
Adverse Mental Health Sequelae of COVID-19 Pandemic in the Pregnant Population and Useful Implications for Clinical Practice


Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search and Study Selection
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection
2.4. Data Extraction and Investigated Variables
2.5. Quality Assessment Tool
3. Results
3.1. Characteristics of Included Studies
3.2. Quality of Included Studies
3.3. Domain 1: Social and Medical Consequences of COVID-19 in Pregnant Women Population
3.4. Domain 2: Main Psychological Factors Responsible for Adverse COVID-19 Mental Health Outcomes in Pregnant Women
3.5. Domain 3: Determination of COVID-19 Mental Health Problems Including Symptoms and Diagnosis among Pregnant Women in Different Countries
3.6. Domain 4: Influence of COVID-19 on Psychological and Medical Factors Related to Adverse Pregnancy and Offspring Development Outcomes
3.7. Domain 5: Dilemmas and Hopes in Ways to Improve the Provision of Services to Pregnant Women during Disasters, Including the COVID-19 Pandemic
4. Discussion
4.1. Useful Implications for Clinical Practice
- pregnant women should be informed of the increase in severity of COVID-19, including admission to intensive care units, need for ECMO and invasive ventilation compared with non-pregnant women, and encouraged to undertake safety measures to reduce the risk of infection, and pregnant women with preexisting comorbidities will need to be considered as a high-risk group for COVID-19 [8];
- early cord clamping may minimize the risk of viral transmission by avoiding longer, close contact with the infected mother [46], and in turn, it may increase the mother’s good feelings about the safety of the newborn;
- a positive impact on the depressive symptoms of new mothers may be achieved by providing appropriate isolation in hospitals for pregnant women [31], including. but not limited to. quarantine;
- the psychological stress of the COVID-19 pandemic during pregnancy can increase the risk of preterm delivery, low birth weight, postnatal complications, and neurodevelopmental disorders in offspring [10,25,57,58]; in some cases, a 100% reduction in ELBW infants was noted during the COVID-19 pandemic [32,33];
- a midwife should have the right and duty to order, prescribe, and administer pharmacological agents that, on a daily basis, are prescribed at the discretion of an OB/GYN specialist and must be prepared for sudden maternal cardiac arrest in a pregnant woman and to address the moral dilemma of delivering a fetus from a deceased mother’s womb [64];
- critically important are methods of supportive parenting and using techniques to downregulate arousal in time of occurred stress, and physical activity was associated with lower psychological symptoms [26];
- effective screening strategies for depressive and anxiety symptoms during the pandemic should be prioritized to allow for timely treatment [25];
- mental health specialists and other medical providers, midwives, and nurses can prevent adverse outcomes by identifying problems early (paying special attention to the group of women with adverse mental health and psychiatric symptoms, including assessing sleep patterns, sources of fear, anxiety, swinging moods, irritability, depression, worries, and suicidal ideation or its attempt), and establishing comprehensive treatment plans for pregnant women in conditions such as emergencies and the COVID-19 natural disasters [25];
- routine assessment of trauma history and psychopathology during prenatal visits is warranted to identify women at risk; abnormalities of the early bonding of mother–offspring always must be taken into consideration, if mental health impairment symptoms occur [74], and in the case of necessity, a perinatal psychiatrist should be consulted [75];
- promoting marital and relationship wellbeing may play a valuable role in anxiety control, lowering stress, and reducing depression in pregnant women [28];
- patient testing and screening should be conducted in person, while follow-up visits can be carried out via telehealth, and the recommended model allows for providers to lower the risk COVID-19 infection while maintaining a high standard of prenatal care [63];
- women who became mothers during the COVID-19 emergency appear to be at high risk for developing mental health problems [5];
- implementing community-based strategies to support resilience and psychologically vulnerable individuals during the COVID-19 crisis is fundamental for any community [77], including pregnant women;
- copying with psychological distress of the COVID-19 pandemic during pregnancy should be more recommended to prevent adverse effects on the fetal growth and neurodevelopment disorders in offspring, because maternal psychological distress (e.g., stress, anxiety, and depression) has been found as a risk factor of child or adult neurodevelopment disorders, including, but not limited to, ADHD, ASD, schizophrenia spectrum disorder, antisocial behavior, and depressive symptoms [3,55,56,57];
- observation highlights the need for increased screening and treatment for perinatal mood and anxiety disorders in the postpartum period as the COVID-19 pandemic continues [75];
- providing psychological support to pregnant and lactating women may reduce the long-term negative effects of COVID-19 pandemic [76].
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The Outbreak of COVID-19 Coronavirus and its Impact on Global Mental Health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef] [Green Version]
- Martins-Filho, P.R.; Tavares, C.; Santos, V.S. Factors Associated with Mortality in Patients with COVID-19. A Quantitative Evidence Synthesis of Clinical and Laboratory Data. Eur. J. Intern. Med. 2020, 76, 97–99. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, S.A.; Smulian, J.C.; Lednicky, J.A.; Wen, T.S.; Jamieson, D.J. Coronavirus Disease 2019 (COVID-19) and Pregnancy: What Obstetricians Need to Know. Am. J. Obstet. Gynecol. 2020, 222, 415–426. [Google Scholar] [CrossRef]
- Grumi, S.; Provenzi, L.; Accorsi, P.; Biasucci, G.; Cavallini, A.; Decembrino, L.; Falcone, R.; Fazzi, E.M.; Gardella, B.; Giacchero, R.; et al. Depression and Anxiety in Mothers Who Were Pregnant During the COVID-19 Outbreak in Northern Italy: The Role of Pandemic-Related Emotional Stress and Perceived Social Support. Front. Psychiatry 2021, 12, 716488. [Google Scholar] [CrossRef] [PubMed]
- Wróblewska-Seniuk, K.; Basiukajc, A.; Wojciechowska, D.; Telge, M.; Miechowicz, I.; Mazela, J. Clinical Characteristics of Newborns Born to Mothers with COVID-19. J. Clin. Med. 2021, 10, 4383. [Google Scholar] [CrossRef] [PubMed]
- Celewicz, A.; Celewicz, M.; Michalczyk, M.; Wozniakowska-Gondek, P.; Krejczy, K.; Misiek, M.; Rzepka, R. Pregnancy as a Risk Factor of Severe COVID-19. J. Clin. Med. 2021, 10, 5458. [Google Scholar] [CrossRef] [PubMed]
- Allotey, J.; Stallings, E.; Bonet, M.; Yap, M.; Chatterjee, S.; Kew, T.; Debenham, L.; Llavall, A.C.; Dixit, A.; Zhou, D.; et al. Clinical Manifestations, Risk Factors, and Maternal and Perinatal Outcomes of Coronavirus Disease 2019 in Pregnancy: Living Systematic Review and Meta-Analysis. BMJ 2020, 370, 1641–1647. [Google Scholar] [CrossRef]
- Trad, A.T.A.; Ibirogba, E.R.; Elrefaei, A.; Narang, K.; Tonni, G.; Picone, O.; Suy, A.; Moratonas, E.C.; Kilby, M.; Ruano, R. Complications and Outcomes of SARS-CoV-2 in Pregnancy: Where and What Is the Evidence? Hypertens. Pregnancy 2020, 39, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Weston, D.; Greenberg, N. Psychological Impact of Infectious Disease Outbreaks on Pregnant Women: Rapid Evidence Review. Public Health 2020, 189, 26–36. [Google Scholar] [CrossRef] [PubMed]
- Buekens, P.; Alger, J.; Bréart, G.; Cafferata, M.L.; Harville, E.; Tomasso, G. A Call for Action for COVID-19 Surveillance and Research during Pregnancy. Lancet Glob. Health 2020, 8, 877–878. [Google Scholar] [CrossRef]
- Orsolini, L.; Valchera, A.; Vecchiotti, R.; Tomasetti, C.; Iasevoli, F.; Fornaro, M.; De Berardis, D.; Perna, G.; Pompili, M.; Bellantuono, C. Suicide during Perinatal Period: Epidemiology, Risk Factors, and Clinical Correlates. Front. Psychiatry 2016, 7, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Field, T.; Diego, M.; Hernandez-Reif, M.; Figueiredo, B.; Deeds, O.; Ascencio, A.; Schanberg, S.; Kuhn, C. Comorbid Depression and Anxiety Effects on Pregnancy and Neonatal Outcome. Infant Behav. Dev. 2010, 33, 23–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, B.; Han, B.; Zheng, H.; Liu, H.; Zhao, T.; Wan, Y.; Cui, F. Who Is the Most Vulnerable to Anxiety at the Beginning of the COVID-19 Outbreak in China? A Cross-Sectional Nationwide Survey. Healthcare 2021, 9, 970. [Google Scholar] [CrossRef] [PubMed]
- Hessami, K.; Romanelli, C.; Chiurazzi, M.; Cozzolino, M. COVID-19 Pandemic and Maternal Mental Health: A Systematic Review and Meta-Analysis. J. Matern. Fetal Neonatal Med. 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Tomfohr-Madsen, L.M.; Racine, N.; Giesbrecht, G.F.; Lebel, C.; Madigan, S. Depression and Anxiety in Pregnancy during COVID-19: A Rapid Review and Meta-Analysis. Psychiatry Res. 2021, 300, 113912. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Wang, Y.; Xue, J.; Zhao, N.; Zhu, T. The Impact of COVID-19 Epidemic Declaration on Psychological Consequences: A Study on Active Weibo Users. Int. J. Environ. Res. Public Health 2020, 17, 2032. [Google Scholar] [CrossRef] [Green Version]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic Review or Scoping Review? Guidance for Authors When Choosing between a Systematic or Scoping Review Approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.; Shi, H.; Liu, Z.; Peng, S.; Wang, R.; Qi, L.; Li, Z.; Yang, J.; Ren, Y.; Song, X.; et al. The Prevalence of Psychiatric Symptoms of Pregnant and Non-pregnant Women during the COVID-19 Epidemic. Transl. Psychiatry 2020, 10, 319. [Google Scholar] [CrossRef] [PubMed]
- Preis, H.; Mahaffey, B.; Heiselman, C.; Lobel, M. Vulnerability and Resilience to Pandemic-Related Stress among U.S. Women Pregnant at the Start of the COVID-19 Pandemic. Soc. Sci. Med. 2020, 266, 113348. [Google Scholar] [CrossRef] [PubMed]
- Kajdy, A.; Feduniw, S.; Ajdacka, U.; Modzelewski, J.; Baranowska, B.; Sys, D.; Pokropek, A.; Pawlicka, P.; Kaźmierczak, M.; Rabijewski, M.; et al. Risk Factors for Anxiety and Depression among Pregnant Women during the COVID-19 Pandemic: A Web-Based Cross-Sectional Survey. Medicine 2020, 99, e21279. [Google Scholar] [CrossRef] [PubMed]
- Preis, H.; Mahaffey, B.; Heiselman, C.; Lobel, M. Pandemic-Related Pregnancy Stress and Anxiety among Women Pregnant during the Coronavirus Disease 2019 Pandemic. Am. J. Obstet. Gynecol. MFM 2020, 2, 100155. [Google Scholar] [CrossRef]
- Durankuş, F.; Aksu, E. Effects of the COVID-19 Pandemic on Anxiety and Depressive Symptoms in Pregnant Women: A Preliminary Study. J. Matern. Fetal Neonatal Med. 2020, 35, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ayaz, R.; Hocaoğlu, M.; Günay, T.; Yardımcı, O.D.; Turgut, A.; Karateke, A. Anxiety and Depression Symptoms in the Same Pregnant Women before and during the COVID-19 Pandemic. J. Perinat. Med. 2020, 48, 965–970. [Google Scholar] [CrossRef] [PubMed]
- Lebel, C.; MacKinnon, A.; Bagshawe, M.; Tomfohr-Madsen, L.; Giesbrecht, G. Elevated Depression and Anxiety Symptoms among Pregnant Individuals during the COVID-19 Pandemic. J. Affect. Disord. 2020, 277, 5–13. [Google Scholar] [CrossRef]
- Saccone, G.; Florio, A.; Aiello, F.; Venturella, R.; De Angelis, M.C.; Locci, M.; Bifulco, G.; Zullo, F.; Di Spiezio Sardo, A. Psychological Impact of Coronavirus Disease 2019 in Pregnant Women. Am. J. Obstet. Gynecol. 2020, 223, 293–295. [Google Scholar] [CrossRef] [PubMed]
- Effati-Daryani, F.; Zare, S.; Mohammadi, A.; Hemmati, E.; Ghasemi; Yngyknd, S.; Mirghafourvand, M. Depression, Stress, Anxiety and Their Predictors in Iranian Pregnant Women during the Outbreak of COVID-19. BMC Psychol. 2020, 8, 99. [Google Scholar] [CrossRef] [PubMed]
- Parra-Saavedra, M.; Villa-Villa, I.; Pérez-Olivo, J.; Guzman-Polania, L.; Galvis-Centurion, P.; Cumplido-Romero, Á.; Santacruz-Vargas, D.; Rivera-Moreno, E.; Molina-Giraldo, S.; Guillen-Burgos, H.; et al. Attitudes and Collateral Psychological Effects of COVID-19 in Pregnant Women in Colombia. Int. J. Gynaecol. Obstet. 2020, 151, 203–208. [Google Scholar] [CrossRef]
- Taubman-Ben-Ari, O.; Chasson, M.; Abu Sharkia, S.; Weiss, E. Distress and Anxiety Associated with COVID-19 among Jewish and Arab Pregnant Women in Israel. J. Reprod. Infant Psychol. 2020, 38, 340–348. [Google Scholar] [CrossRef] [PubMed]
- Oskovi-Kaplan, Z.A.; Buyuk, G.N.; Ozgu-Erdinc, A.S.; Keskin, H.L.; Ozbas, A.; Moraloglu Tekin, O. The Effect of COVID-19 Pandemic and Social Restrictions on Depression Rates and Maternal Attachment in Immediate Postpartum Women: A Preliminary Study. Psychiatr. Q. 2020, 92, 675–682. [Google Scholar] [CrossRef] [PubMed]
- Philip, R.K.; Purtill, H.; Reidy, E.; Daly, M.; Imcha, M.; McGrath, D.; O’Connell, N.H.; Dunne, C.P. Unprecedented Reduction in Births of Very Low Birthweight (VLBW) And Extremely Low Birthweight (ELBW) Infants during the COVID-19 Lockdown in Ire-Land: A ‘Natural Experiment’ Allowing Analysis of Data from the Prior Two Decades. BMJ Global Health 2020, 5, e003075. [Google Scholar] [CrossRef] [PubMed]
- Hedermann, G.; Hedley, P.L.; Bækvad-Hansen, M.; Hjalgrim, H.; Rostgaard, K.; Poorisrisak, P.; Breindahl, M.; Melbye, M.; Hougaard, D.M.; Christiansen, M.; et al. Danish Premature Birth Rates during the COVID-19 Lockdown. Arch. Dis. Childhood. Fetal Neonatal Ed. 2020, 106, 93–95. [Google Scholar] [CrossRef]
- Facchetti, F.; Bugatti, M.; Drera, E.; Tripodo, C.; Sartori, E.; Cancila, V.; Papaccio, M.; Castellani, R.; Casola, S.; Boniotti, M.B.; et al. SARS-CoV2 Vertical Transmission with Adverse Effects on the Newborn Revealed through Integrated Immunohistochemical, Electron Microscopy and Molecular Analyses of Placenta. EBioMedicine 2020, 59, 102951. [Google Scholar] [CrossRef] [PubMed]
- Ilska, M.; Kołodziej-Zaleska, A.; Brandt-Salmeri, A.; Preis, H.; Lobel, M. Pandemic Stress and Its Correlates among Pregnant Women during the Second Wave of COVID-19 in Poland. Int. J. Environ. Res. Public Health 2021, 18, 11140. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P.; Ga, S.W.; Zello, G.A.; Petersen, J.A. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2014. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 30 November 2021).
- Zanardo, V.; Manghina, V.; Giliberti, L.; Vettore, M.; Severino, L.; Straface, G. Psychological Impact of COVID-19 Quarantine Measures in Northeastern Italy on Mothers in the Immediate Postpartum Period. Int. J. Gynaecol. Obstet. 2020, 150, 184–188. [Google Scholar] [CrossRef]
- Esterwood, E.; Saeed, S.A. Past Epidemics, Natural Disasters, COVID19, and Mental Health: Learning from History as we Deal with the Present and Prepare for the Future. Psychiatr. Q. 2020, 91, 1121–1133. [Google Scholar] [CrossRef]
- Thapa, S.B.; Mainali, A.; Schwank, S.E.; Acharya, G. Maternal Mental Health in the Time of the COVID-19 Pandemic. Acta Obstet. Et Gynecol. Scand. 2020, 99, 817–818. [Google Scholar] [CrossRef] [PubMed]
- Caparros-Gonzalez, R.A.; Alderdice, F. The COVID-19 Pandemic and Perinatal Mental Health. J. Reprod. Infant Psychol. 2020, 38, 223–225. [Google Scholar] [CrossRef] [PubMed]
- Yassa, M.; Birol, P.; Yirmibes, C.; Usta, C.; Haydar, A.; Yassa, A.; Sandal, K.; Tekin, A.B.; Tug, N. Near-Term Pregnant Women’s Attitude Toward, Concern about and Knowledge of the COVID-19 Pandemic. J. Matern. Fetal Neonatal Med. 2020, 33, 3827–3834. [Google Scholar] [CrossRef] [PubMed]
- Okuyama, M.; Mezawa, H.; Kawai, T.; Urashima, M. Elevated Soluble PD-L1 in Pregnant Women’s Serum Suppresses the Immune Reaction. Front. Immunol. 2019, 10, 86. [Google Scholar] [CrossRef] [Green Version]
- Easterlin, M.C.; Crimmins, E.M.; Finch, C.E. Will Prenatal Exposure to SARS-CoV-2 Define a Birth Cohort with Accelerated Aging in the Century Ahead? J. Dev. Orig. Health Dis. 2020, 12, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Mehew, J.; Johnson, R.; Roberts, D.; Harvala, H. Convalescent Plasma for COVID-19: Male Gender, Older Age and Hospitalization Associated with High Neutralizing Antibody Levels, England, 22 April to 12 May 2020. Eurosurveillance 2020, 25, 2001754. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, D.J.; Rasmussen, S.A. An Update on COVID-19 and Pregnancy. Am. J. Obstet. Gynecol. 2022, 226, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.L.; Liu, Y.Y.; Wu, C.H.; Wang, C.Y.; Wang, C.H.; Long, C.Y. Impact of COVID-19 on Pregnancy. Int. J. Med. Sci. 2021, 18, 763–767. [Google Scholar] [CrossRef]
- Vivanti, A.J.; Vauloup-Fellous, C.; Prevot, S.; Zupan, V.; Suffee, C.; Do Cao, J.; Benachi, A.; De Luca, D. Transplacental Transmission of SARS-CoV-2 Infection. Nat. Commun. 2020, 11, 3572. [Google Scholar] [CrossRef]
- Sharps, M.C.; Hayes, D.; Lee, S.; Zou, Z.; Brady, C.A.; Almoghrabi, Y.; Kerby, A.; Tamber, K.K.; Jones, C.J.; Adams Waldorf, K.M.; et al. A Structured Review of Placental Morphology and Histopathological Lesions Associated with SARS-CoV-2 Infection. Placenta 2020, 101, 13–29. [Google Scholar] [CrossRef]
- Van Bavel, J.J.; Baicker, K.; Boggio, P.S.; Capraro, V.; Cichocka, A.; Cikara, M.; Crockett, M.J.; Crum, A.J.; Douglas, K.M.; Druckman, J.N.; et al. Using Social and Behavioural Science to Support COVID-19 Pandemic Response. Nat. Hum. Behav. 2020, 4, 460–471. [Google Scholar] [CrossRef] [PubMed]
- Van der Zee-van den Berg, A.I.; Boere-Boonekamp, M.M.; Groothuis-Oudshoorn, C.; Reijneveld, S.A. The Edinburgh Postpartum Depression Scale: Stable Structure but Subscale of Limited Value to Detect Anxiety. PLoS ONE 2019, 14, e0221894. [Google Scholar] [CrossRef] [Green Version]
- Berthelot, N.; Lemieux, R.; Garon-Bissonnette, J.; Drouin-Maziade, C.; Martel, É.; Maziade, M. Uptrend in Distress and Psychiatric Symptomatology in Pregnant Women during the Coronavirus Disease 2019 Pandemic. Acta Obstet. Et Gynecol. Scand. 2020, 99, 848–855. [Google Scholar] [CrossRef]
- Wong, S.F.; Chow, K.M.; Leung, T.N.; Ng, W.F.; Ng, T.K.; Shek, C.C.; Ng, P.C.; Lam, P.W.; Ho, L.C.; To, W.W.; et al. Pregnancy and Perinatal Outcomes of Women with Severe Acute Respiratory Syndrome. Am. J. Obstet. Gynecol. 2004, 191, 292–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alfaraj, S.H.; Al-Tawfiq, J.A.; Memish, Z.A. Middle East Respiratory Syndrome Coronavirus (MERS-CoV) Infection during Pregnancy: Report of Two Cases and Review of the Literature. J. Microbiol. Immunol. Infect. 2019, 52, 501–503. [Google Scholar] [CrossRef] [PubMed]
- Ming-Zhu, Y.; Lijuan, Z.; Guangtong, D.; Chaofei, H.; Minxue, S.; Hongyin, S.; Furong, Z.; Wei, Z.; Lan, C.; Qingqing, L.; et al. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection During Pregnancy in China: A Retrospective Cohort Study. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Scheinost, D.; Sinha, R.; Cross, S.N.; Kwon, S.H.; Sze, G.; Constable, R.T.; Ment, L.R. Does Prenatal Stress Alter the Developing Connectome? Pediatric Res. 2017, 81, 214–226. [Google Scholar] [CrossRef] [Green Version]
- Fatima, M.; Srivastav, S.; Mondal, A.C. Prenatal Stress and Depression Associated Neuronal Development in Neonates. Int. J. Dev. Neurosci. 2017, 60, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Abdoli, A.; Falahi, S.; Kenarkoohi, A.; Shams, M.; Mir, H.; Jahromi, M. The COVID-19 Pandemic, Psychological Stress during Pregnancy, and Risk of Neurodevelopmental Disorders in Offspring: A Neglected Consequence. J. Psychosom. Obstet. Gynaecol. 2020, 41, 247–248. [Google Scholar] [CrossRef] [PubMed]
- Castro, P.; Narciso, C.; Matos, A.P.; Werner, H.; Araujo Júnior, E. Pregnant, Uninfected, Stressed, and Confined in the COVID-19 Period: What Can We Expect in the near Future? Revista da Associacao Medica Brasileira 2020, 66, 386–387. [Google Scholar] [CrossRef] [PubMed]
- Shoib, S.; Arafat, S.; Ahmad, W. Perinatal Mental Health in Kashmir, India during the COVID-19 Pandemic. Matern. Child Health J. 2020, 24, 1365–1366. [Google Scholar] [CrossRef] [PubMed]
- Ceulemans, M.; Verbakel, J.Y.; Van Calsteren, K.; Eerdekens, A.; Allegaert, K.; Foulon, V. SARS-CoV-2 Infections and Impact of the COVID-19 Pandemic in Pregnancy and Breastfeeding: Results from an Observational Study in Primary Care in Belgium. Int. J. Environ. Res. Public Health 2020, 17, 6766. [Google Scholar] [CrossRef] [PubMed]
- Implementing Telehealth in Practice. ACOG Committee Opinion Summary, Number 798. Obstet. Gynecol. 2020, 135, 493–494. [Google Scholar] [CrossRef] [PubMed]
- Rad, S.; Smith, D.; Malish, T.; Jain, V. SMFM Coding White Paper: Interim Coding Guidance: Coding for Telemedicine and Remote Patient Monitoring Services during the COVID-19 Pandemic. Soc. Matern. Fetal Med. 2020. Available online: https://www.smfm.org/covid-19-white-paper (accessed on 19 January 2022).
- Jakubowski, D.; Sys, D.; Kajdy, A.; Lewandowska, R.; Kwiatkowska, E.; Cymbaluk-Płoska, A.; Rabijewski, M.; Torbé, A.; Kwiatkowski, S. Application of Telehealth in Prenatal Care during the COVID-19 Pandemic—A Cross-Sectional Survey of Polish Women. J. Clin. Med. 2021, 10, 2570. [Google Scholar] [CrossRef] [PubMed]
- Mazurkiewicz, D.W.; Piechocka, D.I.; Miela, R.; Koniecko, K.; Sawka, J.H.; Strzelecka, J. A New Challenge for Midwives and Medical Doctors in Time of the Threat of a Mass Terrorist Attack and a Life-Threatening Mass Disaster. Prog. Health Sci. 2018, 8, 181–193. [Google Scholar] [CrossRef]
- Coelho, C.M.; Suttiwan, P.; Arato, N.; Zsido, A.N. On the Nature of Fear and Anxiety Triggered by COVID-19. Front. Psychol. 2020, 11, 581314. [Google Scholar] [CrossRef] [PubMed]
- Janik, K.; Cwalina, U.; Iwanowicz-Palus, G.; Cybulski, M. An Assessment of the Level of COVID-19 Anxiety among Pregnant Women in Poland: A Cross-Sectional Study. J. Clin. Med. 2021, 10, 5869. [Google Scholar] [CrossRef]
- Witteveen, D.; Velthorst, E. Economic Hardship and Mental Health Complaints during COVID-19. Proc. Natl. Acad. Sci. USA 2020, 117, 27277–27284. [Google Scholar] [CrossRef] [PubMed]
- Takubo, Y.; Tsujino, N.; Aikawa, Y.; Fukiya, K.; Iwai, M.; Uchino, T.; Ito, M.; Akiba, Y.; Mizuno, M.; Nemoto, T. Psychological Impacts of the COVID-19 Pandemic on One-Month Postpartum Mothers in a Metropolitan Area of Japan. BMC Pregnancy Childbirth 2021, 21, 845. [Google Scholar] [CrossRef]
- Choi, K.W.; Kim, H.H.; Basu, A.; Kwong, A.S.F.; Hernandez-Diaz, S.; Wyszynski, D.F.; Koenen, K.C. COVID-19 Perceived Impacts on Sleep, Fitness, and Diet and Associations with Mental Health during Pregnancy: A Cross-National Study. J. Affect. Disord. Rep. 2022, 7, 100288. [Google Scholar] [CrossRef] [PubMed]
- Fryer, K.; Delgado, A.; Foti, T.; Reid, C.N.; Marshall, J. Implementation of Obstetric Telehealth During COVID-19 and beyond. Matern. Child Health J. 2020, 24, 1104–1110. [Google Scholar] [CrossRef] [PubMed]
- Aryal, S.; Pant, S.B. Maternal Mental Health in Nepal and Its Prioritization during COVID-19 Pandemic: Missing the Obvious. Asian J. Psychiatry 2020, 54, 102281. [Google Scholar] [CrossRef] [PubMed]
- Martins-Filho, P.R.; Tanajura, D.M.; Santos, H.P., Jr.; Santos, V.S. COVID-19 during Pregnancy: Potential Risk for Neurodevelopmental Disorders in Neonates? Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 250, 255–256. [Google Scholar] [CrossRef] [PubMed]
- Shatri, H.; Faisal, E.; Putranto, R. Mass Panic Disaster Management in COVID-19 Pandemic. Acta Medica Indones. 2020, 52, 179–184. [Google Scholar]
- Lehnig, F.; Nagl, M.; Stepan, H.; Wagner, B.; Kersting, A. Associations of Postpartum Mother-Infant Bonding with Maternal Childhood Maltreatment and Postpartum Mental Health: A Cross-Sectional Study. BMC Pregnancy Childbirth 2019, 19, 278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, C.; Okeke, J.C.; Levitan, R.D.; Murphy, K.E.; Foshay, K.; Lye, S.J.; Knight, J.A.; Matthews, S.G. Evaluating Depression and Anxiety throughout Pregnancy and after Birth: Impact of the COVID-19 Pandemic. Am. J. Obstet. Gynecol. MFM 2022, 4, 100605. [Google Scholar] [CrossRef]
- Demissie, D.B.; Bitew, Z.W. Mental Health Effect of COVID-19 Pandemic among Women Who Are Pregnant and/or Lactating: A Systematic Review and Meta-Analysis. SAGE Open Med. 2021, 9, 20503121211026195. [Google Scholar] [CrossRef]
- Serafini, G.; Parmigiani, B.; Amerio, A.; Aguglia, A.; Sher, L.; Amore, M. The Psychological Impact of COVID-19 on the Mental Health in the General Population. QJM Mon. J. Assoc. Physicians 2020, 113, 531–537. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Aim of Study | Country | Sample Size | Study Design and Assessment Tool | Study Summary Benefits | Limitations | Study Quality |
|---|---|---|---|---|---|---|
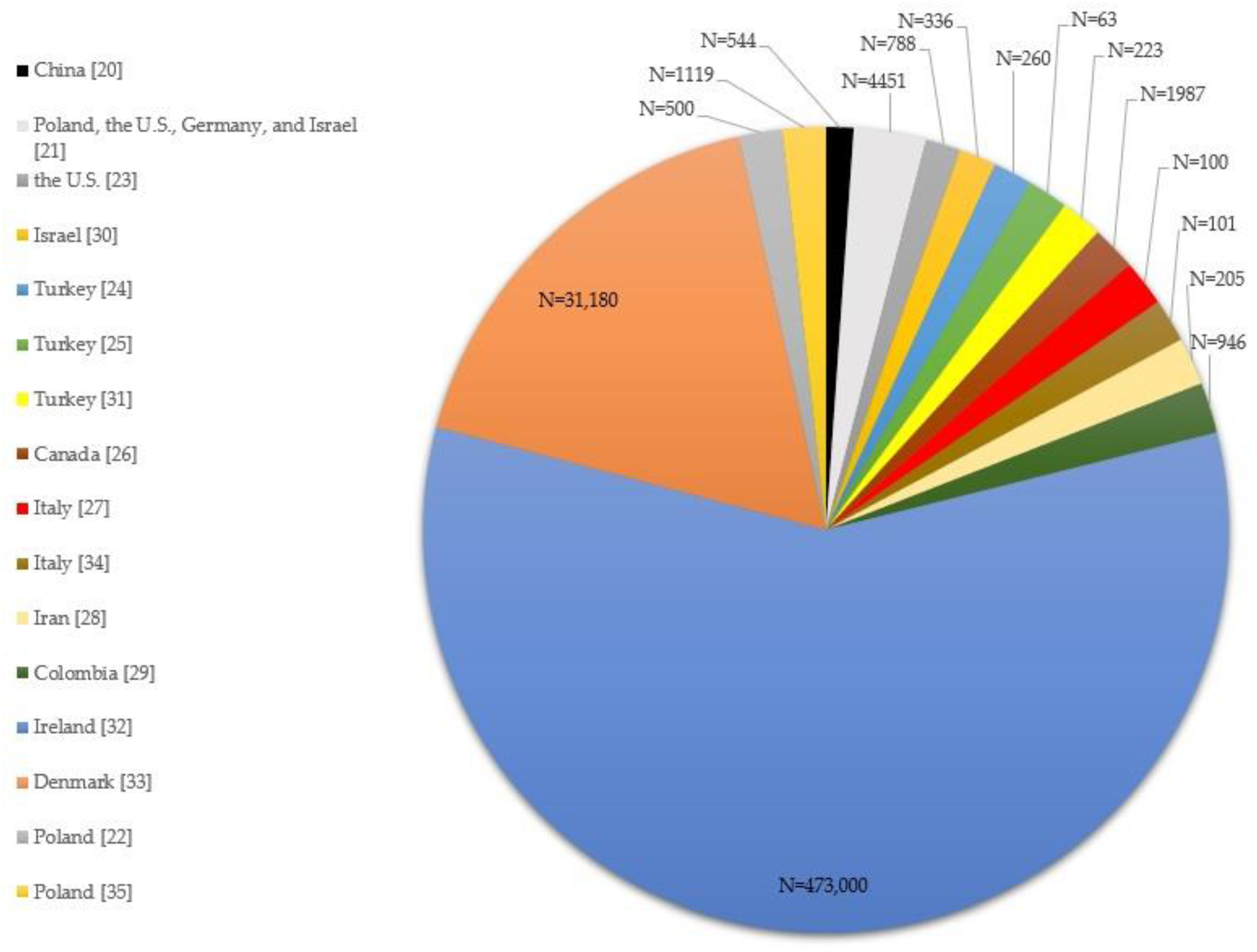
| Prevalence of psychiatric symptoms of pregnant and non-pregnant women during the COVID-19 epidemic (Zhou et al., 2020) [20] | China | N = 544 pregnant; n = 315 nonpregnant. | Cross-sectional study: used social media application; online patient health questionnaire (PHQ-9); generalized anxiety disorder scale (GAD-7); somatization subscale of the symptom checklist 90 (SCL-90); insomnia severity index (ISI); post-traumatic stress disorder checklist-5 (PCL-5). | Pregnant women have an advantage of facing mental problems caused by COVID-19, showing fewer depression, anxiety, insomnia, and PTSD symptoms than nonpregnant women do. | Lacks longitudinal follow-up, limiting the generalization of findings to other regions; No data on psychological interventions for pregnant women. | 8/10 |
| Vulnerability and resilience to pandemic-related stress among U.S. woman pregnant at the start of the COVID-19 pandemic (Preis et al., 2020.a.) [21] | U.S. | N = 4451 | Cross-sectional study: secure online software survey Questionnaire. The Pandemic-Related Pregnancy Stress Scale (PREPS). | Two major pandemic-related stress domains for pregnant women in Poland, the U.S., Germany, Israel: fears of perinatal COVID-19 infection, and being unprepared for birth. | Excluded women without access to the Internet and social media. | 7/10 |
| Risk factors for anxiety and depression among pregnant women during the COVID-19 pandemic: web-based cross-sectional survey (Kajdy et al., 2020) [22] | Poland | N = 500 | Web-based cross-sectional survey: GAD-7; PHQ-9. Available in 15 languages. | Pregnant women are worried about the COVID-19 pandemic and have difficulty in accessing professional medical help; feel insecure about exposure risk to the coronavirus when accessing medical facilities; infection of the infant in the peripartum period; financial problems lead to conflict in the family; a single mother may be more prone to anxiety isolation, fear of being trapped and rumors spreading on social media, growing anxiety and social panic; fear of blame, guilt and stigmatization related to being infected with COVID-19. | Survey may reach more women of a higher socioeconomic status and from larger agglomerations. | 9/10 |
| Pandemic-related pregnancy stress and anxiety among women pregnant during the coronavirus disease 2019 pandemic. (Preis et al., 2020.b.) [23] | U.S. | N = 788 | Cross-sectional study: social media to complete online questionnaire GAD-7; PREPS. | COVID-19 pandemic-related stress predicts heightened anxiety in women pregnant during this crisis: preparation for birth; worries about COVID-19 infection to self and baby. | Inclusion criteria: pregnant at the time of questionnaire completion and older than 18 years; exclusion was inability to read or write English. | 8/10 |
| Effects of the COVID-19 pandemic on anxiety and depressive symptoms in pregnant women: preliminary study. (Durankuş and Aksu, 2020) [24] | Turkey | N = 260 out of 318 | Cross-sectional study: online questionnaire survey study EPDS-Edinburgh Postpartum Depression Scale. | Urgent need to provide psychosocial support to this population during the crisis. Adverse events may otherwise occur during pregnancy, and thus affect both mother and fetus. | Survey was administered online, thus preventing a face-to-face evaluation of participants; authors used their own created questionnaire on the pandemic, and its psychological effects were subjective. | 6/10 |
| Anxiety and depression symptoms in the same pregnant women before and during the COVID-19 pandemic (Ayaz et al., 2020) [25] | Turkey | N = 63 | Cross-sectional study: Beck Anxiety Inventory (BAI) questionnaire; Depression and Anxiety Symptoms II (IDAS II) questionnaire. | Depressive and anxiety symptoms were significantly increased during the SARS-CoV-2 pandemic compared with pre-pandemic surveys. Effective screening strategies for depression and anxiety symptoms during the pandemic should be prioritized to allow for timely treatment. | Sample size, but power analysis indicated that the effect of this limitation was reduced. | 3/10 |
| Elevated depression and anxiety symptoms among pregnant individuals during the COVID-19 pandemic (Lebel et al., 2020) [26] | Canada | N = 1987 <35 weeks gestation | Cross-sectional study: Online survey of standardized measures of depression, anxiety, pregnancy-related anxiety, and social support. EPDS; PROMIS Anxiety Adult 7-item short form; social support effectiveness questionnaire (SSEQ); interpersonal support evaluation list (ISEL); Godin-Shephard Leisure-Time Exercise Questionnaire. | Elevated anxiety and depression symptoms that may have a long-term impact on offspring related to COVID-19 worries about threats to their own lives, their baby’s health, not getting enough prenatal care, and social isolation. | Inclusion criteria: living in Canada, able to read and write English, and having a confirmed pregnancy <35 weeks gestation. | 9/10 |
| Psychological impact of coronavirus disease 2019 in pregnant women (Saccone et al., 2020) [27] | Italy | N = 100 | Cross-sectional study: Event Scale-Revised (IES-R) questionnaire; Spielberger State-Trait Anxiety Inventory (STAI); visual analog scale (VAS). | Psychological impact and anxiety of the COVID-19 epidemic found be more severe in women who are in the first trimester of pregnancy during the outbreak; high anxiety regarding the vertical transmission of the disease was reported by almost half of the respondents. | Findings from the study were limited by the single-center study design and small sample size. | 5/10 |
| Depression, stress, anxiety, and their predictors in Iranian pregnant women during the outbreak of COVID-19 (Effati-Daryani et al., 2020) [28] | Iran | N = 205 | Online descriptive–analytical cross-sectional study; Depression, Anxiety and Stress Scale 21 (DASS-21). | Promoting marital life satisfaction and socioeconomic status can play an effective role in controlling anxiety, and reducing stress and depression in pregnant women. | Those who had a mobile phone with Internet connection could participate in this study. | 7/10 |
| Attitudes and collateral psychological effects of COVID-19 in pregnant women in Colombia (Parra-Saavedra et al., 2020) [29] | Colombia | N = 946 out of 1021 | Cross-sectional web survey. | Rate of psychological consequences of the pandemic was much larger than the number of patients clinically affected by the virus, with symptoms of anxiety, insomnia, and depression. | Excluded women without access to the Internet and social media. | 8/10 |
| Distress and anxiety associated with COVID-19 among Jewish and Arab pregnant women in Israel. (Taubman-Ben-Ari et al., 2020) [30] | Israel | N = 336 comprising 225 Jewish and 111 Arab pregnant women | Cross-sectional study: social media to complete online questionnaire. Mental Health Inventory- Short Form based on the original MHI. | COVID-19-related anxieties were quite high, especially in Arab women, with concern over the health of the fetus, public transportation and place, being infected themselves, and the delivery of the baby. | Cannot be considered representative of population of pregnant women in Israel, questionnaire only in Hebrew. | 6/10 |
| The effect of COVID-19 pandemic and social restrictions on depression rates and maternal attachment in immediate postpartum women: a preliminary study. (Oskovi-Kaplan et al., 2020) [31] | Turkey | N = 223 | Cross-sectional study: EPDS and Maternal Attachment Inventory (MAI). | Positive impact on the depressive symptoms of new mothers may have providing appropriate isolation in hospitals; psychological status of pregnant and postpartum women may help in the improvement of psychosocial support. | Lack of a control group that was evaluated before the onset of pandemic and due to ongoing cases with a high incidence; a lack of any validated questionnaire for COVID-19 infection on psychological status. | 7/10 |
| Unprecedented reduction in births of very low birthweight (VLBW) and extremely low birthweight (ELBW) infants during the COVID-19 lockdown in Ireland: a ‘natural experiment’ allowing analysis of data from the prior two decades. (Philip et al., 2020) [32] | Ireland | N = 473,000 | Descriptive cohort study: VON international benchmarking; labor ward weekly statistics for live and stillbirths; early pregnancy assessment unit (EPAU) statistics for early pregnancy loss/miscarriage information; inpatient ward statistics for early or late fetal loss during hospital admission. | 100% reduction in ELBW infants was noted in one designated health region of Ireland from January to April 2020 compared with the preceding 20 years. | Retrospective nature of birth cohort data from one health region of Ireland; completion of the study prior to the official finish of lockdown; 3. ELBW cohort analyzed with the small number of births. | 8/10 |
| Danish premature birth rates during the COVID-19 lockdown. (Hedermann et al., 2020) [33] | Denmark | N = 31,180 live singleton infants | Cross-sectional study; Nationwide prevalence proportion study with premature births as cases, term pregnancies as controls, and birth during lockdown from 12 March to 14 April 2015–2020. | Lockdowns (e.g., reduced infection load and reduced physical activity) are possibly beneficial for reducing extreme prematurity and potentially reducing infant mortality; a nonsignificant but slightly increased number of very premature births. | Study summary benefits data need to be confirmed in other countries. | 8/10 |
| SARS-CoV-2 vertical transmission with adverse effects on the newborn revealed through integrated immunohistochemical, electron microscopy and molecular analyses of Placenta. (Facchetti et al., 2020) [34] | Italy | N = 101 | Cross-sectional study; Research: comprehensive immunohistochemical and immune- fluorescence analysis: RNA-in situ hybridization and RT-PCR for S transcripts, and by electron microscopy. | First evidence for maternal–fetal transmission of SARS-CoV-2, likely propagated by circulating virus-infected fetal mononuclear cells. | No limitation reported. | 9/10 |
| Pandemic stress and its correlates among pregnant women during the second wave of COVID-19 in Poland (Ilska et al., 2021) [35] | Poland | N = 1119 | Cross-sectional study design, online survey; PREPS. | 38.5% of participants reported high preparedness stress; 26% reported high perinatal infection stress, pregnant women are most vulnerable to pandemic-related stress. | Excluded women who had no access to the Internet or social media. | 8/10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazurkiewicz, D.W.; Strzelecka, J.; Piechocka, D.I. Adverse Mental Health Sequelae of COVID-19 Pandemic in the Pregnant Population and Useful Implications for Clinical Practice. J. Clin. Med. 2022, 11, 2072. https://doi.org/10.3390/jcm11082072
Mazurkiewicz DW, Strzelecka J, Piechocka DI. Adverse Mental Health Sequelae of COVID-19 Pandemic in the Pregnant Population and Useful Implications for Clinical Practice. Journal of Clinical Medicine. 2022; 11(8):2072. https://doi.org/10.3390/jcm11082072
Chicago/Turabian StyleMazurkiewicz, Dariusz Wojciech, Jolanta Strzelecka, and Dorota Izabela Piechocka. 2022. "Adverse Mental Health Sequelae of COVID-19 Pandemic in the Pregnant Population and Useful Implications for Clinical Practice" Journal of Clinical Medicine 11, no. 8: 2072. https://doi.org/10.3390/jcm11082072