
Lung Congestion Severity in Kidney Transplant Recipients Is Not Affected by Arteriovenous Fistula Function

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ultrasound Assessment
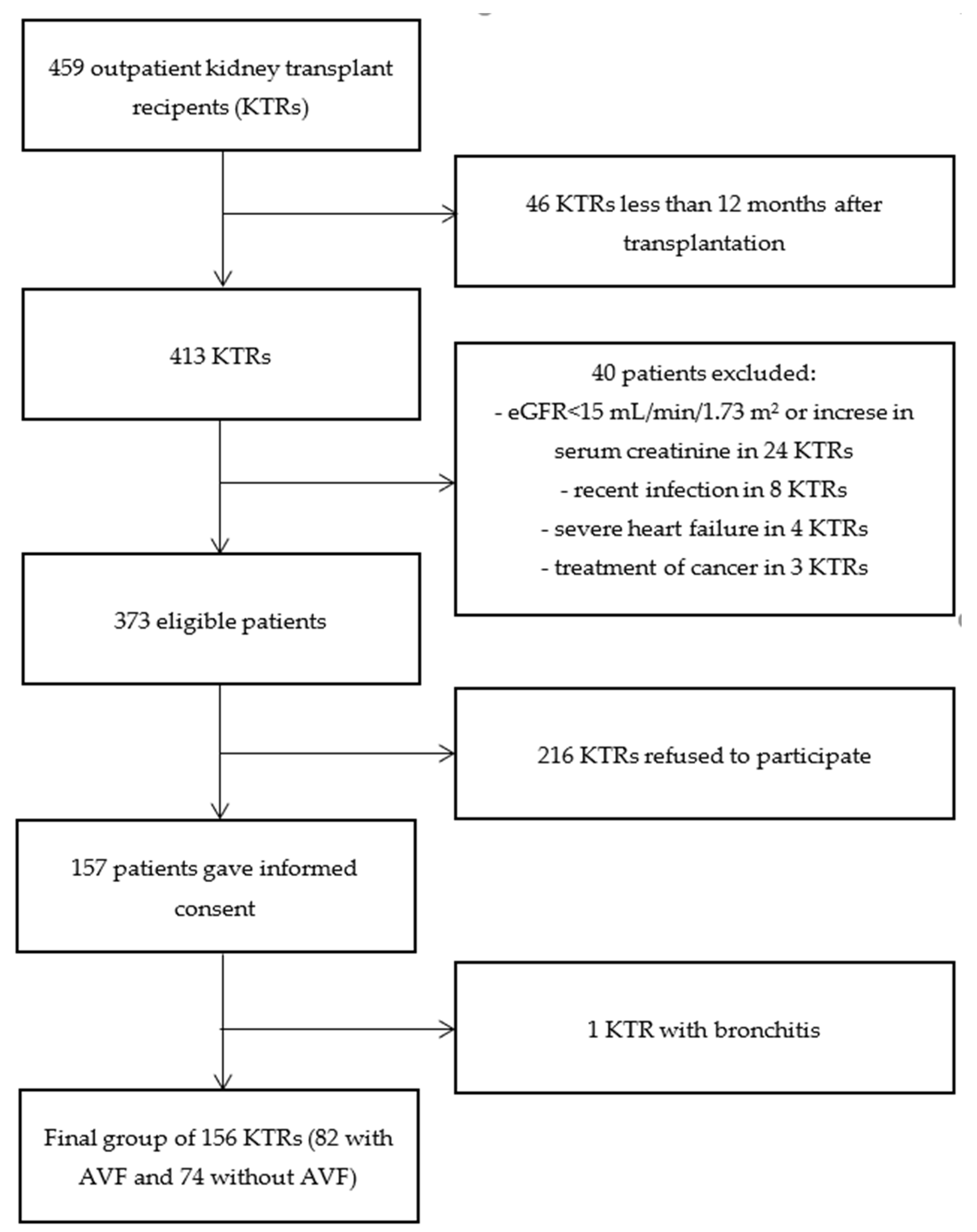
2.2. Study Group
2.3. Statistical Analysis
3. Results
3.1. Lung Ultrasound B-Lines
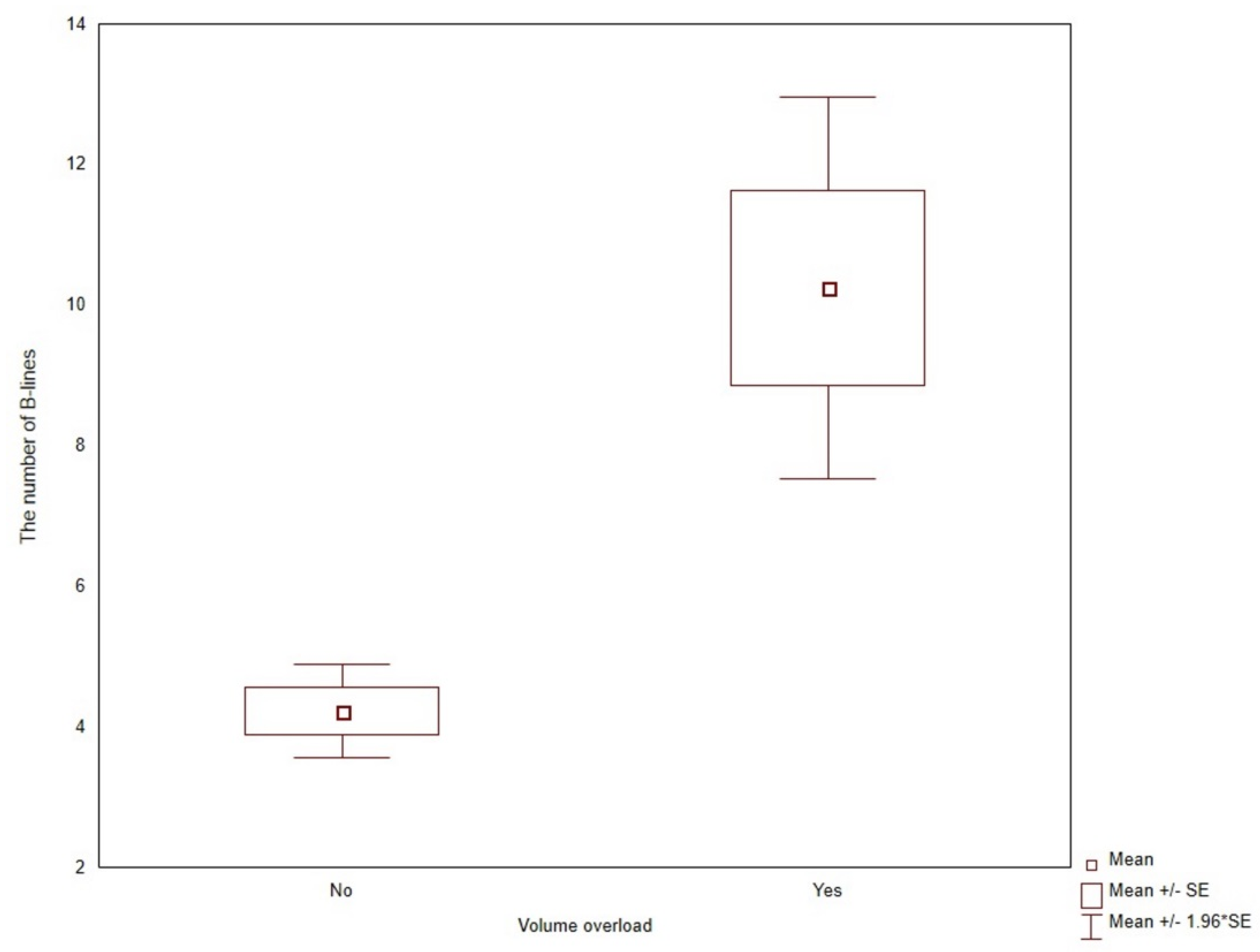
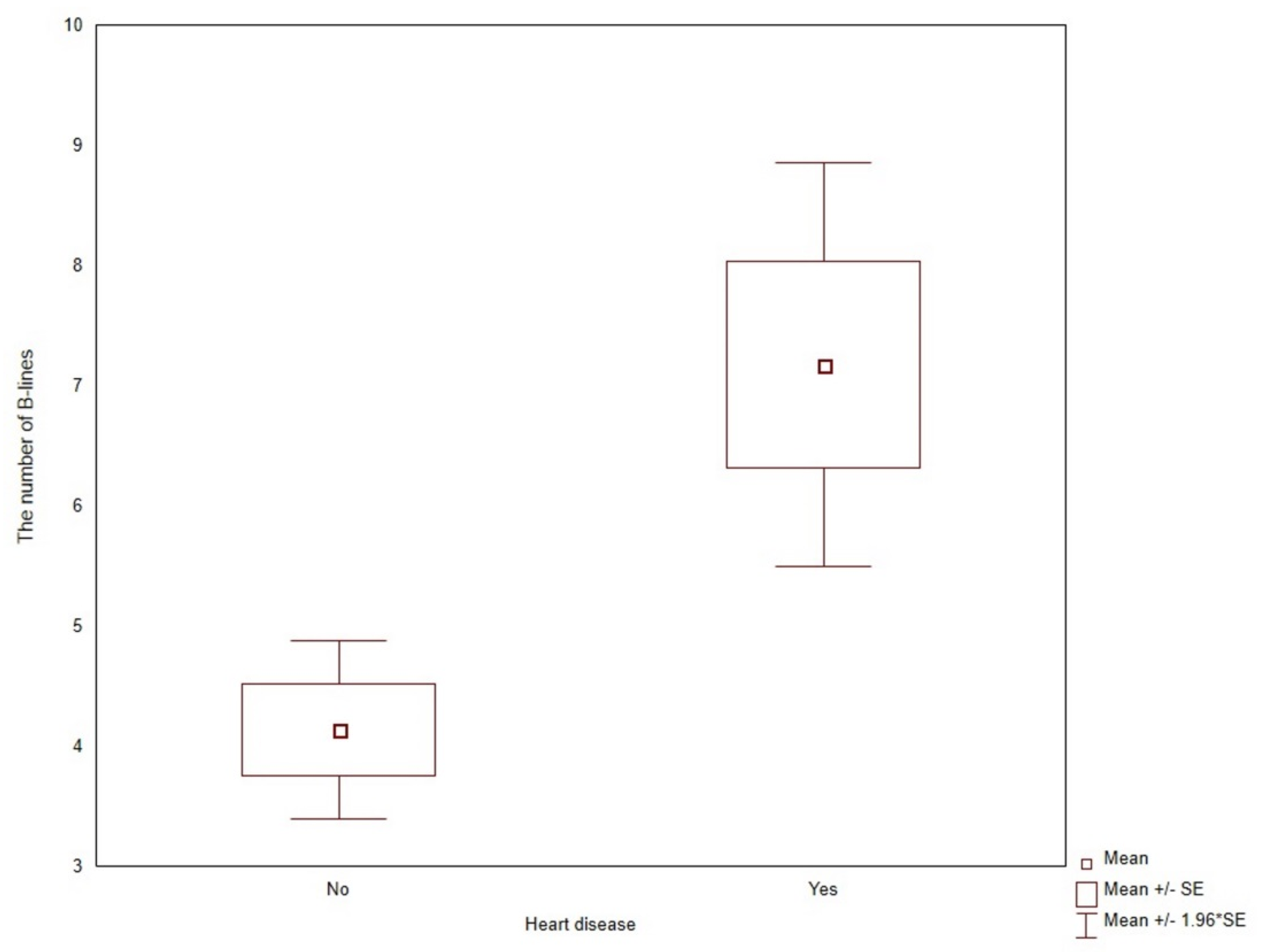
3.2. Predictors of Lung Congestion
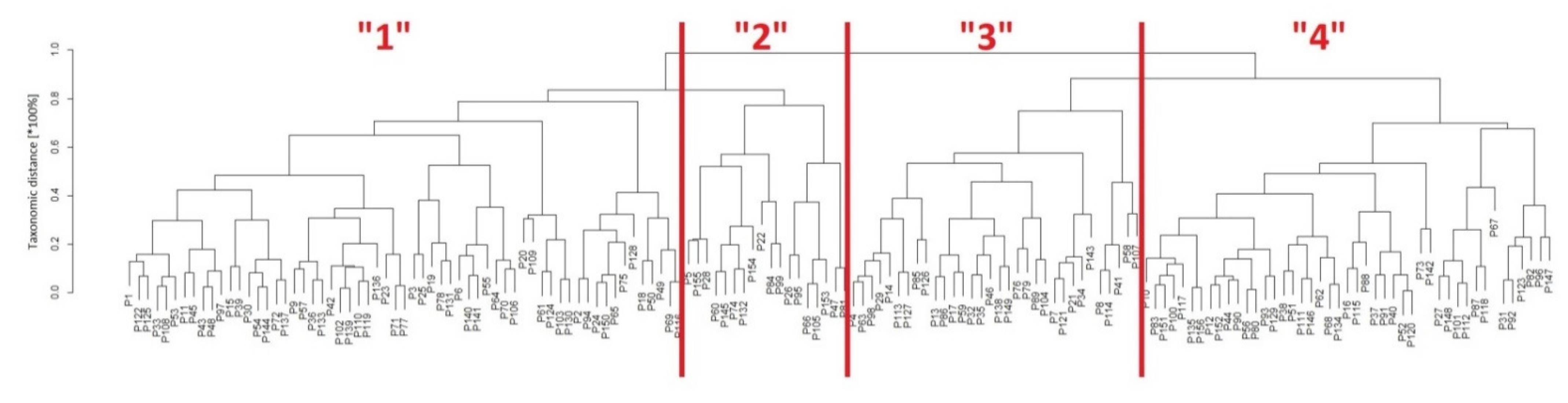
3.3. Classification of Patients with Taxonomy
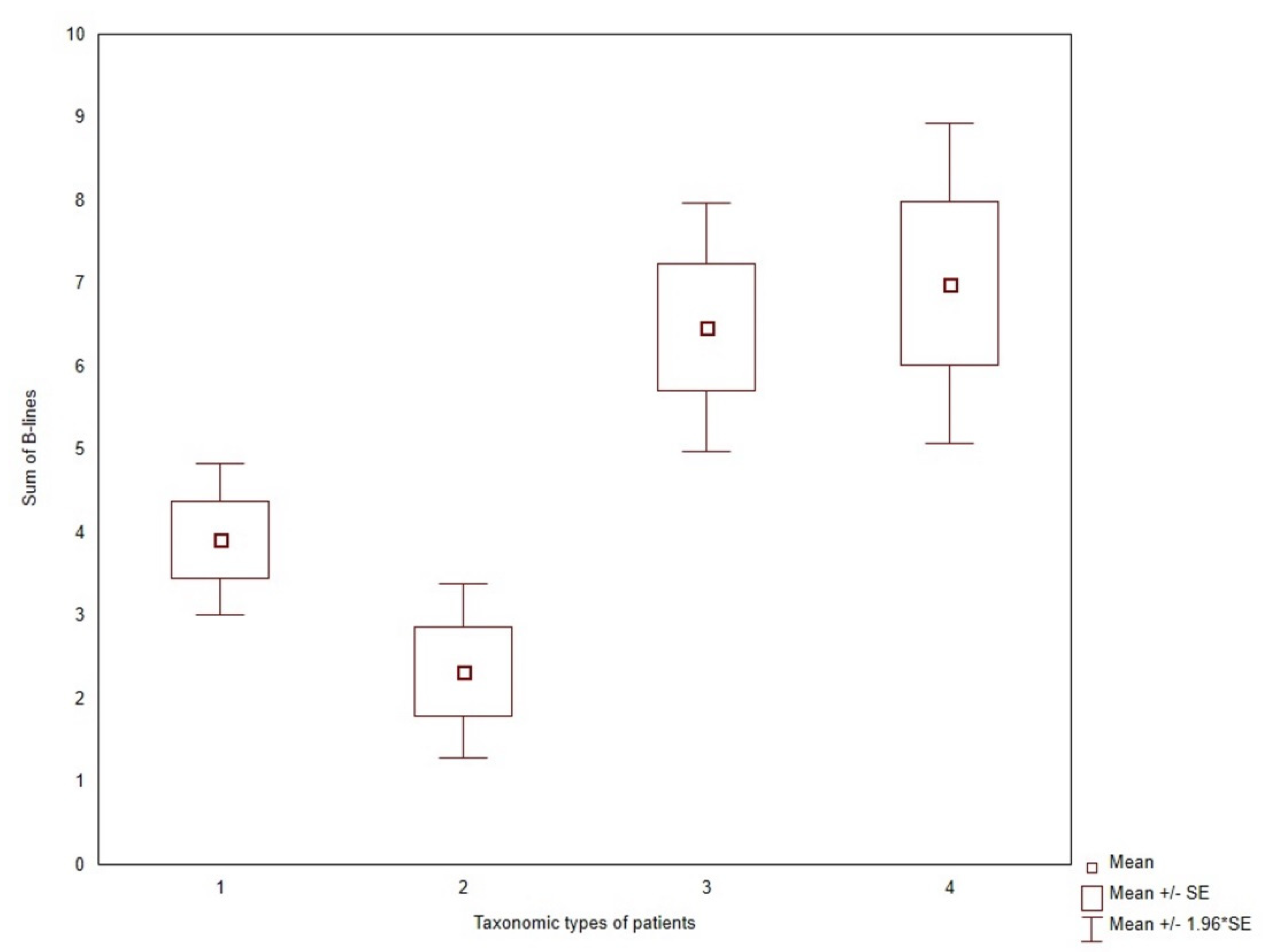
3.4. Lung Ultrasound B-Lines in Clusters of Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lichtenstein, D.; Mézière, G.; Biderman, P.; Gepner, A.; Barré, O. The comet-tail artifact. An ultrasound sign of alveolar-interstitial syndrome. Am. J. Respir. Crit. Care Med. 1997, 156, 1640–1646. [Google Scholar] [CrossRef]
- Lichtenstein, D.; Goldstein, I.; Mourgeon, E.; Cluzel, P.; Grenier, P.; Rouby, J.-J. Comparative diagnostic performances of auscultation, chest radiography, and lung ultrasonography in acute respiratory distress syndrome. Anesthesiology 2004, 100, 9–15. [Google Scholar] [CrossRef]
- Lichtenstein, D.A. BLUE-protocol and FALLS-protocol: Two applications of lung ultrasound in the critically ill. Chest 2015, 147, 1659–1670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Picano, E.; Frassi, F.; Agricola, E.; Gligorova, S.; Gargani, L.; Mottola, G. Ultrasound lung comets: A clinically useful sign of extravascular lung water. J. Am. Soc. Echocardiogr. 2006, 19, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Gargani, L.; Pang, P.S.; Frassi, F.; Miglioranza, M.; Dini, F.L.; Landi, P.; Picano, E. Persistent pulmonary congestion before discharge predicts rehospitalization in heart failure: A lung ultrasound study. Cardiovasc. Ultrasound 2015, 13, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Öhman, J.; Harjola, V.-P.; Karjalainen, P.; Lassus, J. Focused echocardiography and lung ultrasound protocol for guiding treatment in acute heart failure. ESC Heart Fail. 2018, 5, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Zoccali, C.; Torino, C.; Tripepi, R.; Tripepi, G.; D’Arrigo, G.; Postorino, M.; Gargani, L.; Sicari, R.; Picano, E.; Mallamaci, F.; et al. Pulmonary congestion predicts cardiac events and mortality in ESRD. J. Am. Soc. Nephrol. 2013, 24, 639–646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zoccali, C.; Torino, C.; Mallamaci, F.; Sarafidis, P.; Papagianni, A.; Ekart, R.; Hojs, R.; Klinger, M.; Letachowicz, K.; Fliser, D.; et al. A randomized multicenter trial on a lung ultrasound-guided treatment strategy in patients on chronic hemodialysis with high cardiovascular risk. Kidney Int. 2021, 100, 1325–1333. [Google Scholar] [CrossRef]
- Volpicelli, G.; Lamorte, A.; Villén, T. What’s new in lung ultrasound during the COVID-19 pandemic. Intensiv. Care Med. 2020, 46, 1445–1448. [Google Scholar] [CrossRef]
- Covic, A.; Siriopol, D.; Voroneanu, L. Use of Lung Ultrasound for the Assessment of Volume Status in CKD. Am. J. Kidney Dis. 2018, 71, 412–422. [Google Scholar] [CrossRef]
- Marino, F.; Martorano, C.; Tripepi, R.; Bellantoni, M.; Tripepi, G.; Mallamaci, F.; Zoccali, C. Subclinical pulmonary congestion is prevalent in nephrotic syndrome. Kidney Int. 2016, 89, 421–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciumanghel, A.; Siriopol, I.; Blaj, M.; Siriopol, D.; Gavrilovici, C.; Covic, A. B-lines score on lung ultrasound as a direct measure of respiratory dysfunction in ICU patients with acute kidney injury. Int. Urol. Nephrol. 2018, 50, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Panuccio, V.; Tripepi, R.; Parlongo, G.; Mafrica, A.; Caridi, G.; Catalano, F.; Marino, F.; Tripepi, G.; Mallamaci, F.; Zoccali, C. Lung ultrasound to detect and monitor pulmonary congestion in patients with acute kidney injury in nephrology wards: A pilot study. J. Nephrol. 2020, 33, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Mottola, C.; Girerd, N.; Coiro, S.; Lamiral, Z.; Rossignol, P.; Frimat, L.; Girerd, S. Evaluation of Subclinical Fluid Overload Using Lung Ultrasound and Estimated Plasma Volume in the Postoperative Period Following Kidney Transplantation. Transplant. Proc. 2018, 50, 1336–1341. [Google Scholar] [CrossRef]
- Vanderweckene, P.; Weekers, L.; Lancellotti, P.; Jouret, F. Controversies in the management of the haemodialysis-related arteriovenous fistula following kidney transplantation. Clin. Kidney J. 2018, 11, 406–412. [Google Scholar] [CrossRef] [Green Version]
- Malik, J.; Valerianova, A.; Tuka, V.; Trachta, P.; Bednarova, V.; Hruskova, Z.; Slavikova, M.; Rosner, M.H.; Tesar, V. The effect of high-flow arteriovenous fistulas on systemic haemodynamics and brain oxygenation. ESC Heart Fail. 2021, 8, 2165–2171. [Google Scholar] [CrossRef]
- Valerianova, A.; Malik, J.; Janeckova, J.; Kovarova, L.; Tuka, V.; Trachta, P.; Lachmanova, J.; Hladinova, Z.; Hruskova, Z.; Tesar, V. Reduction of arteriovenous access blood flow leads to biventricular unloading in haemodialysis patients. Int. J. Cardiol. 2021, 334, 148–153. [Google Scholar] [CrossRef]
- Mudoni, A.; Caccetta, F.; Caroppo, M.; Musio, F.; Accogli, A.; Zacheo, M.D.; Burzo, M.D.; Gallieni, M.; Nuzzo, V. Echo color Doppler ultrasound: A valuable diagnostic tool in the assessment of arteriovenous fistula in hemodialysis patients. J. Vasc. Access 2016, 17, 446–452. [Google Scholar] [CrossRef]
- Jambrik, Z.; Monti, S.; Coppola, V.; Agricola, E.; Mottola, G.; Miniati, M.; Picano, E. Usefulness of ultrasound lung comets as a nonradiologic sign of extravascular lung water. Am. J. Cardiol. 2004, 93, 1265–1270. [Google Scholar] [CrossRef]
- Gargani, L.; Volpicelli, G. How I do it: Lung ultrasound. Cardiovasc. Ultrasound 2014, 12, 25. [Google Scholar] [CrossRef] [Green Version]
- Gargani, L.; Sicari, R.; Raciti, M.; Serasini, L.; Passera, M.; Torino, C.; Letachowicz, K.; Ekart, R.; Fliser, D.; Covic, A.; et al. Efficacy of a remote web-based lung ultrasound training for nephrologists and cardiologists: A LUST trial sub-project. Nephrol. Dial. Transplant. 2016, 31, 1982–1988. [Google Scholar] [CrossRef]
- Abreo, K.; Sachdeva, B.; Abreo, A.P. To ligate or not to ligate hemodialysis arteriovenous fistulas in kidney transplant patients. J. Vasc. Access 2021, 22, 942–946. [Google Scholar] [CrossRef] [PubMed]
- Letachowicz, K.; Banasik, M.; Królicka, A.; Mazanowska, O.; Gołębiowski, T.; Augustyniak-Bartosik, H.; Zmonarski, S.; Kamińska, D.; Kuriata-Kordek, M.; Krajewska, M. Vascular Access Perspectives in Patients After Kidney Transplantation. Front. Surg. 2021, 8, 640986. [Google Scholar] [CrossRef] [PubMed]
- Torino, C.; Gargani, L.; Sicari, R.; Letachowicz, K.; Ekart, R.; Fliser, D.; Covic, A.; Siamopoulos, K.; Stavroulopoulos, A.; Massy, Z.A.; et al. Inflammation is an amplifier of lung congestion by high lv filling pressure in hemodialysis patients: A longitudinal study. J. Nephrol. 2020, 33, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Cluster: Cluster Analysis Basics and Extensions. R Package Version 2.1.2. Available online: https://cran.rproject.org/web/packages/cluster/cluster.pdf (accessed on 5 December 2021).
- R Core Team. A Language and Environment for Statistical Computing, version 4.1.2; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.r-project.org (accessed on 5 December 2021).
- Marczewski, E.; Steinhaus, H. On a certain distance of sets and the corresponding distance of functions. Colloq. Math. 1958, 6, 319–327. [Google Scholar] [CrossRef]
- Tukiendorf, A.; Kaźmierski, R.; Michalak, S. The taxonomy statistic uncovers novel clinical patterns in a population of ischemic stroke patients. PLoS ONE 2013, 8, e69816. [Google Scholar] [CrossRef] [Green Version]
- Miglioranza, M.H.; Gargani, L.; Sant’Anna, R.T.; Rover, M.M.; Martins, V.M.; Mantovani, A.; Weber, C.; Moraes, M.A.; Feldman, C.J.; Kalil, R.A.K.; et al. Lung ultrasound for the evaluation of pulmonary congestion in outpatients: A comparison with clinical assessment, natriuretic peptides, and echocardiography. JACC Cardiovasc. Imaging 2013, 6, 1141–1151. [Google Scholar] [CrossRef] [Green Version]
- Picano, E.; Scali, M.C. The lung water cascade in heart failure. Echocardiography 2017, 34, 1503–1507. [Google Scholar] [CrossRef]
- Dwyer, K.H.; Merz, A.; Lewis, E.F.; Claggett, B.L.; Crousillat, D.R.; Lau, E.S.; Silverman, M.B.; Peck, J.; Rivero, J.; Cheng, S.; et al. Pulmonary Congestion by Lung Ultrasound in Ambulatory Patients with Heart Failure with Reduced or Preserved Ejection Fraction and Hypertension. J. Card. Fail. 2018, 24, 219–226. [Google Scholar] [CrossRef]
- Torino, C.; Tripepi, R.; Loutradis, C.; Sarafidis, P.; Tripepi, G.; Mallamaci, F.; Zoccali, C. Can the assessment of ultrasound lung water in haemodialysis patients be simplified? Nephrol. Dial. Transplant. 2021, 36, 2321–2326. [Google Scholar] [CrossRef]
- Palazzuoli, A.; Ruocco, G.; Franci, B.; Evangelista, I.; Lucani, B.; Nuti, R.; Pellicori, P. Ultrasound indices of congestion in patients with acute heart failure according to body mass index. Clin. Res. Cardiol. 2020, 109, 1423–1433. [Google Scholar] [CrossRef]
- Brainin, P.; Claggett, B.; Lewis, E.F.; Dwyer, K.H.; Merz, A.A.; Silverman, M.B.; Swamy, V.; Biering-Sørensen, T.; Rivero, J.; Cheng, S.; et al. Body mass index and B-lines on lung ultrasonography in chronic and acute heart failure. ESC Heart Fail. 2020, 7, 1201–1209. [Google Scholar] [CrossRef] [Green Version]
- Torino, C.; Gargani, L.; Sicari, R.; Letachowicz, K.; Ekart, R.; Fliser, D.; Covic, A.; Siamopoulos, K.; Stavroulopoulos, A.; Massy, Z.A.; et al. The Agreement between Auscultation and Lung Ultrasound in Hemodialysis Patients: The LUST Study. Clin. J. Am. Soc. Nephrol. 2016, 11, 2005–2011. [Google Scholar] [CrossRef]
- Coiro, S.; Rossignol, P.; Ambrosio, G.; Carluccio, E.; Alunni, G.; Murrone, A.; Tritto, I.; Zannad, F.; Girerd, N. Prognostic value of residual pulmonary congestion at discharge assessed by lung ultrasound imaging in heart failure. Eur. J. Heart. Fail. 2015, 17, 1172–1181. [Google Scholar] [CrossRef]
- Platz, E.; Merz, A.; Jhund, P.; Vazir, A.; Campbell, R.; Mcmurray, J. Dynamic changes and prognostic value of pulmonary congestion by lung ultrasound in acute and chronic heart failure: A systematic review. Eur. J. Heart Fail. 2017, 19, 1154–1163. [Google Scholar] [CrossRef] [PubMed]
- Miglioranza, M.H.; Picano, E.; Badano, L.; Sant’Anna, R.; Rover, M.; Zaffaroni, F.; Sicari, R.; Kalil, R.K.; Leiria, T.L.; Gargani, L. Pulmonary congestion evaluated by lung ultrasound predicts decompensation in heart failure outpatients. Int. J. Cardiol. 2017, 240, 271–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Platz, E.; Campbell, R.T.; Claggett, B.; Lewis, E.F.; Groarke, J.D.; Docherty, K.; Lee, M.; Merz, A.; Silverman, M.; Swamy, V.; et al. Lung Ultrasound in Acute Heart Failure: Prevalence of Pulmonary Congestion and Short- and Long-Term Outcomes. JACC Heart Fail. 2019, 7, 849–858. [Google Scholar] [CrossRef] [PubMed]
- Gargani, L.; Pugliese, N.R.; Frassi, F.; Frumento, P.; Poggianti, E.; Mazzola, M.; De Biase, N.; Landi, P.; Masi, S.; Taddei, S.; et al. Prognostic value of lung ultrasound in patients hospitalized for heart disease irrespective of symptoms and ejection fraction. ESC Heart Fail. 2021, 8, 2660–2669. [Google Scholar] [CrossRef] [PubMed]
- Šrajer, L.L.; Marko, K.; Hojs, N.V.; Piko, N.; Bevc, S.; Hojs, R.; Ekart, R. Lung ultrasound, hemoglobin, and NT-proBNP in peritoneal dialysis patients. Clin. Nephrol. 2021, 96, 85–88. [Google Scholar] [CrossRef]
- Saad, M.M.; Kamal, J.; Moussaly, E.; Karam, B.; Mansour, W.; Gobran, E.; Abbasi, S.H.; Mahgoub, A.; Singh, P.; Hardy, R.; et al. Relevance of B-Lines on Lung Ultrasound in Volume Overload and Pulmonary Congestion: Clinical Correlations and Outcomes in Patients on Hemodialysis. Cardiorenal Med. 2018, 8, 83–91. [Google Scholar] [CrossRef]
- Pellicori, P.; Shah, P.; Cuthbert, J.; Urbinati, A.; Zhang, J.; Kallvikbacka-Bennett, A.; Clark, A.L.; Cleland, J.G. Prevalence, pattern and clinical relevance of ultrasound indices of congestion in outpatients with heart failure. Eur. J. Heart Fail. 2019, 21, 904–916. [Google Scholar] [CrossRef]
- Rao, N.N.; Stokes, M.B.; Rajwani, A.; Ullah, S.; Williams, K.; King, D.; Macaulay, E.; Russell, C.H.; Olakkengil, S.; Carroll, R.P.; et al. Effects of Arteriovenous Fistula Ligation on Cardiac Structure and Function in Kidney Transplant Recipients. Circulation 2019, 139, 2809–2818. [Google Scholar] [CrossRef] [PubMed]
- Hetz, P.; Pirklbauer, M.; Müller, S.; Posch, L.; Gummerer, M.; Tiefenthaler, M. Prophylactic Ligature of AV Fistula Prevents High Output Heart Failure after Kidney Transplantation. Am. J. Nephrol. 2020, 51, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Golper, T.A.; Hartle, P.M.; Bian, A. Arteriovenous fistula creation may slow estimated glomerular filtration rate trajectory. Nephrol. Dial. Transplant. 2015, 30, 2014–2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weekers, L.; Vanderweckene, P.; Castanares-Zapatero, D.; Bonvoisin, C.; Hamoir, E.; Maweja, S.; Krzesinski, J.-M.; Delanaye, P.; Pottel, H.; Jouret, F. The closure of arteriovenous fistula in kidney transplant recipients is associated with an acceleration of kidney function decline. Nephrol. Dial. Transplant. 2017, 32, 196–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bardowska, K.; Letachowicz, K.; Kamińska, D.; Kusztal, M.; Gołębiowski, T.; Królicki, T.; Zajdel, K.; Mazanowska, O.; Janczak, D.; Krajewska, M. The attitude of kidney transplant recipients towards elective arteriovenous fistula ligation. PLoS ONE 2020, 15, e0234931. [Google Scholar] [CrossRef]
- Trampuž, B.V.; Arnol, M.; Gubenšek, J.; Ponikvar, R.; Ponikvar, J.B. A national cohort study on hemodialysis arteriovenous fistulas after kidney transplantation–Long-term patency, use and complications. BMC Nephrol. 2021, 22, 344. [Google Scholar] [CrossRef]
- Letachowicz, K.; Kusztal, M.; Gołębiowski, T.; Letachowicz, W.; Weyde, W.; Klinger, M. External dilator-assisted banding for high-flow hemodialysis arteriovenous fistula. Ren. Fail. 2016, 38, 1067–1070. [Google Scholar] [CrossRef]
- Bojakowski, K.; Gziut, A.; Góra, R.; Foroncewicz, B.; Kaźmierczak, S.; Kasprzak, D.; Małyszko, J.; Andziak, P. To Close, Observe, or Reconstruct: The Third Way of Managing Dialysis Fistula Aneurysms in Kidney Transplant Recipients. J. Clin. Med. 2021, 10, 4567. [Google Scholar] [CrossRef]
- Iwakura, K.; Onishi, T. A practical guide to the lung ultrasound for the assessment of congestive heart failure. J. Echocardiogr. 2021, 19, 195–204. [Google Scholar] [CrossRef]
- Yang, F.; Wang, Q.; Zhi, G.; Zhang, L.; Huang, D.; Dangsheng, H.; Zhang, M. The application of lung ultrasound in acute decompensated heart failure in heart failure with preserved and reduced ejection fraction. Echocardiography 2017, 34, 1462–1469. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | AVF Present n = 82 | AVF Absent n = 74 | p-Value |
|---|---|---|---|
| Sum of B-lines | 5.5 ± 5.0 | 4.8 ± 4.9 | 0.3507 |
| Age (years) | 56.4 ± 10.9 | 54.1 ± 12.2 | 0.2137 |
| Male, n (%) | 56 (68.3%) | 42 (56.7 %) | 0.1397 |
| BMI (kg/m2) | 27.0 ± 4.3 | 26.6 ± 5.4 | 0.5612 |
| Serum creatinine concentration (mg/dL) | 1.45 ± 0.50 | 1.47 ± 0.55 | 0.7658 |
| eGFR (mL/min/1.73m2) | 53.5 ± 14.7 | 53.2 ± 17.1 | 0.9802 |
| Duration between study visit and transplantation (months) | 90 ± 57 | 129 ± 66 | 0.0001 |
| Duration between study visit and RRT initiation (months) | 144 ± 81 | 174 ± 72 | 0.0154 |
| First transplantation, n (%) | 68 (82.9%) | 64 (86.5%) | 0.8753 |
| Diabetes mellitus, n (%) | 19 (23.2%) | 15 (20.3%) | 0.6641 |
| Heart disease, n (%) | 32 (39%) | 20 (27%) | 0.1141 |
| Charlson comorbidity index | 4.5 ± 2.0 | 4.3 ± 1.6 | 0.4179 |
| Smoking, current or previous, n (%) | 38 (46.3%) | 34 (45.9%) | 0.9114 |
| Medications, n (%) | |||
| Steroids, calcineurin inhibitor, mycophenolate, n (%) | 66 (80.5%) | 53 (71.6%) | 0.2663 |
| Antihypertensive, n (%) | 75 (91.5%) | 66 (89.2%) | 0.8346 |
| Statins, n (%) | 33 (40.2%) | 26 (35.1%) | 0.6229 |
| Antiplatelet/anticoagulants, n (%) | 24 (29.3%) | 14 (18.9%) | 0.1879 |
| Characteristics | No Congestion n = 101 | Mild Congestion n = 49 | Moderate Congestion n = 6 | p-Value |
|---|---|---|---|---|
| Sum of B-lines | 2.2 ± 1.5 | 9.4 ± 2.7 | 20.3 ± 4.7 | <0.001 |
| Age (years) | 53.9 ± 12 | 57.1 ± 10.4 | 64.3 ± 4 | 0.0356 |
| Male, n (%) | 59 (58.4%) | 35 (71.4%) | 4 (66.7%) | 0.2965 |
| BMI (kg/m2) | 25.9 ± 4.6 | 28.5 ± 5 | 28.9 ± 4.6 | 0.0048 |
| Serum creatinine concentration, (mg/dL) | 1.39 ± 0.46 | 1.58 ± 0.64 | 1.67 ± 0.33 | 0.044 |
| eGFR (mL/min/1.73 m2) | 55.3 ± 15.5 | 50.7 ± 16.3 | 42.2 ± 10.9 | 0.0503 |
| Duration between study visit and transplantation (months) | 106 ± 64 | 115 ± 677 | 95 ± 43 | 0.65 |
| Duration between study visit and RRT initiation, (months) | 157 ± 82 | 164 ± 73 | 141 ± 54 | 0.68 |
| Prior diabetes mellitus, n (%) | 17 (16.8%) | 13 (26.5%) | 4 (66.7%) | 0.0101 |
| Prior heart disease, n (%) | 22 (21.8%) | 25 (51%) | 5 (83.3%) | <0.0001 |
| Charlson comorbidity index | 4.1 ± 1.7 | 4.7 ± 1.7 | 6.8 ± 1.5 | 0.0005 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| Risk Factor | OR | 95% CI | p | OR | 95% CI | p |
| Charlson comorbidity index | 1.21 | (1.03,1.44) | 0.0233 | 1.07 | (0.89,1.29) | 0.4537 |
| Heart disease | 2.45 | (1.31,4.58) | 0.0049 | 1.24 | (0.61,2.50) | 0.5423 |
| Symptoms of volume overload | 7.50 | (3.32,17.0) | <0.0001 | 5.90 | (2.43,14.3) | 0.0001 |
| BMI | 1.09 | (1.03,1.16) | 0.0026 | 1.09 | (1.03,1.17) | 0.0046 |
| eGFR | 0.98 | (0.96,0.99) | 0.0057 | 1.29 | (0.51,3.26) | 0.5721 |
| Uric acid | 1.44 | (1.16,1.78) | 0.0009 | 0.97 | (0.94,1.01) | 0.1132 |
| Cholesterol | 0.993 | (0.988,0.999) | 0.0160 | 0.994 | (0.988,1.000) | 0.0452 |
| Donor age | 1.03 | (1.01,1.05) | 0.0122 | 1.01 | (0.99,1.03) | 0.4657 |
| Risk Factor | n = 61 | n = 18 | n = 32 | n = 45 | p-Value |
|---|---|---|---|---|---|
| Charlson comorbidity index | 3.36 ± 0.88 | 2.83 ± 0.79 | 4.28 ± 1.20 | 6.44 ± 1.49 | <0.0001 |
| BMI | 27.5 ± 5.22 | 20.9 ± 2.03 | 29.2 ± 3.54 | 26.6 ± 4.06 | <0.0001 |
| Cholesterol | 251 ± 54.3 | 212 ± 32.8 | 166 ± 17.0 | 222 ± 38.5 | <0.0001 |
| Males | 59% | 56% | 34% | 38% | 0.0555 |
| Age | 51.0 ± 10.1 | 45.6 ± 10.2 | 56.2 ± 10.9 | 64.4 ± 7.5 | <0.0001 |
| Heart disease | 18% | 17% | 47% | 51% | 0.0004 |
| Diabetes | 13% | 0% | 28% | 38% | 0.0013 |
| Symptoms of volume overload | 8% | 11% | 13% | 29% | 0.0261 |
| USBLs | 3.9 ± 3.6 | 2.3 ± 2.3 | 6.5 ± 4.3 | 7.0 ± 6.6 | 0.0003 |
| Presence of AVF | 41% | 44% | 66% | 62% | 0.0539 |
| AVF burden | 80.1 ± 58.9 | 83.3 ± 86.6 | 108.1 ± 69.7 | 120.8 ± 83.3 | 0.0247 |
| Weight | 80.4 ± 16.5 | 61.7 ± 11.3 | 87.3 ± 12.7 | 76.4 ± 12.9 | <0.0001 |
| Waist | 94.2 ± 13.5 | 78.4 ± 10.1 | 102 ± 12.3 | 96.0 ± 12.5 | <0.0001 |
| Serum creatinine | 1.45 ± 0.42 | 1.59 ± 0.76 | 1.43 ± 0.40 | 1.45 ± 0.61 | 0.7558 |
| eGFR | 54.0 ± 16.0 | 50.4 ± 17.7 | 53.7 ± 14.5 | 53.4 ± 16.2 | 0.8715 |
| Platelets | 239 ± 66.6 | 216 ± 37.0 | 205 ± 51.7 | 198 ± 53.9 | 0.0021 |
| Uric acid | 7.12 ± 1.14 | 6.25 ± 1.37 | 7.21 ± 1.36 | 6.90 ± 1.42 | 0.0598 |
| Total protein | 7.22 ± 0.45 | 7.16 ± 0.50 | 7.00 ± 0.48 | 6.94 ± 0.53 | 0.0176 |
| Albumin | 4.33 ± 0.26 | 4.34 ± 0.26 | 4.28 ± 0.32 | 4.15 ± 0.30 | 0.0060 |
| HDL cholesterol | 63.0 ± 17.7 | 61.9 ± 10.6 | 52.5 ± 10.7 | 63.8 ± 15.1 | 0.0061 |
| LDL cholesterol | 153 ± 43.4 | 127 ± 28.4 | 85.6 ± 22.5 | 123 ± 33.0 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Letachowicz, K.; Królicka, A.; Tukiendorf, A.; Banasik, M.; Kamińska, D.; Gołębiowski, T.; Kuriata-Kordek, M.; Madziarska, K.; Mazanowska, O.; Krajewska, M. Lung Congestion Severity in Kidney Transplant Recipients Is Not Affected by Arteriovenous Fistula Function. J. Clin. Med. 2022, 11, 842. https://doi.org/10.3390/jcm11030842
Letachowicz K, Królicka A, Tukiendorf A, Banasik M, Kamińska D, Gołębiowski T, Kuriata-Kordek M, Madziarska K, Mazanowska O, Krajewska M. Lung Congestion Severity in Kidney Transplant Recipients Is Not Affected by Arteriovenous Fistula Function. Journal of Clinical Medicine. 2022; 11(3):842. https://doi.org/10.3390/jcm11030842
Chicago/Turabian StyleLetachowicz, Krzysztof, Anna Królicka, Andrzej Tukiendorf, Mirosław Banasik, Dorota Kamińska, Tomasz Gołębiowski, Magdalena Kuriata-Kordek, Katarzyna Madziarska, Oktawia Mazanowska, and Magdalena Krajewska. 2022. "Lung Congestion Severity in Kidney Transplant Recipients Is Not Affected by Arteriovenous Fistula Function" Journal of Clinical Medicine 11, no. 3: 842. https://doi.org/10.3390/jcm11030842