
Direct Photocoagulation for Treating Microaneurysms with Hyperreflective Ring in Eyes with Refractory Macular Edema Associated with Branch Retinal Vein Occlusion

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Examinations
2.2. Assessment of the Hyperreflective Rings and Laser Setting
2.3. Assessment of Central Macular Volume and Parafoveal Macular Volume by Optical Coherence Tomography Map
2.4. Endpoints
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
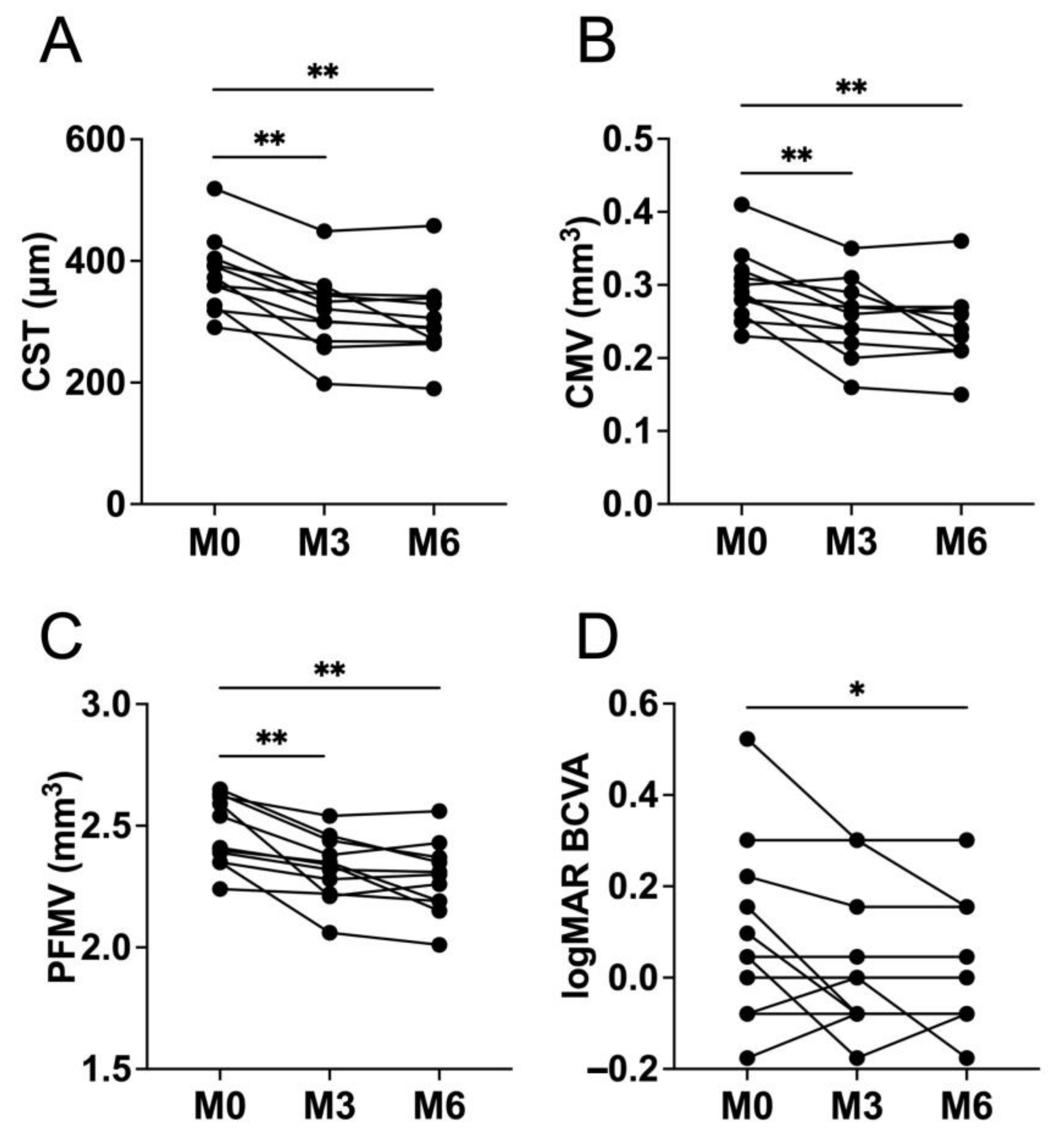
3.2. Changes in the Central Subfield Thickness, Central Macular Volume, and Parafoveal Macular Volume
3.3. Correlation of the Largest Microaneurysm Size with Central Subfield Thickness, Central Macular Volume, and Parafoveal Macular Volume
3.4. Changes in the Best-Corrected Visual Acuity and Complications
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- The Branch Vein Occlusion Study Group. Argon laser photocoagulation for macular edema in branch vein occlusion. Am. J. Ophthalmol. 1984, 98, 271–282. [Google Scholar] [CrossRef]
- Glacet-Bernard, A.; Coscas, G.; Chabanel, A.; Zourdani, A.; Lelong, F.; Samama, M.M. Prognostic factors for retinal vein occlusion: Prospective study of 175 cases. Ophthalmology 1996, 103, 551–560. [Google Scholar] [CrossRef]
- Rogers, S.L.; McIntosh, R.L.; Lim, L.; Mitchell, P.; Cheung, N.; Kowalski, J.W.; Nguyen, H.P.; Wang, J.J.; Wong, T.Y. Natural history of branch retinal vein occlusion: An evidence-based systematic review. Ophthalmology 2010, 117, 1094–1101. [Google Scholar] [CrossRef]
- Campochiaro, P.A.; Heier, J.S.; Feiner, L.; Gray, S.; Saroj, N.; Rundle, A.C.; Murahashi, W.Y.; Rubio, R.G.; BRAVO Investigators. Ranibizumab for macular edema following branch retinal vein occlusion: Six-month primary end point results of a phase III study. Ophthalmology 2010, 117, 1102–1112. [Google Scholar] [CrossRef]
- Campochiaro, P.A.; Clark, W.L.; Boyer, D.S.; Heier, J.S.; Brown, D.M.; Vitti, R.; Kazmi, H.; Berliner, A.J.; Erickson, K.; Chu, K.W.; et al. Intravitreal aflibercept for macular edema following branch retinal vein occlusion: The 24-week results of the VIBRANT study. Ophthalmology 2015, 122, 538–544. [Google Scholar] [CrossRef] [PubMed]
- Murata, T.; Kondo, M.; Inoue, M.; Nakao, S.; Osaka, R.; Shiragami, C.; Sogawa, K.; Mochizuki, A.; Shiraga, R.; Ohashi, Y.; et al. The randomized ZIPANGU trial of ranibizumab and adjunct laser for macular edema following branch retinal vein occlusion in treatment-naïve patients. Sci. Rep. 2021, 11, 551. [Google Scholar] [CrossRef] [PubMed]
- Heier, J.S.; Campochiaro, P.A.; Yau, L.; Li, Z.; Saroj, N.; Rubio, R.G.; Lai, P. Ranibizumab for macular edema due to retinal vein occlusions: Long-term follow-up in the HORIZON trial. Ophthalmology 2012, 119, 802–809. [Google Scholar] [CrossRef] [PubMed]
- Campochiaro, P.A.; Sophie, R.; Pearlman, J.; Brown, D.M.; Boyer, D.S.; Heier, J.S.; Marcus, D.M.; Feiner, L.; Patel, A.; RETAIN Study Group. Long-term outcomes in patients with retinal vein occlusion treated with ranibizumab: The RETAIN study. Ophthalmology 2014, 121, 209–219. [Google Scholar] [CrossRef]
- Tomiyasu, T.; Hirano, Y.; Yoshida, M.; Suzuki, N.; Nishiyama, T.; Uemura, A.; Yasukawa, T.; Ogura, Y. Microaneurysms cause refractory macular edema in branch retinal vein occlusion. Sci. Rep. 2016, 6, 29445. [Google Scholar] [CrossRef]
- Sakimoto, S.; Kamei, M.; Sakaguchi, H.; Suzuki, M.; Matsumura, N.; Nishida, K.; Nishida, K. Direct photocoagulation to leakage points to treat chronic macular edema associated with branch retinal vein occlusion: A pilot study. Clin. Ophthalmol. 2014, 8, 2055–2060. [Google Scholar] [CrossRef] [Green Version]
- Writing Committee for the Diabetic Retinopathy Clinical Research Network; Fong, D.S.; Strauber, S.F.; Aiello, L.P.; Beck, R.W.; Callanan, D.G.; Danis, R.P.; Davis, M.D.; Feman, S.S.; Ferris, F. Comparison of the modified Early Treatment Diabetic Retinopathy Study and mild grid laser photocoagulation strategies for diabetic macular edema. Arch. Ophthalmol. 2007, 125, 469–480. [Google Scholar]
- Aiello, L.P.; Edwards, A.R.; Beck, R.W.; Bressler, N.M.; Davis, M.D.; Ferris, F.; Glassman, A.R.; Ip, M.S.; Miller, L.M.; Diabetic Retinopathy Clinical Research Network. Factors associated with improvement and worsening of visual acuity 2 years after focal/grid photocoagulation for diabetic macular edema. Ophthalmology 2010, 117, 946–953. [Google Scholar] [CrossRef] [Green Version]
- Blair, N.P.; Shahidi, M.; Lai, W.W.; Zelkha, R. Correlation between microaneurysms and retinal thickness in diabetic macular edema. Retina 2008, 28, 1097–1103. [Google Scholar] [CrossRef] [Green Version]
- Bolz, M.; Schmidt-Erfurth, U.; Deak, G.; Mylonas, G.; Kriechbaum, K.; Scholda, C.; Diabetic Retinopathy Research Group Vienna. Optical coherence tomographic hyperreflective foci: A morphologic sign of lipid extravasation in diabetic macular edema. Ophthalmology 2009, 116, 914–920. [Google Scholar] [CrossRef]
- Horii, T.; Murakami, T.; Nishijima, K.; Sakamoto, A.; Ota, M.; Yoshimura, N. Optical coherence tomographic characteristics of microaneurysms in diabetic retinopathy. Am. J. Ophthalmol. 2010, 150, 840–848. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Chhablani, J.; Freeman, W.R.; Chan, C.K.; Kozak, I.; Bartsch, D.U.; Cheng, L. Characterization of diabetic microaneurysms by simultaneous fluorescein angiography and spectral-domain optical coherence tomography. Am. J. Ophthalmol. 2012, 153, 861–867. [Google Scholar] [CrossRef] [Green Version]
- Byeon, S.H.; Chu, Y.K.; Hong, Y.T.; Kim, M.; Kang, H.M.; Kwon, O.W. New insights into the pathoanatomy of diabetic macular edema: Angiographic patterns and optical coherence tomography. Retina 2012, 32, 1087–1099. [Google Scholar] [CrossRef]
- Shin, J.Y.; Byeon, S.H.; Kwon, O.W. Optical coherence tomography-guided selective focal laser photocoagulation: A novel laser protocol for diabetic macular edema. Graefes Arch. Clin. Exp. Ophthalmol. 2015, 253, 527–535. [Google Scholar] [CrossRef]
- Paques, M.; Philippakis, E.; Bonnet, C.; Falah, S.; Ayello-Scheer, S.; Zwillinger, S.; Girmens, J.F.; Dupas, B. Indocyanine-green-guided targeted laser photocoagulation of capillary macroaneurysms in macular oedema: A pilot study. Br. J. Ophthalmol. 2017, 101, 170–174. [Google Scholar] [CrossRef]
- Bresnick, G.H.; Davis, M.D.; Myers, F.L.; de Venecia, G. Clinicopathologic correlations in diabetic retinopathy. Ⅱ. Clinical and histologic appearances of retinal capillary microaneurysms. Arch. Ophthalmol. 1977, 95, 1215–1220. [Google Scholar] [CrossRef]
- Trempe, C.L.; Mainster, M.A.; Pomerantzeff, O.; Avila, M.P.; Jalkh, A.E.; Weiter, J.J.; McMeel, J.W.; Schepens, C.L. Macular photocoagulation. Optimal wavelength selection. Ophthalmology 1982, 89, 721–728. [Google Scholar] [CrossRef]
- Ulbig, M.W.; McHugh, D.A.; Hamilton, A.M. Diode laser photocoagulation for diabetic macular oedema. Br. J. Ophthalmol. 1995, 79, 318–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| No. of eyes | 11 |
| Age (years) | 70 ± 12.8 |
| Sex (male/female) | 3/8 |
| Eye (right/left) | 4/7 |
| Lens status (phakic/pseudophakic) | 6/5 |
| Duration before initial laser treatment (months) | 42 ± 35.3 |
| logMAR BCVA | 0.096 ± 0.2 |
| Central subfield thickness (μm) | 378.7 ± 61.8 |
| Central macular volume (mm3) | 0.3 ± 0.049 |
| Parafoveal macular volume (mm3) | 2.5 ± 0.14 |
| No. of hyperreflective rings | 3.5 ± 2.0 |
| Largest MA size (μm) | 134.3 ± 51.5 |
| Distance between the fovea and closest MA (μm) | 1966.7 ± 738.2 |
| Case | Age | Period (M) | Previous Treatment (Times) | No. of MA | Largest MA (μm) | Distance to Fovea (μm) | logMAR BCVA | CST (μm) | CMV (mm3) | PFMV (mm3) | Additional Laser | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 M | 3 M | 6 M | 0 M | 3 M | 6 M | 0 M | 3 M | 6 M | 0 M | 3 M | 6 M | ||||||||
| 1 | 63 | 12 | Anti-VEGF (3), STTA (1) | 5 | 85 | 1861 | −0.079 | 0 | −0.18 | 431 | 344 | 329 | 0.34 | 0.27 | 0.26 | 2.65 | 2.46 | 2.35 | 3 M |
| 2 | 71 | 94 | Anti-VEGF (40), scatter laser | 3 | 205 | 2193 | 0.046 | 0.046 | 0.046 | 391 | 321 | 306 | 0.31 | 0.29 | 0.24 | 2.41 | 2.34 | 2.15 | None |
| 3 | 58 | 30 | Anti-VEGF (10) | 4 | 110 | 980 | 0 | 0 | 0 | 404 | 333 | 339 | 0.32 | 0.26 | 0.27 | 2.54 | 2.38 | 2.43 | 3, 4 M |
| 4 | 78 | 24 | Anti-VEGF (9), scatter laser | 1 | 88 | 1769 | −0.18 | −0.079 | −0.079 | 291 | 268 | 267 | 0.23 | 0.22 | 0.21 | 2.39 | 2.32 | 2.31 | None |
| 5 | 88 | 51 | Anti-VEGF (17), scatter laser | 4 | 199 | 2684 | 0.52 | 0.3 | 0.3 | 519 | 449 | 458 | 0.41 | 0.35 | 0.36 | 2.62 | 2.54 | 2.56 | 1, 3, 4 M |
| 6 | 58 | 12 | Anti-VEGF (3), scatter laser | 2 | 85 | 960 | 0.15 | −0.079 | −0.079 | 393 | 359 | 271 | 0.3 | 0.31 | 0.21 | 2.4 | 2.35 | 2.19 | None |
| 7 | 71 | 14 | Anti-VEGF (3) | 2 | 143 | 1887 | 0.22 | 0.15 | 0.15 | 327 | 198 | 190 | 0.26 | 0.16 | 0.15 | 2.35 | 2.06 | 2.01 | None |
| 8 | 48 | 33 | Anti-VEGF (3), IVTA (6), scatter laser | 8 | 140 | 2036 | 0.097 | −0.079 | −0.079 | 359 | 301 | 289 | 0.28 | 0.24 | 0.23 | 2.63 | 2.44 | 2.37 | 1, 3 M |
| 9 | 71 | 113 | Anti-VEGF (16) | 3 | 113 | 2415 | 0.046 | −0.18 | −0.079 | 319 | 300 | 291 | 0.25 | 0.24 | 0.23 | 2.35 | 2.28 | 2.3 | 1, 3 M |
| 10 | 90 | 12 | Anti-VEGF (3) | 5 | 90 | 1372 | 0.3 | 0.3 | 0.15 | 373 | 258 | 264 | 0.29 | 0.2 | 0.21 | 2.59 | 2.21 | 2.26 | None |
| 11 | 74 | 67 | Anti-VEGF (3), vitrectomy, scatter laser | 2 | 219 | 3477 | −0.079 | −0.079 | −0.079 | 359 | 346 | 342 | 0.28 | 0.27 | 0.27 | 2.24 | 2.22 | 2.19 | None |
| OCT-Guided Laser (This Study) | FA-Guided Laser * | |
|---|---|---|
| No. of eyes | 11 | 16 |
| Age (years) | 70 ± 12.8 | 72.0 ± 6.3 |
| Period between the initial visit and the initial laser treatment (M) | 42 ± 35 | 20.9 ± 9.9 |
| Follow-up period from the initial laser treatment (M) | 6 | 20.3 ± 8.0 |
| No. of applications of laser treatment | 1.9 ± 1.1 | 1.7 ± 0.9 |
| Central subfield thickness (μm) | ||
| Baseline | 378.7 ± 61.8 | 465.0 ± 107.6 |
| 3 M following initial laser treatment | 316.1 ± 64.5 | 355.3 ± 91.3 |
| 6 M following initial laser treatment | 304.2 ± 66.7 | 334.3 ± 68.8 |
| BCVA (logMAR) | ||
| Baseline | 0.096 ± 0.2 | 0.39 ± 0.28 |
| 3 M following initial laser treatment | 0.028 ± 0.16 | 0.31 ± 0.23 |
| 6 M following initial laser treatment | 0.0077 ± 0.14 | 0.24 ± 0.22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sasajima, H.; Zako, M.; Ueta, Y.; Tate, H.; Otaki, C.; Murotani, K.; Suzuki, T.; Ishida, H.; Hashimoto, Y.; Tachi, N. Direct Photocoagulation for Treating Microaneurysms with Hyperreflective Ring in Eyes with Refractory Macular Edema Associated with Branch Retinal Vein Occlusion. J. Clin. Med. 2022, 11, 823. https://doi.org/10.3390/jcm11030823
Sasajima H, Zako M, Ueta Y, Tate H, Otaki C, Murotani K, Suzuki T, Ishida H, Hashimoto Y, Tachi N. Direct Photocoagulation for Treating Microaneurysms with Hyperreflective Ring in Eyes with Refractory Macular Edema Associated with Branch Retinal Vein Occlusion. Journal of Clinical Medicine. 2022; 11(3):823. https://doi.org/10.3390/jcm11030823
Chicago/Turabian StyleSasajima, Hirofumi, Masahiro Zako, Yoshiki Ueta, Hideo Tate, Chisato Otaki, Kenta Murotani, Takafumi Suzuki, Hidetoshi Ishida, Yoshihiro Hashimoto, and Naoko Tachi. 2022. "Direct Photocoagulation for Treating Microaneurysms with Hyperreflective Ring in Eyes with Refractory Macular Edema Associated with Branch Retinal Vein Occlusion" Journal of Clinical Medicine 11, no. 3: 823. https://doi.org/10.3390/jcm11030823