
Inhalative Treatment of Laryngitis Sicca in Patients with Sjögren’s Syndrome—A Pilot Study

 , ,
, ,
Abstract
:1. Introduction
2. Study Design and Methods
2.1. Study Population
2.2. Outcome Parameters
- -
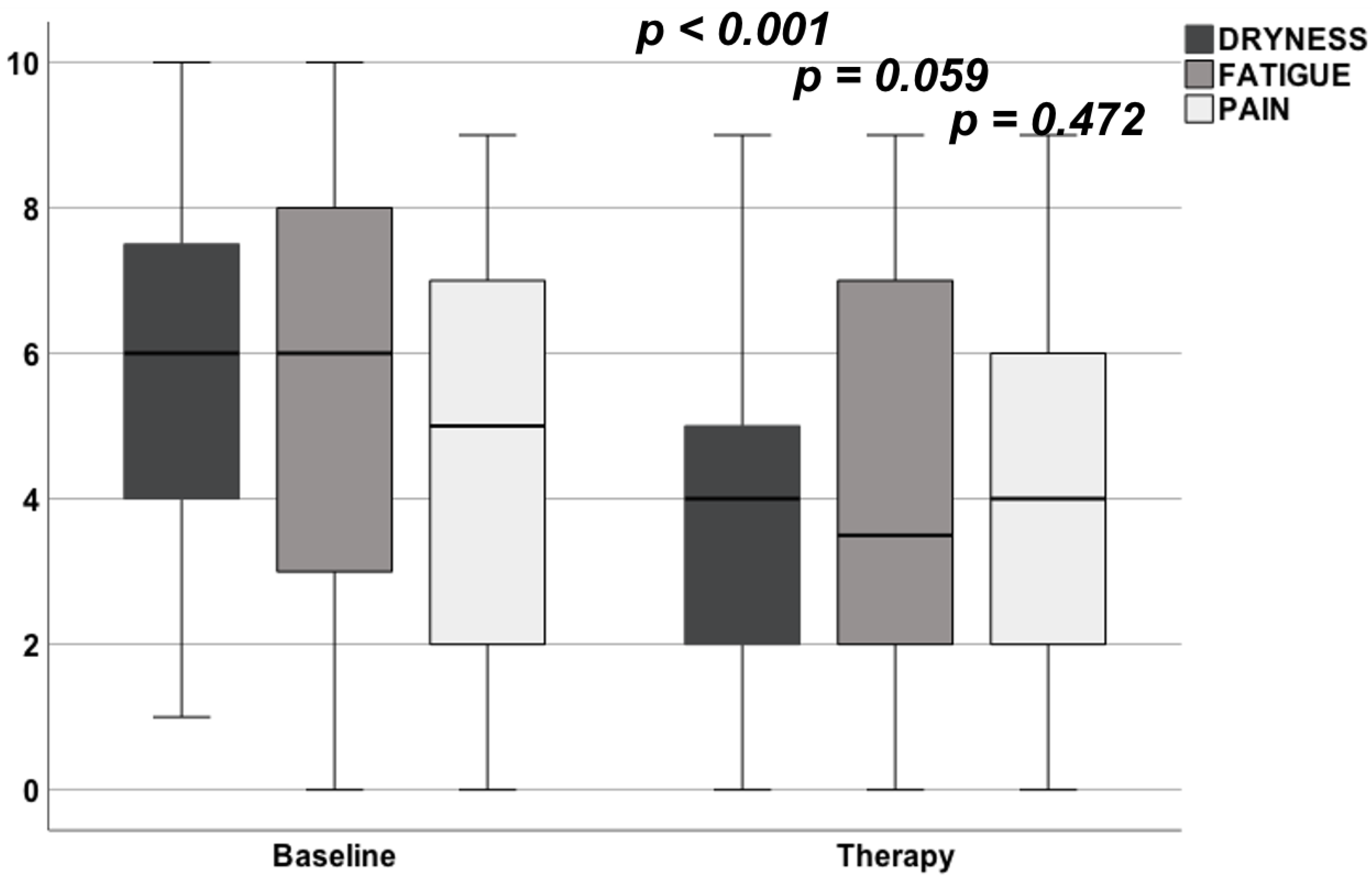
- ESSPRI: The EULAR SS patient reported index was completed by the patients. This index contains the variables of pain, fatigue and dryness and are scored by the patients in between a range of 0 and 10, the final score is the mean of the three single items [15].
- -
- EORTC QLQ H&N 35: The quality of life questionnaire of the European Organization for Research and Treatment of Cancer incorporates nine multi-item scales, five functional scales (physical, role, cognitive, emotional and social), three symptom scales (fatigue, pain and nausea/vomiting) and a global health and quality of life scale [16].
- -
- ADI: The Anderson Dysphagia Inventory consists of 20 questions from the global, emotional, functional and physical domains. Each question can be scored 1 to 5 points. A value of less than 55 is considered “highly noticeable”, 55–70 as “rather noticeable” and greater than 70 “not noticeable” [17].
- -
- VHI: The Voice Handicap Index measures voice-related impairment of the quality of life in the functional, physical and emotional dimension. VHI values of 0–11 are classified as grade 0 (almost certainly no noticeable grade of suffering), values of 12–28 a grade 1 (more likely unnoticeable than conspicuous grade of suffering), values of 29–56 as grade 2 (more probably noticeable suffering than not) and values of 57–120 as grade 3 (certainly noticeable) [18,19].
- -
- Unstimulated whole salivary flow (UWSF) was measured at baseline and after the treatment period.
- -
- Head and neck high-resolution B-mode sonography using a 9–14 MHz linear transducer (Acuson S2000, Siemens Healthcare, Erlangen, Germany) was performed for all patients in order to assess glandular morphology. To evaluate the glandular stiffness, the glandular shear wave velocity was evaluated applying virtual touch tissue quantification in a technique described in detail previously [20].
- -
- Side effects of the inhalative treatment were documented.
2.3. Inhalative Agent
2.4. Statistical Analysis
3. Results
3.1. Study Population
3.2. Effect on Subjective Parameters
3.3. Effect on UWSF and Sonographic Parameter
3.4. Therapy Adherence
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hofauer, B.; Chaker, A.; Thurmel, K.; Knopf, A. Manifestations of autoimmune disorders in otorhinolaryngology: Classical symptoms and diagnostic approach. HNO 2017, 65, 695–708. [Google Scholar] [CrossRef] [PubMed]
- Knopf, A.; Bas, M.; Chaker, A.; Strassen, U.; Pickhard, A.; Stark, T.; Thürmel, K. Rheumatic disorders affecting the head and neck: Underestimated diseases. Rheumatology 2011, 50, 2029–2034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brito-Zeron, P.; Baldini, C.; Bootsma, H.; Bowman, S.J.; Jonsson, R.; Mariette, X.; Ramos-Casals, M. Sjogren syndrome. Nat. Rev. Dis. Primers. 2016, 2, 16047. [Google Scholar] [CrossRef] [PubMed]
- Brito-Zerón, P.; Acar-Denizli, N.; Ng, W.-F.; Horváth, I.F.; Rasmussen, A.; Seror, R.; Li, X.; Baldini, C.; Gottenberg, J.-E.; Danda, D.; et al. Epidemiological profile and north-south gradient driving baseline systemic involvement of primary Sjogren’s syndrome. Rheumatology 2020, 59, 2350–2359. [Google Scholar] [CrossRef] [Green Version]
- Brito-Zerón, P.; Acar-Denizli, N.; Zeher, M.; Rasmussen, A.; Seror, R.; Theander, E.; Ramos-Casals, M. Influence of geolocation and ethnicity on the phenotypic expression of primary Sjogren’s syndrome at diagnosis in 8310 patients: A cross-sectional study from the Big Data Sjogren Project Consortium. Ann. Rheum. Dis. 2017, 76, 1042–1050. [Google Scholar] [CrossRef]
- Fox, R.I.; Stern, M.; Michelson, P. Update in Sjogren syndrome. Curr. Opin. Rheumatol. 2000, 12, 391–398. [Google Scholar] [CrossRef]
- Retamozo, S.; Acar-Denizli, N.; Rasmussen, A.; Horváth, I.F.; Baldini, C.; Priori, R.; Sandhya, P.; Hernandez-Molina, G.; Armagan, B.; Praprotnik, S.; et al. Systemic manifestations of primary Sjogren’s syndrome out of the ESSDAI classification: Prevalence and clinical relevance in a large international, multi-ethnic cohort of patients. Clin. Exp. Rheumatol. 2019, 37 (Suppl. 118), 97–106. [Google Scholar]
- Graf, S.; Kirschstein, L.; Knopf, A.; Mansour, N.; Jeleff-Wölfler, O.; Buchberger AM, S.; Hofauer, B. Systematic evaluation of laryngeal impairment in Sjogren’s syndrome. Eur. Arch. Otorhinolaryngol. 2021, 278, 2421–2428. [Google Scholar] [CrossRef]
- Ogut, F.; Midilli, R.; Oder, G.; Engin, E.Z.; Karci, B.; Kabasakal, Y. Laryngeal findings and voice quality in Sjogren’s syndrome. Auris Nasus Larynx 2005, 32, 375–380. [Google Scholar] [CrossRef]
- Ramos-Casals, M.; Brito-Zerón, P.; Bombardieri, S.; Bootsma, H.; De Vita, S.; Dörner, T.; Fisher, B.A.; Gottenberg, J.-E.; Hernandez-Molina, G.; Kocher, A.; et al. EULAR recommendations for the management of Sjogren’s syndrome with topical and systemic therapies. Ann. Rheum. Dis. 2020, 79, 3–18. [Google Scholar] [CrossRef] [Green Version]
- Hofauer, B.; Bas, M.; Manour, N.; Knopf, A. Liposomal local therapy as treatment for sicca symptoms in patients with primary Sjogren’s syndrome. HNO 2013, 61, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Hofauer, B.; Straßen, U.; Chaker, A.; Schossow, B.; Wirth, M.; Wirth, M.; Knopf, A. Liposomal Inhalation after Tracheostomy-A Randomized Controlled Trial. J. Clin. Med. 2021, 10, 3312. [Google Scholar] [CrossRef] [PubMed]
- Shiboski, C.H.; Shiboski, S.C.; Seror, R.; Criswell, L.A.; Labetoulle, M.; Lietman, T.M.; Rasmussen, A.; Scofield, H.; Vitali, C.; Bowman, S.J.; et al. 2016 American College of Rheumatology/European League Against Rheumatism classification criteria for primary Sjogren’s syndrome: A consensus and data-driven methodology involving three international patient cohorts. Ann. Rheum. Dis. 2017, 76, 9–16. [Google Scholar] [CrossRef]
- Seror, R.; Theander, E.; Brun, J.G.; Ramos-Casals, M.; Valim, V.; Dörner, T.; Bootsma, H.; Tzioufas, A.; Solans-Laqué, R.; Mandl, T.; et al. Validation of EULAR primary Sjogren’s syndrome disease activity (ESSDAI) and patient indexes (ESSPRI). Ann. Rheum. Dis. 2015, 74, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Seror, R.; Bootsma, H.; Saraux, A.; Bowman, S.J.; Theander, E.; Brun, J.G.; Baron, G.; Le Guern, V.; Devauchelle-Pensec, V.; Ramos-Casals, M.; et al. Defining disease activity states and clinically meaningful improvement in primary Sjogren’s syndrome with EULAR primary Sjogren’s syndrome disease activity (ESSDAI) and patient-reported indexes (ESSPRI). Ann. Rheum. Dis. 2016, 75, 382–389. [Google Scholar] [CrossRef]
- Bjordal, K.; Hammerlid, E.; Ahlner-Elmqvist, M.; de Graeff, A.; Boysen, M.; Evensen, J.F.; Biörklund, A.; de Leeuw, J.R.; Fayers, P.M.; Jannert, M.; et al. Quality of life in head and neck cancer patients: Validation of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-H&N35. J. Clin. Oncol. 1999, 17, 1008–1019. [Google Scholar]
- Bauer, F.; Seiss, M.; Grassel, E.; Stelzle, F.; Klotz, M.; Rosanowski, F. Swallowing-related quality of life in oral cavity cancer. The German version of the Anderson Dysphagia Inventory. HNO 2010, 58, 692–697. [Google Scholar] [CrossRef]
- Grassel, E.; Hoppe, U.; Rosanowski, F. Grading of the Voice Handicap Index. HNO 2008, 56, 1221–1228. [Google Scholar] [CrossRef]
- Nawka, T.; Wiesmann, U.; Gonnermann, U. Validation of the German version of the Voice Handicap Index. HNO 2003, 51, 921–930. [Google Scholar] [CrossRef]
- Knopf, A.; Hofauer, B.; Thürmel, K.; Meier, R.; Stock, K.; Bas, M.; Manour, N. Diagnostic utility of Acoustic Radiation Force Impulse (ARFI) imaging in primary Sjoegren`s syndrome. Eur. Radiol. 2015, 25, 3027–3034. [Google Scholar] [CrossRef]
- Tanner, K.; Pierce, J.L.; Merrill, R.M.; Miller, K.L.; Kendall, K.A.; Roy, N. The Quality of Life Burden Associated with Voice Disorders in Sjogren’s Syndrome. Ann. Otol. Rhinol. Laryngol. 2015, 124, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Ruiz Allec, L.D.; Hernandez Lopez, X.; Arreguin Porras, J.B.; Velasco Ramos, R.; Pacheco del Valle, J.C.; Perez Garcia, A.I. Alterations in voice, speech and swallowing in patients with Sjogren’s syndrome. Acta Otorrinolaringol. Esp. 2011, 62, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Heiser, C.; Hofauer, B.; Scherer, E.; Schukraft, J.; Knopf, A. Liposomal treatment of xerostomia, odor, and taste abnormalities in patients with head and neck cancer. Head Neck 2016, 38 (Suppl. 1), E1232–E1237. [Google Scholar] [CrossRef] [PubMed]
- Park, E.H.; Ha, Y.J.; Kang, E.H.; Song, Y.W.; Scofield, R.H.; Lee, Y.J. Baseline disease activity influences subsequent achievement of patient acceptable symptom state in Sjögren’s syndrome. Rheumatology 2021, 60, 2714–2724. [Google Scholar] [CrossRef] [PubMed]
- Hofauer, B.; Mansour, N.; Heiser, C.; Strassen, U.; Bas, M.; Knopf, A. Effect of liposomal local therapy on salivary glands in acoustic radiation force impulse imaging in Sjogren’s syndrome. Clin. Rheumatol. 2016, 35, 2597–2601. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Age (years) | 58.2 ± 15.6 |
| Gender (%female) | 90 |
| Disease duration (years) | 7.1 ± 5.4 |
| Keratoconjunctivitis sicca (% positive) | 86 |
| Xerostomia (% positive) | 89 |
| Schirmer’s test (% positive) | 43 |
| Histopathology (% positive) | 71 |
| UWSF (% positive) | 96 |
| Antibodies to Ro (SS-A) (% positive) | 48 |
| Antibodies to La (SS-B) (% positive) | 29 |
| ESSDAI | 7.0 ± 8.5 |
| ESSPRI | 5.1 ± 2.0 |
| Parameter | Baseline | Therapy | p-Value |
|---|---|---|---|
| Xerostomia | 30.3 ± 15.3 | 26.9 ± 15.2 | 0.066 |
| ADI | 65.6 ± 11.6 | 66.5 ± 12.0 | 0.583 |
| VHI | 16.0 ± 19.6 | 15.7 ± 15.5 | 0.614 |
| EORTC QLQ H&N 35 | 53.8 ± 10.3 | 50.9 ± 9.2 | 0.063 |
| Parameter | Baseline | Therapy | p-Value |
|---|---|---|---|
| ESSPRI | 5.0 ± 2.1 | 4.1 ± 2.4 | 0.012 |
| Dryness | 5.7 ± 2.1 | 4.1 ± 2.4 | <0.001 |
| Fatigue | 5.0 ± 3.0 | 4.1 ± 3.0 | 0.059 |
| Pain | 4.6 ± 2.4 | 4.2 ± 2.8 | 0.472 |
| Parameter | Baseline | Therapy | p-Value |
|---|---|---|---|
| UWSF (mL/5 min) | 0.65 ± 0.57 | 0.70 ± 0.64 | 0.500 |
| SWV PG (m/s) | 1.89 ± 0.53 | 1.89 ± 0.43 | 0.987 |
| SWV SMG (m/s) | 1.72 ± 0.44 | 1.64 ± 0.40 | 0.336 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hofauer, B.; Kirschstein, L.; Graf, S.; Strassen, U.; Johnson, F.; Zhu, Z.; Knopf, A. Inhalative Treatment of Laryngitis Sicca in Patients with Sjögren’s Syndrome—A Pilot Study. J. Clin. Med. 2022, 11, 1081. https://doi.org/10.3390/jcm11041081
Hofauer B, Kirschstein L, Graf S, Strassen U, Johnson F, Zhu Z, Knopf A. Inhalative Treatment of Laryngitis Sicca in Patients with Sjögren’s Syndrome—A Pilot Study. Journal of Clinical Medicine. 2022; 11(4):1081. https://doi.org/10.3390/jcm11041081
Chicago/Turabian StyleHofauer, Benedikt, Lara Kirschstein, Simone Graf, Ulrich Strassen, Felix Johnson, Zhaojun Zhu, and Andreas Knopf. 2022. "Inhalative Treatment of Laryngitis Sicca in Patients with Sjögren’s Syndrome—A Pilot Study" Journal of Clinical Medicine 11, no. 4: 1081. https://doi.org/10.3390/jcm11041081