunningham, D.J.; Wooster, B.M.; Wellman, S.S.; Bolognesi, M.P.; Green, C.L.; Garrigues, G.E. Comparing Standard versus Extended Culture Duration in Acute Hip and Knee Periprosthetic Joint Infection. J. Am. Acad. Orthop. Surg. 2019, 27, e437–e443. [Google Scholar] [CrossRef]
- Ting, N.T.; Della Valle, C.J. Diagnosis of Periprosthetic Joint Infection-An Algorithm-Based Approach. J. Arthroplast. 2017, 32, 2047–2050. [Google Scholar] [CrossRef]
- Zimmerli, W.; Trampuz, A.; Ochsner, P.E. Prosthetic-joint infections. N. Engl. J. Med. 2004, 351, 1645–1654. [Google Scholar] [CrossRef] [Green Version]
- Tarabichi, M.; Shohat, N.; Goswami, K.; Alvand, A.; Silibovsky, R.; Belden, K.; Parvizi, J. Diagnosis of Periprosthetic Joint Infection: The Potential of Next-Generation Sequencing. J. Bone Jt. Surg. Am. 2018, 100, 147–154. [Google Scholar] [CrossRef]
- Parvizi, J.; Gehrke, T.; Chen, A.F. Proceedings of the International Consensus on Periprosthetic Joint Infection. Bone Jt. J. 2013, 95, 1450–1452. [Google Scholar] [CrossRef]
- Ascione, T.; Barrack, R.; Benito, N.; Blevins, K.; Brause, B.; Cornu, O.; Frommelt, L.; Gant, V.; Goswami, K.; Hu, R.; et al. General Assembly, Diagnosis, Pathogen Isolation—Culture Matters: Proceedings of International Consensus on Orthopedic Infections. J. Arthroplast. 2019, 34, S197–S206. [Google Scholar] [CrossRef]
- Schäfer, P.; Fink, B.; Sandow, D.; Margull, A.; Berger, I.; Frommelt, L. Prolonged bacterial culture to identify late periprosthetic joint infection: A promising strategy. Clin. Infect Dis. 2008, 47, 1403–1409. [Google Scholar] [CrossRef] [Green Version]
- Wood, T.K.; Knabel, S.J.; Kwan, B.W. Bacterial persister cell formation and dormancy. Appl. Environ. Microbiol. 2013, 79, 7116–7121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Birlutiu, R.M.; Roman, M.D.; Cismasiu, R.S.; Fleaca, S.R.; Popa, C.M.; Mihalache, M.; Birlutiu, V. Sonication contribution to identifying prosthetic joint infection with Ralstonia pickettii: A case report and review of the literature. BMC Musculoskelet. Disord. 2017, 18, 311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Birlutiu, R.M.; Birlutiu, V.; Cismasiu, R.S.; Mihalache, M. bbFISH-ing in the sonication fluid. Medicine 2019, 98, e16501. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Zmistowski, B.; Berbari, E.F.; Bauer, T.W.; Springer, B.D.; Della Valle, C.J.; Garvin, K.L.; Mont, M.A.; Wongworawat, M.D.; Zalavras, C.G. New definition for periprosthetic joint infection: From the Workgroup of the Musculoskeletal Infection Society. Clin. Orthop. Relat. Res. 2011, 469, 2992–2994. [Google Scholar] [CrossRef] [Green Version]
- Parvizi, J.; Tan, T.L.; Goswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria. J. Arthroplast. 2018, 33, 1309–1314.e2. [Google Scholar] [CrossRef]
- Birlutiu, R.M.; Mihalache, M.; Mihalache, P.; Cismasiu, R.S.; Birlutiu, V. Mid-term follow-up results after implementing a new strategy for the diagnosis and management of periprosthetic joint infections. BMC Infect. Dis. 2021, 21, 807. [Google Scholar] [CrossRef]
- Parvizi, J.; Erkocak, O.F.; Della Valle, C.J. Culture-negative periprosthetic joint infection. J. Bone Jt. Surg. Am. 2014, 96, 430–436. [Google Scholar] [CrossRef]
- Talsma, D.T.; Ploegmakers, J.J.W.; Jutte, P.C.; Kampinga, G.; Wouthuyzen-Bakker, M. Time to positivity of acute and chronic periprosthetic joint infection cultures. Diagn. Microbiol. Infect. Dis. 2021, 99, 115178. [Google Scholar] [CrossRef]
- Tsai, Y.; Chang, C.H.; Lin, Y.C.; Lee, S.H.; Hsieh, P.H.; Chang, Y. Different microbiological profiles between hip and knee prosthetic joint infections. J. Orthop. Surg. 2019, 27, 2309499019847768. [Google Scholar] [CrossRef] [Green Version]
- Löwik, C.A.; Zijlstra, W.P.; Knobben, B.A.; Ploegmakers, J.J.; Dijkstra, B.; de Vries, A.J.; Kampinga, G.A.; Mithoe, G.; Al Moujahid, A.; Jutte, P.C.; et al. Obese patients have higher rates of polymicrobial and Gram-negative early periprosthetic joint infections of the hip than non-obese patients. PLoS ONE 2019, 14, e0215035. [Google Scholar] [CrossRef]
- Deroche, L.; Bémer, P.; Valentin, A.S.; Jolivet-Gougeon, A.; Tandé, D.; Héry-Arnaud, G.; Lemarié, C.; Kempf, M.; Bret, L.; Burucoa, C.; et al. The Right Time to Safely Re-Evaluate Empirical Antimicrobial Treatment of Hip or Knee Prosthetic Joint Infections. J. Clin. Med. 2019, 8, 2113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butler-Wu, S.M.; Burns, E.M.; Pottinger, P.S.; Magaret, A.S.; Rakeman, J.L.; Matsen, F.A., III; Cookson, B.T. Optimization of periprosthetic culture for diagnosis of Propionibacterium acnes prosthetic joint infection. J. Clin. Microbiol. 2011, 49, 2490–2495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwotzer, N.; Wahl, P.; Fracheboud, D.; Gautier, E.; Chuard, C. Optimal culture incubation time in orthopedic device-associated infections: A retrospective analysis of prolonged 14-day incubation. J. Clin. Microbiol. 2014, 52, 61–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Microorganisms | No. of Positive Cultures (No. of Strains Identified) from Sonication Fluid/Incubation Period Days | ||||||
|---|---|---|---|---|---|---|---|
| D 1 | D 2 | D 3 | D 4 | D 5–D 7 | D 8 | D 9–D14 | |
| S. epidermidis | 3 + 3 | 1 + 2 | 0 | 0 | 0 | 0 | 0 |
| S. lentus | 1 | 1 | 0 | 1 | 0 | 0 | 0 |
| S. xylosus | 0 | 1 | 1 | 0 | 0 | 0 | 0 |
| MRSA | 1 + 3 | 2 + 2 | 0 | 0 | 0 | 0 | 0 |
| MSSA | 1 | 1 + 1 | 1 | 0 | 0 | 0 | 0 |
| Str. group D | 0 | 1 | 1 | 0 | 0 | 0 | 0 |
| Ent. faecalis | 0 | 1 | 1 | 0 | 0 | 0 | 0 |
| E. coli | 0 | 1 | 0 | 0 | 0 | 0 | 0 |
| Enterobacter cloacae complex | 0 | 0 | 1 | 1 | 0 | 0 | 0 |
| Enterobacter amnigenus 2 | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| Klebsiella spp. | 0 | 1 | 0 | 0 | 0 | 0 | 0 |
| P. fluorescens | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| P. aeruginosa | 0 | 0 | 1 | 1 | 0 | 0 | 0 |
| Acinetobacter spp. | 0 | 1 | 0 | 1 | 0 | 0 | 0 |
| Ralstonia pickettii | 0 | 0 | 0 | 1 | 0 | 3 | 0 |
| Microorganisms | No. of Positive Cultures (No. of Strains Identified) from Periprosthetic Tissue/Incubation PERIOD Days | ||||||
|---|---|---|---|---|---|---|---|
| D 1 | D 2 | D 3 | D 4 | D 5–D 7 | D 8 | D 9–D 14 | |
| S. epidermidis | 0 | 1 + 1 | 1 | 0 | 0 | 0 | 0 |
| S. lentus | 0 | 0 | 0 | 1 | 0 | 0 | 0 |
| S. xylosus | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| MRSA | 1 + 2 | 1 + 1 | 1 | 1 | 0 | 0 | 0 |
| MSSA | 1 | 1 | 0 | 0 | 0 | 0 | 0 |
| Str. group D | 0 | 1 | 0 | 0 | 0 | 0 | 0 |
| Ent. faecalis | 0 | 1 | 1 | 0 | 0 | 0 | 0 |
| E. coli | 0 | 1 | 0 | 0 | 0 | 0 | 0 |
| Enterobacter cloacae complex | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| Enterobacter amnigenus 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Klebsiella spp. | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| P. fluorescens | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| P. aeruginosa | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| Acinetobacter spp. | 0 | 1 | 0 | 0 | 0 | 0 | 0 |
| Ralstonia pickettii | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Microorganisms | No. of Positive Cultures (No. of Strains Identified) from Synovial Fluid/Incubation Period Days | ||||||
|---|---|---|---|---|---|---|---|
| D 1 | D 2 | D 3 | D 4 | D 5–D 7 | D 8 | D 9–D 14 | |
| S. epidermidis | 0 | 1 | 1 | 0 | 0 | 0 | 0 |
| S. lentus | 0 | 0 | 0 | 1 | 0 | 0 | 0 |
| S. xylosus | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| MRSA | 1 | 1 | 1 | 1 | 0 | 0 | 0 |
| MSSA | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| Str. group D | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Ent. faecalis | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| E. coli | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Enterobacter cloacae complex | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Enterobacter amnigenus 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Klebsiella spp. | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| P. fluorescens | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| P.aeruginosa | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Acinetobacter spp. | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Ralstonia pickettii | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Birlutiu, R.M.; Stoica, C.I.; Russu, O.; Cismasiu, R.S.; Birlutiu, V. Positivity Trends of Bacterial Cultures from Cases of Acute and Chronic Periprosthetic Joint Infections. J. Clin. Med. 2022, 11, 2238. https://doi.org/10.3390/jcm11082238
Birlutiu RM, Stoica CI, Russu O, Cismasiu RS, Birlutiu V. Positivity Trends of Bacterial Cultures from Cases of Acute and Chronic Periprosthetic Joint Infections. Journal of Clinical Medicine. 2022; 11(8):2238. https://doi.org/10.3390/jcm11082238
Chicago/Turabian StyleBirlutiu, Rares Mircea, Cristian Ioan Stoica, Octav Russu, Razvan Silviu Cismasiu, and Victoria Birlutiu. 2022. "Positivity Trends of Bacterial Cultures from Cases of Acute and Chronic Periprosthetic Joint Infections" Journal of Clinical Medicine 11, no. 8: 2238. https://doi.org/10.3390/jcm11082238