
Improved Kidney Allograft Function after Early Conversion of Fast IR-Tac Metabolizers to LCP-Tac

 , , ,
, , ,
Abstract
:1. Introduction
2. Patients and Methods
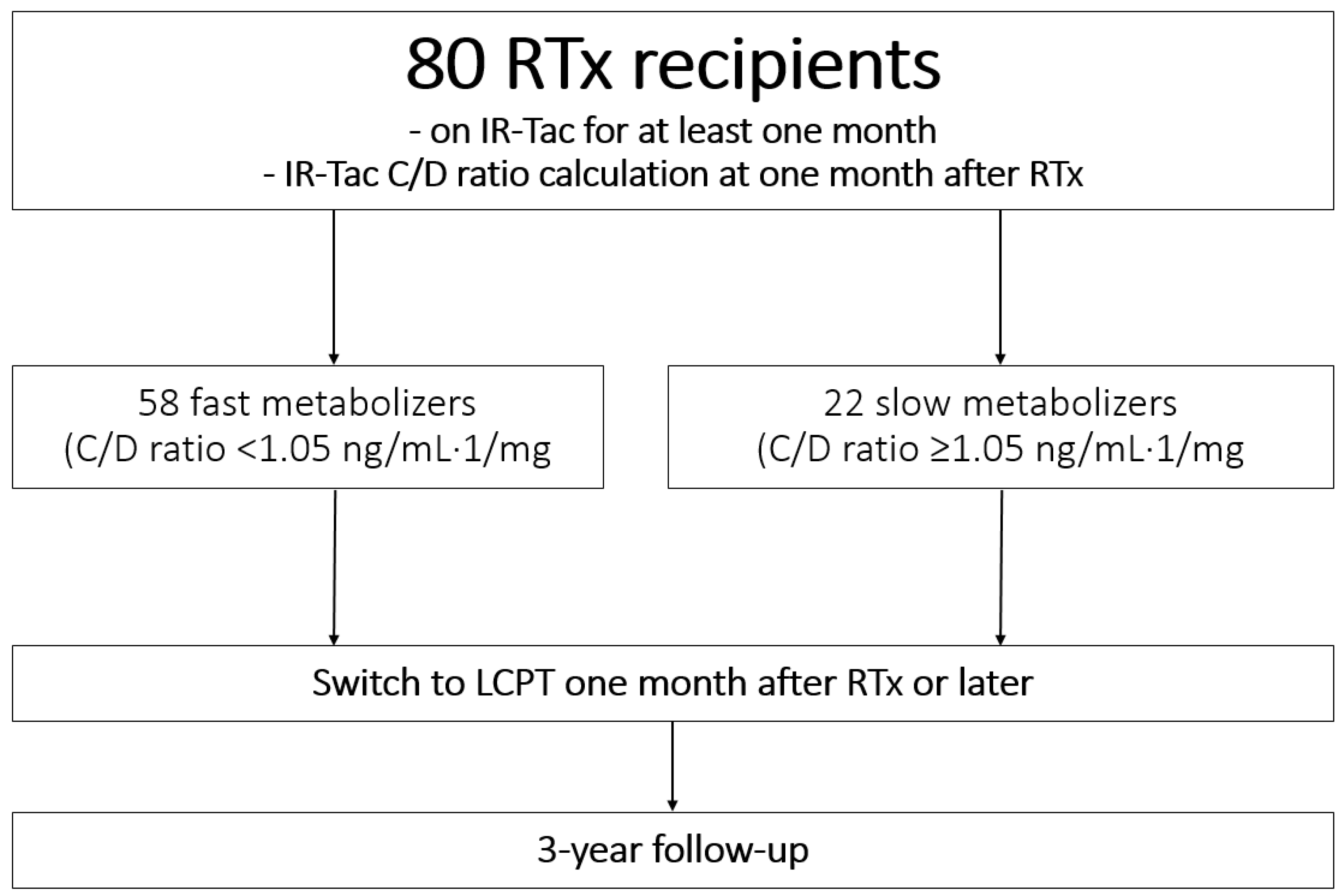
2.1. Study Cohort
2.2. Statistics
3. Results
3.1. Study Cohort
3.2. Immunosuppression
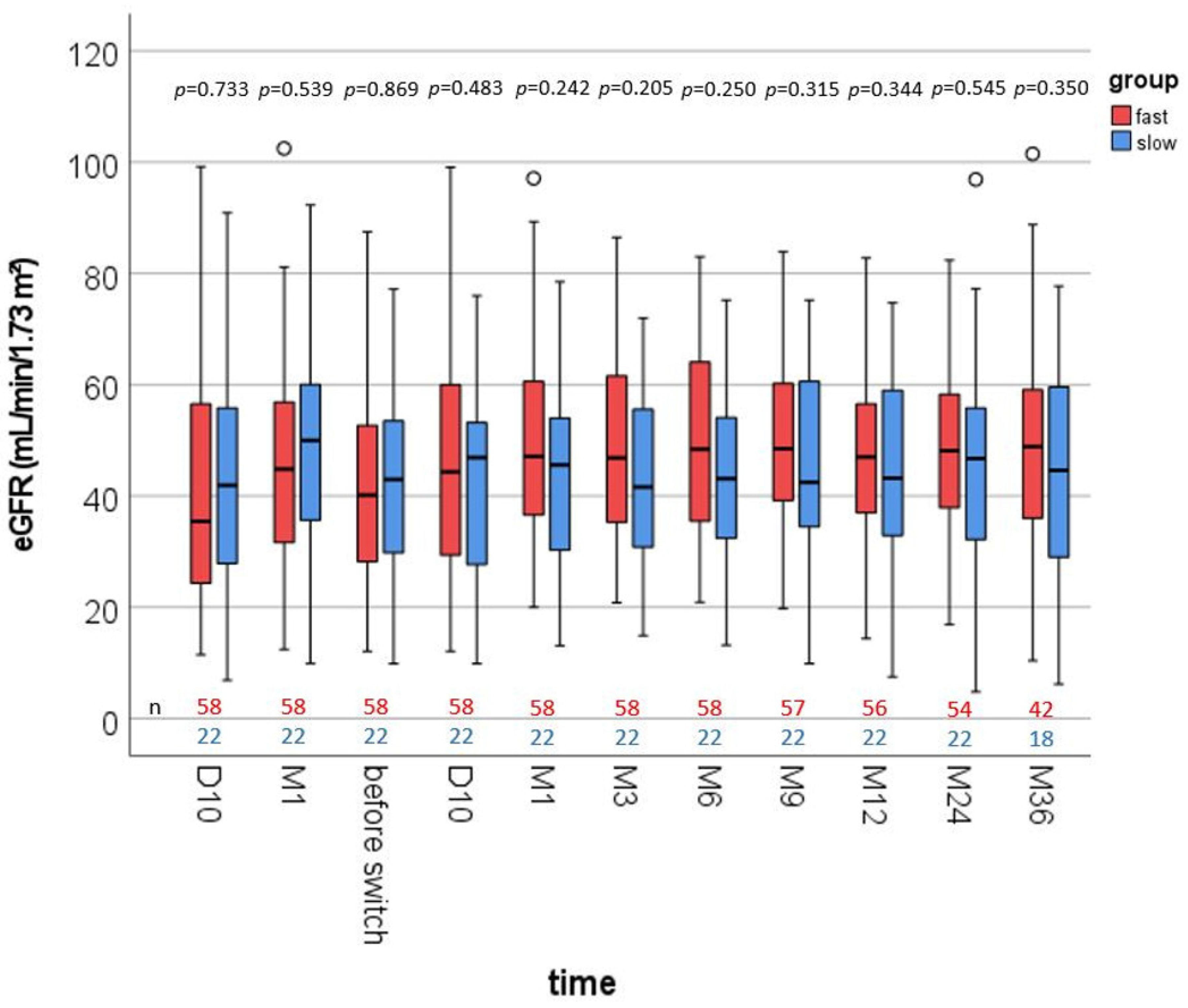
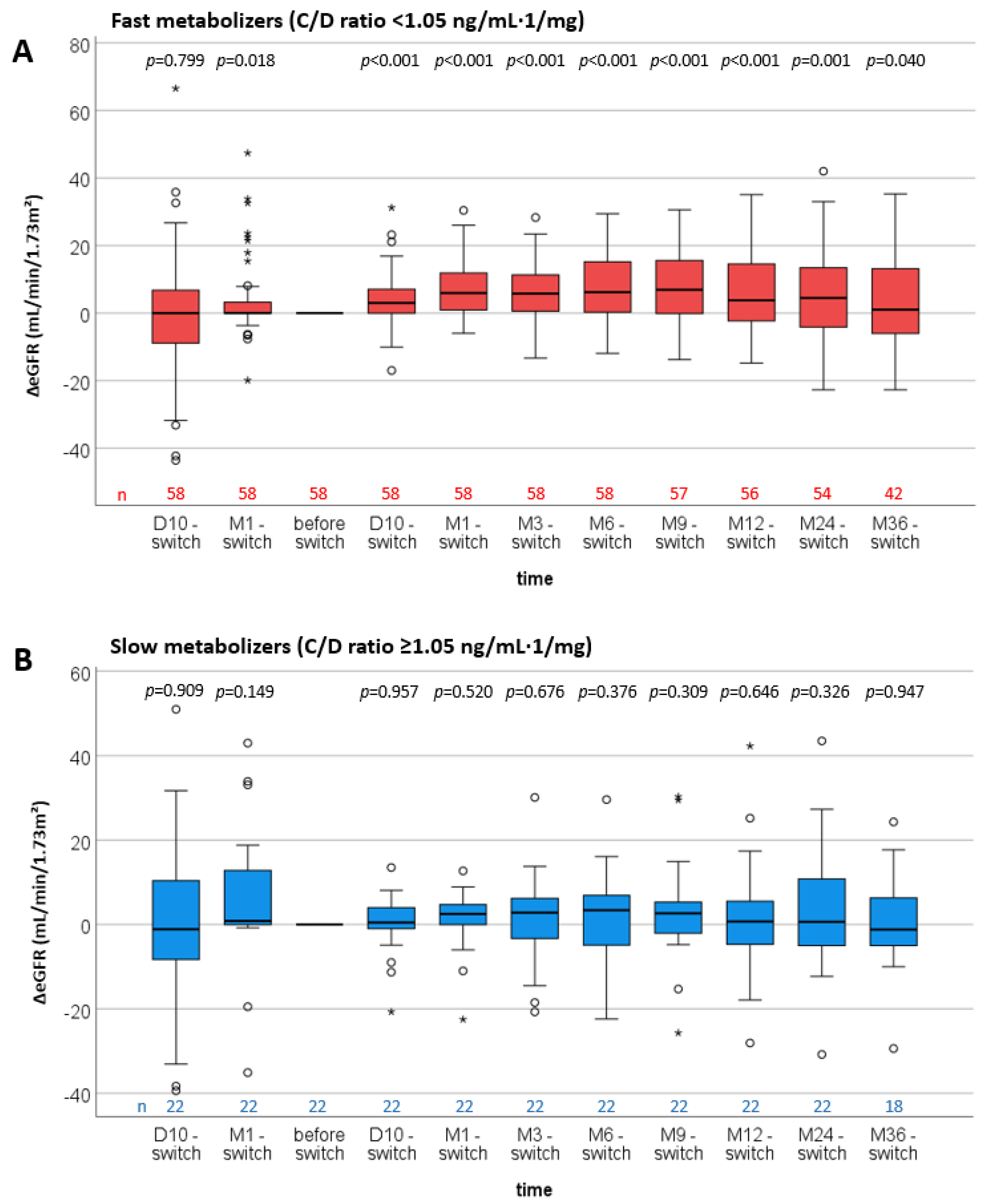
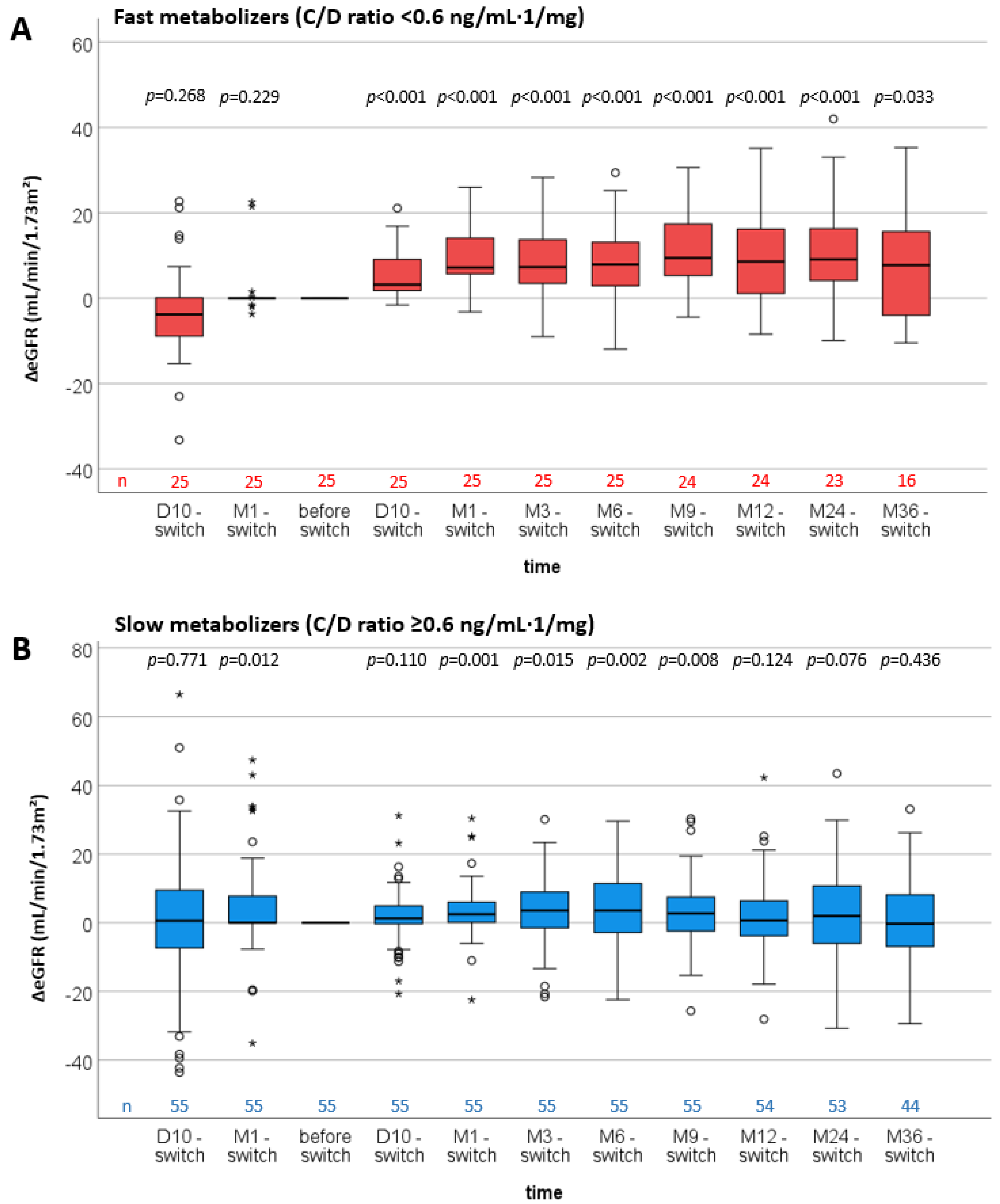
3.3. Renal Function
3.4. Complication Rates
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Tholking, G.; Gerth, H.U.; Schuette-Nuetgen, K.; Reuter, S. Influence of tacrolimus metabolism rate on renal function after solid organ transplantation. World J. Transplant. 2017, 7, 26–33. [Google Scholar] [CrossRef]
- Ong, S.C.; Gaston, R.S. Thirty years of tacrolimus in clinical practice. Transplantation 2021, 105, 484–495. [Google Scholar] [CrossRef]
- Tremblay, S.; Nigro, V.; Weinberg, J.; Woodle, E.S.; Alloway, R.R. A steady-state head-to-head pharmacokinetic comparison of all FK-506 (Tacrolimus) formulations (ASTCOFF): An open-label, prospective, randomized, two-arm, three-period crossover study. Am. J. Transplant. 2017, 17, 432–442. [Google Scholar] [CrossRef] [PubMed]
- Kuypers, D.R.; Peeters, P.C.; Sennesael, J.J.; Kianda, M.N.; Vrijens, B.; Kristanto, P.; Dobbels, F.; Vanrenterghem, Y.; Kanaan, N.; Team, A.S. Improved adherence to tacrolimus once-daily formulation in renal recipients: A randomized controlled trial using electronic monitoring. Transplantation 2013, 95, 333–340. [Google Scholar] [CrossRef] [Green Version]
- Tholking, G.; Fortmann, C.; Koch, R.; Gerth, H.U.; Pabst, D.; Pavenstadt, H.; Kabar, I.; Husing, A.; Wolters, H.; Reuter, S.; et al. The tacrolimus metabolism rate influences renal function after kidney transplantation. PLoS ONE 2014, 9, e111128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schutte-Nutgen, K.; Tholking, G.; Steinke, J.; Pavenstadt, H.; Schmidt, R.; Suwelack, B.; Reuter, S. Fast tac metabolizers at risk (-) it is time for a C/D ratio calculation. J. Clin. Med. 2019, 8, 587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nowicka, M.; Gorska, M.; Nowicka, Z.; Edyko, K.; Edyko, P.; Wislicki, S.; Zawiasa-Bryszewska, A.; Strzelczyk, J.; Matych, J.; Kurnatowska, I. Tacrolimus: Influence of the posttransplant concentration/dose ratio on kidney graft function in a two-year follow-up. Kidney Blood Press Res. 2019, 44, 1075–1088. [Google Scholar] [CrossRef] [PubMed]
- Jouve, T.; Fonrose, X.; Noble, J.; Janbon, B.; Fiard, G.; Malvezzi, P.; Stanke-Labesque, F.; Rostaing, L. The TOMATO study (TacrOlimus MetabolizAtion in kidney TransplantatiOn): Impact of the concentration-dose ratio on death-censored graft survival. Transplantation 2019, 104, 1263–1271. [Google Scholar] [CrossRef]
- Egeland, E.J.; Reisaeter, A.V.; Robertsen, I.; Midtvedt, K.; Strom, E.H.; Holdaas, H.; Hartmann, A.; Asberg, A. High tacrolimus clearance—A risk factor for development of interstitial fibrosis and tubular atrophy in the transplanted kidney: A retrospective single-center cohort study. Transpl. Int. 2019, 32, 257–269. [Google Scholar] [CrossRef] [PubMed]
- Egeland, E.J.; Robertsen, I.; Hermann, M.; Midtvedt, K.; Storset, E.; Gustavsen, M.T.; Reisaeter, A.V.; Klaasen, R.; Bergan, S.; Holdaas, H.; et al. High tacrolimus clearance is a risk factor for acute rejection in the early phase after renal transplantation. Transplantation 2017, 101, e273–e279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tholking, G.; Schutte-Nutgen, K.; Schmitz, J.; Rovas, A.; Dahmen, M.; Bautz, J.; Jehn, U.; Pavenstadt, H.; Heitplatz, B.; Van Marck, V.; et al. A Low tacrolimus concentration/dose ratio increases the risk for the development of acute calcineurin inhibitor-induced nephrotoxicity. J. Clin. Med. 2019, 8, 1586. [Google Scholar] [CrossRef] [Green Version]
- Tholking, G.; Filensky, B.; Jehn, U.; Schutte-Nutgen, K.; Koch, R.; Kurschat, C.; Pavenstadt, H.; Suwelack, B.; Reuter, S.; Kuypers, D. Increased renal function decline in fast metabolizers using extended-release tacrolimus after kidney transplantation. Sci. Rep. 2021, 11, 15606. [Google Scholar] [CrossRef] [PubMed]
- Tholking, G.; Schmidt, C.; Koch, R.; Schuette-Nuetgen, K.; Pabst, D.; Wolters, H.; Kabar, I.; Husing, A.; Pavenstadt, H.; Reuter, S.; et al. Influence of tacrolimus metabolism rate on BKV infection after kidney transplantation. Sci. Rep. 2016, 6, 32273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Einsiedel, J.; Tholking, G.; Wilms, C.; Vorona, E.; Bokemeyer, A.; Schmidt, H.H.; Kabar, I.; Husing-Kabar, A. Conversion from standard-release tacrolimus to MeltDose((R)) Tacrolimus (LCPT) improves renal function after liver transplantation. J. Clin. Med. 2020, 9, 1654. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Chamoun, B.; Torres, I.B.; Gabaldon, A.; Sellares, J.; Perello, M.; Castella, E.; Guri, X.; Salcedo, M.; Toapanta, N.G.; Cidraque, I.; et al. Progression of interstitial fibrosis and tubular atrophy in low immunological risk renal transplants monitored by sequential surveillance biopsies: The influence of TAC exposure and metabolism. J. Clin. Med. 2021, 10, 141. [Google Scholar] [CrossRef] [PubMed]
- Tholking, G.; Schulte, C.; Jehn, U.; Schutte-Nutgen, K.; Pavenstadt, H.; Suwelack, B.; Reuter, S. The tacrolimus metabolism rate and dyslipidemia after kidney transplantation. J. Clin. Med. 2021, 10, 3066. [Google Scholar] [CrossRef]
- Kuypers, D.R.J. Intrapatient variability of tacrolimus exposure in solid organ transplantation: A novel marker for clinical outcome. Clin. Pharmacol. Ther. 2020, 107, 347–358. [Google Scholar] [CrossRef]
- Gaber, A.O.; Alloway, R.R.; Bodziak, K.; Kaplan, B.; Bunnapradist, S. Conversion from twice-daily tacrolimus capsules to once-daily extended-release tacrolimus (LCPT): A phase 2 trial of stable renal transplant recipients. Transplantation 2013, 96, 191–197. [Google Scholar] [CrossRef] [Green Version]
- Bunnapradist, S.; Rostaing, L.; Alloway, R.R.; West-Thielke, P.; Denny, J.; Mulgaonkar, S.; Budde, K. LCPT once-daily extended-release tacrolimus tablets versus twice-daily capsules: A pooled analysis of two phase 3 trials in important de novo and stable kidney transplant recipient subgroups. Transpl. Int. 2016, 29, 603–611. [Google Scholar] [CrossRef] [Green Version]
- Budde, K.; Bunnapradist, S.; Grinyo, J.M.; Ciechanowski, K.; Denny, J.E.; Silva, H.T.; Rostaing, L.; Envarsus Study Group. Novel once-daily extended-release tacrolimus (LCPT) versus twice-daily tacrolimus in de novo kidney transplants: One-year results of Phase III, double-blind, randomized trial. Am. J. Transplant. 2014, 14, 2796–2806. [Google Scholar] [CrossRef]
- Trofe-Clark, J.; Brennan, D.C.; West-Thielke, P.; Milone, M.C.; Lim, M.A.; Neubauer, R.; Nigro, V.; Bloom, R.D. Results of ASERTAA, a Randomized Prospective Crossover Pharmacogenetic Study of Immediate-Release Versus Extended-Release Tacrolimus in African American Kidney Transplant Recipients. Am. J. Kidney Dis. 2018, 71, 315–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schutte-Nutgen, K.; Tholking, G.; Suwelack, B.; Reuter, S. Tacrolimus—Pharmacokinetic considerations for clinicians. Curr. Drug Metab. 2018, 19, 342–350. [Google Scholar] [CrossRef]
- Suwelack, B.; Bunnapradist, S.; Meier-Kriesche, U.; Stevens, D.R.; Procaccianti, C.; Morganti, R.; Budde, K. Effect of concentration/dose ratio in de novo kidney transplant recipients receiving LCP-tacrolimus or immediate-release tacrolimus: Post hoc analysis of a phase 3 clinical trial. Ann. Transplant. 2020, 25, e923278. [Google Scholar] [CrossRef] [PubMed]
- Glander, P.; Waiser, J.; Kasbohm, S.; Friedersdorff, F.; Peters, R.; Rudolph, B.; Wu, K.; Budde, K.; Liefeldt, L. Bioavailability and costs of once-daily and twice-daily tacrolimus formulations in de novo kidney transplantation. Clin. Transplant. 2018, 32, e13311. [Google Scholar] [CrossRef]
- Kuypers, D.R.; Naesens, M.; de Jonge, H.; Lerut, E.; Verbeke, K.; Vanrenterghem, Y. Tacrolimus dose requirements and CYP3A5 genotype and the development of calcineurin inhibitor-associated nephrotoxicity in renal allograft recipients. Ther. Drug Monit. 2010, 32, 394–404. [Google Scholar] [CrossRef] [PubMed]
- Hryniewiecka, E.; Zegarska, J.; Zochowska, D.; Samborowska, E.; Jazwiec, R.; Kosieradzki, M.; Nazarewski, S.; Dadlez, M.; Paczek, L. Dose-adjusted and dose/kg-adjusted concentrations of mycophenolic acid precursors reflect metabolic ratios of their metabolites in contrast with tacrolimus and cyclosporine. Biosci. Rep. 2019, 39, 39. [Google Scholar] [CrossRef] [Green Version]
- Alloway, R.R.; Trofe-Clark, J.; Brennan, D.C.; Kerr, J.; Cohen, E.A.; Meier-Kriesche, U.; Stevens, D.R.; Moten, M.A.; Momper, J.D. Chronopharmacokinetics and food effects of single-dose LCP-tacrolimus in healthy volunteers. Ther. Drug Monit. 2020, 42, 679–685. [Google Scholar] [CrossRef]
- Tremblay, S.; Alloway, R.R. Clinical evaluation of modified release and immediate release tacrolimus formulations. AAPS J. 2017, 19, 1332–1347. [Google Scholar] [CrossRef]
- Huppertz, A.; Ott, C.; Bruckner, T.; Foerster, K.I.; Burhenne, J.; Weiss, J.; Zorn, M.; Haefeli, W.E.; Czock, D. Prolonged-release tacrolimus is less susceptible to interaction with the strong CYP3A inhibitor voriconazole in healthy volunteers. Clin. Pharmacol. Ther. 2019, 106, 1290–1298. [Google Scholar] [CrossRef]
- Rostaing, L.; Bunnapradist, S.; Grinyo, J.M.; Ciechanowski, K.; Denny, J.E.; Silva, H.T., Jr.; Budde, K.; Envarsus Study Group. Novel once-daily extended-release tacrolimus versus twice-daily tacrolimus in de novo kidney transplant recipients: Two-year results of phase 3, double-blind, randomized trial. Am. J. Kidney Dis. 2016, 67, 648–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faravardeh, A.; Akkina, S.; Villicana, R.; Guerra, G.; Moten, M.A.; Meier-Kriesche, U.; Stevens, D.R.; Patel, S.J.; Bunnapradist, S. Efficacy and safety of once-daily lcp-tacrolimus versus twice-daily immediate-release tacrolimus in adult hispanic stable kidney transplant recipients: Sub-Group analysis from a phase 3 trial. Ann. Transplant. 2021, 26, e929535. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Fast Metabolizers n = 58 | Slow Metabolizers n = 22 | p-Value | |
|---|---|---|---|
| age (years) | 50.0 ± 16.1 | 49.8 ± 14.7 | 0.957 a |
| sex (m/f), n (%) | 37 (63.8%)/21 (36.2%) | 13 (59.1%)/9 (40.9%) | 0.797 b |
| weight (kg) | 80.8 ± 18.3 | 76.4 ± 15.1 | 0.274 a |
| height (m) | 1.77 ± 0.09 | 1.75 ± 0.09 | 0.267 a |
| BMI (kg/m²) | 25.5 ± 5.3 | 24.9 ± 4.3 | 0.570 a |
| living donor transplantation | 37 (63.8%) | 16 (72.7%) | 0.598 b |
| ABO-i | 13 (22.4%) | 7 (31.8%) | 0.399 b |
| ESP transplantation | 4 (6.9%) | 1 (4.5%) | 1 b |
| DGF | 6 (10.3%) | 3 (13.6%) | 0.700 b |
| cold ischemic time (h) | 7.4 ± 5.0 | 6.7 ± 4.3 | 0.539 a |
| warm ischemic time (min) | 35.9 ± 8.3 | 35.9 ± 9.2 | 0.968 a |
| Number of Transplantations | |||
| 1 | 51 (87.9%) | 19 (86.4%) | 0.785 b |
| 2 | 6 (10.3%) | 3 (13.6%) | |
| 3 | 1 (1.7%) | 0 | |
| HLA MM | |||
| 0 | 13 (22.4%) | 8 (36.4%) | 0.462 b |
| 1–3 | 23 (39.7%) | 7 (31.8%) | |
| 4–6 | 22 (37.9%) | 7 (31.8%) | |
| PRA > 20% | 5 (8.6%) | 2 (9.1%) | 1 b |
| CMV risk status | |||
| low | 13 (22.4%) | 2 (9.1%) | 0.105 b |
| intermediate | 34 (58.6%) | 11(50.0%) | |
| high | 11 (19.0%) | 9 (40.9%) | |
| Donor Characteristics | |||
| donor age (years) | 52.7 ± 12.2 | 55.8 ± 9.7 | 0.246 a |
| donor sex (m/f), n (%) | 24 (41.4%)/34 (58.6%) | 7 (31.8%)/15 (68.2%) | 0.608 b |
| Diagnosis of ESRD | |||
| benign nephrosclerosis | 4 (6.9%) | 1 (4.5%) | 0.345 b |
| diabetic nephropathy | 3 (5.2%) | 1 (4.5%) | |
| glomerulonephritis | 31 (53.4%) | 14 (63.6%) | |
| chronic pyelonephritis | 0 | 1 (4.5%) | |
| cystic nephropathy | 14 (24.1%) | 2 (9.1%) | |
| Alport syndrome | 1 (1.7%) | 0 | |
| Mediterranean fever | 0 | 1 (4.5%) | |
| congenital renal dysgenesis | 4 (6.9%) | 1 (4.5%) | |
| interstitial nephritis | 1 (1.7%) | 1 (4.5%) | |
| Comorbidities Before Transplantation | |||
| arterial hypertension | 56 (96.6%) | 21 (95.5%) | 1 b |
| diabetes mellitus | 8 (13.8%) | 1 (4.5%) | 0.432 b |
| Fast Metabolizers n = 58 | Slow Metabolizers n = 22 | p-Value | |
|---|---|---|---|
| infection | 1 (1.7%) | 1 (4.5%) | 0.778 |
| neurological disorder | 2 (3.4%) | 0 | |
| acute rejection | 1 (1.7%) | 0 | |
| CNIT | 2 (3.4%) | 2 (9.1%) | |
| DGF | 2 (3.4%) | 1 (4.5%) | |
| diabetes mellitus | 1 (1.7%) | 0 | |
| trough level variation/avoidance of adverse effects | 49 (84.5%) | 18 (81.8%) |
| Fast Metabolizers n = 58 | Slow Metabolizers n = 22 | p-Value | |
|---|---|---|---|
| Prednisolone Dose after 1 Month | 17.5 (5–25) | 15 (5–50) | 0.680 a |
| Mycophenolate after 1 Month | |||
| mycophenolate mofetil, n (%) | 30 (51.7%) | 13 (59.1%) | 0.621 b |
| mycophenolate sodium, n (%) | 28 (48.3%) | 9 (40.9%) | |
| mycophenolate mofetil dose (mg) | 1000 (500–2000) | 1000 (500–2000) | 0.932 a |
| mycophenolate sodium dose (mg) | 1440 (720–1440) | 1080 (720–1440) | 0.213 a |
| Tac Doses (mg) | |||
| IR-Tac M1 | 12 (5–20) | 7 (4–12) | <0.001 a |
| before switch (IR-Tac) | 10.25 (3–18) | 6.75 (1.5–17) | <0.001 a |
| D10 LCPT | 7 (1.5–14) | 3.5 (1.8 11) | <0.001 a |
| M1 LCPT | 6 (1.5–13.5) | 3 (1.5–11) | <0.001 a |
| M3 LCPT | 4.75 (1.5–12) | 3 (1–8) | 0.002 a |
| M6 LCPT | 4 (1.5–12) | 2.5 (0.75–5) | 0.001 a |
| M9 LCPT | 4 (1.5–11) | 2.5 (1–6) | 0.001 a |
| M12 LCPT | 3.63 (1.5–11) | 2.25 (1–5) | 0.001 a |
| M24 LCPT | 3.38 (1–9) | 2.13 (0.75–5.5) | 0.008 a |
| M36 LCPT | 3 (1–8.5) | 2 (0.75–3.5) | 0.016 a |
| Tac trough Levels (ng/mL) | |||
| IR-Tac M1 | 6.8 (2.4–15.9) | 8.7 (6.8–13.5) | <0.001 a |
| before switch (IR-Tac) | 6.3 (2.4–12.3) | 7.5 (3.9–13.5) | 0.065 a |
| D10 LCPT | 7.2 (1.6–14.7) | 6.3 (4.1–9.9) | 0.026 a |
| M1 LCPT | 7.6 (1.5–19.5) | 6.2 (3.7–12.9) | 0.041 a |
| M3 LCPT | 7.3 (3.8–18.1) | 6.7 (4.9–9.9) | 0.311 a |
| M6 LCPT | 7.0 (2.7–11.4) | 6.2 (4.0–10.4) | 0.043 a |
| M9 LCPT | 6.5 (3.4–10.7) | 6.3 (4.2–9.2) | 0.992 a |
| M12 LCPTT | 6.2 (3.5–10.3) | 6.05 (3.8–8.3) | 0.224 a |
| M24 LCPT | 6.2 (4.0–10.7) | 6.2 (2.1–9.4) | 0.254 a |
| M36 LCPT | 5.5 (4.1–8.9) | 5.40 (4.0–8.7) | 0.698 a |
| Tac C/D Ratio (ng/mL·1/mg) | |||
| IR-Tac M1 | 0.64 (0.24–1.01) | 1.25 (1.08–3.38) | <0.001 a |
| before switch (IR-Tac) | 0.66 (0.24–2.10) | 1.15 (0.32–3.60) | 0.001 a |
| D10 LCPT | 1.08 (0.33–4.90) | 1.91 (0.40–4.06) | 0.002 a |
| M1 LCPT | 1.24 (0.21–6.93) | 2.23 (0.55–3.47) | 0.010 a |
| M3 LCPT | 1.52 (0.55–4.93) | 2.33 (0.94–6.60) | 0.004 a |
| M6 LCPT | 1.58 (0.39–5.93) | 2.65 (1.06–7.07) | 0.007 a |
| M9 LCPT | 1.63 (0.40–5.07) | 3.23 (1.23–6.30) | <0.001 a |
| M12 LCPTT | 1.74 (0.42–5.43) | 2.75 (1.08–5.90) | 0.007 a |
| M24 LCPT | 1.81 (0.64–5.40) | 2.58 (0.96–6.27) | 0.083 a |
| M36 LCPT | 1.85 (0.69–5.80) | 2.65 (1.32–5.73) | 0.026 a |
| Fast Metabolizers n = 58 | Slow Metabolizers n = 22 | p-Value | |
|---|---|---|---|
| CMV infection | |||
| before switch to LCPT | 8 (13.8%) | 2 (9.1%) | 0.719 |
| after switch to LCPT (3 y-follow up) | 3 (5.2%) | 2 (9.1%) | 0.612 |
| BKV infection | |||
| before switch to LCPT | 3 (5.2%) | 3 (13.6%) | 0.338 |
| after switch to LCPT (3 y-follow up) | 1 (1.7%) | 0 | 1 |
| BKV nephropathy | |||
| before switch to LCPT | 1 (1.7%) | 2 (9.1%) | 0.182 |
| after switch to LCPT (3 y-follow up) | 0 | 0 | - |
| CNIT | |||
| before switch to LCPT | 3 (5.2%) | 2 (9.1%) | 0.612 |
| after switch to LCPT (3 y-follow up) | 1 (1.7%) | 0 | 1 |
| acute rejection | |||
| before switch to LCPT | 12 (20.7%) | 9 (40.9%) | 0.089 |
| after switch to LCPT (3 y-follow up) | 8 (13.8%) | 2 (9.1%) | 0.719 |
| death within 3 years after switch | 2 (3.4%) | 0 | 1 |
| diabetes mellitus | |||
| before switch to LCPT | 1 (1.7%) | 1 (4.5%) | 0.477 |
| after switch to LCPT (3 y-follow up) | 0 | 0 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thölking, G.; Tosun-Koç, F.; Jehn, U.; Koch, R.; Pavenstädt, H.; Suwelack, B.; Reuter, S. Improved Kidney Allograft Function after Early Conversion of Fast IR-Tac Metabolizers to LCP-Tac. J. Clin. Med. 2022, 11, 1290. https://doi.org/10.3390/jcm11051290
Thölking G, Tosun-Koç F, Jehn U, Koch R, Pavenstädt H, Suwelack B, Reuter S. Improved Kidney Allograft Function after Early Conversion of Fast IR-Tac Metabolizers to LCP-Tac. Journal of Clinical Medicine. 2022; 11(5):1290. https://doi.org/10.3390/jcm11051290
Chicago/Turabian StyleThölking, Gerold, Filiz Tosun-Koç, Ulrich Jehn, Raphael Koch, Hermann Pavenstädt, Barbara Suwelack, and Stefan Reuter. 2022. "Improved Kidney Allograft Function after Early Conversion of Fast IR-Tac Metabolizers to LCP-Tac" Journal of Clinical Medicine 11, no. 5: 1290. https://doi.org/10.3390/jcm11051290