
Cardiac Glycosides Lower C-Reactive Protein Plasma Levels in Patients with Decompensated Heart Failure: Results from the Single-Center C-Reactive Protein-Digoxin Observational Study (C-DOS)

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Controls/Comparators
2.3. Inclusion and Exclusion Criteria, Patient Characteristics
2.4. Outcome Measures
2.5. Methods against Bias
2.6. Sample Size/Power Calculations
2.7. Feasibility of Treatment
2.8. Statistical Analysis
3. Results
3.1. Baseline Patient Characteristics, Medication Follow-Up and Drop-Outs
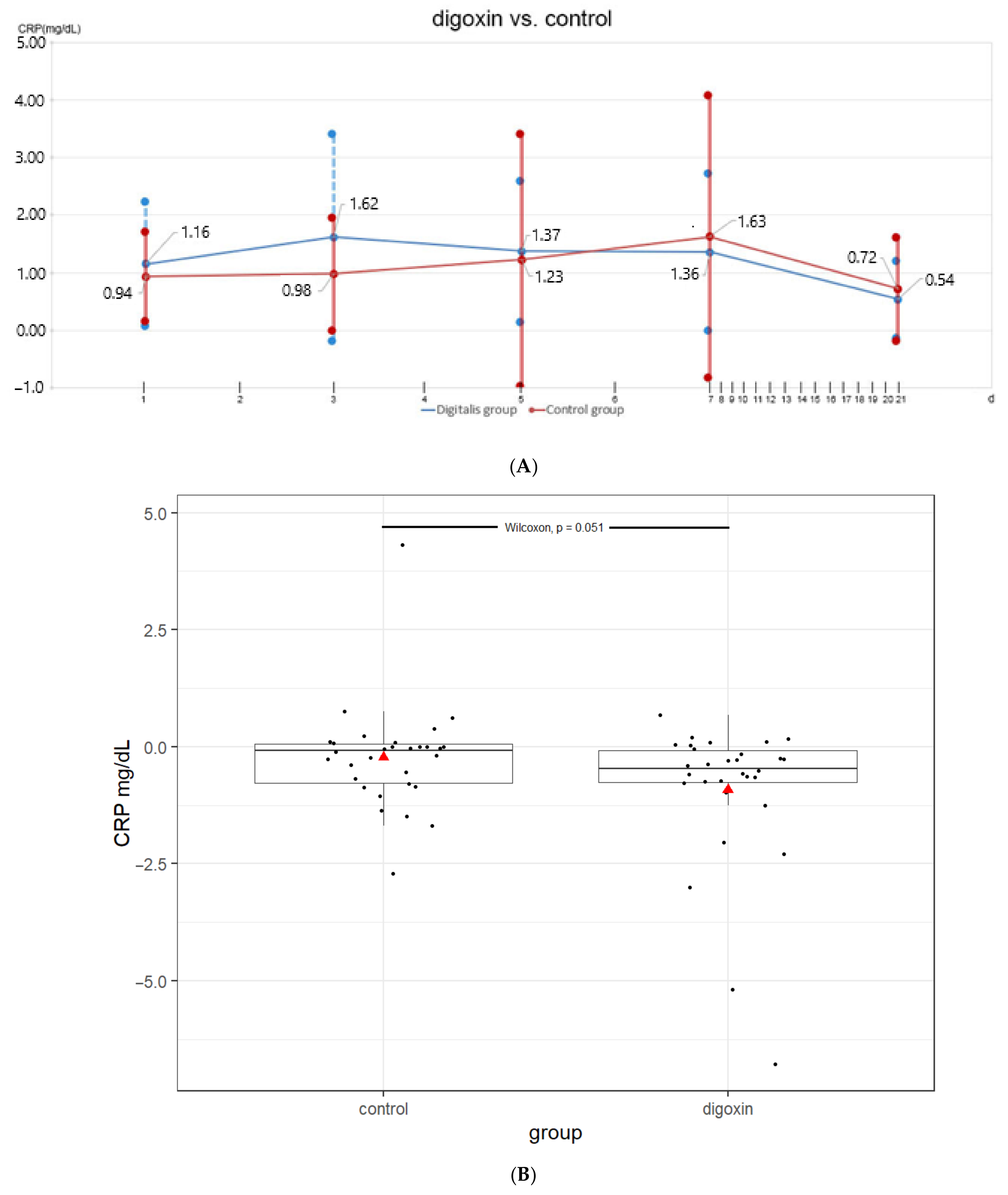
3.2. CRP Levels in the Digoxin Versus Control Group
4. Discussion
4.1. Limitiations
4.2. Possible Implications
4.3. Context of C-DOS
4.4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pearson, T.A.; Mensah, G.A.; Alexander, R.W.; Anderson, J.L.; Cannon, R.O.; Criqui, M.; Fadl, Y.Y.; Fortmann, S.P.; Hong, Y.; Myers, G.L.; et al. Markers of inflammation and cardiovascular disease: Application to clinical and public health practice: A statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation 2003, 107, 499–511. [Google Scholar] [CrossRef] [PubMed]
- Torzewski, J. C-reactive protein and atherogenesis: New insights from established animal models. Am. J. Pathol. 2005, 167, 923–925. [Google Scholar] [CrossRef]
- Pepys, M.B. C-reactive protein is neither a marker nor a mediator of atherosclerosis. Nat. Clin. Pract. Nephrol. 2008, 4, 234–235. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, G.D.; Vance, R.P. C-reactive protein immunohistochemical localization in normal and atherosclerotic human aortas. Arch. Pathol. Lab. Med. 1987, 111, 265–269. [Google Scholar] [PubMed]
- Torzewski, J.; Torzewski, M.; Bowyer, D.E.; Fröhlich, M.; Koenig, W.; Waltenberger, J.; Fitzsimmons, C.; Hombach, V. C-reactive protein frequently colocalizes with the terminal complement complex in the intima of early atherosclerotic lesions of human coronary arteries. Arterioscler. Thromb. Vasc. Biol. 1998, 18, 1386–1392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasojima, K.; Schwab, C.; McGeer, E.G.; McGeer, P.L. Generation of C-reactive protein and complement components in atherosclerotic plaques. Am. J. Pathol. 2001, 158, 1039–1051. [Google Scholar] [CrossRef] [Green Version]
- Zacho, J.; Tybjaerg-Hansen, A.; Jensen, J.; Grande, P.; Sillesen, H.; Nordestgaard, B.G. Genetically elevated C-reactive protein and ischemic vascular disease. N. Engl. J. Med. 2008, 30, 1897–1908. [Google Scholar] [CrossRef] [PubMed]
- Morita, H.; Nagai, R. Genetically elevated C-reactive protein and vascular disease. N. Engl. J. Med. 2009, 360, 934–935. [Google Scholar]
- Taylor, K.E.; Giddings, J.C.; van den Berg, C.W. C-reactive protein-induced in vitro endothelial cell activation is an artefact caused by azide and lipopolysaccharide. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 1225–1230. [Google Scholar] [CrossRef] [Green Version]
- Kaplan, M.H.; Volanakis, J.E. Interaction of C-reactive protein complexes with the complement system. I. Consumption of human complement associated with the reaction of C-reactive protein with pneumococcal C-polysaccharide and with the choline phosphatides, lecithin and sphingomyelin. J. Immunol. 1974, 112, 2135–2147. [Google Scholar]
- Bharadwaj, D.; Stein, M.P.; Volzer, M.; Mold, C.; Du Clos, T.W. The major receptor for C-reactive protein on leukocytes is fcgamma receptor II. J. Exp. Med. 1999, 190, 585–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ridker, P.M.; Danielson, E.; Fonseca, F.A.H.; Genest, J.; Gotto Jr, A.M.; Kastelein, J.J.P.; Koenig, W.; Libby, P.; Lorenzatti, A.J.; MacFadyen, J.G.; et al. JUPITER Study Group. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N. Engl. J. Med. 2008, 359, 2195–2207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. CANTOS Trial Group. Antiinflammatory Therapy with Canakinumab for atherosclerotic disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef] [PubMed]
- Tardif, J.C.; Kouz, S.; Waters, D.D.; Bertrand, O.F.; Diaz, R.; Maggioni, A.P.; Pinto, F.J.; Ibrahim, R.; Gamra, H.; Kiwan, G.S.; et al. Efficacy and Safety of Low-Dose Colchicine after Myocardial Infarction. N. Engl. J. Med. 2019, 381, 2497–2505. [Google Scholar] [CrossRef]
- Kolkhof, P.; Geerts, A.; Schäfer, S.; Torzewski, J. Cardiac glycosides potently inhibit C-reactive protein synthesis in human hepatocytes. Biochem. Biophys. Res. Commun. 2010, 394, 233–239. [Google Scholar] [CrossRef]
- Kostenzer, K. Anwendungsbeobachtung: Hemmung der Synthese des C-Reaktiven Proteins durch kardiale Glykoside. Ph.D. Thesis, Universität Ulm, Ulm, Germany, 2021. [Google Scholar] [CrossRef]
- Torzewski, J.; Graf, M.; Weber, K.; Zaczkiewicz, M.; Leier, M.; Froehlich, M.; Zimmermann, O. Inhibiting C-Reactive Protein Synthesis by Cardiac Glycosides in Humans. Open Conf. Proc. J. 2016, 7, 7–11. [Google Scholar] [CrossRef] [Green Version]
- Saylav, B.E.; Erdoğan, M.; Bahattin, Ö.; Ibrahim, S.; Ibrahim, S.; Canan, H.; Oytun, E. Short term protective effect of digitoxin in sepsis-induced acute lung injury. Biocell 2022, 46, 433–439. [Google Scholar] [CrossRef]
- NVL Chronische Herzinsuffizienz, 3. Auflage. Available online: https://www.leitlinien.de/nvl/html/nvl-chronische-herzinsuffizienz/3-auflage/tabellenverzeichnis (accessed on 22 January 2022).
- McMurray, J.J.; Adamopoulos, S.; Anker, S.D.; Auricchio, A.; Böhm, M.; Dickstein, K.; Falk, V.; Filippatos, G.; Fonseca, C.; Gomez-Sanchez, M.; et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2012, 33, 17871847. [Google Scholar] [CrossRef]
- Withering, W. An Account of the Foxglove and Some of Its Medical Uses with Practical Remarks on Dropsy and Other Diseases; GGJ and J Robinson: London, UK, 1785. [Google Scholar]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation 2017, 136, e137–e161. [Google Scholar] [CrossRef]
- Dávila, L.A.; Weber, K.; Bavendiek, U.; Bauersachs, J.; Wittes, J.; Yusuf, S.; Koch, A. Digoxin-mortality: Randomized vs. observational comparison in the DIG trial. Eur. Heart J. 2019, 40, 3336–3341. [Google Scholar] [CrossRef]
- Andrade, J.; Khairy, P.; Dobrev, D.; Nattel, S. The clinical profile and pathophysiology of atrial fibrillation: Relationships among clinical features, epidemiology, and mechanisms. Circ. Res. 2014, 114, 145314–145368. [Google Scholar] [CrossRef] [PubMed]
- Prasad, K. C-reactive (CRP)-lowering agents. Cardiovasc. Drug Rev. 2006, 24, 33–50. [Google Scholar] [CrossRef] [PubMed]
- Nidorf, S.M.; Eikelboom, J.W.; Budgeon, C.A.; Thompson, P.L. Low-dose colchicine for secondary prevention of cardiovascular disease. J. Am. Coll. Cardiol. 2013, 61, 404–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheriff, A.; Schindler, R.; Vogt, B.; Abdel-Aty, H.; Unger, J.K.; Bock, C.; Gebauer, F.; Slagman, A.; Jerichow, T.; Mans, D.; et al. Selective apheresis of C-reactive protein: A new therapeutic option in myocardial infarction? J. Clin. Apher. 2015, 30, 15–21. [Google Scholar] [CrossRef]
- Ries, W.; Sheriff, A.; Heigl, F.; Zimmermann, O.; Garlichs, C.D.; Torzewski, J. “First in Man”: Case Report of Selective C-Reactive Protein Apheresis in a Patient with Acute ST Segment Elevation Myocardial Infarction. Case Rep. Cardiol. 2018, 2018, 4767105. [Google Scholar] [CrossRef]
- Ries, W.; Torzewski, J.; Heigl, F.; Pfluecke, C.; Kelle, S.; Darius, H.; Ince, H.; Mitzner, S.; Nordbeck, P.; Butter, C.; et al. C-Reactive Protein Apheresis as Anti-inflammatory Therapy in Acute Myocardial Infarction: Results of the CAMI-1 Study. Front. Cardiovasc. Med. 2021, 8, 155. [Google Scholar] [CrossRef]
- Torzewski, J.; Heigl, F.; Zimmermann, O.; Wagner, F.; Schumann, C.; Hettich, R.; Bock, C.; Kayser, S.; Sheriff, A. First-in-Man: Case Report of Selective C-Reactive Protein Apheresis in a Patient with SARS-CoV-2 Infection. Am. J. Case Rep. 2020, 21, e925020. [Google Scholar] [CrossRef]


{kind=link}
| Demographic Data | Digoxin Group | Control Group | p-Value |
|---|---|---|---|
| Age (±SD) | 71.8 years (±10.6) | 73.7 years (±8.6) | n.s. |
| Sex: male/female | 26/4 | 22/8 | n.s. |
| Clinical data | |||
| NYHA III/IV | 26/4 | 24/6 | n.s. |
| LVEF (±SD) | 26.1% (±0.08) | 24.5% (±0.06) | n.s. |
| Ischemic cardiomyopathy (total) | 12 | 11 | n.s. |
| Dilated cardiomyopathy (total) | 18 | 19 | n.s. |
| Clinical chemistry | |||
| Digoxin serum level d1 (±SD) | 0.28 µg/L (±0.38) | ||
| Digoxin serum level d21 (±SD) | 1.46 µg/L (±0.81) | ||
| Creatinine (±SD) | 1.20 mg/dL (±0.35) | 1.16 mg/dL (±0.35) | n.s. |
| Sodium (±SD) | 140.53 mmol/L (±3.76) | 139.00 mmol/L (±3.38) | n.s. |
| Potassium (±SD) | 4.22 mmol/L (±0.43) | 4.34 mmol/L (±0.55) | n.s. |
| Calcium (±SD) | 2.27 mmol/L (±0.12) | 2.29 mmol/L (±0.88) | n.s. |
| proBNP (d1) | 8484 pg/mL | 8528 pg/mL | n.s. |
| Red blood cell count (d1) | 498 million/µL | 464 million/µL | n.s. |
| ECG rhythm at baseline | Number of patients | ||
| Sinus rhythm | 17 | 26 | 0.010 |
| Atrial fibrillation | 11 | 4 | 0.037 |
| Slow VT | 1 | 0 | n.s. |
| Atrial flutter | 1 | 0 | n.s. |
| Class IA medication | Number of patients | ||
| b-blocker (d1/d21) | 27/27 | 26/30 | n.s./n.s. |
| ACE inhibitor (d1/d21) | 20/22 | 24/23 | n.s./n.s. |
| AT1 blocker (d1/d21) | 5/5 | 4/5 | n.s./n.s. |
| Aldosterone antagonist (d1/d21) | 19/18 | 17/28 | n.s./0.002 |
| CRP d1 (mg/dL) | CRP d3 (mg/dL) | CRP d5 (mg/dL) | CRP d7 (mg/dL) | CRP d21 (mg/dL) | |
|---|---|---|---|---|---|
| Digoxin group (±SD) | 1.16 (±1.07) | 1.62 (±1.80) | 1.37 (±1.22) | 1.36 (±1.36) | 0.54 (±0.67) |
| Control group (±SD) | 0.94 (±0.77) | 0.98 (±0.98) | 1.23 (±2.19) | 1.63 (±2.45) | 0.72 (±0.90) |
| Non-standard distribution | Shapiro–Wilk test | Shapiro–Wilk test | Shapiro–Wilk test | ||
| Digoxin group | <0.001 | <0.001 | <0.001 | ||
| Control group | <0.001 | <0.001 | <0.001 | ||
| Wilcoxon test | Wilcoxon test | Wilcoxon test | |||
| Digoxin group | Control group | Group comparison | |||
| d1/d21 (control group) | <0.001 | <0.001 | 0.268 | ||
| d3/d21 (control group) | <0.001 | 0.029 | 0.051 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaczkiewicz, M.; Kostenzer, K.; Graf, M.; Mayer, B.; Zimmermann, O.; Torzewski, J. Cardiac Glycosides Lower C-Reactive Protein Plasma Levels in Patients with Decompensated Heart Failure: Results from the Single-Center C-Reactive Protein-Digoxin Observational Study (C-DOS). J. Clin. Med. 2022, 11, 1762. https://doi.org/10.3390/jcm11071762
Zaczkiewicz M, Kostenzer K, Graf M, Mayer B, Zimmermann O, Torzewski J. Cardiac Glycosides Lower C-Reactive Protein Plasma Levels in Patients with Decompensated Heart Failure: Results from the Single-Center C-Reactive Protein-Digoxin Observational Study (C-DOS). Journal of Clinical Medicine. 2022; 11(7):1762. https://doi.org/10.3390/jcm11071762
Chicago/Turabian StyleZaczkiewicz, Myron, Katharina Kostenzer, Matthias Graf, Benjamin Mayer, Oliver Zimmermann, and Jan Torzewski. 2022. "Cardiac Glycosides Lower C-Reactive Protein Plasma Levels in Patients with Decompensated Heart Failure: Results from the Single-Center C-Reactive Protein-Digoxin Observational Study (C-DOS)" Journal of Clinical Medicine 11, no. 7: 1762. https://doi.org/10.3390/jcm11071762