
Comparison of the Effects of Propofol and Sevoflurane Anesthesia on Optic Nerve Sheath Diameter in Robot-Assisted Laparoscopic Gynecology Surgery: A Randomized Controlled Trial

Abstract
:1. Introduction
2. Material and Methods
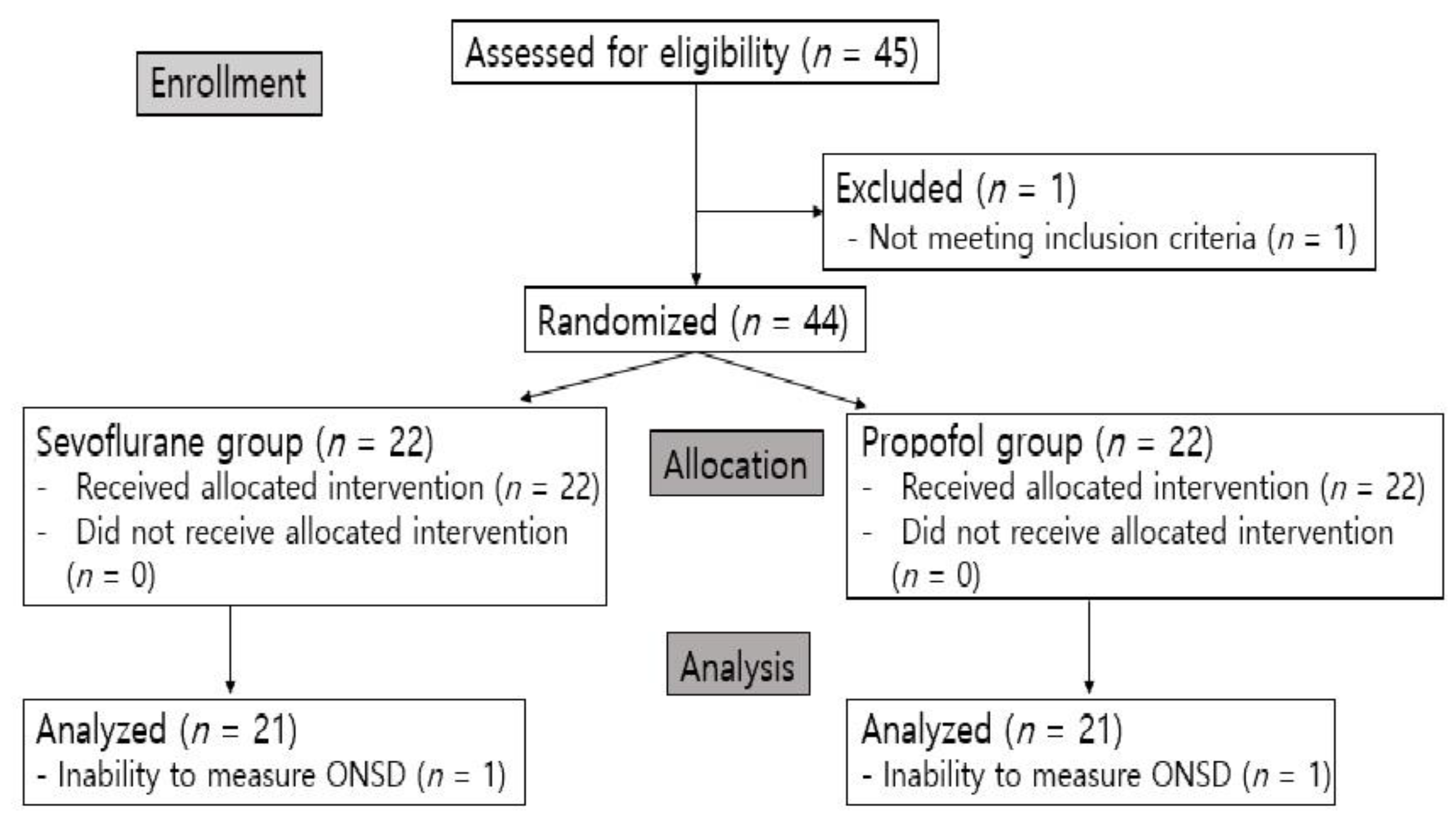
2.1. Participants
2.2. Anesthetic and Surgical Techniques
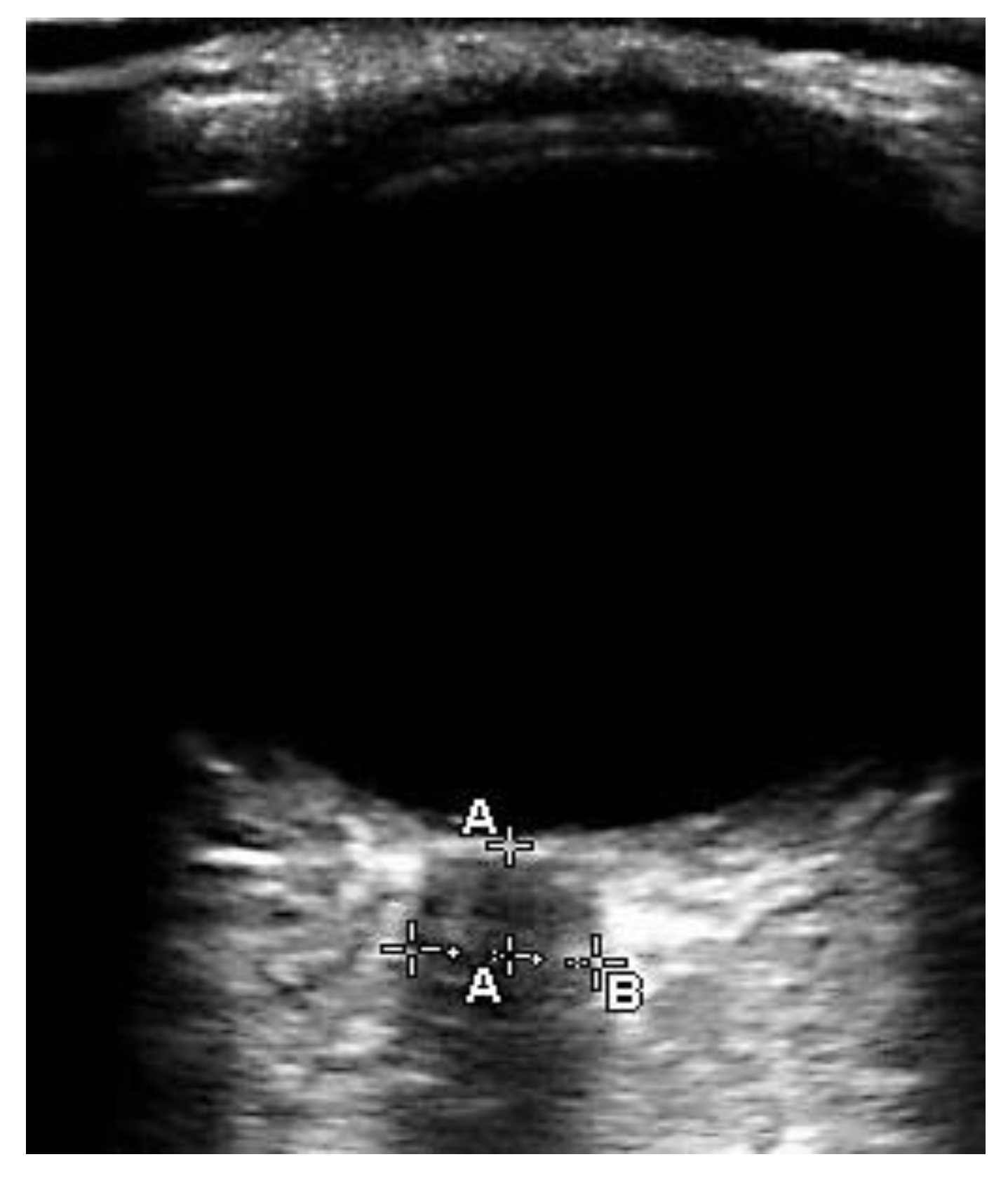
2.3. Measurements
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Prodromidou, A.; Spartalis, E.; Tsourouflis, G.; Dimitroulis, D.; Nikiteas, N. Robotic versus laparoendoscopic single-site hysterectomy: A systematic review and meta-analysis. J. Robot. Surg. 2020, 14, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, M.; Watanabe, H.; Kurahashi, T. Effects of 25- and 30-degree Trendelenburg positions on intraocular pressure changes during robot-assisted radical prostatectomy. Prostate Int. 2017, 5, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Robba, C.; Cardim, D.; Donnelly, J.; Bertuccio, A.; Bacigaluppi, S.; Bragazzi, N.; Cabella, B.; Liu, X.; Matta, B.; Lattuada, M.; et al. Effects of pneumoperitoneum and Trendelenburg position on intracranial pressure assessed using different non-invasive methods. Br. J. Anaesth. 2016, 117, 783–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sujata, N.; Tobin, R.; Tamhankar, A.; Gautam, G.; Yatoo, A.H. A randomised trial to compare the increase in intracranial pressure as correlated with the optic nerve sheath diameter during propofol versus sevoflurane-maintained anesthesia in robot-assisted laparoscopic pelvic surgery. J. Robot. Surg. 2019, 13, 267–273. [Google Scholar] [CrossRef]
- Whiteley, J.R.; Taylor, J.; Henry, M.; Epperson, T.I.; Hand, W.R. Detection of elevated intracranial pressure in robot-assisted laparoscopic radical prostatectomy using ultrasonography of optic nerve sheath diameter. J. NeuroSurg. Anesthesiol. 2015, 27, 155–159. [Google Scholar] [CrossRef]
- Blecha, S.; Harth, M.; Schlachetzki, F.; Zeman, F.; Blecha, C.; Flora, P.; Burger, M.; Denzinger, S.; Graf, B.M.; Helbig, H.; et al. Changes in intraocular pressure and optic nerve sheath diameter in patients undergoing robotic-assisted laparoscopic prostatectomy in steep 45 degrees Trendelenburg position. BMC Anesthesiol. 2017, 17, 40. [Google Scholar] [CrossRef] [Green Version]
- Jun, I.J.; Kim, M.; Lee, J.; Park, S.U.; Hwang, J.H.; Hong, J.H.; Kim, Y.K. Effect of Mannitol on Ultrasonographically Measured Optic Nerve Sheath Diameter as a Surrogate for Intracranial Pressure During Robot-Assisted Laparoscopic Prostatectomy with Pneumoperitoneum and the Trendelenburg Position. J. Endourol. 2018, 32, 608–613. [Google Scholar] [CrossRef]
- Shah, S.B.; Bhargava, A.K.; Choudhury, I. Noninvasive intracranial pressure monitoring via optic nerve sheath diameter for robotic surgery in steep Trendelenburg position. Saudi J. Anaesth. 2015, 9, 239–246. [Google Scholar] [CrossRef]
- Kim, S.J.; Kwon, J.Y.; Cho, A.R.; Kim, H.K.; Kim, T.K. The effects of sevoflurane and propofol anesthesia on cerebral oxygenation in gynecological laparoscopic surgery. Korean J. Anesthesiol. 2011, 61, 225–232. [Google Scholar] [CrossRef] [Green Version]
- Engelhard, K.; Werner, C. Inhalational or intravenous anesthetics for craniotomies? Pro inhalational. Curr. Opin. Anaesthesiol. 2006, 19, 504–508. [Google Scholar] [CrossRef]
- Tayal, V.S.; Neulander, M.; Norton, H.J.; Foster, T.; Saunders, T.; Blaivas, M. Emergency department sonographic measurement of optic nerve sheath diameter to detect findings of increased intracranial pressure in adult head injury patients. Ann. Emerg. Med. 2007, 49, 508–514. [Google Scholar] [CrossRef]
- Potgieter, D.; Kippin, A.; Ngu, F.; McKean, C. Can accurate ultrasonographic measurement of the optic nerve sheath diameter (a non-invasive measure of intracranial pressure) be taught to novice operators in a single training session? Anaesth. Intensive Care 2011, 39, 95–100. [Google Scholar] [CrossRef] [Green Version]
- Soliman, I.; Johnson, G.; Gillman, L.M.; Zeiler, F.A.; Faqihi, F.; Aletreby, W.T.; Balhamar, A.; Mahmood, N.N.; Ahmad Mumtaz, S.; Alharthy, A.; et al. New Optic Nerve Sonography Quality Criteria in the Diagnostic Evaluation of Traumatic Brain Injury. Crit. Care Res. Pract. 2018, 2018, 3589762. [Google Scholar] [CrossRef] [Green Version]
- Yu, J.; Hong, J.H.; Park, J.Y.; Hwang, J.H.; Cho, S.S.; Kim, Y.K. Propofol attenuates the increase of sonographic optic nerve sheath diameter during robot-assisted laparoscopic prostatectomy: A randomized clinical trial. BMC Anesthesiol. 2018, 18, 72. [Google Scholar] [CrossRef] [Green Version]
- Geng, W.; Chen, C.; Sun, X.; Huang, S. Effects of sevoflurane and propofol on the optic nerve sheath diameter in patients undergoing laparoscopic gynecological surgery: A randomized controlled clinical studies. BMC Anesthesiol. 2021, 21, 30. [Google Scholar] [CrossRef]
- Choi, E.S.; Jeon, Y.T.; Sohn, H.M.; Kim, D.W.; Choi, S.J.; In, C.B. Comparison of the effects of desflurane and total intravenous anesthesia on the optic nerve sheath diameter in robot assisted laparoscopic radical prostatectomy: A randomized controlled trial. Medicine 2018, 97, e12772. [Google Scholar] [CrossRef]
- Kim, Y.; Choi, S.; Kang, S.; Park, B. Propofol Affects Optic Nerve Sheath Diameter less than Sevoflurane during Robotic Surgery in the Steep Trendelenburg Position. Biomed. Res. Int. 2019, 2019, 5617815. [Google Scholar] [CrossRef]
- Petersen, K.D.; Landsfeldt, U.; Cold, G.E.; Petersen, C.B.; Mau, S.; Hauerberg, J.; Holst, P.; Olsen, K.S. Intracranial pressure and cerebral hemodynamic in patients with cerebral tumors: A randomized prospective study of patients subjected to craniotomy in propofol-fentanyl, isoflurane-fentanyl, or sevoflurane-fentanyl anesthesia. Anesthesiology 2003, 98, 329–336. [Google Scholar] [CrossRef]
- Kuzkov, V.V.; Obraztsov, M.Y.; Ivashchenko, O.Y.; Ivashchenko, N.Y.; Gorenkov, V.M.; Kirov, M.Y. Total Intravenous Versus Volatile Induction and Maintenance of Anesthesia in Elective Carotid Endarterectomy: Effects on Cerebral Oxygenation and Cognitive Functions. J. Cardiothorac. Vasc. Anesth. 2018, 32, 1701–1708. [Google Scholar] [CrossRef]
- Iida, H.; Ohata, H.; Iida, M.; Watanabe, Y.; Dohi, S. Isoflurane and sevoflurane induce vasodilation of cerebral vessels via ATP-sensitive K+ channel activation. Anesthesiology 1998, 89, 954–960. [Google Scholar] [CrossRef]
- Matta, B.F.; Heath, K.J.; Tipping, K.; Summors, A.C. Direct cerebral vasodilatory effects of sevoflurane and isoflurane. Anesthesiology 1999, 91, 677–680. [Google Scholar] [CrossRef] [PubMed]
- Vimala, S.; Arulvelan, A.; Chandy Vilanilam, G. Comparison of the Effects of Propofol and Sevoflurane Induced Burst Suppression on Cerebral Blood Flow and Oxygenation: A Prospective, Randomised, Double-Blinded Study. World NeuroSurg. 2019, 135, e427–e434. [Google Scholar] [CrossRef]
- Klein, K.U.; Fukui, K.; Schramm, P.; Stadie, A.; Fischer, G.; Werner, C.; Oertel, J.; Engelhard, K. Human cerebral microcirculation and oxygen saturation during propofol-induced reduction of bispectral index. Br. J. Anaesth. 2011, 107, 735–741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halverson, A.; Buchanan, R.; Jacobs, L.; Shayani, V.; Hunt, T.; Riedel, C.; Sackier, J. Evaluation of mechanism of increased intracranial pressure with insufflation. Surg. Endosc. 1998, 12, 266–269. [Google Scholar] [CrossRef] [PubMed]
- Sahay, N.; Sharma, S.; Bhadani, U.K.; Singh, A.; Sinha, C.; Sahay, A.; Ranjan, A.; Agarwal, M. Effect of Pneumoperitoneum and Patient Positioning on Intracranial Pressures during Laparoscopy: A Prospective Comparative Study. J. Minim. Invasive Gynecol. 2018, 25, 147–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doe, A.; Kumagai, M.; Tamura, Y.; Sakai, A.; Suzuki, K. A comparative analysis of the effects of sevoflurane and propofol on cerebral oxygenation during steep Trendelenburg position and pneumoperitoneum for robotic-assisted laparoscopic prostatectomy. J. Anesth. 2016, 30, 949–955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yonekura, H.; Hirate, H.; Sobue, K. Comparison of anesthetic management and outcomes of robot-assisted vs pure laparoscopic radical prostatectomy. J. Clin. Anesth. 2016, 35, 281–286. [Google Scholar] [CrossRef]
- Yilmaz, G.; Akca, A.; Kiyak, H.; Salihoglu, Z. Elevation in optic nerve sheath diameter due to the pneumoperitoneum and Trendelenburg is associated to postoperative nausea, vomiting and headache in patients undergoing laparoscopic hysterectomy. Minerva Anestesiol. 2020, 86, 270–276. [Google Scholar] [CrossRef]
- Uchinami, Y.; Takikawa, S.; Takashima, F.; Maeda, Y.; Nasu, S.; Ito, A.; Saito, T. Incidence of postoperative nausea and vomiting is not increased by combination of low concentration sevoflurane and propofol compared with propofol alone in patients undergoing laparoscopic gynecological surgery. JA Clin. Rep. 2019, 5, 1–5. [Google Scholar] [CrossRef]
- Lee, K.-H.; Shin, H.-S.; Jeon, Y.-H.; Kim, S.-O.; Hong, J.-G. Comparison of ondansetron with ondansetron and dexamethasone in preventing of PONV in major gynecologic surgery. Korean J. Pain 2001, 14, 76–82. [Google Scholar]
- Sneyd, J.R.; Andrews, C.J.; Tsubokawa, T. Comparison of propofol/remifentanil and sevoflurane/remifentanil for maintenance of anaesthesia for elective intracranial surgery. Br. J. Anaesth. 2005, 94, 778–783. [Google Scholar] [CrossRef] [Green Version]
- Kumar, G.; Stendall, C.; Mistry, R.; Gurusamy, K.; Walker, D. A comparison of total intravenous anaesthesia using propofol with sevoflurane or desflurane in ambulatory surgery: Systematic review and meta-analysis. Anaesthesia 2014, 69, 1138–1150. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Sevoflurane Group (n = 21) | Propofol Group (n = 21) | p |
|---|---|---|---|
| Age (years) | 44.4 ± 5.5 | 44.9 ± 6.8 | 0.805 |
| Height (cm) | 158.5 ± 4.7 | 158 ± 5.1 | 0.778 |
| Weight (kg) | 58.6 ± 6.5 | 61 ± 8.4 | 0.289 |
| Body mass index (kg/m2) | 23.2 ± 2.6 | 24.2 ± 3.3 | 0.282 |
| Hypertension | 3 (14.3) | 1 (4.8) | 0.606 |
| Diabetes mellitus | 1 (4.8) | 1 (4.8) | 1.000 |
| Operation time (min) | 140 (105–145) | 130 (120–151) | 0.791 |
| Anesthesia time (min) | 175 (145–195) | 170 (155–191) | 1.000 |
| Crystalloid amount (mL) | 1381 ± 278.6 | 1395.2 ± 327.5 | 0.880 |
| Estimated blood loss (mL) | 200 (200–300) | 200 (200–300) | 0.379 |
| Sevoflurane Group (n = 21) | Propofol Group (n = 21) | Difference in the Means | 95% CI | p | |
|---|---|---|---|---|---|
| T0 (mm) | 4.54 ± 0.38 | 4.6 ± 0.26 | −0.06 | −0.27 to 0.14 | 0.530 |
| T1 (mm) | 4.94 ± 0.41 | 4.81 ± 0.27 | 0.13 | −0.09 to 0.35 | 0.236 |
| T2 (mm) | 5.08 ± 0.47 | 4.85 ± 0.29 | 0.23 | −0.02 to 0.47 | 0.070 |
| T3 (mm) | 5.18 ± 0.38 | 4.93 ± 0.31 | 0.25 | 0.03 to 0.47 | 0.025 |
| T4 (mm) | 4.59 ± 0.39 | 4.61 ± 0.26 | −0.02 | −0.22 to 0.19 | 0.872 |
| Change in ONSD at T1 (mm) | 0.41 ± 0.26 | 0.21 ± 0.13 | 0.19 | 0.06 to 0.32 | 0.005 |
| Change in ONSD at T2 (mm) | 0.54 ± 0.30 | 0.25 ± 0.09 | 0.29 | 0.15 to 0.43 | <0.001 |
| Change in ONSD at T3 (mm) | 0.64 ± 0.23 | 0.33 ± 0.11 | 0.31 | 0.2 to 4.3 | <0.001 |
| Change in ONSD at T4 (mm) | 0.05 ± 0.13 | 0.00 ± 0.07 | 0.05 | −0.02 to 0.12 | 0.126 |
| Maximum increase from baseline (%) | 14.1 ± 5.08 | 7.17 ± 2.48 | 6.93 | 4.52 to 9.56 | <0.001 |
| Number | |||||
| Patients with ONSD over 5 mm at T0 | 2 (9.5) | 1 (4.8) | 0.549 | ||
| Patients with ONSD over 5 mm at T1 | 11 (52.4) | 8 (38.1) | 0.352 | ||
| Patients with ONSD over 5 mm at T2 | 15 (71.4) | 11 (52.4) | 0.204 | ||
| Patients with ONSD over 5 mm at T3 | 15 (71.4) | 11 (52.4) | 0.204 | ||
| Patients with ONSD over 5 mm at T4 | 4 (19) | 1 (4.8) | 0.153 |
| Sevoflurane Group (n = 21) | Propofol Group (n = 21) | p | |
|---|---|---|---|
| EtCO2 (mmHg) | |||
| T0 | 32 (32–33) | 32 (32–33) | 0.450 |
| T1 | 34 (33–34) | 34 (33–35) | 0.949 |
| T2 | 34 (34–35) | 34 (33–35) | 0.469 |
| T3 | 34 (33–35) | 34 (33–35) | 0.601 |
| T4 | 33 (32–34) | 34 (32–34) | 0.170 |
| SBP (mmHg) | |||
| T0 | 115.8 ± 18.1 | 115.7 ± 17.9 | 0.993 |
| T1 | 124.4 ± 9.8 | 129.9 ± 11.5 | 0.105 |
| T2 | 122.4 ± 12.1 | 128.2 ± 10.9 | 0.110 |
| T3 | 120.0 ± 11.1 | 128.3 ± 8.2 | 0.009 |
| T4 | 109.2 ± 11.6 | 115 ± 14.1 | 0.156 |
| MBP (mmHg) | |||
| T0 | 86.8 ± 15.1 | 84.9 ±13.8 | 0.664 |
| T1 | 97.4 ± 8.2 | 98.8 ± 8.7 | 0.588 |
| T2 | 95 ± 8.9 | 98.9 ± 8.5 | 0.165 |
| T3 | 93.8 ± 8.4 | 97.7 ± 6.8 | 0.109 |
| T4 | 82.6 ± 10.1 | 87.9 ± 11.8 | 0.128 |
| DBP (mmHg) | |||
| T0 | 67.3 ± 10.2 | 66.9 ± 12.2 | 0.913 |
| T1 | 78.9 ± 7.7 | 79.9 ± 7.2 | 0.682 |
| T2 | 77.1 ± 8.7 | 80.1 ± 8.0 | 0.259 |
| T3 | 76.1 ± 7.9 | 78.8 ± 5.4 | 0.193 |
| T4 | 64.4 ± 8.7 | 66.4 ± 9.4 | 0.468 |
| Heart rate (beats/min) | |||
| T0 | 77.2 ± 13.7 | 67.1 ± 10.9 | 0.012 |
| T1 | 68.2 ± 10.3 | 62.8 ± 8.4 | 0.071 |
| T2 | 69.4 ± 11.1 | 64.1 ± 9.5 | 0.108 |
| T3 | 68.7 ± 9.8 | 63.3 ± 9.4 | 0.074 |
| T4 | 64.4 ± 8.8 | 58.6 ± 7.8 | 0.028 |
| SPO2 (%) | |||
| T0 | 99.6 ± 0.6 | 99.4 ± 0.8 | 0.389 |
| T1 | 99.8 ± 0.4 | 99.6 ± 0.6 | 0.246 |
| T2 | 99.8 ± 0.4 | 99.6 ± 0.6 | 0.139 |
| T3 | 99.8 ± 0.4 | 99.6 ± 0.6 | 0.229 |
| T4 | 99.8 ± 0.4 | 99.9 ± 0.3 | 0.225 |
| PPV (%) | |||
| T0 | 5.1 ± 2.8 | 3.8 ± 2.6 | 0.114 |
| T1 | 6.4 ± 3.4 | 6.2 ± 2.9 | 0.846 |
| T2 | 6.0 ± 3.2 | 6.1 ± 2.3 | 0.871 |
| T3 | 6 (4–7) | 5 (4–7) | 0.909 |
| T4 | 6 (3–7) | 3 (3–7) | 0.291 |
| PAP (cmH2O) | |||
| T0 | 12 (10–13) | 13 (12–15) | 0.027 |
| T1 | 22 ± 3.9 | 23.5 ± 4 | 0.220 |
| T2 | 21.6 ± 3.8 | 23.2 ± 3.8 | 0.190 |
| T3 | 21.4 ± 4.3 | 23.7 ± 3.4 | 0.061 |
| T4 | 13.6 ± 2.6 | 14.5 ± 2.6 | 0.268 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.E.; Koh, S.Y.; Jun, I.-J. Comparison of the Effects of Propofol and Sevoflurane Anesthesia on Optic Nerve Sheath Diameter in Robot-Assisted Laparoscopic Gynecology Surgery: A Randomized Controlled Trial. J. Clin. Med. 2022, 11, 2161. https://doi.org/10.3390/jcm11082161
Kim JE, Koh SY, Jun I-J. Comparison of the Effects of Propofol and Sevoflurane Anesthesia on Optic Nerve Sheath Diameter in Robot-Assisted Laparoscopic Gynecology Surgery: A Randomized Controlled Trial. Journal of Clinical Medicine. 2022; 11(8):2161. https://doi.org/10.3390/jcm11082161
Chicago/Turabian StyleKim, Jung Eun, Seong Yoon Koh, and In-Jung Jun. 2022. "Comparison of the Effects of Propofol and Sevoflurane Anesthesia on Optic Nerve Sheath Diameter in Robot-Assisted Laparoscopic Gynecology Surgery: A Randomized Controlled Trial" Journal of Clinical Medicine 11, no. 8: 2161. https://doi.org/10.3390/jcm11082161