
Iron Deficiency and Reduced Muscle Strength in Patients with Acute and Chronic Ischemic Stroke

 , ,
, , 
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Population
2.2. Assessment of Functional Status
2.3. Body Composition and Nutritional Status
2.4. Blood Sampling and Iron Deficiency
2.5. Statistical Analysis
3. Results
3.1. Baseline
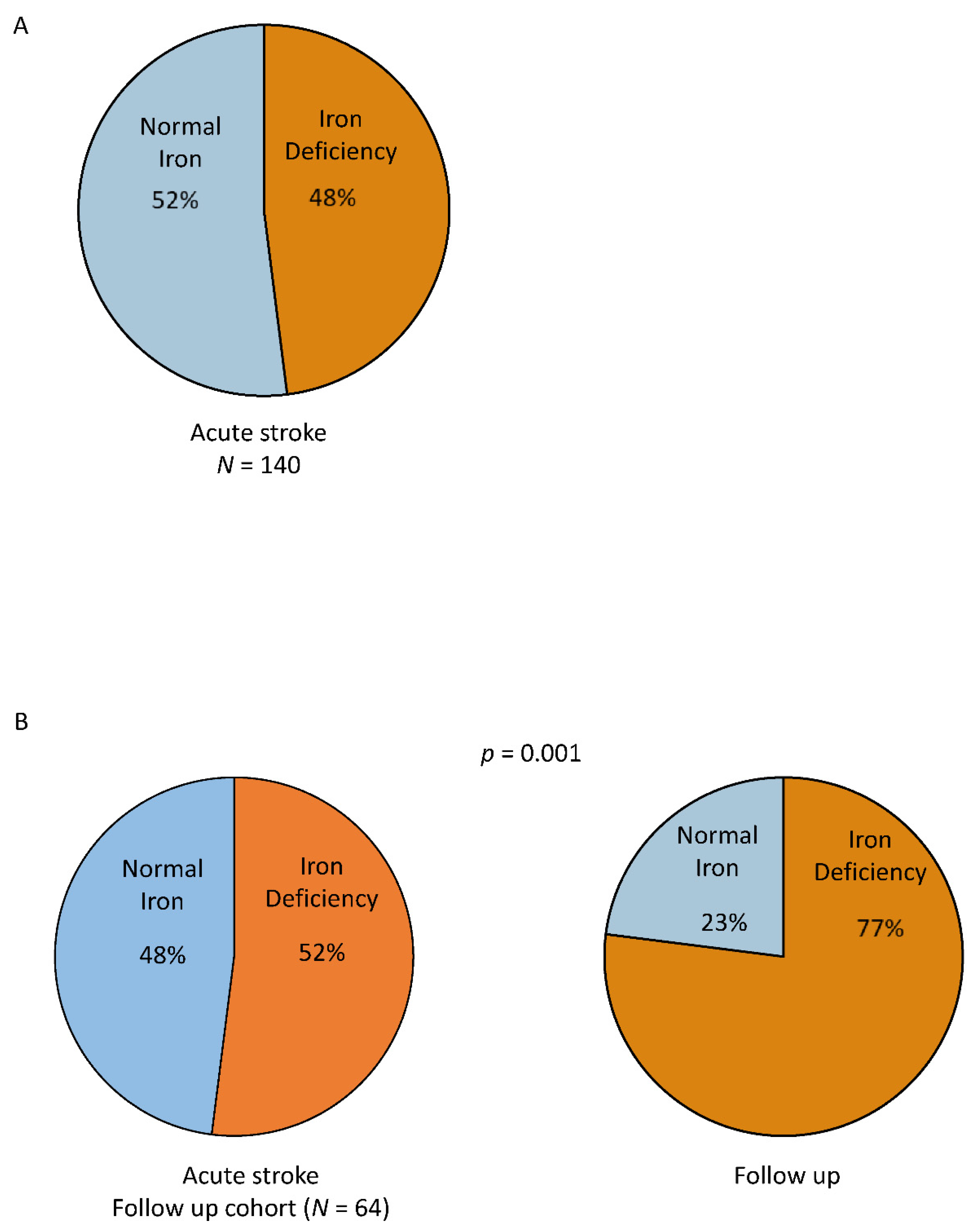
3.1.1. Iron Status at Baseline
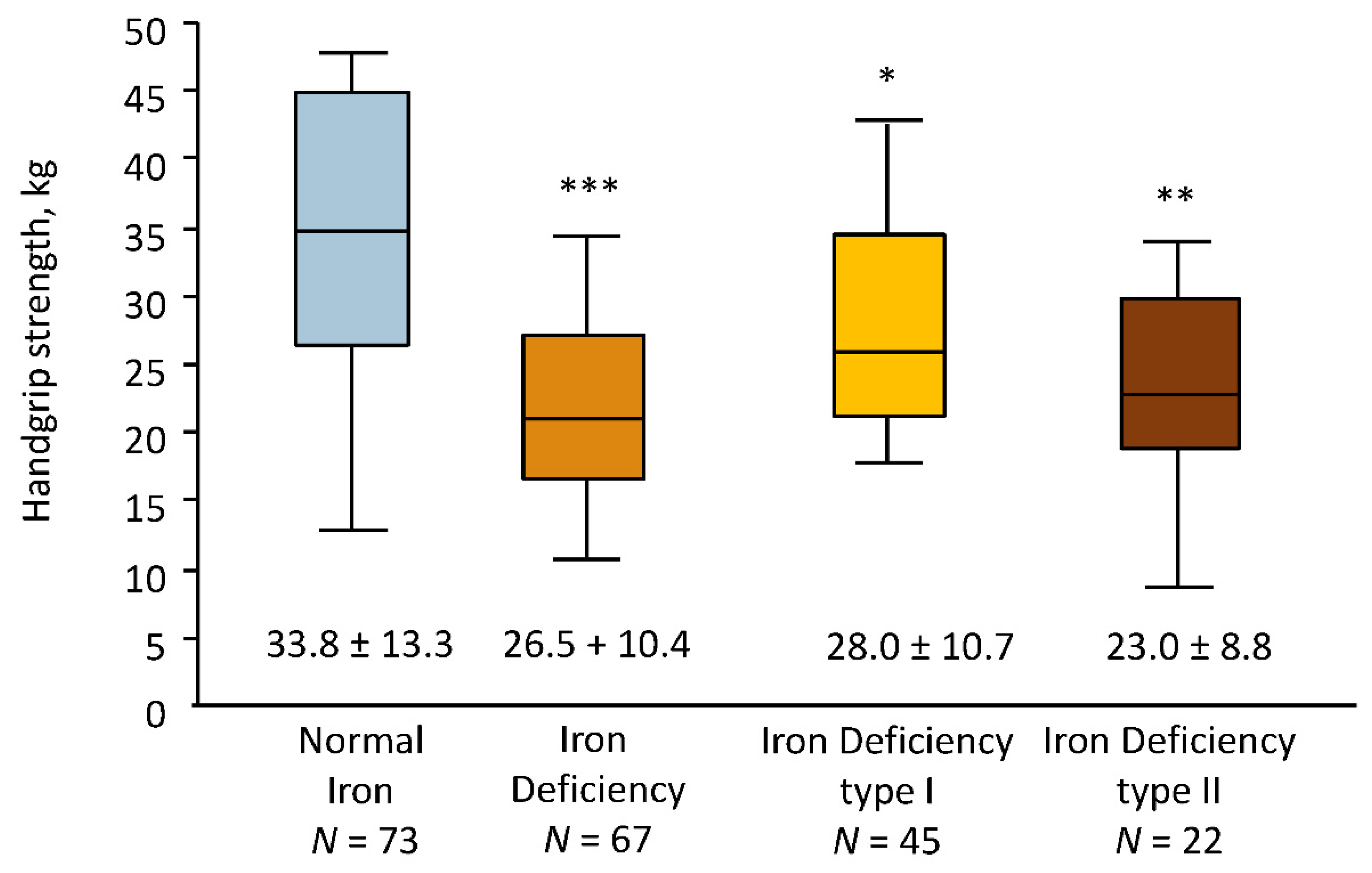
3.1.2. Physical Status at Baseline
3.1.3. Nutritional Status at Baseline
3.1.4. Regression Analyses of Handgrip Strength at Baseline
3.2. Follow Up
3.2.1. Iron Status
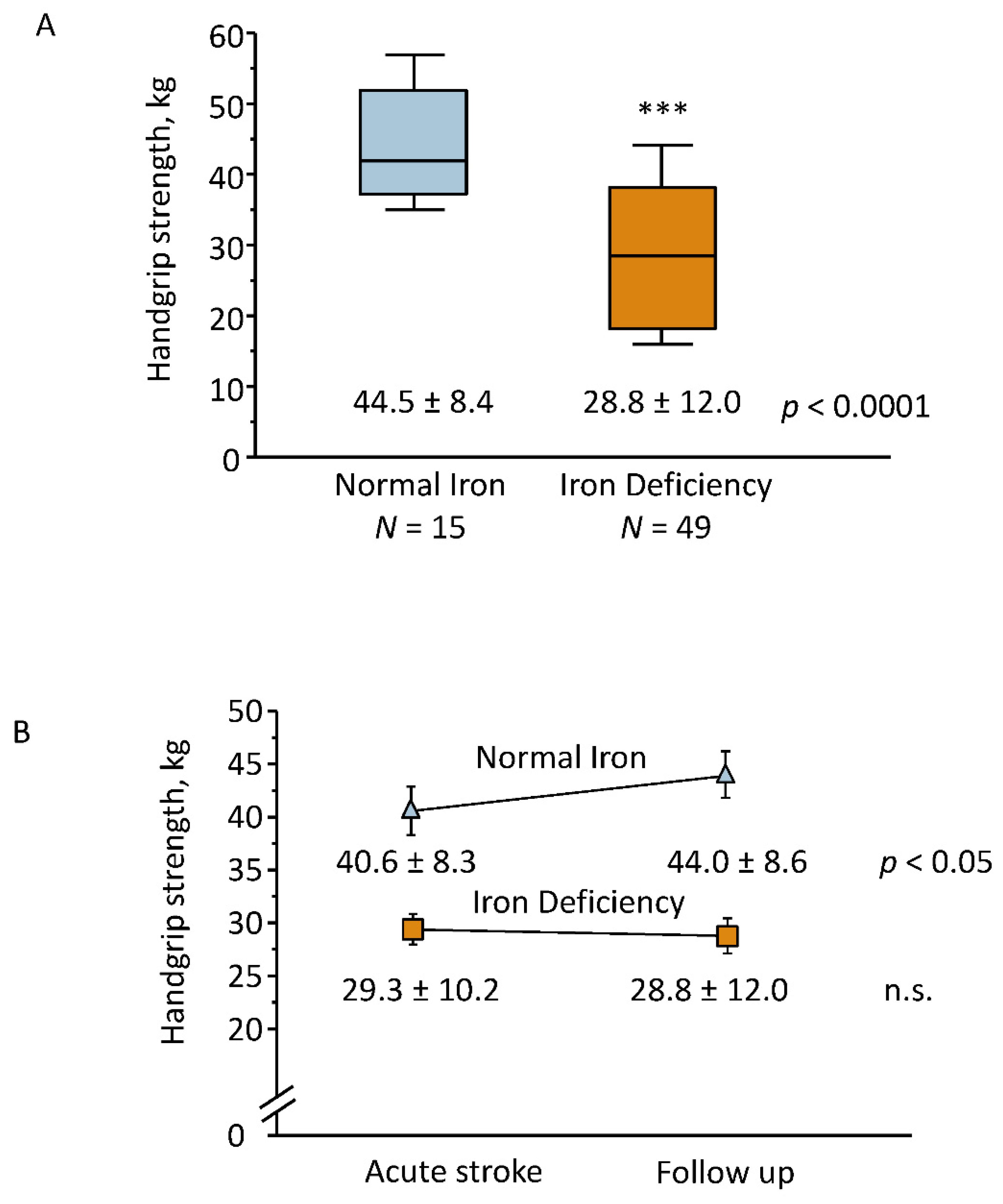
3.2.2. Muscle Strength
3.2.3. Nutritional Status
3.2.4. Logistic Regression Analyses of Handgrip Strength at Follow Up
4. Discussion
4.1. ID Categories in Stroke
4.2. Physical Performance and Muscle Strength
4.3. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Krishnamurthi, R.V.; Ikeda, T.; Feigin, V.L. Global, Regional and Country-Specific Burden of Ischaemic Stroke, Intracerebral Haemorrhage and Subarachnoid Haemorrhage: A Systematic Analysis of the Global Burden of Disease Study. Neuroepidemiology 2020, 54, 171–179. [Google Scholar] [CrossRef]
- Burkot, J.; Kopeć, G.; Pera, J.; Slowik, A.; Dziedzic, T. Decompensated Heart Failure Is a Strong Independent Predictor of Functional Outcome After Ischemic Stroke. J. Card. Fail. 2015, 21, 642–646. [Google Scholar] [CrossRef]
- Patlolla, S.H.; Lee, H.-C.; Noseworthy, P.A.; Wysokinski, W.E.; Hodge, D.O.; Greene, E.L.; Gersh, B.J.; Melduni, R.M. Impact of Diabetes Mellitus on Stroke and Survival in Patients with Atrial Fibrillation. Am. J. Cardiol. 2020, 131, 33–39. [Google Scholar] [CrossRef]
- Holmqvist, L.; Boström, K.B.; Kahan, T.; Schiöler, L.; Hasselström, J.; Hjerpe, P.; Wettermark, B.; Manhem, K. Cardiovascular outcome in treatment-resistant hypertension: Results from the Swedish Primary Care Cardiovascular Database (SPCCD). J. Hypertens. 2018, 36, 402–409. [Google Scholar] [CrossRef]
- Barandiarán Aizpurua, A.; Sanders-van Wijk, S.; Brunner-La Rocca, H.P.; Henkens, M.T.H.M.; Weerts, J.; Spanjers, M.H.A.; Knackstedt, C.; van Empel, V.P.M. Iron deficiency impacts prognosis but less exercise capacity in heart failure with preserved ejection fraction. ESC Heart Fail. 2021, 8, 1304–1313. [Google Scholar] [CrossRef]
- Guedes, M.; Muenz, D.; Zee, J.; Lopes, M.B.; Waechter, S.; Stengel, B.; Massy, Z.; Speyer, E.; Ayav, C.; Finkelstein, F.; et al. Serum biomarkers of iron stores are associated with worse physical health-related quality of life in nondialysis-dependent chronic kidney disease patients with or without anemia. Nephrol. Dial. Transplant. 2021, 36, 1694–1703. [Google Scholar] [CrossRef]
- Chopra, V.K.; Anker, S.D. Anaemia, ID and heart failure in 2020: Facts and numbers. ESC Heart Fail. 2020, 7, 2007–2011. [Google Scholar] [CrossRef]
- Neidlein, S.; Wirth, R.; Pourhassan, M. Iron deficiency, fatigue and muscle strength and function in older hospitalized patients. Eur. J. Clin. Nutr. 2021, 75, 456–463. [Google Scholar] [CrossRef]
- Muñoz, I.V.M.; Villar, I.; García-Erce, J.A. An update on iron physiology. World J. Gastroenterol. 2009, 15, 4617–4626. [Google Scholar] [CrossRef]
- Kulkarni, A.; Khade, M.; Arun, S.; Badami, P.; Kumar, G.R.K.; Dattaroy, T.; Soni, B.; Dasgupta, S. An overview on mechanism, cause, prevention and multi-nation policy level interventions of dietary ID. Crit. Rev. Food Sci. Nutr. 2021, 1–15. [Google Scholar] [CrossRef]
- Guida, C.; Altamura, S.; Klein, F.A.; Galy, B.; Boutros, M.; Ulmer, A.J.; Hentze, M.W.; Muckenthaler, M.U. A novel inflammatory pathway mediating rapid hepcidin-independent hypoferremia. Blood 2015, 125, 2265–2275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasricha, S.R.; Tye-Din, J.; Muckenthaler, M.U.; Swinkels, D.W. Iron deficiency. Lancet 2021, 397, 233–248. [Google Scholar] [CrossRef]
- Von Haehling, S.; Ebner, N.; Evertz, R.; Ponikowski, P.; Anker, S.D. ID in Heart Failure: An Overview. JACC Heart Fail. 2019, 7, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Knops, M.; Werner, C.G.; Scherbakov, N.; Fiebach, J.; Dreier, J.P.; Meisel, A.; Heuschmann, P.U.; Jungehülsing, G.J.; von Haehling, S.; Dirnagl, U.; et al. Investigation of changes in body composition, metabolic profile and skeletal muscle functional capacity in ischemic stroke patients: The rationale and design of the Body Size in Stroke Study (BoSSS). J. Cachex Sarcopenia Muscle 2013, 4, 199–207. [Google Scholar] [CrossRef]
- Adams, H.P., Jr.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E., 3rd. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Kasner, S. Clinical interpretation and use of stroke scales. Lancet Neurol. 2006, 5, 603–612. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A Short Physical Performance Battery Assessing Lower Extremity Function: Association with Self-Reported Disability and Prediction of Mortality and Nursing Home Admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef]
- Doehner, W.; Turhan, G.; Leyva, F.; Rauchhaus, M.; Sandek, A.; Jankowska, E.; Von Haehling, S.; Anker, S.D. Skeletal muscle weakness is related to insulin resistance in patients with chronic heart failure. ESC Heart Fail. 2015, 2, 85–89. [Google Scholar] [CrossRef]
- Koehler, F.; Doehner, W.; Hoernig, S.; Witt, C.; Anker, S.D.; John, M. Anorexia in chronic obstructive pulmonary disease—Association to cachexia and hormonal derangement. Int. J. Cardiol. 2007, 119, 83–89. [Google Scholar] [CrossRef]
- Vellas, B.; Guigoz, Y.; Garry, P.J.; Nourhashemi, F.; Bennahum, D.; Lauque, S.; Albarede, J.L. The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition 1999, 15, 116–122. [Google Scholar] [CrossRef]
- Moliner, P.; Jankowska, E.; van Veldhuisen, D.J.; Farre, N.; Rozentryt, P.; Enjuanes, C.; Polonski, L.; Meroño, O.; Voors, A.A.; Ponikowski, P.; et al. Clinical correlates and prognostic impact of impaired iron storage versus impaired iron transport in an international cohort of 1821 patients with chronic heart failure. Int. J. Cardiol. 2017, 243, 360–366. [Google Scholar] [CrossRef] [PubMed]
- Loncar, G.; Obradovic, D.; Thiele, H.; von Haehling, S.; Lainscak, M. Iron deficiency in heart failure. ESC Heart Fail. 2021, 2368–2379. [Google Scholar] [CrossRef] [PubMed]
- Schaap, L.A.; Pluijm, S.M.; Deeg, D.J.; Visser, M. Inflammatory Markers and Loss of Muscle Mass (Sarcopenia) and Strength. Am. J. Med. 2006, 119, 526.e9–526.e17. [Google Scholar] [CrossRef] [PubMed]
- Wieczorek, M.; Schwarz, F.; Sadlon, A.; Abderhalden, L.A.; Molino, C.D.G.R.C.; Spahn, D.R.; Schaer, D.J.; Orav, E.J.; Egli, A.; Bischoff-Ferrari, H.A.; et al. Iron deficiency and biomarkers of inflammation: A 3-year prospective analysis of the DO-HEALTH trial. Aging Clin. Exp. Res. 2021, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, D.S.; Mor, R.; Weu, M.T.; Schwartz, D.; Schwartz, I.F.; Chernin, G. Anemia and iron deficiency in COPD patients: Prevalence and the effects of correction of the anemia with erythropoiesis stimulating agents and intra-venous iron. BMC Pulm. Med. 2014, 14, 24. [Google Scholar] [CrossRef] [Green Version]
- Silva, C.; Martins, J.; Campos, I.; Arantes, C.; Braga, C.G.; Salomé, N.; Gaspar, A.; Azevedo, P.; Pereira, M.Á.; Marques, J.; et al. Prognostic impact of iron deficiency in acute coronary syndromes. Rev. Port. Cardiol. 2021, 40, 525–536. [Google Scholar] [CrossRef]
- Jacob, J.; Miró, Ò.; Ferre, C.; Borraz-Ordás, C.; Llopis-García, G.; Comabella, R.; Fernández-Cañadas, J.M.; Mercado, A.; Roset, A.; Richard-Espiga, F.; et al. ID and safety of ferric carboxymaltose in patients with acute heart failure. AHF-ID study. Int. J. Clin. Pract. 2020, 74, e13584. [Google Scholar] [CrossRef] [PubMed]
- Jankowska, E.A.; Rozentryt, P.; Witkowska, A.; Nowak, J.; Hartmann, O.; Ponikowska, B.; Borodulin-Nadzieja, L.; Banasiak, W.; Polonski, L.; Filippatos, G.; et al. Iron deficiency: An ominous sign in patients with systolic chronic heart failure. Eur. Heart J. 2010, 31, 1872–1880. [Google Scholar] [CrossRef]
- Quatredeniers, M.; Mendes-Ferreira, P.; Santos-Ribeiro, D.; Nakhleh, M.K.; Ghigna, M.R.; Cohen-Kaminsky, S.; Perros, F. ID in Pulmonary Arterial Hypertension: A Deep Dive into the Mechanisms. Cells 2021, 10, 477. [Google Scholar] [CrossRef]
- Čiburienė, E.; Čelutkienė, J.; Aidietienė, S.; Ščerbickaitė, G.; Lyon, A.R. The prevalence of ID and anemia and their im-pact on survival in patients at a cardio-oncology clinic. Cardiooncology 2020, 6, 29. [Google Scholar]
- Camaschella, C. ID. Blood 2019, 133, 30–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scherbakov, N.; Dirnagl, U.; Doehner, W. Body weight after stroke: Lessons from the obesity paradox. Stroke 2011, 42, 3646–3650. [Google Scholar] [CrossRef] [Green Version]
- Perry, L. Eating and dietary intake in communication-impaired stroke survivors: A cohort study from acute-stage hospital admission to 6 months post-stroke. Clin. Nutr. 2004, 23, 1333–1343. [Google Scholar] [CrossRef] [PubMed]
- Douwes, R.M.; Gomes-Neto, A.W.; Eisenga, M.F.; Vinke, J.S.J.; De Borst, M.H.; van den Berg, E.; Berger, S.P.; Touw, D.J.; Hak, E.; Blokzijl, H.; et al. Chronic Use of Proton-Pump Inhibitors and Iron Status in Renal Transplant Recipients. J. Clin. Med. 2019, 8, 1382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Veldhuisen, D.J.; Anker, S.D.; Ponikowski, P.; Macdougall, I.C. Anemia and iron deficiency in heart failure: Mechanisms and therapeutic approaches. Nat. Rev. Cardiol. 2011, 8, 485–493. [Google Scholar] [CrossRef]
- Pozzo, J.; Fournier, P.; Delmas, C.; Vervueren, P.-L.; Roncalli, J.; Elbaz, M.; Galinier, M.; Lairez, O. Absolute iron deficiency without anaemia in patients with chronic systolic heart failure is associated with poorer functional capacity. Arch. Cardiovasc. Dis. 2017, 110, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Van Dalen, D.H.; Kragten, J.A.; Emans, M.E.; van Ofwegen-Hanekamp, C.E.E.; Klaarwater, C.C.R.; Spanjers, M.H.A.; Hendrick, R.; van Deursen, C.T.B.M.; Rocca, H.B. Acute heart failure and iron deficiency: A prospective, multicentre, observational study. ESC Hear. Fail. 2021. [Google Scholar] [CrossRef]
- Grote Beverborg, N.; Klip, I.T.; Meijers, W.C.; Voors, A.A.; Vegter, E.L.; van der Wal, H.H.; Swinkels, D.W.; van Pelt, J.; Mulder, A.B.; Bulstra, S.K.; et al. Definition of Iron Defi-ciency Based on the Gold Standard of Bone Marrow Iron Staining in Heart Failure Patients. Circ. Heart Fail. 2018, 11, e004519. [Google Scholar] [CrossRef]
- Wish, J.B. Assessing Iron Status: Beyond Serum Ferritin and Transferrin Saturation. Clin. J. Am. Soc. Nephrol. 2006, 1, S4–S8. [Google Scholar] [CrossRef]
- Doehner, W.; Scherbakov, N.; Schellenberg, T.; Jankowska, E.A.; Scheitz, J.F.; von Haehling, S.; Joebges, M. Iron deficiency is related to low functional outcome in patients at early rehabilitation after acute stroke. 2021; in press. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Clinical Parameters | All Patients N = 140 | Normal Iron N = 73 | ID N = 67 | ID Type I N = 45 | ID Type II N = 22 | p Value ID vs. Normal Iron | p Value ID I vs. ID II vs. Normal Iron |
|---|---|---|---|---|---|---|---|
| Age, y, mean ± SD | 69 ± 13 | 67 ± 12 | 70 ± 14 | 66 ± 14 | 77 ± 12 * | n.s. | <0.01 |
| Body mass index, kg/m², mean ± SD | 27.7 ± 4.6 | 28.3 ± 4.8 | 27.1 ± 4.2 | 26.0 ± 3.8 | 27.5 ± 4.3 | n.s. | n.s. |
| Systolic RR, mmHg, mean ± SD | 136 ± 28 | 137 ± 33 | 135 ± 21 | 146 ± 18 | 136 ± 22 | n.s. | n.s. |
| Diastolic RR, mmHg, mean ± SD | 79 ± 14 | 81 ± 13 | 77 ± 14 | 84 ± 10 | 75 ± 16 | n.s. | n.s. |
| Female sex N, % | 55 (39) | 17 (23) | 38 (57) | 26 (58) | 12 (55) | <0.001 | <0.001 |
| Self-reported appetite | 6.5 ± 2.2 | 6.7 ± 2.1 | 6.3 ±2.3 | 6.8 ± 2.1 | 5.4 ± 2.4 * | n.s. | 0.05 |
| Stroke severity National Institute of Health Stroke Scale (NIHSS) | |||||||
| Mean score ± SD | 4.7 ± 3.4 | 4.8 ± 3.6 | 4.6 ± 3.1 | 4.1 ± 2.7 | 5.6 ± 3.6 | n.s | n.s. |
| 0–4, N (%) | 83 (59) | 42 (57) | 41 (62) | 32 (71) | 9 (41) | n.s. | n.s. |
| Trial of ORG 10172 in Acute Stroke Treatment | |||||||
| Cardioembolic, N (%) | 44 (31) | 20 (27) | 24 (36) | 12 (27) | 12 (55) * | n.s. | <0.05 |
| Large-artery atherosclerosis, N (%) | 49 (35) | 26 (36) | 23 (35) | 16 (36) | 7 (32) | n.s. | n.s. |
| Small-vessel occlusion, N (%) | 25 (18) | 14 (19) | 11 (16) | 9 (20) | 2 (9) | n.s. | n.s. |
| Stroke of undetermined etiology | 22 (16) | 13 (18) | 9 (13) | 8 (17) | 1 (4) | n.s. | n.s. |
| Physical status | |||||||
| Modified Rankin Scale (mRS) | |||||||
| Mean score ± SD | 2.4 ± 1.5 | 2.4 ± 1.6 | 2.4 ± 1.6 | 2.1 ± 1.3 | 2.9 ± 1.6 | n.s | n.s. |
| 0–1, N (%) | 58 (41) | 32 (44) | 26 (39) | 19 (42) | 7 (32) | n.s. | n.s. |
| Low Handgrip strength, N (%) | 61 (44) | 28 (38) | 33 (49) | 19 (42) | 14 (64) | n.s. | n.s. |
| Comorbidities | |||||||
| Diabetes mellitus, N (%) | 40 (29) | 19 (26) | 21 (38) | 13 (36) | 7 (33) | n.s. | n.s. |
| Arterial hypertension, N (%) | 96 (69) | 49 (67) | 47 (70) | 31 (69) | 16 (76) | n.s. | n.s. |
| Dyslipidemia, N (%) | 45 (32) | 22 (30) | 23 (34) | 17 (38) | 6 (27) | n.s. | n.s. |
| Anemia, N (%) | 25 (19) | 7 (10) | 18 (27) | 9 (20) | 9 (41) | <0.01 | <0.01 |
| Cardiovascular disease, N (%) | 56 (40) | 29 (40) | 29 (43) | 15 (33) | 5 (23) | n.s. | n.s. |
| Biochemistry | |||||||
| Hemoglobin, mg/dL, mean ± SD | 14.0 ± 1.9 | 14.6 ± 1.7 | 13.3 ± 1.8 | 13.4 ± 1.8 | 13.1 ± 1.9 | n.s. | 0.0001 |
| White blood cells count | 8.3 ± 2.5 | 8.1 ± 1.9 | 8.7 ± 3.1 | 8.1 ± 2.3 | 10.1 ± 4.2 ** | n.s. | <0.01 |
| Creatinine, mg/dL, mean ± SD | 1.0 ± 0.4 | 1.0 ± 0.4 | 1.0 ± 0.4 | 1.0 ± 0.4 | 0.9 ± 1.9 | n.s. | n.s. |
| Cholesterol, mg/dL, mean ± SD | 186 ± 43 | 189 ± 37 | 182 ± 49 | 190 ± 50 | 166 ± 43 * | n.s. | n.s. |
| High density lipoprotein, mg/dL, mean ± SD | 49 ± 15 | 46 ± 12 | 51 ± 16 | 54 ± 17 * | 46 ± 12 | <0.05 | <0.05 |
| Low density lipoprotein, mg/dL, mean ± SD | 110 ± 38 | 115 ± 34 | 104 ± 41 | 109 ± 39 | 93 ± 45 | n.s. | n.s. |
| Hemoglobin A1c, %, median [IQR] | 5.9 [5.4–6.5] | 5.8 [5.4–6.5] | 5.9 [5.5–6.5] | 5.8 [5.5–6.7] | 5.6 [5.6–6.6] | n.s | n.s. |
| C-reactive protein, mg/L, median [IQR] | 4.8 [1.7–11.8] | 4.1 [1.7–12] | 6.6 [1.7–10.35] | 4.1 [1.7–7] | 16.7 [7.2–26.2] * | n.s | <0.01 |
| Systemic inflammation, N (%) | 63 (45) | 30 (41) | 33 (49) | 16 (35) | 17 (77) * | n.s. | n.s. |
| Medication | |||||||
| Antiplatelet drugs, N (%) | 120 (86) | 61 (84) | 59 (88) | 41 (91) | 18 (82) | n.s. | n.s. |
| Anticoagulants, N (%) | 29 (21) | 16 (22) | 13 (19) | 6 (13) | 7 (32) | n.s. | n.s. |
| Proton pump inhibitors, N (%) | 34 (24) | 16 (22) | 18 (27) | 13 (29) | 5 (23) | n.s. | n.s. |
| β-blocker, N (%) | 57 (41) | 28 (38) | 29 (43) | 17 (38) | 12 (55) | n.s. | n.s. |
| ACE-inhibitors, N (%) | 65 (46) | 39 (53) | 26 (39) | 15 (45) | 11 (50) | n.s. | n.s. |
| Ca2+-channel antagonists, N (%) | 14 (10) | 7 (10) | 7 (19) | 5 (11) | 2 (9) | n.s. | n.s. |
| Angiotensin II receptor blockers, N (%) | 4 (3) | 2 (3) | 2 (3) | 1 (2) | 1 (5) | n.s. | n.s. |
| Diuretics, N (%) | 29 (21) | 12 (16) | 17 (25) | 10 (22) | 7 (32) | n.s. | n.s. |
| Statins, N (%) | 100 (71) | 53 (73) | 47 (70) | 37 (82) | 10 (45) | n.s. | n.s. |
| Parameter | OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p |
|---|---|---|---|---|---|---|---|---|---|
| Univariate | Model 1 | Model 2 | |||||||
| Transferrin saturation < 20% | 3.81 | 1.74–8.33 | <0.001 | 3.0 | 1.24–7.18 | <0.05 | |||
| Presence of ID | 2.04 | 1.00–4.15 | <0.05 | ||||||
| Presence of ID I | 0.96 | 0.44–2.08 | 0.9 | ||||||
| Presence of ID II | 4.42 | 1.25–15.65 | 0.02 | 4.35 | 1.23–15.45 | 0.03 | |||
| BMI (per kg/m2 increase) | 1.07 | 0.98–1.16 | 0.1 | 0.96 | 0.88–1.04 | 0.3 | 0.97 | 0.88–1.06 | 0.5 |
| Age (per year increase) | 1.07 | 1.04–1.11 | <0.001 | 1.06 | 1.03–1.10 | <0.001 | |||
| NIHSS (per point increase) | 1.06 | 0.95–1.19 | 0.3 | ||||||
| Hemoglobin, per mg/dL | 0.88 | 0.72–1.07 | 0.2 | ||||||
| Presence of Inflammation | 1.89 | 0.92–3.86 | 0.08 | 1.16 | 0.51–2.64 | 0.7 | |||
| Parameter | OR | 95% CI | p |
|---|---|---|---|
| Univariate | |||
| Transferrin saturation < 20% | 2.86 | 0.97–8.42 | 0.06 |
| Presence of ID | 3.0 | 0.91–9.91 | 0.07 |
| Presence of ID I | 2.59 | 0.73–9.25 | 0.1 |
| Presence of ID II | 3.9 | 0.91–16.8 | 0.07 |
| BMI (per kg/m2 increase) | 0.92 | 0.82–1.04 | 0.2 |
| Age (per year increase) | 1.08 | 1.02–1.14 | <0.001 |
| Hemoglobin, per mg/dL | 0.98 | 0.75–1.29 | 0.9 |
| Presence of Inflammation | 4.69 | 0.94–23.3 | 0.06 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scherbakov, N.; Sandek, A.; Valentova, M.; Mayer, A.; von Haehling, S.; Jankowska, E.; Anker, S.D.; Doehner, W. Iron Deficiency and Reduced Muscle Strength in Patients with Acute and Chronic Ischemic Stroke. J. Clin. Med. 2022, 11, 595. https://doi.org/10.3390/jcm11030595
Scherbakov N, Sandek A, Valentova M, Mayer A, von Haehling S, Jankowska E, Anker SD, Doehner W. Iron Deficiency and Reduced Muscle Strength in Patients with Acute and Chronic Ischemic Stroke. Journal of Clinical Medicine. 2022; 11(3):595. https://doi.org/10.3390/jcm11030595
Chicago/Turabian StyleScherbakov, Nadja, Anja Sandek, Miroslava Valentova, Antje Mayer, Stephan von Haehling, Ewa Jankowska, Stefan D. Anker, and Wolfram Doehner. 2022. "Iron Deficiency and Reduced Muscle Strength in Patients with Acute and Chronic Ischemic Stroke" Journal of Clinical Medicine 11, no. 3: 595. https://doi.org/10.3390/jcm11030595