
One Year of COVID-19: Lessons Learned in a Hand Trauma Center

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
- Age;
- Sex;
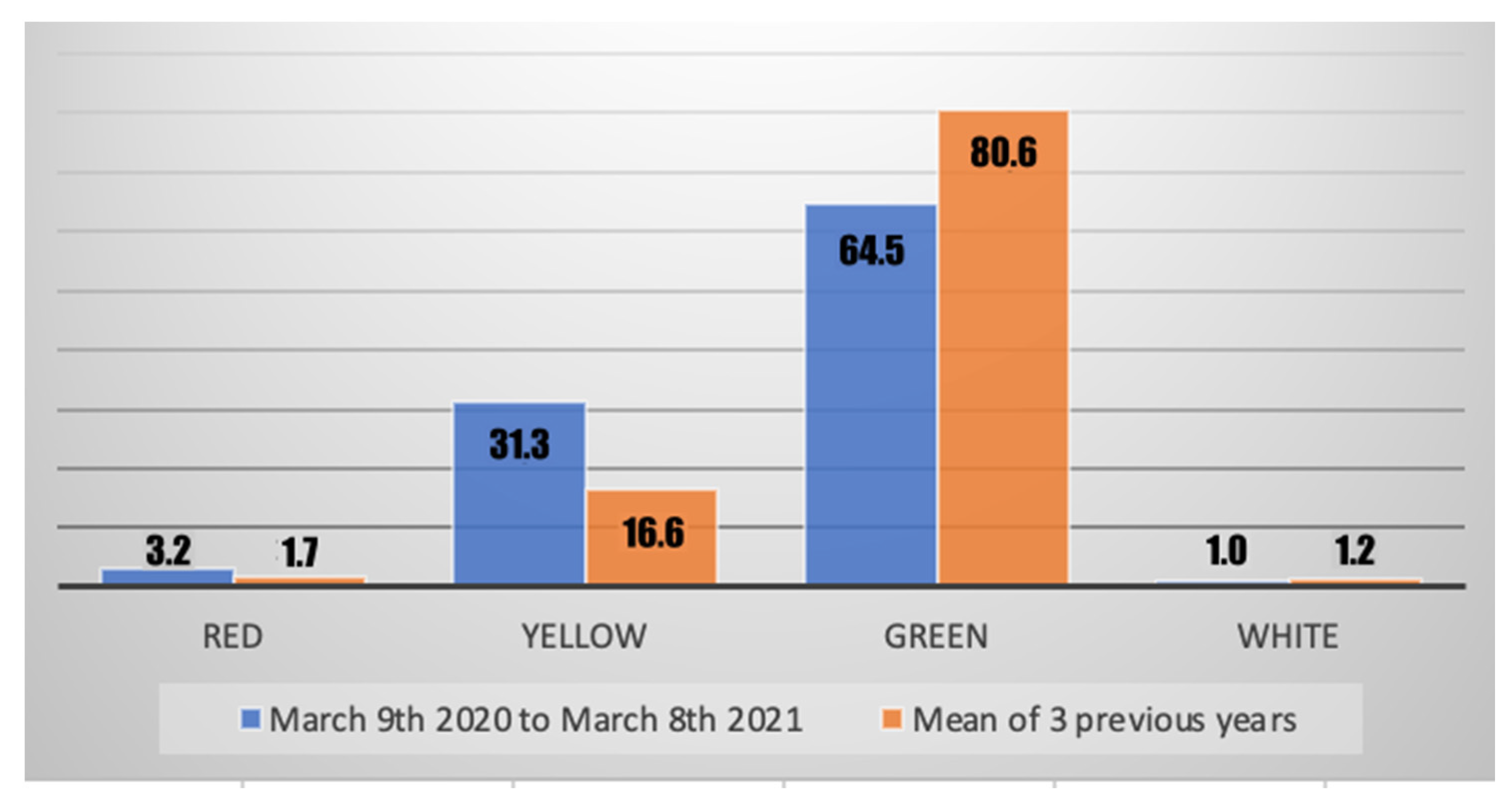
- Triage severity code: increasing from white and green (ambulatorial) to yellow (urgency) and red (emergency);
- Days of prognosis;
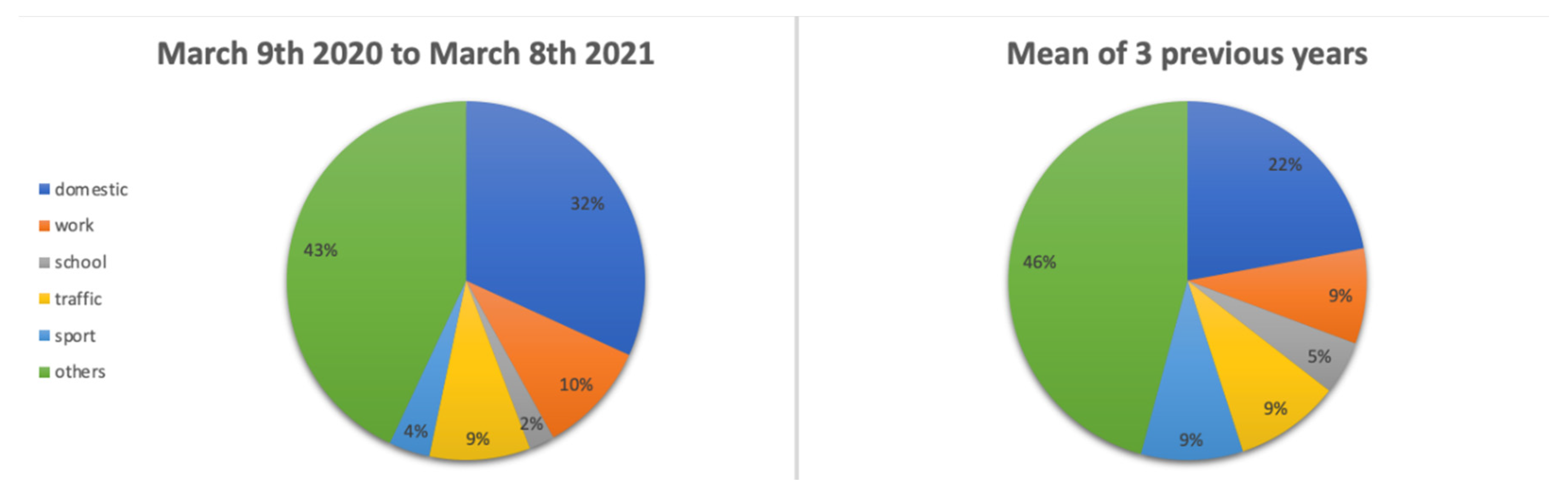
- Cause of the accident: domestic, work, school, traffic, sport, other (including self-harm lesions, bites, assaults, non-specified);
- Type of lesion: amputation, fracture, tendinous, other (including nerves, dislocation, bruise, cutaneous, infection, non-specified);
- If the patient underwent surgery for the hand lesion that brought them to the ED;
- If the patient was hospitalized directly from the ED.
3. Results
3.1. Accesses to ED
3.2. Age and Sex
3.3. Severity of Lesions
3.4. Causes and Types of Lesions
3.5. Treatment and Hospitalization
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marco, G.; Anna, D.L.; Andrea, L.A.; Giorgio, P.; Carlo, M.; Fabio, V.; Francesco, F.; Gianni, F.; Alessio, P. Incidence estimates of hand and upper extremity injuries in Italy. Ann. Ist. Super. Sanita. 2015, 51, 305–312. [Google Scholar] [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Covino, M.; De Matteis, G.; Santoro, M.; Sabia, L.; Simeoni, B.; Candelli, M.; Ojetti, V.; Franceschi, F. Clinical characteristics and prognostic factors in COVID-19 patients aged ≥ 80 years. Geriatr. Gerontol. Int. 2020, 20, 704–708. [Google Scholar] [CrossRef] [PubMed]
- Ojetti, V.; Covino, M.; Brigida, M.; Petruzziello, C.; Saviano, A.; Migneco, A.; Candelli, M.; Franceschi, F. Non-COVID Diseases during the Pandemic: Where Have All Other Emergencies Gone? Medicina 2020, 56, 512. [Google Scholar] [CrossRef]
- Perna, A.; Passiatore, M.; Massaro, A.; Terrinoni, A.; Bianchi, L.; Cilli, V.; D’Orio, M.; Proietti, L.; Taccardo, G.; De Vitis, R. Skin manifestations in COVID-19 patients, state of the art. A systematic review. Int. J. Dermatol. 2021, 60, 547–553. [Google Scholar] [CrossRef]
- Barbary, S.; Dap, F.; Dautel, G. Finger replantation: Surgical technique and indications. Chir. Main 2013, 32, 363–372. [Google Scholar] [CrossRef]
- Maccagnano, G.; Noia, G.; Vicenti, G.; Baglioni, M.; Masciale, M.R.; Cassano, G.D.; Vitiello, R.; Moretti, B.; Pesce, V. Volar locking plate versus external fixation in distal radius fractures: A meta-analysis. Orthop. Rev. 2021, 13, 9147. [Google Scholar] [CrossRef]
- Tang, J.B. Flexor Tendon Injuries. Clin. Plast. Surg. 2019, 46, 295–306. [Google Scholar] [CrossRef]
- Hwee, J.; Chiew, J.; Sechachalam, S. The Impact of Coronavirus Disease 2019 (COVID-19) on the Practice of Hand Surgery in Singapore. J. Hand Surg. 2020, 45, 536–541. [Google Scholar] [CrossRef]
- Qazi, U.A.; Sutton, J.; Farner, S.C.; Bhandari, L. Impact of the COVID-19 Pandemic on the Practice of Hand and Upper Extremity Surgeons. Cureus 2020, 12, e12072. [Google Scholar] [CrossRef]
- Toia, F.; Romeo, M.; Abate, M.; Avarotti, E.; Battiston, B.; Bruno, G.; Cannavò F, F.; Casamichele, C.; Colonna, M.; Catena, N.; et al. Impact of COVID-19 on hand surgery in Italy: A comparison between the Northern and the Southern regions. Hand Surg. Rehabil. 2020, 40, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Venkatesan, A.; Iyengar, K.; Loh, W.Y. Strategies in reconfiguration of hand injuries management during COVID-19 pandemic. J. Clin. Orthop. Trauma 2020, 11, 697–699. [Google Scholar] [CrossRef]
- Ho, E.; Riordan, E.; Nicklin, S. Hand injuries during COVID-19: Lessons from lockdown. J. Plast. Reconstr. Aesthetic Surg. 2020, 74, 1408–1412. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.V.; Holmes, D.G.; Jansen, V.; Fowler, C.L.; Wormald, J.C.; Wade, R.G.; Reay, E.K.; Gardiner, M.D. Adapting to the COVID-19 pandemic: A survey of UK and European hand surgery units. J. Plast. Reconstr. Aesthetic Surg. 2021, in press. [CrossRef] [PubMed]
- Saha, S.; Dash, S.; Ansari, M.T.; Bichupuriya, A.D.; Gupta, A.K.; Singhal, M. Optimising Hand Surgery during COVID-19 Pandemic. J. Hand Surg. 2021, 26, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Poggetti, A.; Del Chiaro, A.; Nucci, A.M.; Suardi, C.; Pfanner, S. How hand and wrist trauma has changed during covid-19 emergency in Italy: Incidence and distribution of acute injuries. What to learn? J. Clin. Orthop. Trauma 2020, 12, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Atia, F.; Pocnetz, S.; Selby, A.; Russell, P.; Bainbridge, C.; Johnson, N. The effect of the COVID-19 lockdown on hand trauma surgery utilization. Bone Jt. Open 2020, 1, 633–637. [Google Scholar] [CrossRef] [PubMed]
- Pichard, R.; Kopel, L.; Lejeune, Q.; Masmoudi, R.; Masmejean, E.H. Impact of the COronaVIrus Disease 2019 lockdown on hand and upper limb emergencies: Experience of a referred university trauma hand centre in Paris, France. Int. Orthop. 2020, 44, 1497–1501. [Google Scholar] [CrossRef]
- Fortané, T.; Bouyer, M.; Le Hanneur, M.; Belvisi, B.; Courtiol, G.; Chevalier, K.; Dainotto, C.; Loret, M.; Kling, A.; Bentejac, A.; et al. Epidemiology of hand traumas during the COVID-19 confinement period. Injury 2021, 52, 679–685. [Google Scholar] [CrossRef]
- Pidgeon, T.; Parthiban, S.; Malone, P.; Foster, M.; Chester, D. Injury patterns of patients with upper limb and hand trauma sustained during the COVID-19 pandemic lockdown in the UK: A retrospective cohort study. Hand Surg. Rehabil. 2021, 40, 235–240. [Google Scholar] [CrossRef]
- Regas, I.; Pichonnat, M.; Pluvy, I.; Obert, L.; Bellemère, P.; Chaves, C.; Loisel, F. The impact of COVID-19 on hand surgery: A French retrospective comparative study in COVID-19 and non-COVID-19 hand trauma centers. Orthop. Traumatol. Surg. Res. 2021, 103118, Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Katt, B.M.; Imbergamo, C.; Fletcher, D.; Aita, D.; Nakashian, M.; Kwok, M.; Beredjiklian, P.K. Telehealth for Upper Extremity Conditions: Perceptions of the Patient and Provider. JAAOS Glob. Res. Rev. 2020, 4, e20.00127. [Google Scholar] [CrossRef] [PubMed]
- Martin-Playa, P.; Calzacorta-Muñoz, P.; Elizalde, L.A.; Carrera-Casal, O.; Gutiérrez, J.G. An overview of the situation of hand surgery in Spain during the peak of COVID-19 pandemic. Hand Surg. Rehabil. 2020, 39, 454–458. [Google Scholar] [CrossRef] [PubMed]
- Picardo, N.E.; Walker, H.; Vanat, Q.; Nizar, B.; Madura, T.; Jose, R. Service reconfiguration in the department of hand surgery during the UK COVID-19 lockdown: Birmingham experience. Postgrad. Med. J. 2021, 97, 532–538. [Google Scholar] [CrossRef] [PubMed]
- Westley, S.; Mistry, R.; Dheansa, B. Accuracy of virtual assessment in hand trauma. JPRAS Open 2021, 31, 92–98. [Google Scholar] [CrossRef]
- Bartoletta, J.J.; Hinchcliff, K.M.; Rhee, P.C. Comparison of Patient Perception and Satisfaction of Face-to-Face Versus Telemedicine Encounters in Hand Surgery. Hand 2021, 15589447211044786, Epub ahead of print. [Google Scholar] [CrossRef]
- Acciaro, A.L.; Montanari, S.; Venturelli, M.; DE Santis, G.; Starnoni, M.; Adani, R. New management and trauma incidence in hand surgery during the phase 1 of COVID-19 pandemic in a referral hand surgery and microsurgery center into the outbreak in North Italy. Minerva Orthop. 2021, 72, 520–525. [Google Scholar] [CrossRef]
- De Vitis, R.; Passiatore, M.; Perna, A.; Proietti, L.; Taccardo, G. COVID-19 contagion and contamination through hands of trauma patients: What risks and what precautions? J. Hosp. Infect. 2020, 105, 354–355. [Google Scholar] [CrossRef]
- Saleh, S.; Faulkner, H.; Golledge, K.; Graham, D.J.; Lawson, R.D.; Symes, M.J.; Sivakumar, B.S. The Impact of COVID-19 on Hand Trauma. Hand 2021, 155894472110289, Epub ahead of print. [Google Scholar] [CrossRef]
- Fulchignoni, C.; Bonetti, M.A.; Rovere, G.; Ziranu, A.; Maccauro, G.; Pataia, E. Wide awake surgery for flexor tendon primary repair: A literature review. Orthop. Rev. 2020, 12, 8668. [Google Scholar] [CrossRef]
- Acciaro, A.L.; Montanari, S.; Venturelli, M.; Starnoni, M.; Adani, R. Retrospective study in clinical governance and financing system impacts of the COVID-19 pandemic in the hand surgery and microsurgery HUB center. Musculoskelet. Surg. 2021, 1–6, Epub ahead of print. [Google Scholar] [CrossRef]
- Munz, G.; Poggetti, A.; Cenci, L.; Rizzo, A.R.; Biondi, M.; Pfanner, S. Up to five-week delay in primary repair of Zone 2 flexor tendon injuries: Outcomes and complications. J. Hand Surg. 2021, 46, 818–824. [Google Scholar] [CrossRef] [PubMed]
- Cinci, G.F. Scaphoid non-union during Covid-19 pandemic: Need for a smart strategy. Injury 2020, 52, 1102. [Google Scholar] [CrossRef] [PubMed]
- Svorai Band, S.; Gannot, G.; Oron, A. Failure to Approach the Emergency Room Following a Hand Laceration Due to Fear during the COVID-19 Pandemic. Isr. Med. Assoc. J. 2021, 23, 88. [Google Scholar]



{kind=link}
{kind=link}
| 9 March 2020 to 8 March 2021 | 9 March 2019 to 8 March 2020 | 9 March 2018 to 8 March 2019 | 9 March 2017 to 8 March 2018 | Mean of Previous 3 Years | ||
|---|---|---|---|---|---|---|
| Total number of patients | 974 | 1848 | 1872 | 1785 | 1835 | |
| Mean age of patients * | 39.6 | 35.1 | 35.3 | 34.8 | 35.1 | |
| (range) | (0–96) | (0–92) | (0–96) | (0–93) | (0–96) | |
| (Standard deviation) | (21.0) | (21.8) | (22.0) | (22.0) | (21.9) | |
| Sex | Male | 653 (67.0%) | 1212 (65.6%) | 1208 (64.5%) | 1152 (64.5%) | 1190.7 (64.9%) |
| Female | 321 (33.0%) | 636 (34.4%) | 664 (35.5%) | 633 (35.5%) | 644.3 (35.1%) | |
| 9 March 2020 to 8 March 2021 | 9 March 2019 to 8 March 2020 | 9 March 2018 to 8 March 2019 | 9 March 2017 to 8 March 2018 | Mean of Previous 3 Years | |
|---|---|---|---|---|---|
| Domestic | 310 (31.8%) | 404 (21.9%) | 418 (22.3%) | 395 (22.1%) | 405.7 (22.1%) |
| Work | 98 (10.1%) | 170 (9.2%) | 145 (7.7%) | 159 (8.9%) | 158 (8.6%) |
| School | 22 (2.3%) | 92 (5.0%) | 90 (4.8%) | 83 (4.7%) | 88.3 (4.8%) |
| Traffic | 89 (9.1%) | 186 (10.1%) | 165 (8.8%) | 171 (9.6%) | 174 (9.2%) |
| Sport | 36 (3.7%) | 172 (9.3%) | 181 (9.7%) | 154 (8.6%) | 169 (9.2%) |
| Other | 419 (43.0%) | 824 (44.5%) | 873 (46.7%) | 823 (46.1%) | 840 (45.8%) |
| 9 March 2020 to 8 March 2021 | 9 March 2019 to 8 March 2020 | 9 March 2018 to 8 March 2019 | 9 March 2017 to 8 March 2018 | Mean of Previous Years | |
|---|---|---|---|---|---|
| Amputations | 62 (6.4%) | 98 (5.3%) | 96 (5.1%) | 83 (4.7%) | 92.3 (5.0%) |
| Fractures | 256 (25.2%) | 377 (20.4%) | 385 (20.6%) | 334 (18.7%) | 365.3 (19.9%) |
| Tendinous lesions | 59 (6.1%) | 50 (2.7%) | 55 (2.9%) | 70 (3.9%) | 58.3 (3.1%) |
| Other | 607 (62.3%) | 1323 (71.6%) | 1336 (71.4%) | 1298 (72.7%) | 1319 (71.9%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Covino, M.; Fulchignoni, C.; Pietramala, S.; Barbaliscia, M.; Franceschi, F.; Maccauro, G.; Merendi, G.; Rocchi, L. One Year of COVID-19: Lessons Learned in a Hand Trauma Center. J. Clin. Med. 2022, 11, 2163. https://doi.org/10.3390/jcm11082163
Covino M, Fulchignoni C, Pietramala S, Barbaliscia M, Franceschi F, Maccauro G, Merendi G, Rocchi L. One Year of COVID-19: Lessons Learned in a Hand Trauma Center. Journal of Clinical Medicine. 2022; 11(8):2163. https://doi.org/10.3390/jcm11082163
Chicago/Turabian StyleCovino, Marcello, Camillo Fulchignoni, Silvia Pietramala, Marco Barbaliscia, Francesco Franceschi, Giulio Maccauro, Gianfranco Merendi, and Lorenzo Rocchi. 2022. "One Year of COVID-19: Lessons Learned in a Hand Trauma Center" Journal of Clinical Medicine 11, no. 8: 2163. https://doi.org/10.3390/jcm11082163