
Comparative Longitudinal Analysis of Malignant Transformation in Pleomorphic Adenoma and Recurrent Pleomorphic Adenoma

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Collection of Clinical Data
2.3. Pathological Analyses
2.4. Statistical Analyses
3. Results
3.1. Subject Characteristics
3.2. Pathology Analyses
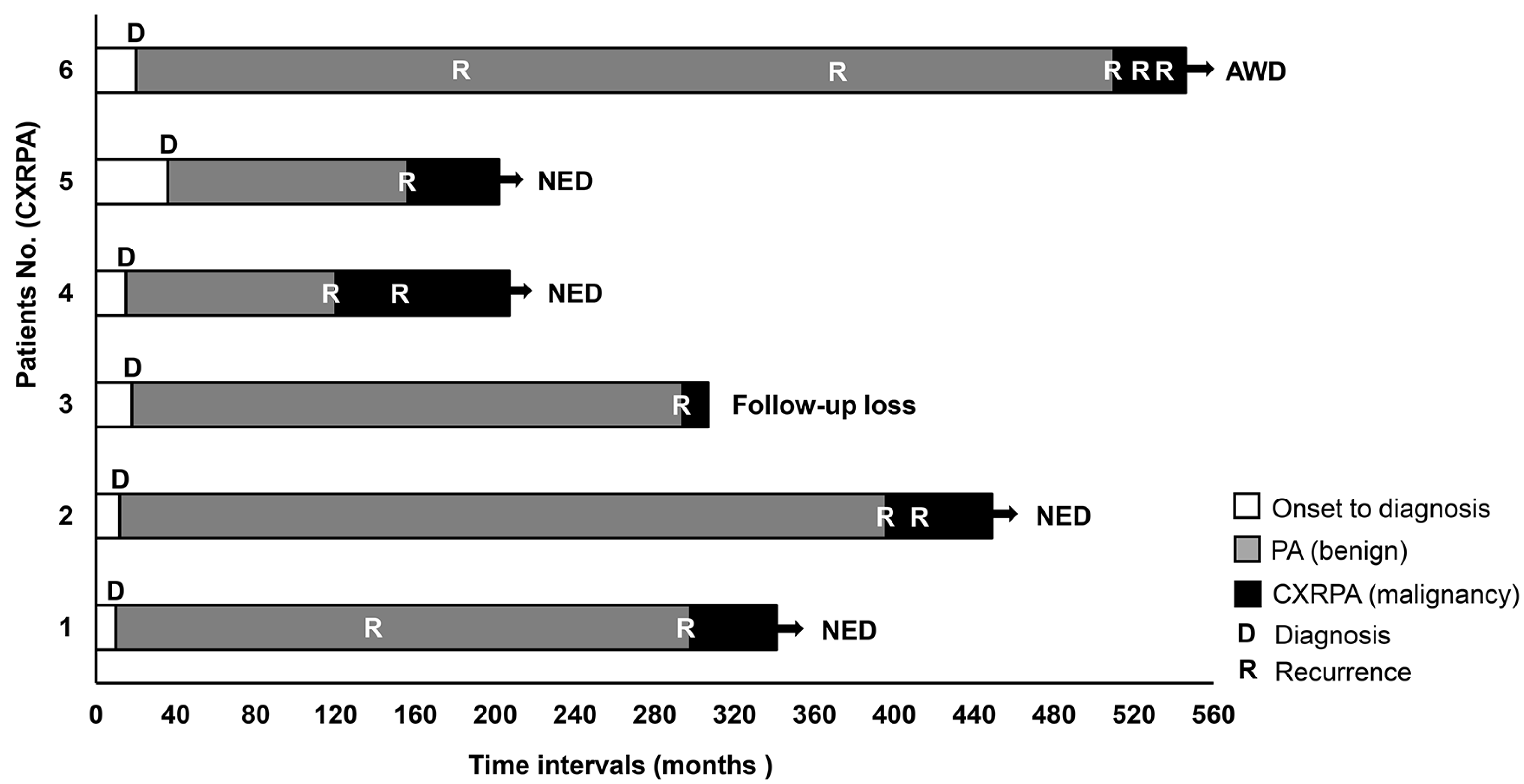
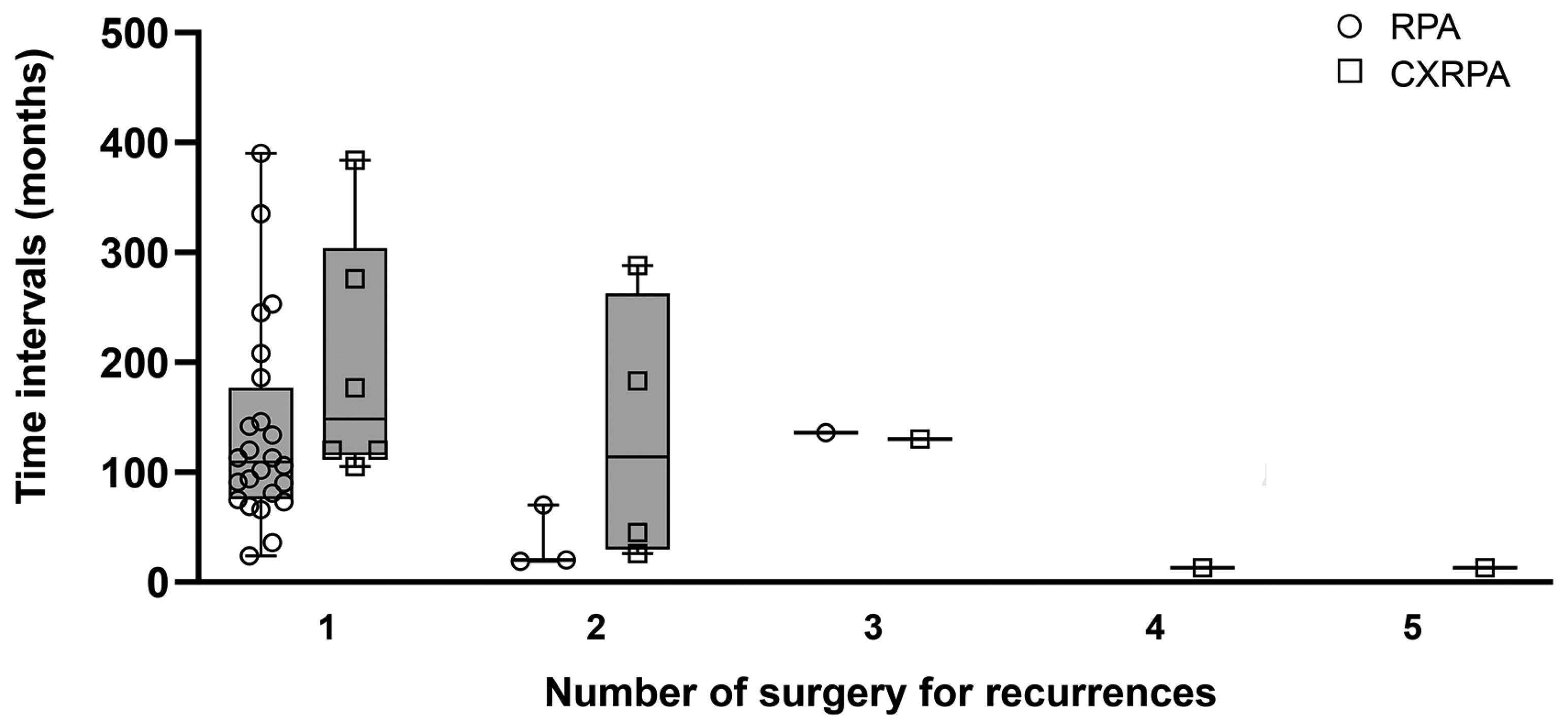
3.3. Longitudinal Time–Event Sequences of Recurrence or Malignant Transformation
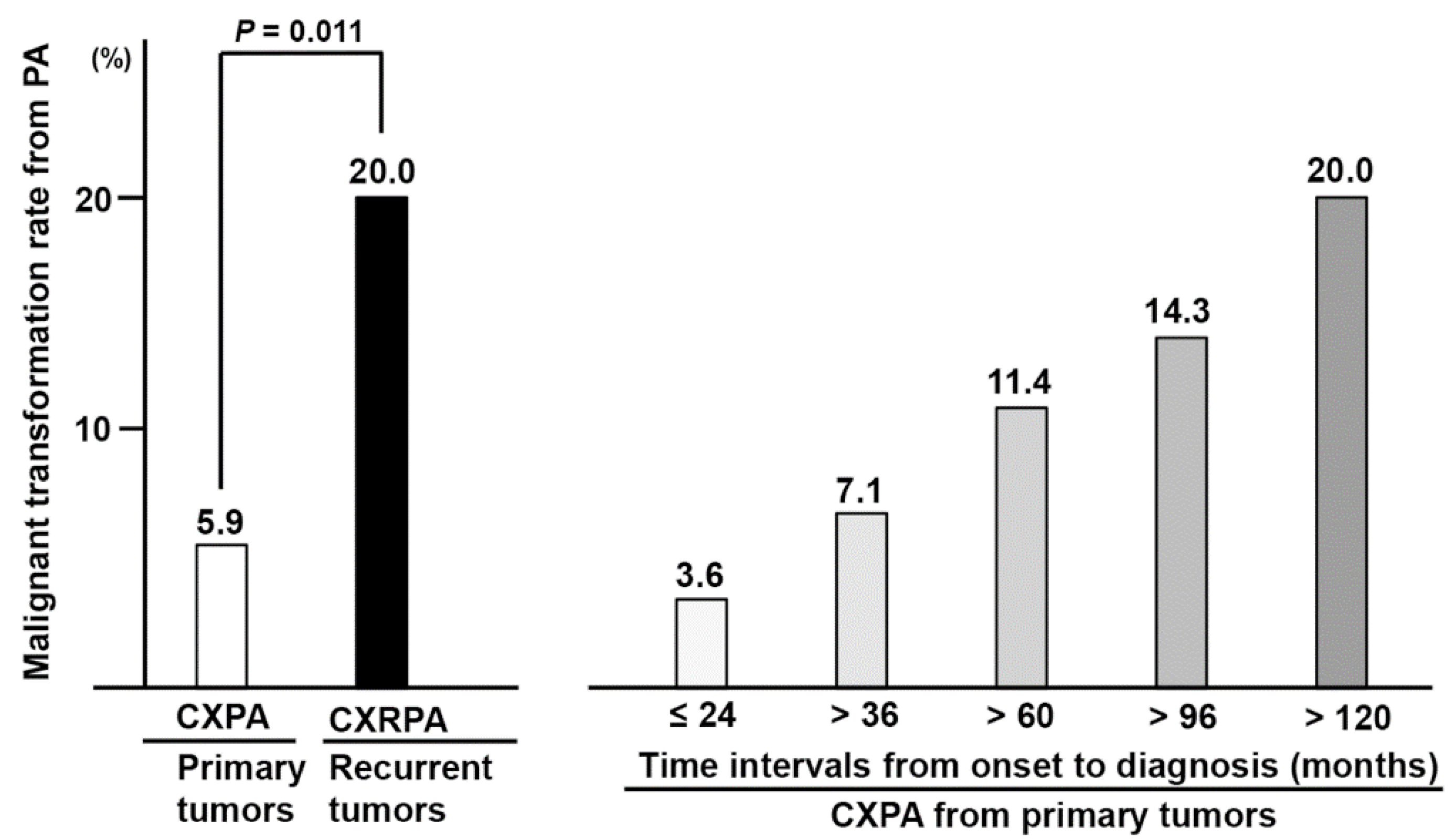
3.4. Overall and Adjusted Rates of Malignant Transformation in Underlying PA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Luers, J.C.; Wittekindt, C.; Streppel, M.; Guntinas-Lichius, O. Carcinoma ex pleomorphic adenoma of the parotid gland. Study and implications for diagnostics and therapy. Acta Oncol. 2009, 48, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Spiro, R.H. The management of salivary neoplasms: An overview. Auris Nasus Larynx 1985, 12 (Suppl. S2), S122–S127. [Google Scholar] [CrossRef]
- Rice, D.H. Salivary gland disorders. Neoplastic and nonneoplastic. Med. Clin. N. Am. 1999, 83, 197–218. [Google Scholar] [CrossRef]
- Kim, J.W.; Kwon, G.Y.; Roh, J.L.; Choi, S.H.; Nam, S.Y.; Kim, S.Y.; Cho, K.J. Carcinoma ex pleomorphic adenoma of the salivary glands: Distinct clinicopathologic features and immunoprofiles between subgroups according to cellular differentiation. J. Korean Med. Sci. 2011, 26, 1277–1285. [Google Scholar] [CrossRef]
- Colella, G.; Cannavale, R.; Chiodini, P. Meta-analysis of surgical approaches to the treatment of parotid pleomorphic adenomas and recurrence rates. J. Craniomaxillofac. Surg. 2015, 43, 738–745. [Google Scholar] [CrossRef]
- Valstar, M.H.; de Ridder, M.; van den Broek, E.C.; Stuiver, M.M.; van Dijk, B.A.C.; van Velthuysen, M.L.F.; Balm, A.J.M.; Smeele, L.E. Salivary gland pleomorphic adenoma in the Netherlands: A nationwide observational study of primary tumor incidence, malignant transformation, recurrence, and risk factors for recurrence. Oral. Oncol. 2017, 66, 93–99. [Google Scholar] [CrossRef]
- Bradley, P.J. The recurrent pleomorphic adenoma conundrum. Curr. Opin. Otolaryngol. Head Neck Surg. 2018, 26, 134–141. [Google Scholar] [CrossRef]
- Stennert, E.; Wittekindt, C.; Klussmann, J.P.; Arnold, G.; Guntinas-Lichius, O. Recurrent pleomorphic adenoma of the parotid gland: A prospective histopathological and immunohistochemical study. Laryngoscope 2004, 114, 158–163. [Google Scholar] [CrossRef]
- Dulguerov, P.; Todic, J.; Pusztaszeri, M.; Alotaibi, N.H. Why Do Parotid Pleomorphic Adenomas Recur? A Systematic Review of Pathological and Surgical Variables. Front. Surg. 2017, 4, 26. [Google Scholar] [CrossRef] [Green Version]
- Antony, J.; Gopalan, V.; Smith, R.A.; Lam, A.K. Carcinoma ex pleomorphic adenoma: A comprehensive review of clinical, pathological and molecular data. Head Neck Pathol. 2012, 6, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Phillips, P.P.; Olsen, K.D. Recurrent pleomorphic adenoma of the parotid gland: Report of 126 cases and a review of the literature. Ann. Otol. Rhinol. Laryngol. 1995, 104, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Mariano, F.V.; Giovanetti, K.; Saccomani, L.F.; Del Negro, A.; Kowalski, L.P.; Krepischi, A.C.; Altemani, A. Carcinoma ex-pleomorphic adenoma derived from recurrent pleomorphic adenoma shows important difference by array CGH compared to recurrent pleomorphic adenoma without malignant transformation. Braz. J. Otorhinolaryngol. 2016, 82, 687–694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andreasen, S.; Therkildsen, M.H.; Bjorndal, K.; Homoe, P. Pleomorphic adenoma of the parotid gland 1985–2010: A Danish nationwide study of incidence, recurrence rate, and malignant transformation. Head Neck 2016, 38 (Suppl. S1), E1364–E1369. [Google Scholar] [CrossRef]
- Valstar, M.H.; Andreasen, S.; Bhairosing, P.A.; McGurk, M. Natural history of recurrent pleomorphic adenoma: Implications on management. Head Neck 2020, 42, 2058–2066. [Google Scholar] [CrossRef] [PubMed]
- El-Naggar, A.K.; Chan, J.K.C.; Grandis, J.R.; Takata, T.; Slootweg, P.J. WHO Classification of Head and Neck Tumours, 4th ed.; World Health Organization: Lyon, France, 2017; pp. 159–201. [Google Scholar]
- Lydiatt, W.M.; Mukherji, S.K.; O’Sullivan, B.; Patel, S.G.; Shah, J.P. Major salivary glands. In AJCC Cancer Staging Manual, 8th ed.; Amin, M.B., Edge, S.B., Eds.; Springer: New York, NY, USA, 2017; pp. 95–101. [Google Scholar]
- Seethala, R.R.; Stenman, G. Update from the 4th Edition of the World Health Organization Classification of Head and Neck Tumours: Tumors of the Salivary Gland. Head Neck Pathol. 2017, 11, 55–67. [Google Scholar] [CrossRef] [Green Version]
- Seethala, R.R. An update on grading of salivary gland carcinomas. Head Neck Pathol. 2009, 3, 69–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seifert, G.; Langrock, I.; Donath, K. A pathological classification of pleomorphic adenoma of the salivary glands (author’s transl). HNO 1976, 24, 415–426. [Google Scholar]
- Satpathy, Y.; Spadigam, A.E.; Dhupar, A.; Syed, S. Epithelial and stromal patterns of pleomorphic adenoma of minor salivary glands: A histopathological and histochemical study. J. Oral. Maxillofac. Pathol. 2014, 18, 379–385. [Google Scholar] [CrossRef] [Green Version]
- Di Palma, S.; Guzzo, M. Malignant myoepithelioma of salivary glands: Clinicopathological features of ten cases. Virchows Arch. A Pathol. Anat. Histopathol. 1993, 423, 389–396. [Google Scholar] [CrossRef]
- Olsen, K.D.; Lewis, J.E. Carcinoma ex pleomorphic adenoma: A clinicopathologic review. Head Neck 2001, 23, 705–712. [Google Scholar] [CrossRef]
- Lewis, J.E.; Olsen, K.D.; Sebo, T.J. Carcinoma ex pleomorphic adenoma: Pathologic analysis of 73 cases. Hum. Pathol. 2001, 32, 596–604. [Google Scholar] [CrossRef] [PubMed]
- Wakasaki, T.; Kubota, M.; Nakashima, Y.; Tomonobe, E.; Mihara, T.; Fukushima, J. Invasive myoepithelial carcinoma ex pleomorphic adenoma of the major salivary gland: Two case reports. BMC Cancer 2016, 16, 827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffith, C.C.; Thompson, L.D.; Assaad, A.; Purgina, B.M.; Lai, C.; Bauman, J.E.; Weinreb, I.; Seethala, R.R.; Chiosea, S.I. Salivary duct carcinoma and the concept of early carcinoma ex pleomorphic adenoma. Histopathology 2014, 65, 854–860. [Google Scholar] [CrossRef] [PubMed]
- Bhardwaj, M.; Gupta, P. Dedifferentiated adenoid cystic carcinoma ex pleomorphic adenoma of the parotid. J. Cancer Res. Ther. 2018, 14, 706–708. [Google Scholar]
- McGregor, A.D.; Burgoyne, M.; Tan, K.C. Recurrent pleomorphic salivary adenoma—The relevance of age at first presentation. Br. J. Plast. Surg. 1988, 41, 177–181. [Google Scholar] [CrossRef]
- Suh, M.W.; Hah, J.H.; Kwon, S.K.; Jung, Y.H.; Kwon, T.K.; Kim, K.H.; Sung, M.W. Clinical manifestations of recurrent parotid pleomorphic adenoma. Clin. Exp. Otorhinolaryngol. 2009, 2, 193–197. [Google Scholar] [CrossRef]
- Bradley, P.J. Recurrent pleomorphic adenoma. In Salivary Gland Disorders; Myers, E.N., Ferris, R.L., Eds.; Springer: Berlin, Heidelberg, 2007; pp. 267–277. [Google Scholar]
- Altemani, A.; Martins, M.T.; Freitas, L.; Soares, F.; Araujo, N.S.; Araujo, V.C. Carcinoma ex pleomorphic adenoma (CXPA): Immunoprofile of the cells involved in carcinomatous progression. Histopathology 2005, 46, 635–641. [Google Scholar] [CrossRef]
- LiVolsi, V.A.; Perzin, K.H. Malignant mixed tumors arising in salivary glands. I. Carcinomas arising in benign mixed tumors: A clinicopathologic study. Cancer 1977, 39, 2209–2230. [Google Scholar] [CrossRef]
- Ihrler, S.; Weiler, C.; Hirschmann, A.; Sendelhofert, A.; Lang, S.; Guntinas-Lichius, O.; Arnold, G.; Zietz, C.; Harrison, J.D. Intraductal carcinoma is the precursor of carcinoma ex pleomorphic adenoma and is often associated with dysfunctional p53. Histopathology 2007, 51, 362–371. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| No. Patients | PA (n = 386) | RPA (n = 24) | p-Value | CXPA (n = 24) | CXRPA (n = 6) | p-Value |
|---|---|---|---|---|---|---|
| Age at diagnosis (years, median, IQR) | 47.0 (35.0–57.0) | 38.0 (31.0–49.0) | 0.044 | 58.5 (47.0–72.0) | 50.5 (43.0–58.0) | 0.139 |
| Sex (M:F, No.,%) | 149:237 (38.6:61.4) | 9:15 (37.5:62.5) | 0.914 | 19:5 (79.2:20.8) | 6:0 | 0.229 |
| Sites of tumor origin (No.) | PG: 386 | PG: 24 | PG: 24 | PG: 5 Lacrimal gland: 1 | ||
| No. of surgery | n = 386 | n = 28 | n = 21 | n = 10 | ||
| Tumor size (max. diameter) (cm, median, IQR) | 2.4 (1.8–3.0) | 1.5 (1.0–2.6) | 0.001 | 2.8 (2.0–4.0) | 3.2 (2.8–3.8) | 0.514 |
| Multiplicity (single vs. multiple, No.,%) | 381:5 (98.7:1.3) | 14:14 (50.0:50.0) | <0.001 | 18:3 | 7:3 | 0.223 |
| * TNM staging | T1-2N0M0 = 13, T3-4N0M0 = 6, T3-4N(+)M0 = 2, M1 = 3 | T1-2N0M0 = 4, T3-4N0M0 = 2, T3-4N(+)M0 = 3 M1 = 1 | ||||
| Surgery (conservative: wide resection, No., %) | 373:13 (96.6:3.4) | 22:6 (78.6:21.4) | 0.001 | 10:11 (47.6:52.4) | 1:9 (10.0:90.0) | 0.055 |
| Postoperative facial weakness (>6 months) (No.,%) | 10 (2.6) | 7 (25.0) | <0.001 | 1 (4.8) | 5 (50.0) | 0.007 |
| Adjuvant radiation (No., %) | 15 (62.5) | 6 (60.0) | >0.999 |
| No. (%) | Pathology Subtypes or Carcinoma Component | Tumor Grade | Pathology Features |
|---|---|---|---|
| PA (n = 30) | * Type 1 = 23 (76.7) Type 2 = 4 (13.3) Type 3 = 3 (10.0) Type 4 = 0 | Incomplete capsule = 0 Satellite nodule = 1 (3.3) Positive resection margin = 1 (3.3) | |
| RPA (n = 24) | * Type 1 = 17 (70.8) Type 2 = 5 (20.8) Type 3 = 2 (8.3) Type 4 = 0 | Incomplete capsule = 2 (8.3) Satellite nodule = 14 (58.3) Positive resection margin = 6/28 surgeries (21.4) | |
| CXPA (n = 24) | Salivary duct carcinoma = 10 (41.7), (Non-invasive type = 3) Adenocarcinoma NOS = 6 (25.0), Myoepithelial carcinoma = 4 (16.7), Adenoid cystic carcinoma = 1 (4.2), Mucoepidermoid carcinoma = 1 (4.2), Unknown = 2 (8.3) | High-grade = 8 (33.3), Low-grade = 14 (58.3), Unknown = 2 (8.3) | Infiltrative border = 9 (37.5) Pushing border = 13 (54.1) Unknown = 2 (8.3) |
| CXRPA (n = 6) | Adenocarcinoma NOS = 3 (50.0), Salivary duct carcinoma = 2 (33.3), Myoepithelial carcinoma = 1 (16.7) | High-grade = 3 (50.0), Low-grade = 3 (50.0), | Infiltrative border = 5 (83.3) Unknown = 1 (16.7) |
| Time Intervals (Months, Median, IQR) | PA (n = 386) | RPA (n = 24) | CXPA (n = 24) | CXRPA (n = 6) | p-Value |
|---|---|---|---|---|---|
| Onset to the 1st diagnosis | 12.0 (4.0–24.0) | 11.0 (2.0–15.0) | 8.0 (2.0–42.0) | 16.5 (12.8–19.5) | NS |
| Onset to recurrence (benign) | 109.5 (79.5–156.0) (1) | 148.5 (134.3–162.8) | NS | ||
| Onset to malignant transformation | 8.0 (2.0–42.0) (2) | 342.0 (190.5–394.5) (3) | (1) vs. (3): p = 0.003 (2) vs. (3): p = 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, S.Y.; Choi, J.; Hwang, I.; Cho, J.; Ko, Y.-H.; Jeong, H.-S. Comparative Longitudinal Analysis of Malignant Transformation in Pleomorphic Adenoma and Recurrent Pleomorphic Adenoma. J. Clin. Med. 2022, 11, 1808. https://doi.org/10.3390/jcm11071808
Choi SY, Choi J, Hwang I, Cho J, Ko Y-H, Jeong H-S. Comparative Longitudinal Analysis of Malignant Transformation in Pleomorphic Adenoma and Recurrent Pleomorphic Adenoma. Journal of Clinical Medicine. 2022; 11(7):1808. https://doi.org/10.3390/jcm11071808
Chicago/Turabian StyleChoi, Sung Yong, Jaehyuck Choi, Inwoo Hwang, Junhun Cho, Young-Hyeh Ko, and Han-Sin Jeong. 2022. "Comparative Longitudinal Analysis of Malignant Transformation in Pleomorphic Adenoma and Recurrent Pleomorphic Adenoma" Journal of Clinical Medicine 11, no. 7: 1808. https://doi.org/10.3390/jcm11071808