
Mobile Single-Lead Electrocardiogram Technology for Atrial Fibrillation Detection in Acute Ischemic Stroke Patients

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics and Recruitment
2.2. Feasibility
- -
- source of recruitment: at stroke unit;
- -
- recruitment rates: from the AIS patients treated at the stroke unit, the number of eligible AIS patients was determined using inclusion and exclusion criteria (≥20%);
- -
- withdrawal rates (before intervention): AIS patients who gave preconsent to participate but withdrew it before the start of intervention were accounted for. AIS patients for whom the device was not available were counted (≤20%);
- -
- withdrawal rates (during the course of intervention): AIS patients who received a tablet and the KM pad for three days but for whom there was no ECG registration on the device were accounted for (≤10%);
- -
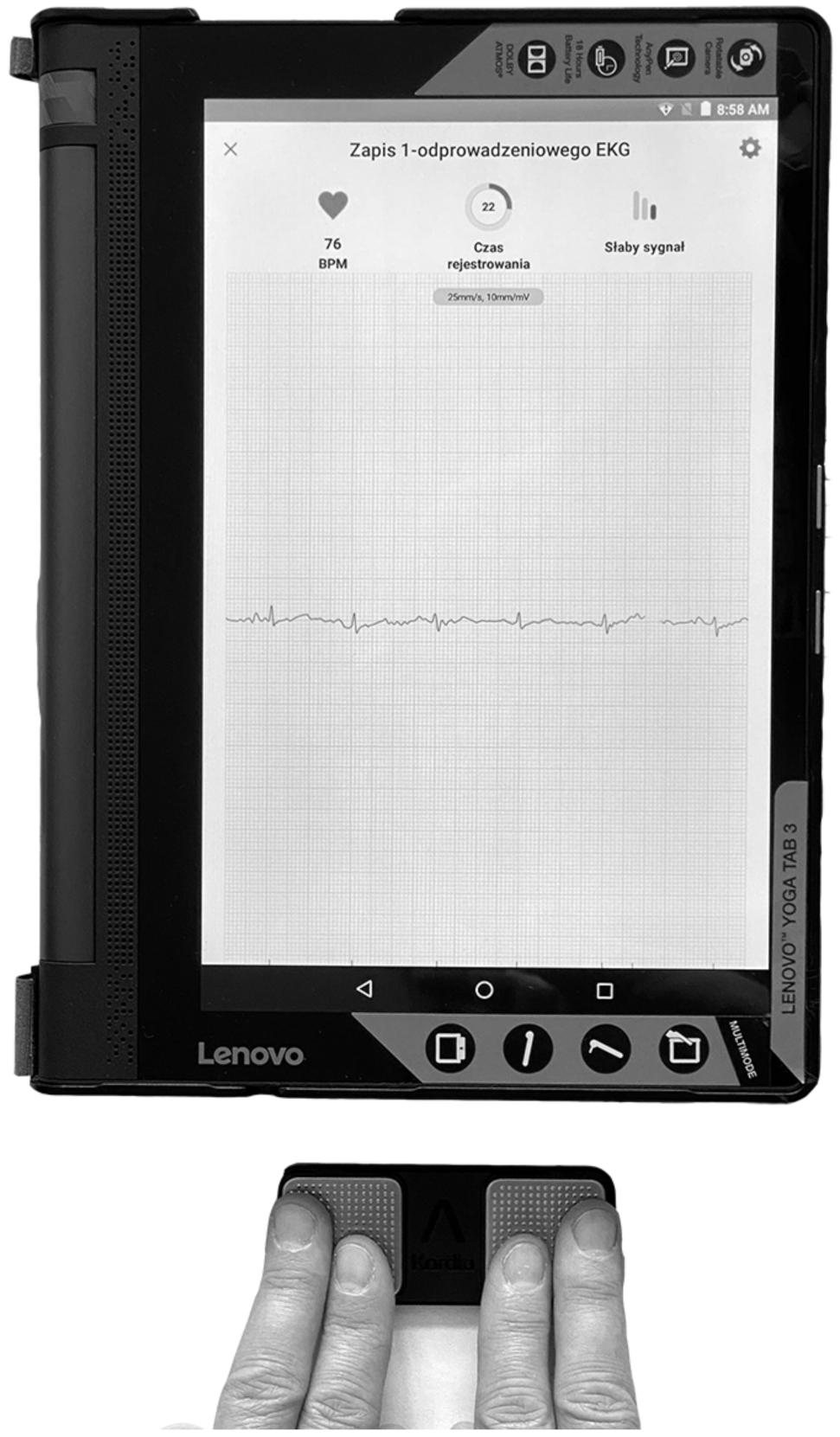
2.3. KM ECG Monitoring
2.4. ECG Adjudication Analysis
2.5. Twenty-Four-Hour Holter ECG
2.6. Statistical Analysis
3. Results
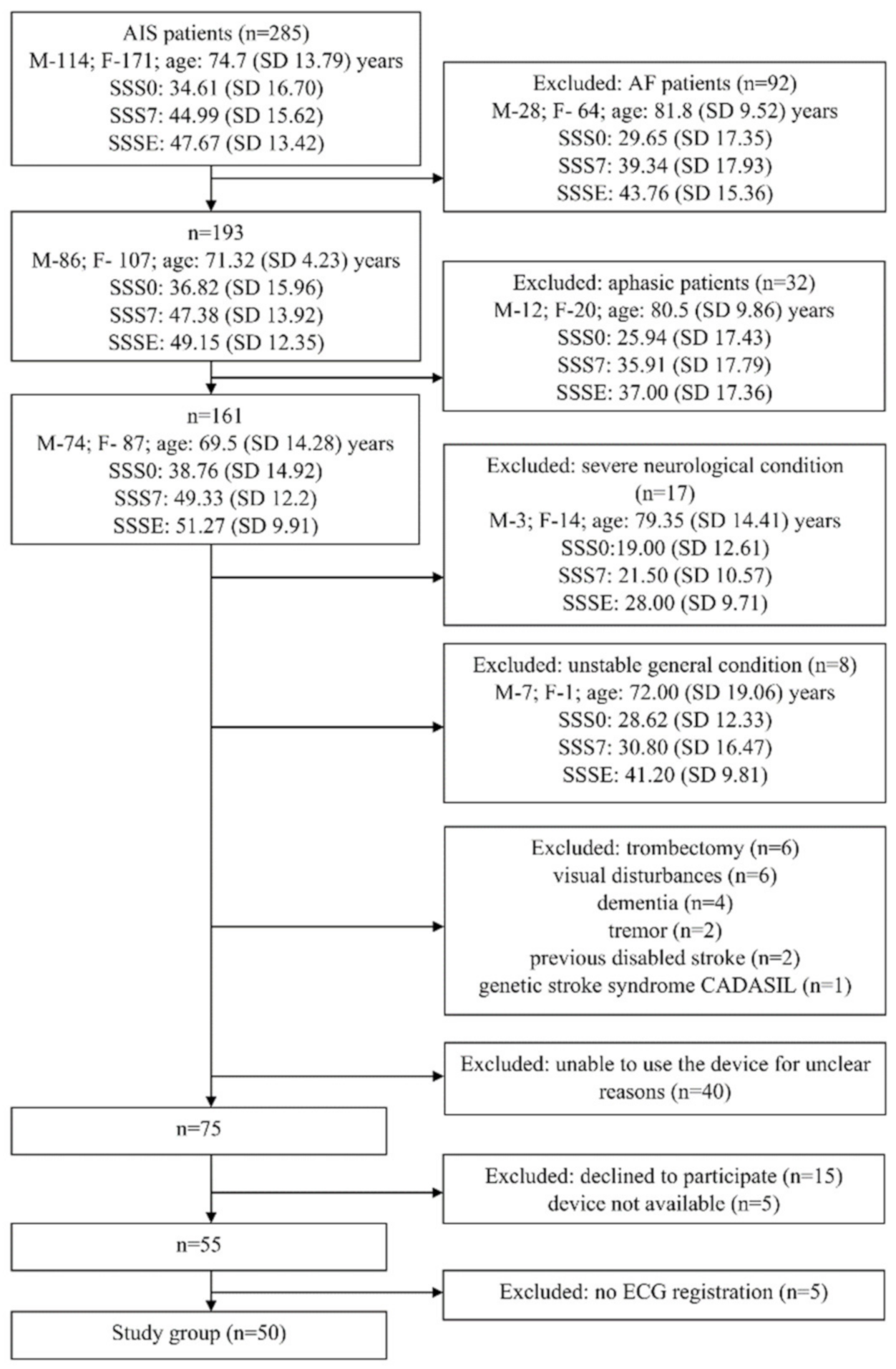
3.1. Participants
3.2. Feasibility
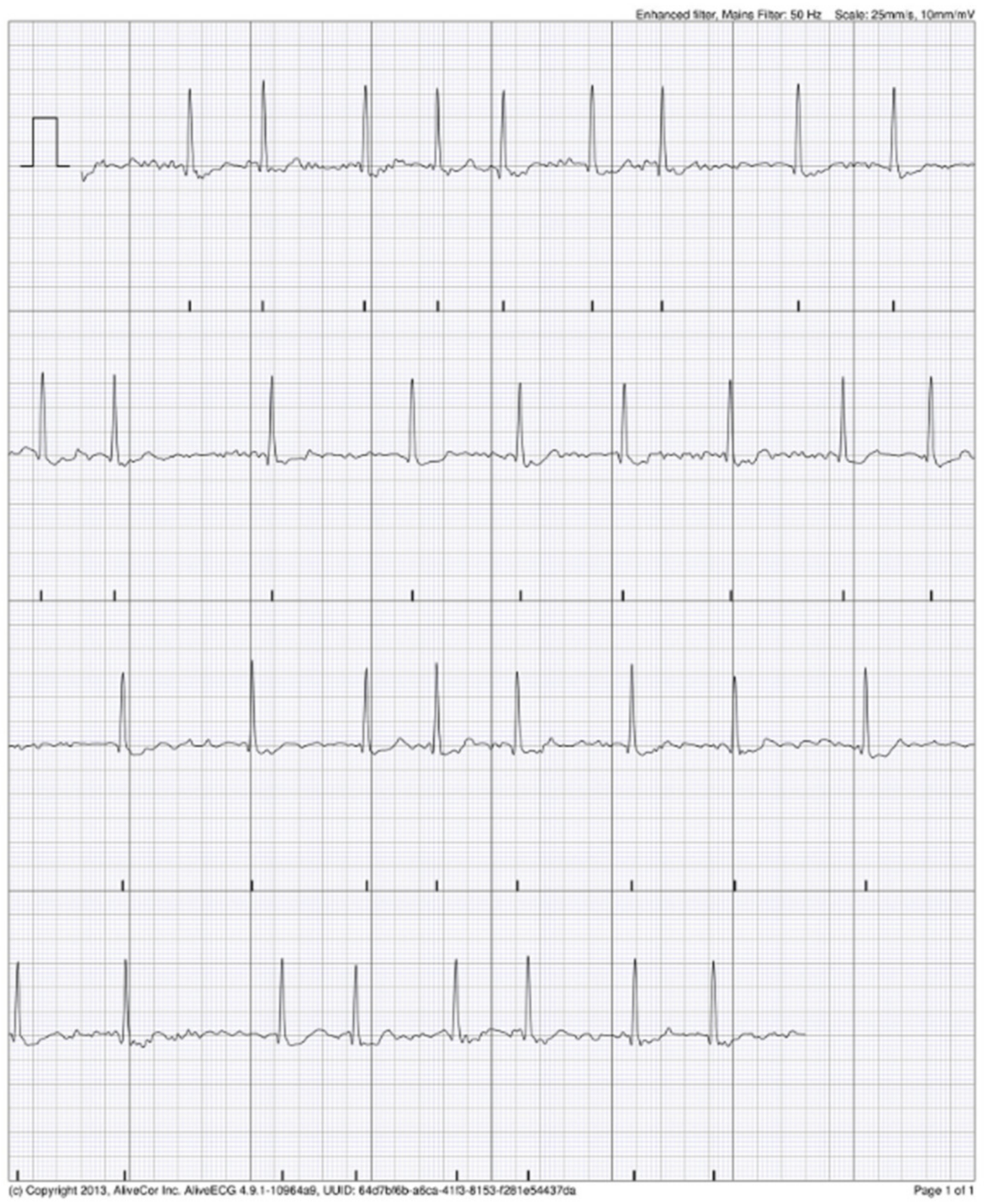
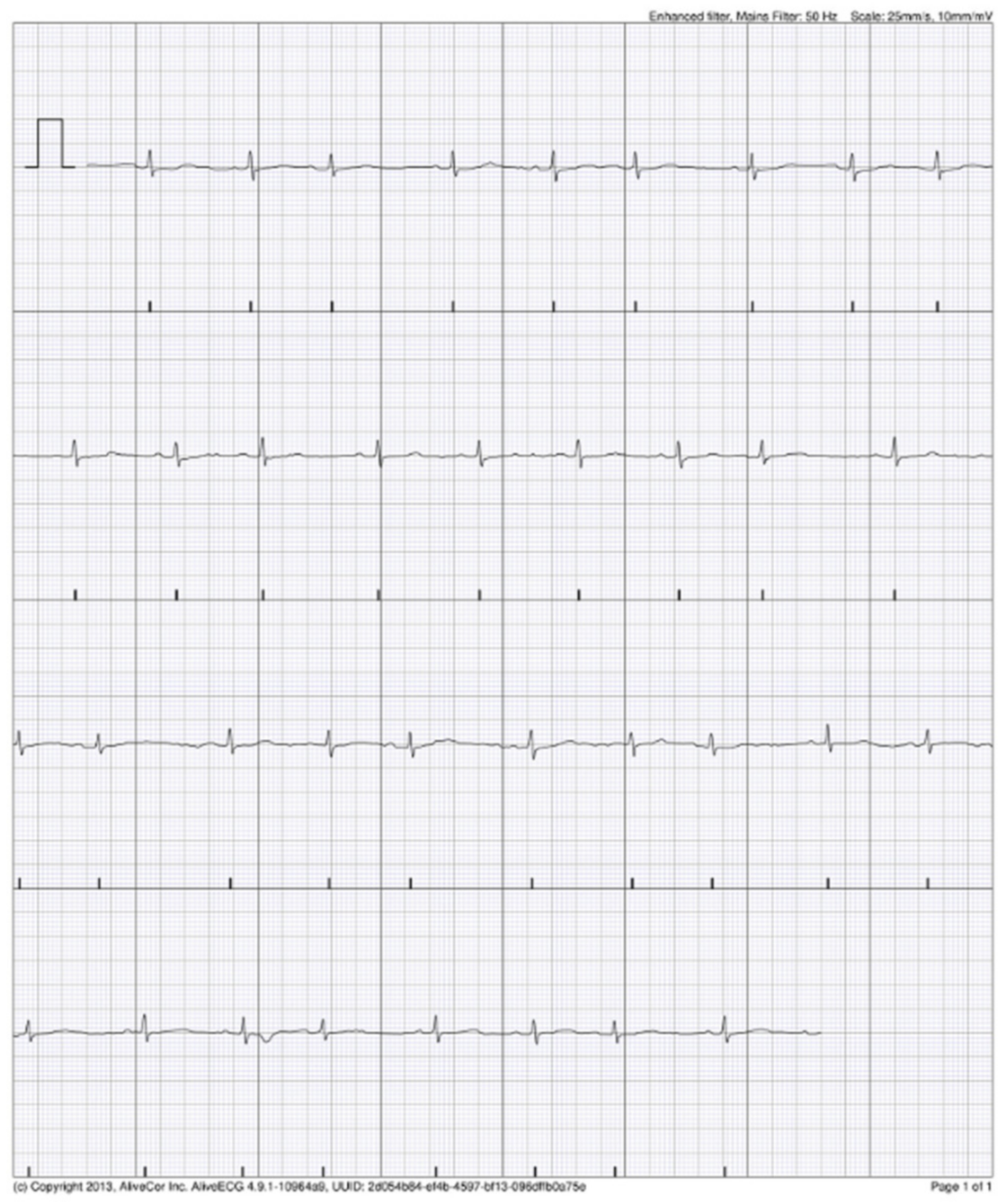
3.3. The KM ECG Monitoring
3.4. KM Automated Algorithm Versus Cardiologist Adjudication
3.5. Twenty-Four-Hour Holter ECG
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yaghi, S.; Bernstein, R.A.; Passman, R.; Okin, P.M.; Furie, K.L. Cryptogenic Stroke. Circ. Res. 2017, 120, 527–540. [Google Scholar] [CrossRef] [PubMed]
- Nah, H.-W.; Lee, J.-W.; Chung, C.-H.; Choo, S.-J.; Kwon, S.U.; Kim, J.S.; Warach, S.; Kang, D.-W. New brain infarcts on magnetic resonance imaging after coronary artery bypass graft surgery: Lesion patterns, mechanism, and predictors. Ann. Neurol. 2014, 76, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Dalen, J.E.; Alpert, J.S. Silent Atrial Fibrillation and Cryptogenic Strokes. Am. J. Med. 2017, 130, 264–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart disease and stroke statistics—2019 update: A report from the American heart association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef] [PubMed]
- Timmermans, C.; Lévy, S.; Ayers, G.M.; Jung, W.; Jordaens, L.; Rosenqvist, M.; Thibault, B.; Camm, J.; Rodriguez, L.-M.; Wellens, H.J. Spontaneous episodes of atrial fibrillation after implantation of the Metrix Atrioverter: Observations on treated and nontreated episodes. J. Am. Coll. Cardiol. 2000, 35, 1428–1433. [Google Scholar] [CrossRef]
- Steinberg, J.S.; O’Connell, H.; Li, S.; Ziegler, P.D. Thirty-Second Gold Standard Definition of Atrial Fibrillation and Its Relationship with Subsequent Arrhythmia Patterns. Circ. Arrhythmia Electrophysiol. 2018, 11, e006274. [Google Scholar] [CrossRef] [PubMed]
- Sgreccia, D.; Manicardi, M.; Malavasi, V.L.; Vitolo, M.; Valenti, A.C.; Proietti, M.; Lip, G.Y.H.; Boriani, G. Comparing Outcomes in Asymptomatic and Symptomatic Atrial Fibrillation: A Systematic Review and Meta-Analysis of 81,462 Patients. J. Clin. Med. 2021, 10, 3979. [Google Scholar] [CrossRef]
- Sposato, L.A.; Cipriano, L.E.; Saposnik, G.; Vargas, E.R.; Riccio, P.M.; Hachinski, V. Diagnosis of atrial fibrillation after stroke and transient ischaemic attack: A systematic review and meta-analysis. Lancet Neurol. 2015, 14, 377–387. [Google Scholar] [CrossRef]
- Sanna, T.; Diener, H.-C.; Passman, R.S.; Di Lazzaro, V.; Bernstein, R.A.; Morillo, C.; Rymer, M.M.; Thijs, V.; Rogers, T.; Beckers, F.; et al. Cryptogenic Stroke and Underlying Atrial Fibrillation. N. Engl. J. Med. 2014, 370, 2478–2486. [Google Scholar] [CrossRef] [Green Version]
- Cerasuolo, J.O.; Cipriano, L.E.; Sposato, L.A. The complexity of atrial fibrillation newly diagnosed after ischemic stroke and transient ischemic attack: Advances and uncertainties. Curr. Opin. Neurol. 2017, 30, 28–37. [Google Scholar] [CrossRef] [Green Version]
- Sposato, L.A.; Klein, F.R.; Jáuregui, A.; Ferrúa, M.; Klin, P.; Zamora, R.; Riccio, P.M.; Rabinstein, A. Newly Diagnosed Atrial Fibrillation after Acute Ischemic Stroke and Transient Ischemic Attack: Importance of Immediate and Prolonged Continuous Cardiac Monitoring. J. Stroke Cerebrovasc. Dis. 2012, 21, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Li, S.; Zhao, X.; Liu, L.; Jiang, Y.; Li, Z.; Wang, Y.; Wang, Y. Atrial fibrillation is not uncommon among patients with ischemic stroke and transient ischemic stroke in China. BMC Neurol. 2017, 17, 207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Proesmans, T.; Mortelmans, C.; Van Haelst, R.; Verbrugge, F.; Vandervoort, P.; Vaes, B. Mobile Phone–Based Use of the Photoplethysmography Technique to Detect Atrial Fibrillation in Primary Care: Diagnostic Accuracy Study of the FibriCheck App. JMIR mHealth uHealth 2019, 7, e12284. [Google Scholar] [CrossRef] [PubMed]
- Perales, C.R.L.; Van Spall, H.G.C.; Maeda, S.; Jimenez, A.; Laţcu, D.G.; Milman, A.; Kirakoya-Samadoulougou, F.; Mamas, M.A.; Muser, D.; Arroyo, R.C. Mobile health applications for the detection of atrial fibrillation: A systematic review. Europace 2020, 23, 11–28. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; ESC Scientific Document Group; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Asso-ciation for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Al-Alusi, M.A.; Ding, E.; McManus, D.D.; Lubitz, S.A. Wearing Your Heart on Your Sleeve: The Future of Cardiac Rhythm Monitoring. Curr. Cardiol. Rep. 2019, 21, 158. [Google Scholar] [CrossRef]
- Chan, P.; Wong, C.; Poh, Y.C.; Pun, L.; Leung, W.W.; Wong, Y.; Wong, M.M.; Poh, M.; Chu, D.W.; Siu, C. Diagnostic Performance of a Smartphone-Based Photoplethysmographic Application for Atrial Fibrillation Screening in a Primary Care Setting. J. Am. Heart Assoc. 2016, 5, e003428. [Google Scholar] [CrossRef]
- Treskes, R.W.; Gielen, W.; Wermer, M.J.; Grauss, R.W.; Van Alem, A.P.; Dehnavi, R.A.; Kirchhof, C.J.; Van Der Velde, E.T.; Maan, A.C.; Wolterbeek, R.; et al. Mobile phones in cryptogenic strOke patients Bringing sIngle Lead ECGs for Atrial Fibrillation detection (MOBILE-AF): Study protocol for a randomised controlled trial. Trials 2017, 18, 402. [Google Scholar] [CrossRef] [Green Version]
- Ding, E.Y.; Svennberg, E.; Wurster, C.; Duncker, D.; Manninger, M.; Lubitz, S.A.; Dickson, E.; Fitzgibbons, T.P.; Akoum, N.; Al-Khatib, S.M.; et al. Survey of current perspectives on consumer-available digital health devices for detecting atrial fibrillation. Cardiovasc. Digit. Heal. J. 2020, 1, 21–29. [Google Scholar] [CrossRef]
- Schnabel, R.B.; Haeusler, K.G.; Healey, J.S.; Freedman, B.; Boriani, G.; Brachmann, J.; Brandes, A.; Bustamante, A.; Casadei, B.; Crijns, H.J.; et al. Searching for Atrial Fibrillation Poststroke. Circulation 2019, 140, 1834–1850. [Google Scholar] [CrossRef]
- Koh, K.T.; Law, W.C.; Zaw, W.M.; Foo, D.H.P.; Tan, C.T.; Steven, A.; Samuel, D.; Fam, T.L.; Chai, C.H.; Wong, Z.S.; et al. Smartphone electrocardiogram for detecting atrial fibrillation after a cerebral ischaemic event: A multicentre randomized controlled trial. Europace 2021, 23, 1016–1023. [Google Scholar] [CrossRef] [PubMed]
- Tayal, A.H.; Tian, M.; Kelly, K.M.; Jones, S.C.; Wright, D.G.; Singh, D.; Jarouse, J.; Brillman, J.; Murali, S.; Gupta, R. Atrial fibrillation detected by mobile cardiac outpatient telemetry in cryptogenic TIA or stroke. Neurology 2008, 71, 1696–1701. [Google Scholar] [CrossRef] [PubMed]
- Gladstone, D.; Spring, M.; Dorian, P.; Panzov, V.; Thorpe, K.; Hall, J.; Vaid, H.; O’Donnell, M.; Laupacis, A.; Côté, R.; et al. Atrial Fibrillation in Patients with Cryptogenic Stroke. N. Engl. J. Med. 2014, 370, 2467–2477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, D.J.; Khan, M.A.; Schultz, L.R.; Simpson, J.R.; Katramados, A.M.; Russman, A.N.; Mitsias, P.D. Outpatient cardiac telemetry detects a high rate of atrial fibrillation in cryptogenic stroke. J. Neurol. Sci. 2013, 324, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Qian, Y.; Smerin, D.; Zhang, S.; Zhao, Q.; Xiong, X. Newly Detected Atrial Fibrillation after Acute Stroke: A Narrative Review of Causes and Implications. Cardiology 2019, 144, 112–121. [Google Scholar] [CrossRef]
- Scandinavian Stroke Study Group. Multicenter trial of hemodilution in ischemic stroke—Background and study protocol. Stroke 1985, 16, 885–890. [Google Scholar] [CrossRef] [Green Version]
- Persson, C.U.; Holmegaard, L.; Redfors, P.; Jern, C.; Blomstrand, C.; Jood, K. Increased muscle tone and contracture late after ischemic stroke. Brain Behav. 2020, 10, e01509. [Google Scholar] [CrossRef] [Green Version]
- Vanbosse, H.; Fafara, A.; Gagnon, M.; Collins, J.; Elfassy, C.; Merlo, G.M.; Marsh, J.; Sawatzky, B.; Yap, R.; Hamdy, R.; et al. A Telerehabilitation Intervention for Youths with Arthrogryposis Multiplex Congenita: Protocol for a Pilot Study. JMIR Res. Protoc. 2020, 9, e18688. [Google Scholar] [CrossRef]
- Gagnon, M.; Merlo, G.M.; Yap, R.; Collins, J.; Elfassy, C.; Sawatzky, B.; Marsh, J.; Hamdy, R.; Veilleux, L.-N.; Dahan-Oliel, N. Using Telerehabilitation to Deliver a Home Exercise Program to Youth with Arthrogryposis: Single Cohort Pilot Study. J. Med. Internet Res. 2021, 23, e27064. [Google Scholar] [CrossRef]
- Garabelli, P.; Stavrakis, S.; Po, S. Smartphone-based arrhythmia monitoring. Curr. Opin. Cardiol. 2017, 32, 53–57. [Google Scholar] [CrossRef]
- Goldenthal, I.L.; Sciacca, R.R.; Riga, T.; Bakken, S.; Baumeister, M.; Biviano, A.B.; Dizon, J.M.; Wang, D.; Wang, K.C.; Whang, W.; et al. Recurrent atrial fibrillation/flutter detection after ablation or cardioversion using the AliveCor KardiaMobile device: iHEART results. J. Cardiovasc. Electrophysiol. 2019, 30, 2220–2228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lowres, N.; Neubeck, L.; Salkeld, G.; Krass, I.; McLachlan, A.J.; Redfern, J.; Bennett, A.A.; Briffa, T.; Bauman, A.; Martinez, C.; et al. Feasibility and cost-effectiveness of stroke prevention through community screening for atrial fibrillation using iPhone ECG in pharmacies. Thromb. Haemost. 2014, 111, 1167–1176. [Google Scholar] [CrossRef] [PubMed]
- Halcox, J.P.; Wareham, K.; Cardew, A.; Gilmore, M.; Barry, J.P.; Phillips, C.; Gravenor, M.B. Assessment of Remote Heart Rhythm Sampling Using the AliveCor Heart Monitor to Screen for Atrial Fibrillation. Circulation 2017, 136, 1784–1794. [Google Scholar] [CrossRef] [PubMed]
- Benezet-Mazuecos, J.; García-Talavera, C.S.; Rubio, J.M. Smart devices for a smart detection of atrial fibrillation. J. Thorac. Dis. 2018, 10, S3824–S3827. [Google Scholar] [CrossRef]
- Atrial Fibrillation in the Old/Very Old: Prevalence and Burden, Predisposing Factors and Complications. Available online: https://www.escardio.org/Journals/E-Journal-of-Cardiology-Practice/Volume-17/Atrial-fibrillation-in-the-old-very-old-prevalence-and-burden-predisposing-factors-and-complications (accessed on 19 November 2021).
- NICE Guidance. KardiaMobile for the Ambulatory Detection of Atrial Fibrillation. Medtech Innovation Briefing [MIB232]. Available online: https://www.nice.org.uk/advice/mib232 (accessed on 29 October 2020).
- Lip, G.Y.; Nieuwlaat, R.; Pisters, R.; Lane, D.A.; Crijns, H.J. Refining Clinical Risk Stratification for Predicting Stroke and Thromboembolism in Atrial Fibrillation Using a Novel Risk Factor-Based Approach. Chest 2010, 137, 263–272. [Google Scholar] [CrossRef]
- Thijs, V. Atrial Fibrillation Detection. Stroke 2017, 48, 2671–2677. [Google Scholar] [CrossRef]
- Ghazal, F.; Theobald, H.; Rosenqvist, M.; Al-Khalili, F. Feasibility and outcomes of atrial fibrillation screening using intermittent electrocardiography in a primary healthcare setting: A cross-sectional study. PLoS ONE 2018, 13, e0198069. [Google Scholar] [CrossRef] [Green Version]
- Rosenfeld, L.E.; Amin, A.N.; Hsu, J.; Oxner, A.; Hills, M.T.; Frankel, D.S. The Heart Rhythm Society/American College of Physicians Atrial Fibrillation Screening and Education Initiative. Heart Rhythm. 2019, 16, e59–e65. [Google Scholar] [CrossRef] [Green Version]
- Lumikari, T.J.; Pirinen, J.; Putaala, J.; Sibolt, G.; Kerola, A.; Pakarinen, S.; Lehto, M.; Nieminen, T. Prolonged ECG with a novel recorder utilizing electrode belt and mobile device in patients with recent embolic stroke of undetermined source: A pilot study. Ann. Noninvasive Electrocardiol. 2020, 25, e12802. [Google Scholar] [CrossRef]
- Jones, N.R.; Taylor, C.J.; Hobbs, F.D.R.; Bowman, L.; Casadei, B. Screening for atrial fibrillation: A call for evidence. Eur. Heart J. 2019, 41, 1075–1085. [Google Scholar] [CrossRef]
- Reed, M.J.; Grubb, N.R.; Lang, C.C.; O’Brien, R.; Simpson, K.; Padarenga, M.; Grant, A.; Tuck, S.; Keating, L.; Coffey, F.; et al. Multi-centre Randomised Controlled Trial of a Smartphone-based Event Recorder Alongside Standard Care Versus Standard Care for Patients Presenting to the Emergency Department with Palpitations and Pre-syncope: The IPED (Investigation of Palpitations in the ED) study. EClinicalMedicine 2019, 8, 37–46. [Google Scholar] [CrossRef] [Green Version]
- Pitman, B.M.; Chew, S.-H.; Wong, C.X.; Jaghoori, A.; Iwai, S.; Thomas, G.; Chew, A.; Sanders, P.; Lau, D.H. Performance of a Mobile Single-Lead Electrocardiogram Technology for Atrial Fibrillation Screening in a Semirural African Population: Insights From “The Heart of Ethiopia: Focus on Atrial Fibrillation” (TEFF-AF) Study. JMIR mHealth uHealth 2021, 9, e24470. [Google Scholar] [CrossRef] [PubMed]
- Chan, P.-H.; Wong, C.-K.; Pun, L.; Wong, Y.-F.; Wong, M.M.-Y.; Chu, D.W.-S.; Siu, C.-W. Head-to-Head Comparison of the AliveCor Heart Monitor and Microlife WatchBP Office AFIB for Atrial Fibrillation Screening in a Primary Care Setting. Circulation 2017, 135, 110–112. [Google Scholar] [CrossRef] [PubMed]
- Brasier, N.; Raichle, C.J.; Dörr, M.; Becke, A.; Nohturfft, V.; Weber, S.; Bulacher, F.; Salomon, L.; Noah, T.; Birkemeyer, R.; et al. Detection of atrial fibrillation with a smartphone camera: First prospective, international, two-centre, clinical validation study (DETECT AF PRO). Europace 2018, 21, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Koltowski, L.; Balsam, P.; Glłowczynska, R.; Rokicki, J.K.; Peller, M.; Maksym, J.; Blicharz, L.; Maciejewski, K.; Niedziela, M.; Opolski, G.; et al. Kardia Mobile applicability in clinical practice: A comparison of Kardia Mobile and standard 12-lead electrocardiogram records in 100 consecutive patients of a tertiary cardiovascular care center. Cardiol. J. 2021, 28, 543–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, K.C.; Klimis, H.; Lowres, N.; Von Huben, A.; Marschner, S.; Chow, C.K. Diagnostic accuracy of handheld electrocardiogram devices in detecting atrial fibrillation in adults in community versus hospital settings: A systematic review and meta-analysis. Heart 2020, 106, 1211–1217. [Google Scholar] [CrossRef] [PubMed]
- Duarte, R.; Stainthorpe, A.; Greenhalgh, J.; Richardson, M.; Nevitt, S.; Mahon, J.; Kotas, E.; Boland, A.; Thom, H.; Marshall, T.; et al. Lead-I ECG for detecting atrial fibrillation in patients with an irregular pulse using single time point testing: A systematic review and economic evaluation. Health Technol. Assess. 2020, 24, 1–164. [Google Scholar] [CrossRef]
- Eun, M.-Y.; Jung, J.-M.; Choi, K.-H.; Seo, W.-K. Statin Effects in Atrial Fibrillation-Related Stroke: A Systematic Review and Meta-Analysis. Front. Neurol. 2020, 11, 589684. [Google Scholar] [CrossRef]
- Wańkowicz, P.; Staszewski, J.; Dębiec, A.; Nowakowska-Kotas, M.; Szylińska, A.; Turoń-Skrzypińska, A.; Rotter, I. Pre-Stroke Statin Therapy Improves In-Hospital Prognosis Following Acute Ischemic Stroke Associated with Well-Controlled Nonvalvular Atrial Fibrillation. J. Clin. Med. 2021, 10, 3036. [Google Scholar] [CrossRef]
- Tu, H.T.; Chen, Z.; Swift, C.; Churilov, L.; Guo, R.; Liu, X.; Jannes, J.; Mok, V.; Freedman, B.; Davis, S.M.; et al. Smartphone electrographic monitoring for atrial fibrillation in acute ischemic stroke and transient ischemic attack. Int. J. Stroke 2017, 12, 786–789. [Google Scholar] [CrossRef]
- Global Health Estimates 2020: Disease Burden by Cause, Age, Sex, by Country and by Region, 2000–2019; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/global-health-estimates-leading-causes-of-dalys (accessed on 18 May 2021).
- Panahi, Y.; Sahebkar, A.; Naderi, Y.; Barreto, G.E. Neuroprotective effects of minocycline on focal cerebral ischemia injury: A systematic review. Neural Regen. Res. 2020, 15, 773–782. [Google Scholar] [CrossRef] [PubMed]
- Mahon, S.; Parmar, P.; Barker-Collo, S.; Krishnamurthi, R.; Jones, K.; Theadom, A.; Feigin, V. Determinants, Prevalence, and Trajectory of Long-Term Post-Stroke Cognitive Impairment: Results from a 4-Year Follow-Up of the Auckland Stroke Regional Outcomes Study-IV Study. Neuroepidemiology 2017, 49, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, A.; Lanctôt, K.L.; Bayley, M.; Kiss, A.; Herrmann, N.; Murray, B.J.; Swartz, R.H. “Good Outcome” Isn’t Good Enough. Stroke 2017, 48, 1688–1690. [Google Scholar] [CrossRef] [PubMed]
- Halevi, D.R.; Bursaw, A.W.; Karamchandani, R.R.; Alderman, S.; Breier, J.I.; Vahidy, F.; Aden, J.K.; Cai, C.; Zhang, X.; Savitz, S.I. Cognitive deficits in acute mild ischemic stroke and TIA and effects of rt-PA. Ann. Clin. Transl. Neurol. 2019, 6, 466–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, J.-H.; Tan, L.; Yu, J.-T. Post-stroke cognitive impairment: Epidemiology, mechanisms and management. Ann. Transl. Med. 2014, 2. [Google Scholar] [CrossRef]
- Chen, L.Y.; Agarwal, S.K.; Norby, F.; Gottesman, R.F.; Loehr, L.; Soliman, E.Z.; Mosley, T.H.; Folsom, A.R.; Coresh, J.; Alonso, A. Persistent but not Paroxysmal Atrial Fibrillation Is Independently Associated with Lower Cognitive Function. J. Am. Coll. Cardiol. 2016, 67, 1379–1380. [Google Scholar] [CrossRef]
- Singh, N.; Chun, S.; Hadley, D.; Froelicher, V. Clinical Implications of Technological Advances in Screening for Atrial Fibrillation. Prog. Cardiovasc. Dis. 2018, 60, 550–559. [Google Scholar] [CrossRef]
- Baturova, M.A.; Lindgren, A.; Carlson, J.; Shubik, Y.V.; Olsson, S.B.; Platonov, P.G. Predictors of new onset atrial fibrillation during 10-year follow-up after first-ever ischemic stroke. Int. J. Cardiol. 2015, 199, 248–252. [Google Scholar] [CrossRef]
- Wańkowicz, P.; Nowacki, P.; Gołąb-Janowska, M. Atrial fibrillation risk factors in patients with ischemic stroke. Arch. Med. Sci. 2021, 17, 19–24. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Group (n = 50) | Patients Not Able to Use Device for Unclear Reason (n = 40) | p Value | |
|---|---|---|---|
| Age, mean (year) | 64.44 (SD 10.52) | 75.15 (SD 11.38) | <0.001 |
| Gender, female (%) | 24/50 (48%) | 26/40 (65%) | 0.11 1 |
| SSS0, mean 2 | 47.10 (SD 11.6) | 36.33 (SD 11.88) | <0.001 |
| SSS7, mean 3 | 55.76 (SD 3.74) | 45.11 (SD 11.97) | <0.001 |
| SSSE, mean 4 | 55.98 (SD 3.39) | 46.83 (SD 11.65) | <0.001 |
| Duration of hospitalization, mean (days) | 9.0 (SD 1.23) | 11.28 (SD 8.94) | 0.22 |
| Results of the Cardiologist Inspection of the KM ECG Records | ||
|---|---|---|
| Number of Patients (n = 50) | Number of KM ECG Records (n = 895) | |
| Extrasystoles | 4/50 (8%) | 13/895 (1.4%) |
| Bigeminy | 1/50 (2%) | 3/895 (0.3%) |
| Bundle branch block | 5/50 (10%) | |
| Data of the standard 24 h Holter ECG | ||
| Number of patients (n = 50) | Number of detected arrhythmias, mean | |
| SVEB 1 | 28/50 (56%) | 564 (SD 1573.13) |
| VEB 2 | 22/50 (44%) | 124.08 (SD 341.04) |
| SVT 3 | 19/50 (38%) | 3.02 (SD 13.84) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leńska-Mieciek, M.; Kuls-Oszmaniec, A.; Dociak, N.; Kowalewski, M.; Sarwiński, K.; Osiecki, A.; Fiszer, U. Mobile Single-Lead Electrocardiogram Technology for Atrial Fibrillation Detection in Acute Ischemic Stroke Patients. J. Clin. Med. 2022, 11, 665. https://doi.org/10.3390/jcm11030665
Leńska-Mieciek M, Kuls-Oszmaniec A, Dociak N, Kowalewski M, Sarwiński K, Osiecki A, Fiszer U. Mobile Single-Lead Electrocardiogram Technology for Atrial Fibrillation Detection in Acute Ischemic Stroke Patients. Journal of Clinical Medicine. 2022; 11(3):665. https://doi.org/10.3390/jcm11030665
Chicago/Turabian StyleLeńska-Mieciek, Marta, Aleksandra Kuls-Oszmaniec, Natalia Dociak, Marcin Kowalewski, Krzysztof Sarwiński, Andrzej Osiecki, and Urszula Fiszer. 2022. "Mobile Single-Lead Electrocardiogram Technology for Atrial Fibrillation Detection in Acute Ischemic Stroke Patients" Journal of Clinical Medicine 11, no. 3: 665. https://doi.org/10.3390/jcm11030665