
Cholangitis Definition and Treatment after Kasai Hepatoportoenterostomy for Biliary Atresia: A Delphi Process and International Expert Panel

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Systematic Literature Review
2.2. Formatting and Pretesting of the 1st Delphi Questionnaire
2.3. Format of the 2nd Delphi Questionnaire
2.4. Pre-Meeting Working Group
2.5. Expert Panel Meeting
2.6. Statistical Analysis
3. Results
3.1. Literature Search
3.2. 1st Delphi Questionnaire
3.3. 2nd Delphi Questionnaire
3.4. Pre-Meeting Working Group
3.5. Expert Panel
4. Discussion
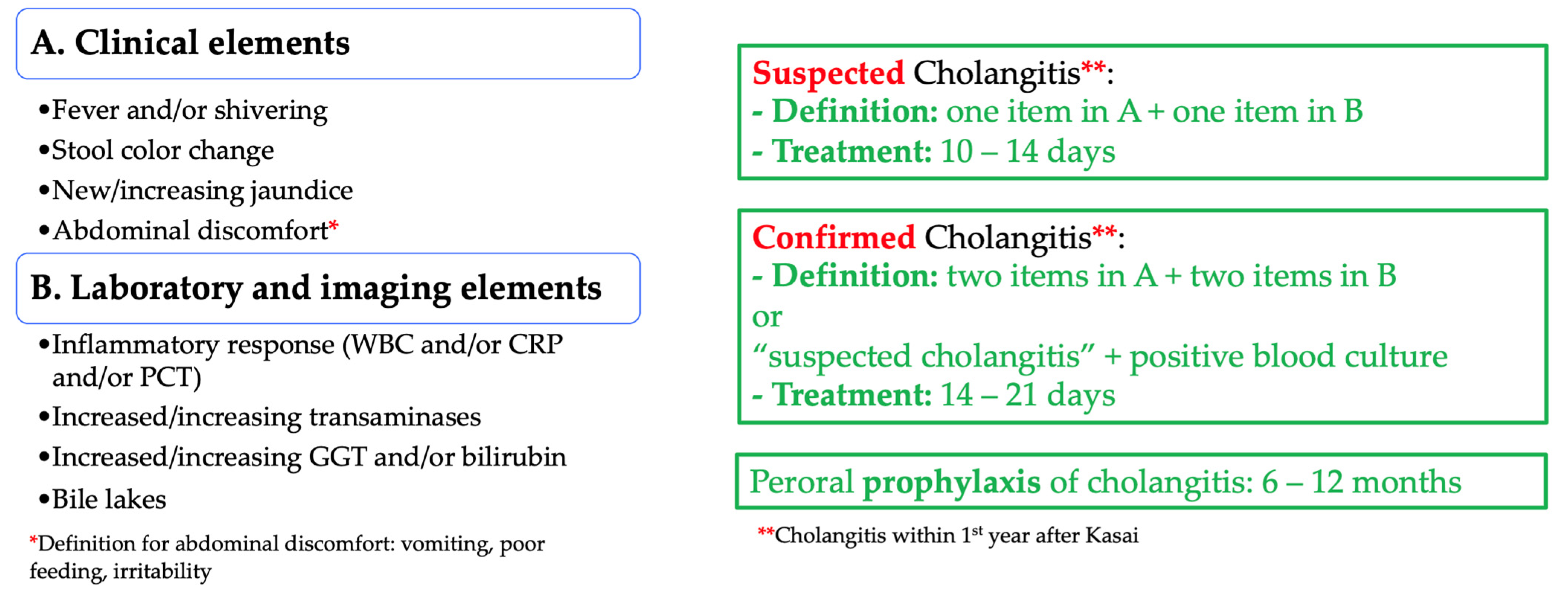
4.1. Definitions of Suspected and Confirmed Cholangitis
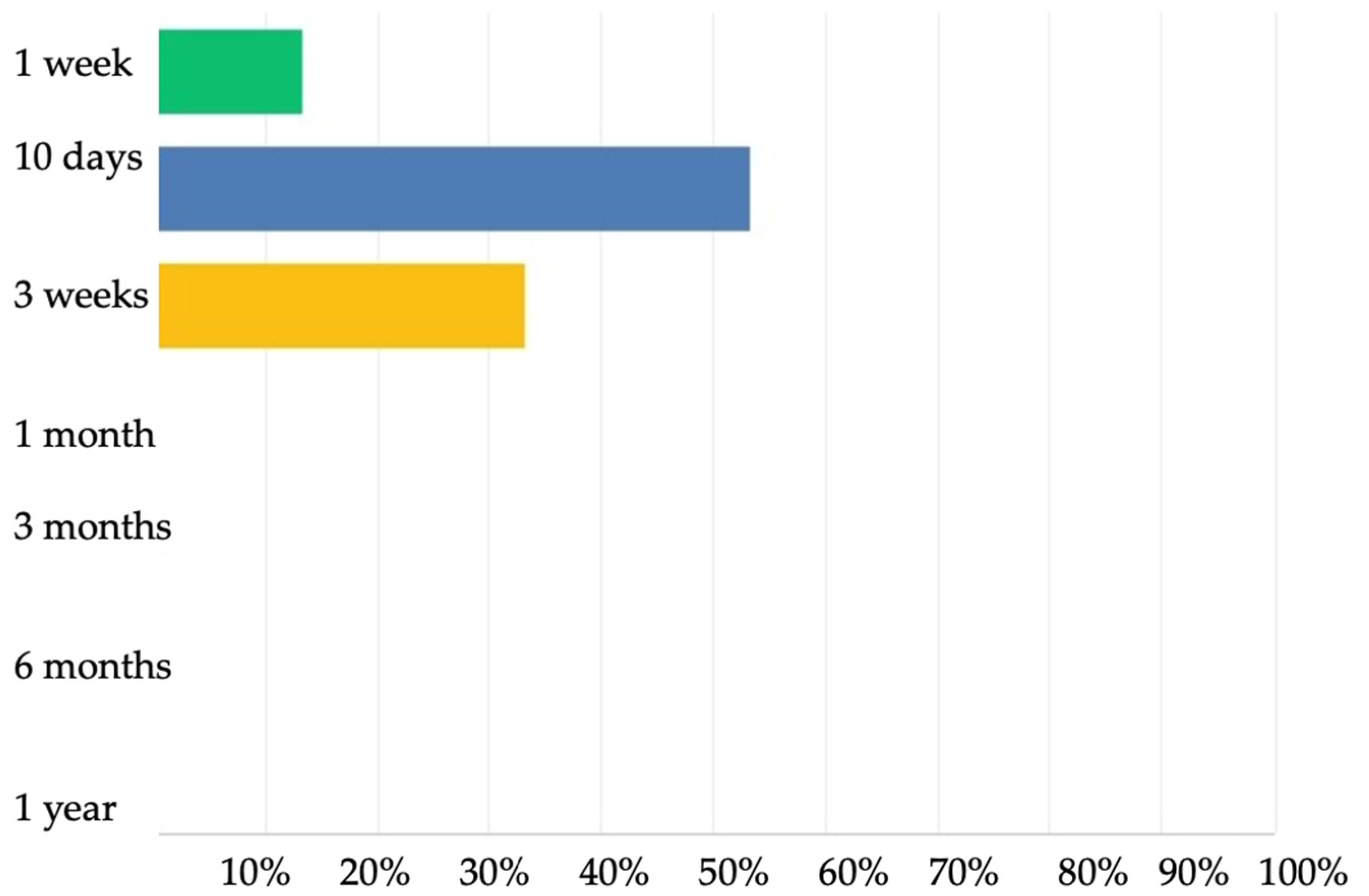
4.2. Treatment of Suspected and Confirmed Cholangitis
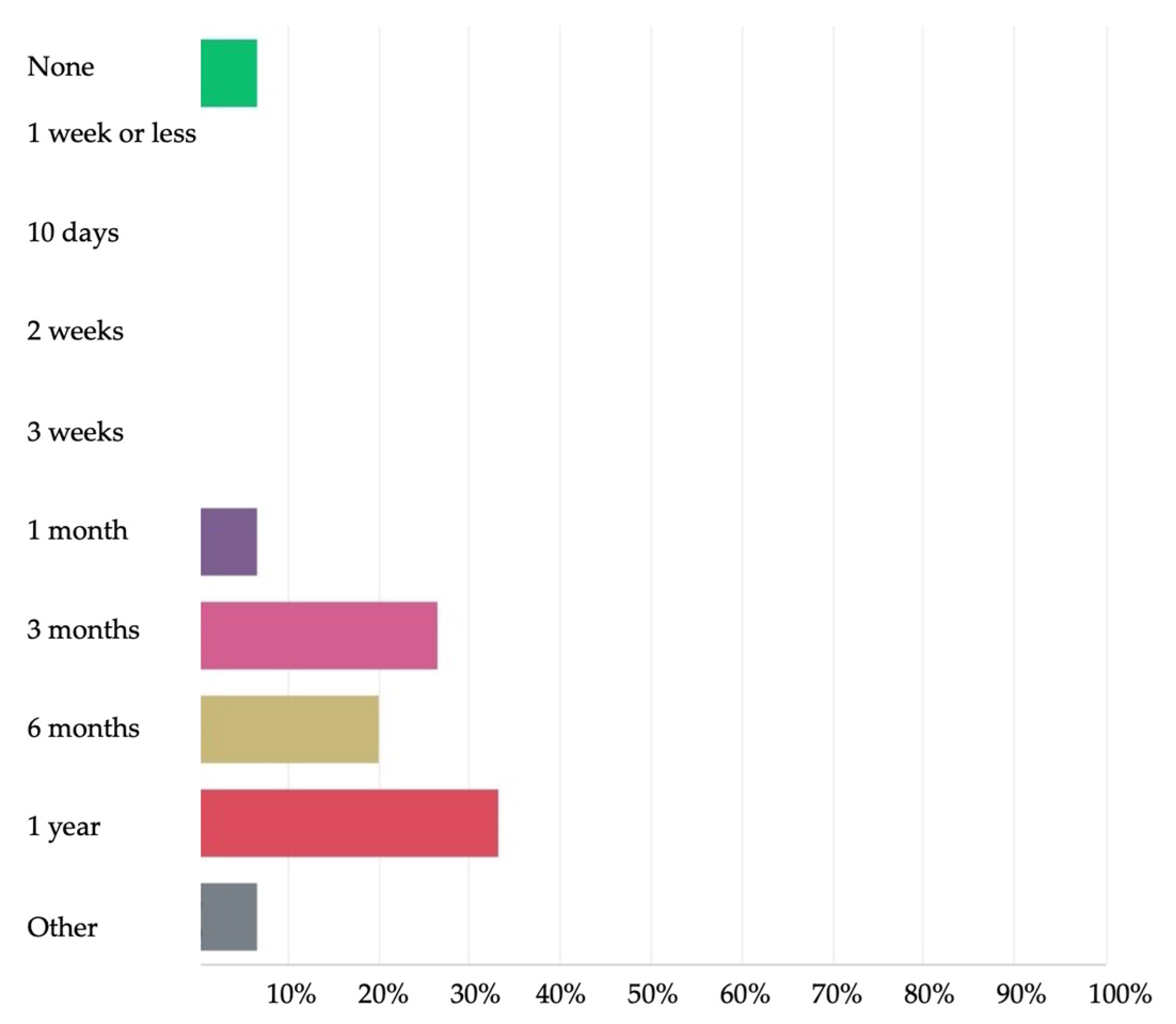
4.3. Cholangitis Prophylaxis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Number of Patients | Cholangitis Definition | Cholangitis Rates | NLS/PS |
|---|---|---|---|---|
| Chuang J., et al., 2000 [13] | 39 | Fever > 38 °C without obvious extrahepatic source with an elevated serum bilirubin | 46% | - |
| Wu E.T., et al., 2001 [10] | 45 | Fever, acholic stools, and/or increasing jaundice +/− positive blood cultures | 75% | PS, 67.5% |
| Selvalingam S., et al., 2002 [52] | 61 | Fever and leukocytosis (no other cause) + increase direct bilirubin or AST or ALT or paler stools +/− positive blood culture | 57% | 1 year PS, 90% |
| Bu L.N., et al., 2003 [9] | 19 | Unexplained fever ≥ 38 °C, acholic stools, increased jaundice or positive blood culture | 100% | - |
| Van Heurn E., et al., 2003 [14] | 77 | Fever > 38 °C, not explained otherwise or abrupt recurrence or increase of clinical jaundice with increased bilirubin levels or acholic stools | ||
| Ogasawara Y., et al., 2003 [53] | 21 | Fever > 38 °C and elevated bilirubin and leukocytosis | 52.3% | PS, 100% |
| Wong K.K., et al., 2004 [20] | 19 | Fever > 38.5 °C of unknown origin more than 48 h, progressive jaundice and derangement of liver function, passage of acholic stools | - | - |
| Kobayashi H., et al., 2005 [54] | 63 | Fever > 38 °C, with elevated serum bilirubin and leukocytosis | 15.8% | - |
| Shinohara T., et al., 2005 [55] | 18 | Unexplained fever > 38 °C, with elevated CRP and bilirubin. | 44.4% | - |
| Hung P., et al., 2006 [4] | 22 | High fever with no other obvious focus with acholic stools, increased jaundice, or positive blood culture | 54.6% | 2 year NLS, 53.2% 5 year NLS, 34.7% 10 year NLS, 30.5% |
| Lai H.S., 2006 [18] | 163 | Recurrent clay colored stool, icterus, or hyperbilirubinemia | 72.3% | - |
| Stringer M.D., et al., 2007 [28] | 71 | Deteriorating liver function + pale stools and fever | 46% | NLS, 67.5% PS, 93.3% |
| Vejchapipat P., et al., 2007 [29] | 53 | Fever > 38.5 °C, change of stool color, leukocytosis (>12 G/L) with polymorphonuclear leukocytes predominance | 45.2% | - |
| Petersen C., et al., 2008 [21] | 49 | Suspected cholangitis: any of fever, recurrence of acholic stools, leukocytosis, elevated liver function tests, increasing bilirubin | - | 6 month, NLS 63% 2 year, NLS 31% 6 month, PS 90% 2 year, PS 78% |
| Sanghai S.R., et al., 2009 [56] | 88 | Fever with clay colored stool, leukocytosis and/or vomiting, abdominal distension and bacteriemia | 33.3% | - |
| Suzuki T., et al., 2010 [57] | 53 | Fever, blood biochemistry and the decrease of bile secretion (fecal color change) | 13.2% (early) | NLS, 73.6% PS, 88.7% |
| Kumagi T., et al., 2011 [46] | 22 | Presumed cholangitis: fever and chills with or without jaundice, nausea or abdominal pain and abnormal biliary imaging: stricture, dilatation and/or stone, with or without evidence of an acute rise in liver tests or improvement upon administration of antibiotics | 50% | PS, 95.5% NLS, 81.8% |
| Lee J.Y., et al., 2014 [12] | 27 | Fever > 37.5 °C or worsening jaundice, transaminitis or acholic stools +/− positive blood cultures | 64.3% | - |
| Ng V., et al., 2014 [58] | 219 | Fever > 38 °C without other obvious source, new onset of acholic stools, right upper quadrant pain or tenderness and both elevation of direct bilirubin by 25% and at least 1 mg/dL above baseline, positive blood culture not required | 62.1% | - |
| Wada M., et al., 2014 [59] | 36 | Elevated serum bilirubin > 2.5 mg/dL, leukocytosis with left shift and normal to acholic stools in a febrile patient (>38 °C) | 48.8% | - |
| Lien T., et al., 2015 [40] | 20 | Unexplained fever > 38 °C, acholic stools, increased jaundice or positive blood cultures | 20% | - |
| Qiao G., et al., 2015 [60] | 262 | Fever > 38 °C, without other reason, recurrence or increased jaundice, increased bilirubin, acholic stools | 54.9% | 5 year PS, 43.3% 5 year NLS, 75.8% |
| Webb N.L., et al., 2016 [33] | 29 | Fever > 38.5 °C, and elevated liver transaminases in the absence of other cause for febrile illness | 75% | 5 year NLS, 45.8% |
| Chiang L.W., et al., 2017 [41] | 58 | Fever without other attributable cause, acholic stool and/or deepening jaundice | 30.5% | Overall NLS, 48.3% 2 year NLS, 72% 5 year NLS, 45.7% |
| Kelay A., et al., 2017 [61] | - | Fever, abdominal pain, worsening or recurring jaundice with acholic stools, changes in bilirubin and liver enzymes level together with acute changes in WBC and inflammatory markers such as CRP | - | - |
| Lee W.S., et al., 2017 [34] | 52 | Fever > 38 °C without other source, abdominal pain and new onset of acholic stools, and elevation of conjugated bilirubin and/or GGT from previous baseline | 52% | NLS, 37% PS, 51% |
| Stagg H., et al., 2017 [15] | - | Fever and/or jaundice, altered liver biochemistry, blood cultures (96%) and liver biopsy (26%) | - | - |
| Chen S., et al., 2018 [3] | 366 | Fever ≥ 38 °C and acholic stool, increase of jaundice and bilirubin or positive blood cultures | 67.7% | NLS, 74% |
| Chung P., et al., 2018 [48] | 192 | Fever ≥ 38.5 °C, with either increased bilirubin ≥ 20 μmol/L or acholic stool. | 35.4% | - |
| Jiang H., et al., 2018 [62] | - | High fever, bile discharge reduced or stopped, abdominal distention, vomiting and reduced liver function, worsening jaundice, elevated levels of Bilirubin and ALAT, pale or clay-colored stools, dark yellow colored urine, WBC and neutrophils elevated | - | - |
| Li D., et al., 2018 [5] | 113 | Fever without identifiable source and 1. Reappearance of jaundice or acholic stools; 2. Sudden elevation of bilirubin > 2.5 mg/dL or AST or 3. Positive blood culture | - | - |
| Nakajima H., et al., 2018 [63] | 66 | Fever > 38 °C, elevated serum bilirubin > 2.5 mg/dL, leukocytosis with left shift and normal to acholic stools | 55% | NLS, 74% |
| Xiao H., et al., 2018 [64] | 166 | Fever > 38 °C, unexplained by other reasons, abrupt recurrence or increased clinical jaundice with increased bilirubin levels, acholic stools, significantly increased serum WBC and neutrophil | 44.5% | 2 year NLS, 79.5% |
| Ginstrom D., et al., 2019 [65] | 61 | Fever > 38 °C without any other identifiable source, treated with intravenous antibiotics | 79% | - |
| Liu J., et al., 2019 [6] | 180 | At least 2 of: 1. Unexplained fever > 38 °C, 2. Recurrence or exacerbation of jaundice with increased bilirubin or changes from yellow to acholic stools, 3. Elevated CRP | 66.1% | NLS, 53.9% PS, 80% |
| Pang W., et al., 2019 [19] | 218 | Fever and/or altered stool or refractory jaundice, CRP and/or WBC elevation and sudden elevation of bilirubin or ALT or AST | 27% | - |
| Parolini F., et al., 2019 [35] | 174 | Fever, abdominal pain, worsening or recurrent jaundice, change in stool color associated with rise in bilirubin and liver enzyme levels, white cell count and inflammatory markers | 32% | 20 year NLS, 18.3% |
| Ramachandran P., et al., 2019 [36] | 62 | 1. Fever, pale stools. 2. Elevated WBC and CRP. 3. Elevation of bilirubin and/or liver enzymes | 43.5% | - |
| Baek S.H., et al., 2020 [37] | 160 | Fever > 38 °C or elevated inflammatory markers and evidence of cholestasis or abnormal liver function tests in accordance with Tokyo guidelines | 78.8% | 5 year PS, 93.3% |
| Madadi-Sanjani O., et al., 2020 [66] | 26 | Acholic stools or increase in serum bilirubin + fever or increase in inflammatory parameters | 34.6% | - |
| Chen G., et al., 2021 [38] | 180 | 1. Fever ≥ 38 °C or elevated CRP and 2. Recurrent acholic stool or jaundice with elevated bilirubin | 66.1% | NLS, 84.4% |
| Chung P.H.Y., et al., 2021 [67] | 231 | Fever > 38.5 °C and bilirubin > 20 μmol/L on 2 consecutive blood samples; severe cholangitis if more than 2 weeks of antibiotics. | 25.7% | NLS, 66.2% |
| Goh L., et al., 2021 [39] | 54 | 1. Systemic inflammation: fever or elevated inflammatory markers CRP and WBC and 2 evidence of cholestasis or abnormal liver function tests—PA, GGT, AST, ALT > 1.5 normal ranges and/or elevation from baseline levels | 72% | NLS, 79.4% |
References
- Nio, M.; Wada, M.; Sasaki, H.; Tanaka, H.; Okamura, A. Risk factors affecting late-presenting liver failure in adult patients with biliary atresia. J. Pediatr. Surg. 2012, 47, 2179–2183. [Google Scholar] [CrossRef]
- Koga, H.; Wada, M.; Nakamura, H.; Miyano, G.; Okawada, M.; Lane, G.J.; Okazaki, T.; Yamataka, A. Factors influencing jaundice-free survival with the native liver in post-portoenterostomy biliary atresia patients: Results from a single institution. J. Pediatr. Surg. 2013, 48, 2368–2372. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.Y.; Lin, C.C.; Tsan, Y.T.; Chan, W.C.; Wang, J.D.; Chou, Y.J.; Lin, C.H. Number of cholangitis episodes as a prognostic marker to predict timing of liver transplantation in biliary atresia patients after Kasai portoenterostomy. BMC Pediatr. 2018, 18, 119. [Google Scholar] [CrossRef] [Green Version]
- Hung, P.Y.; Chen, C.C.; Chen, W.J.; Lai, H.S.; Hsu, W.M.; Lee, P.H.; Ho, M.C.; Chen, T.H.; Ni, Y.H.; Chen, H.L.; et al. Long-term prognosis of patients with biliary atresia: A 25 year summary. J. Pediatr. Gastroenterol. Nutr. 2006, 42, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Chen, X.; Fu, K.; Yang, J.; Feng, J. Preoperative nutritional status and its impact on cholangitis after Kasai portoenterostomy in biliary atresia patients. Pediatr. Surg. Int. 2017, 33, 901–906. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Dong, R.; Chen, G.; Dong, K.; Zheng, S. Risk factors and prognostic effects of cholangitis after Kasai procedure in biliary atresia patients: A retrospective clinical study. J. Pediatr. Surg. 2019, 54, 2559–2564. [Google Scholar] [CrossRef] [PubMed]
- Ryon, E.L.; Parreco, J.P.; Sussman, M.S.; Quiroz, H.J.; Willobee, B.A.; Perez, E.A.; Sola, J.E.; Thorson, C.M. Drivers of Hospital Readmission and Early Liver Transplant after Kasai Portoenterostomy. J. Surg. Res. 2020, 256, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Decharun, K.; Leys, C.M.; West, K.W.; Finnell, S.M. Prophylactic Antibiotics for Prevention of Cholangitis in Patients With Biliary Atresia Status Post-Kasai Portoenterostomy: A Systematic Review. Clin. Pediatr. 2016, 55, 66–72. [Google Scholar] [CrossRef]
- Bu, L.N.; Chen, H.L.; Chang, C.J.; Ni, Y.H.; Hsu, H.Y.; Lai, H.S.; Hsu, W.M.; Chang, M.H. Prophylactic oral antibiotics in prevention of recurrent cholangitis after the Kasai portoenterostomy. J. Pediatr. Surg. 2003, 38, 590–593. [Google Scholar] [CrossRef]
- Wu, E.T.; Chen, H.L.; Ni, Y.H.; Lee, P.I.; Hsu, H.Y.; Lai, H.S.; Chang, M.H. Bacterial cholangitis in patients with biliary atresia: Impact on short-term outcome. Pediatr. Surg. Int. 2001, 17, 390–395. [Google Scholar] [CrossRef]
- Gunadi; Gunawan, T.A.; Widiyanto, G.; Yuanita, A.; Mulyani, N.S.; Makhmudi, A. Liver transplant score for prediction of biliary atresia patients’ survival following Kasai procedure. BMC Res. Notes 2018, 11, 381. [Google Scholar] [CrossRef]
- Lee, J.Y.; Lim, L.T.; Quak, S.H.; Prabhakaran, K.; Aw, M. Cholangitis in children with biliary atresia: Health-care resource utilisation. J. Paediatr. Child Health 2014, 50, 196–201. [Google Scholar] [CrossRef]
- Chuang, J.H.; Lee, S.Y.; Shieh, C.S.; Chen, W.J.; Chang, N.K. Reappraisal of the role of the bilioenteric conduit in the pathogenesis of postoperative cholangitis. Pediatr. Surg. Int. 2000, 16, 29–34. [Google Scholar] [CrossRef]
- Van Heurn, L.W.E.; Saing, H.; Tam, P.K. Cholangitis after hepatic portoenterostomy for biliary atresia: A multivariate analysis of risk factors. J. Pediatr. 2003, 142, 566–571. [Google Scholar] [CrossRef]
- Stagg, H.; Cameron, B.H.; Ahmed, N.; Butler, A.; Jimenez-Rivera, C.; Yanchar, N.L.; Martin, S.R.; Emil, S.; Anthopoulos, G.; Schreiber, R.A.; et al. Variability of diagnostic approach, surgical technique, and medical management for children with biliary atresia in Canada—Is it time for standardization? J. Pediatr. Surg. 2017, 52, 802–806. [Google Scholar] [CrossRef]
- Wada, K.; Takada, T.; Kawarada, Y.; Nimura, Y.; Miura, F.; Yoshida, M.; Mayumi, T.; Strasberg, S.; Pitt, H.A.; Gadacz, T.R.; et al. Diagnostic criteria and severity assessment of acute cholangitis: Tokyo Guidelines. J. Hepatobiliary Pancreat. Surg. 2007, 14, 52–58. [Google Scholar] [CrossRef] [Green Version]
- Takada, T.; Strasberg, S.M.; Solomkin, J.S.; Pitt, H.A.; Gomi, H.; Yoshida, M.; Mayumi, T.; Miura, F.; Gouma, D.J.; Garden, O.J.; et al. TG13: Updated Tokyo Guidelines for the management of acute cholangitis and cholecystitis. J. Hepatobiliary Pancreat. Sci. 2013, 20, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Lai, H.S.; Chen, W.J.; Chen, C.C.; Hung, W.T.; Chang, M.H. Long-term prognosis and factors affecting biliary atresia from experience over a 25 year period. Chang Gung. Med. J. 2006, 29, 234–239. [Google Scholar]
- Pang, W.B.; Zhang, T.C.; Chen, Y.J.; Peng, C.H.; Wang, Z.M.; Wu, D.Y.; Wang, K. Ten-Year Experience in the Prevention of Post-Kasai Cholangitis. Surg. Infect. 2019, 20, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.K.; Fan, A.H.; Lan, L.C.; Lin, S.C.; Tam, P.K. Effective antibiotic regime for postoperative acute cholangitis in biliary atresia—An evolving scene. J. Pediatr. Surg. 2004, 39, 1800–1802. [Google Scholar] [CrossRef] [PubMed]
- Petersen, C.; Harder, D.; Melter, M.; Becker, T.; Wasielewski, R.V.; Leonhardt, J.; Ure, B.M. Postoperative high-dose steroids do not improve mid-term survival with native liver in biliary atresia. Am. J. Gastroenterol. 2008, 103, 712–719. [Google Scholar] [CrossRef]
- Graham, B.; Regehr, G.; Wright, J.G. Delphi as a method to establish consensus for diagnostic criteria. J. Clin. Epidemiol. 2003, 56, 1150–1156. [Google Scholar] [CrossRef]
- Dalkey, N.C. An experimental application of the Delphi method to the use of experts. Manag. Sci. 1963, 9, 458–467. [Google Scholar] [CrossRef]
- Burns, K.E.; Duffett, M.; Kho, M.E.; Meade, M.O.; Adhikari, N.K.; Sinuff, T.; Cook, D.J.; Group, A. A guide for the design and conduct of self-administered surveys of clinicians. CMAJ 2008, 179, 245–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lally, K.P.; Kanegaye, J.; Matsumura, M.; Rosenthal, P.; Sinatra, F.; Atkinson, J.B. Perioperative factors affecting the outcome following repair of biliary atresia. Pediatrics 1989, 83, 723–726. [Google Scholar] [CrossRef] [PubMed]
- Meyers, R.L.; Book, L.S.; O’Gorman, M.A.; Jackson, W.D.; Black, R.E.; Johnson, D.G.; Matlak, M.E. High-dose steroids, ursodeoxycholic acid, and chronic intravenous antibiotics improve bile flow after Kasai procedure in infants with biliary atresia. J. Pediatr. Surg. 2003, 38, 406–411. [Google Scholar] [CrossRef]
- Kelly, D.A.; Davenport, M. Current management of biliary atresia. Arch. Dis. Child. 2007, 92, 1132–1135. [Google Scholar] [CrossRef] [Green Version]
- Stringer, M.D.; Davison, S.M.; Rajwal, S.R.; McClean, P. Kasai portoenterostomy: 12-year experience with a novel adjuvant therapy regimen. J. Pediatr. Surg. 2007, 42, 1324–1328. [Google Scholar] [CrossRef]
- Vejchapipat, P.; Passakonnirin, R.; Sookpotarom, P.; Chittmittrapap, S.; Poovorawan, Y. High-dose steroids do not improve early outcome in biliary atresia. J. Pediatr. Surg. 2007, 42, 2102–2105. [Google Scholar] [CrossRef]
- De Vries, W.; de Langen, Z.J.; Groen, H.; Scheenstra, R.; Peeters, P.M.; Hulscher, J.B.; Verkade, H.J.; Netherlands Study Group of Biliary Atresia and Registry (NeSBAR). Biliary atresia in the Netherlands: Outcome of patients diagnosed between 1987 and 2008. J. Pediatr. 2012, 160, 638–644.e2. [Google Scholar] [CrossRef]
- Wang, B.; Feng, Q.; Ye, X.; Zeng, S. The experience and technique in laparoscopic portoenterostomy for biliary atresia. J. Laparoendosc. Adv. Surg. Tech. A 2014, 24, 350–353. [Google Scholar] [CrossRef]
- Tyraskis, A.; Davenport, M. Steroids after the Kasai procedure for biliary atresia: The effect of age at Kasai portoenterostomy. Pediatr. Surg. Int. 2016, 32, 193–200. [Google Scholar] [CrossRef] [Green Version]
- Webb, N.L.; Jiwane, A.; Ooi, C.Y.; Nightinghale, S.; Adams, S.E.; Krishnan, U. Clinical significance of liver histology on outcomes in biliary atresia. J. Paediatr. Child Health 2017, 53, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.S.; Ong, S.Y.; Foo, H.W.; Wong, S.Y.; Kong, C.X.; Seah, R.B.; Ng, R.T. Chronic liver disease is universal in children with biliary atresia living with native liver. World J. Gastroenterol. 2017, 23, 7776–7784. [Google Scholar] [CrossRef]
- Parolini, F.; Boroni, G.; Milianti, S.; Tonegatti, L.; Armellini, A.; Garcia Magne, M.; Pedersini, P.; Torri, F.; Orizio, P.; Benvenuti, S.; et al. Biliary atresia: 20-40-year follow-up with native liver in an Italian centre. J. Pediatr. Surg. 2019, 54, 1440–1444. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, P.; Safwan, M.; Balaji, M.S.; Unny, A.K.; Akhtarkhavari, A.; Tamizhvanan, V.; Rela, M. Early Cholangitis after Portoenterostomy in Children with Biliary Atresia. J. Indian Assoc. Pediatr. Surg. 2019, 24, 185–188. [Google Scholar] [CrossRef]
- Baek, S.H.; Kang, J.M.; Ihn, K.; Han, S.J.; Koh, H.; Ahn, J.G. The Epidemiology and Etiology of Cholangitis After Kasai Portoenterostomy in Patients With Biliary Atresia. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 171–177. [Google Scholar] [CrossRef]
- Chen, G.; Liu, J.; Huang, Y.; Wu, Y.; Lu, X.; Dong, R.; Shen, Z.; Sun, S.; Jiang, J.; Zheng, S. Preventive effect of prophylactic intravenous antibiotics against cholangitis in biliary atresia: A randomized controlled trial. Pediatr. Surg. Int. 2021, 37, 1089–1097. [Google Scholar] [CrossRef] [PubMed]
- Goh, L.; Phua, K.B.; Low, Y.; Chiang, L.W.; Yong, C.; Chiou, F.K. Analysis of Cholangitis Rates with Extended Perioperative Antibiotics and Adjuvant Corticosteroids in Biliary Atresia. Pediatr. Gastroenterol. Hepatol. Nutr. 2021, 24, 366–376. [Google Scholar] [CrossRef]
- Lien, T.H.; Bu, L.N.; Wu, J.F.; Chen, H.L.; Chen, A.C.; Lai, M.W.; Shih, H.H.; Lee, I.H.; Hsu, H.Y.; Ni, Y.H.; et al. Use of Lactobacillus casei rhamnosus to Prevent Cholangitis in Biliary Atresia After Kasai Operation. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 654–658. [Google Scholar] [CrossRef]
- Chiang, L.W.; Lee, C.Y.; Krishnaswamy, G.; Nah, S.A.; Kader, A.; Ong, C.; Low, Y.; Phua, K.B. Seventeen years of Kasai portoenterostomy for biliary atresia in a single Southeast Asian paediatric centre. J. Paediatr. Child Health 2017, 53, 412–415. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Ye, Y.; Wu, Z.; Wang, B. Learning Curve Analysis of Laparoscopic Kasai Portoenterostomy. J. Laparoendosc. Adv. Surg. Tech. A 2017, 27, 979–982. [Google Scholar] [CrossRef] [PubMed]
- Calinescu, A.M.; Wilde, J.C.H.; Korff, S.; McLin, V.A.; Wildhaber, B.E. Perioperative Complications after Kasai Hepatoportoenterostomy: Data from the Swiss National Biliary Atresia Registry. Eur. J. Pediatr. Surg. 2020, 30, 364–370. [Google Scholar] [CrossRef]
- Chung, P.H.Y.; Chok, K.S.H.; Wong, K.K.Y.; Tam, P.K.H.; Lo, C.M. Determining the optimal timing of liver transplant for pediatric patients after Kasai portoenterostomy based on disease severity scores. J. Pediatr. Surg. 2020, 55, 1892–1896. [Google Scholar] [CrossRef]
- Sifri, C.D.; Madoff, L.C. Infections of the Liver and Biliary system (Liver abscess, cholangitis, cholecystitis). In Mandell, Douglas and Bennett’s Priciples and Practice of Infectious Diseases, 8th ed.; WB Saunders: Philadelphia, PA, USA, 2015. [Google Scholar]
- Kumagi, T.; Drenth, J.P.; Guttman, O.; Ng, V.; Lilly, L.; Therapondos, G.; Hiasa, Y.; Michitaka, K.; Onji, M.; Watanabe, Y.; et al. Biliary atresia and survival into adulthood without transplantation: A collaborative multicentre clinic review. Liver Int. 2012, 32, 510–518. [Google Scholar] [CrossRef] [PubMed]
- Kiriyama, S.; Takada, T.; Hwang, T.L.; Akazawa, K.; Miura, F.; Gomi, H.; Mori, R.; Endo, I.; Itoi, T.; Yokoe, M.; et al. Clinical application and verification of the TG13 diagnostic and severity grading criteria for acute cholangitis: An international multicenter observational study. J. Hepatobiliary Pancreat. Sci. 2017, 24, 329–337. [Google Scholar] [CrossRef]
- Chung, P.H.Y.; Tam, P.K.H.; Wong, K.K.Y. Does the identity of the bacteria matter in post-Kasai cholangitis? A comparison between simple and intractable cholangitis. J. Pediatr. Surg. 2018, 53, 2409–2411. [Google Scholar] [CrossRef]
- Sandy, N.S.; Hessel, G.; Bellomo-Brandao, M.A. Major Complications of Pediatric Percutaneous Liver Biopsy Do Not Differ Among Physicians with Different Degrees of Training. Am. J. Gastroenterol. 2020, 115, 786–789. [Google Scholar] [CrossRef]
- Luo, Y.; Zheng, S. Current concept about postoperative cholangitis in biliary atresia. World J. Pediatr. 2008, 4, 14–19. [Google Scholar] [CrossRef]
- Pakarinen, M.P.; Rintala, R.J. Surgery of biliary atresia. Scand. J. Surg. 2011, 100, 49–53. [Google Scholar] [CrossRef] [Green Version]
- Selvalingam, S.; Mahmud, M.N.; Thambidorai, C.R.; Zakaria, Z.; Mohan, N.; Isa; Sheila, M. Jaundice clearance and cholangitis in the first year following portoenterostomy for biliary atresia. Med. J. Malays. 2002, 57, 92–96. [Google Scholar]
- Ogasawara, Y.; Yamataka, A.; Tsukamoto, K.; Okada, Y.; Lane, G.J.; Kobayashi, H.; Miyano, T. The intussusception antireflux valve is ineffective for preventing cholangitis in biliary atresia: A prospective study. J. Pediatr. Surg. 2003, 38, 1826–1829. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, H.; Yamataka, A.; Koga, H.; Okazaki, T.; Tamura, T.; Urao, M.; Yanai, T.; Lane, G.J.; Miyano, T. Optimum prednisolone usage in patients with biliary atresia postportoenterostomy. J. Pediatr. Surg. 2005, 40, 327–330. [Google Scholar] [CrossRef]
- Shinohara, T.; Muraji, T.; Tsugawa, C.; Nishijima, E.; Satoh, S.; Takamizawa, S. Efficacy of urinary sulfated bile acids for diagnosis of bacterial cholangitis in biliary atresia. Pediatr. Surg. Int. 2005, 21, 701–704. [Google Scholar] [CrossRef] [PubMed]
- Sanghai, S.R.; Shah, I.; Bhatnagar, S.; Murthy, A. Incidence and prognostic factors associated with biliary atresia in western India. Ann. Hepatol. 2009, 8, 120–122. [Google Scholar] [CrossRef]
- Suzuki, T.; Hashimoto, T.; Kondo, S.; Sato, Y.; Hussein, M.H. Evaluating patients’ outcome post-Kasai operation: A 19-year experience with modification of the hepatic portoenterostomy and applying a novel steroid therapy regimen. Pediatr. Surg. Int. 2010, 26, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Ng, V.L.; Haber, B.H.; Magee, J.C.; Miethke, A.; Murray, K.F.; Michail, S.; Karpen, S.J.; Kerkar, N.; Molleston, J.P.; Romero, R.; et al. Medical status of 219 children with biliary atresia surviving long-term with their native livers: Results from a North American multicenter consortium. J. Pediatr. 2014, 165, 539–546.e2. [Google Scholar] [CrossRef] [Green Version]
- Wada, M.; Nakamura, H.; Koga, H.; Miyano, G.; Lane, G.J.; Okazaki, T.; Urao, M.; Murakami, H.; Kasahara, M.; Sakamoto, S.; et al. Experience of treating biliary atresia with three types of portoenterostomy at a single institution: Extended, modified Kasai, and laparoscopic modified Kasai. Pediatr. Surg. Int. 2014, 30, 863–870. [Google Scholar] [CrossRef]
- Qiao, G.; Li, L.; Cheng, W.; Zhang, Z.; Ge, J.; Wang, C. Conditional probability of survival in patients with biliary atresia after Kasai portoenterostomy: A Chinese population-based study. J. Pediatr. Surg. 2015, 50, 1310–1315. [Google Scholar] [CrossRef]
- Kelay, A.; Davenport, M. Long-term outlook in biliary atresia. Semin. Pediatr. Surg. 2017, 26, 295–300. [Google Scholar] [CrossRef]
- Jiang, H.; Gao, P.; Chen, H.; Zhong, Z.; Shu, M.; Zhang, Z.; She, J.; Liu, J. The Prognostic Value of CD8(+) and CD45RO(+) T Cells Infiltration and Beclin1 Expression Levels for Early Postoperative Cholangitis of Biliary Atresia Patients after Kasai Operation. J. Korean Med. Sci. 2018, 33, e198. [Google Scholar] [CrossRef]
- Nakajima, H.; Koga, H.; Okawada, M.; Nakamura, H.; Lane, G.J.; Yamataka, A. Does time taken to achieve jaundice-clearance influence survival of the native liver in post-Kasai biliary atresia? World J. Pediatr. 2018, 14, 191–196. [Google Scholar] [CrossRef]
- Xiao, H.; Huang, R.; Chen, L.; Diao, M.; Li, L. The Application of a Shorter Loop in Kasai Portoenterostomy Reconstruction for Ohi Type III Biliary Atresia: A Prospective Randomized Controlled Trial. J. Surg. Res. 2018, 232, 492–496. [Google Scholar] [CrossRef] [PubMed]
- Ginstrom, D.A.; Hukkinen, M.; Kivisaari, R.; Pakarinen, M.P. Biliary Atresia-associated Cholangitis: The Central Role and Effective Management of Bile Lakes. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 488–494. [Google Scholar] [CrossRef]
- Madadi-Sanjani, O.; Schukfeh, N.; Uecker, M.; Eckmann, S.; Dingemann, J.; Ure, B.M.; Petersen, C.; Kuebler, J.F. The Intestinal Flora at Kasai Procedure in Children with Biliary Atresia Appears Not to Affect Postoperative Cholangitis. Eur. J. Pediatr. Surg. 2021, 31, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Chung, P.H.Y.; Chan, E.K.W.; Yeung, F.; Chan, A.C.Y.; Mou, J.W.C.; Lee, K.H.; Hung, J.W.S.; Leung, M.W.Y.; Tam, P.K.H.; Wong, K.K.Y. Life long follow up and management strategies of patients living with native livers after Kasai portoenterostomy. Sci. Rep. 2021, 11, 11207. [Google Scholar] [CrossRef] [PubMed]







| Authors | Nr. px | Cholangitis Prophylaxis | Cholangitis Prophylaxis Duration | Cholangitis Rates |
|---|---|---|---|---|
| Chuang J., et al., 2000 [13] | 39 | Sulfamethoxazole | 3 months | 46% |
| Lally K.P., et al., 1989 [25] | 41 | Sulfamethoxazole; Ampicillin; Cephalosporins | 1 to several months | 21.9% |
| Wu E.T., et al., 2001 [10] | 37 | Sulfamethoxazole 4 mg/kg or Neomycin 25 mg/kg 4×/week | Unknown | 75% |
| Bu L.N., et al., 2003 [9] | 19 | Sulfamethoxazole 20 mg/kg/d bid or Neomycin 25 mg/kg/d qid, 4 days/week | 6–7 months | - |
| Meyers R.L., et al., 2003 [26] | 28 | Piperacillin/Tazobactam 300 mg/kg/d qid + Gentamycin 5 mg/kg/d or Cefoperazone 150 mg/kg/d divided into 3 doses followed by Sulfamethoxazole 10 mg/kg/d bid | First regimen given 2–3 months and then unknown | 34.4% |
| Lai H.S., et al., 2006 [18] | 163 | Sulfamethoxazole 20 mg/kg/d bid or Neomycin 25 mg/kg/d, qid, 4 days/week | 3 years | 72.3% |
| Hung P.Y., et al., 2006 [4] | 185 | Oral antibiotics | 1–6 months | 54.6% |
| Kelly D.A., et al., 2007 [27] | - | Amoxicillin or Cephalexin or Sulfamethoxazole | Alternate every 2–3 months for 1 year minimum | - |
| Stringer M.D., et al., 2007 [28] | 71 | Cephalexin 25 mg/kg 2×/day oral | 1 month | 46% |
| Vejchapipat P., et al., 2007 [29] | 53 | Cotrimoxazole | 1 year | 45.2% |
| Petersen C., et al., 2008 [21] | 49 | Cefaclor 45 mg/kg/d oral | 1 year | - |
| De Vries W., et al., 2012 [30] | 214 | Sulfamethoxazole or Neomycin/Colistin/Nystatin or Ciprofloxacin | - | 55.1% |
| Wang B., et al., 2014 [31] | 25 | - | 6 months | 35% |
| Tyraskis A., et al., 2016 [32] | 104 | Cefalexin 25 mg/kg/d | 1 month | - |
| Webb N.L., et al., 2016 [33] | 29 | - | >1 year | 75% |
| Lee W.S., et al., 2017 [34] | 52 | - | 3 months | 36% |
| Pang W., et al., 2019 [19] | 218 | 3rd generation Cephalosporin, oral | 6 months | 27% |
| Parolini F., et al., 2019 [35] | 174 | Sulfamethoxazole and Cephalosporin, 1 year if good bile drainage | 1 year | 32% |
| Ramachandran P., et al., 2019 [36] | 62 | Alternating Amoxicillin–Clavulanic Acid 40 mg/kg/d bid and Cefpodoxime 10 mg/kg/d bid, alternating | 6 months | 43.5% |
| Baek S.H., 2020 [37] | 160 | None | None | 78.8% |
| Chen G., et al., 2021 [38] | 180 | Sulfamethoxazole 25 mg/kg/d bid for 2 weeks then Cefaclor 40 mg/kg/d bid for 2 weeks, alternating every 2 weeks | 6 months | 66.1% |
| Goh L., et al., 2021 [39] | 54 | Cotrimoxazole | 1 year minimum | 72% |
| Authors | Number of Patients | Cholangitis Treatment | Cholangitis Treatment Duration | Native Liver Survival |
|---|---|---|---|---|
| Chuang J., et al., 2000 [13] | 39 | Cephalosporin and Aminoglycoside | 7–10 days or till negative CRP | - |
| Wu E.T., et al., 2001 [10] | 37 | Ceftriaxone | At least 5 days | - |
| Van Heurn E., et al., 2003 [14] | 77 | 3rd generation Cephalosporin | 1 week | - |
| Wong K.K., et al., 2004 [20] | 19 | Cefoperazone 25 mg/kg 3×/day or Meropenem 20 mg/kg 3×/day | 2 weeks | - |
| Petersen C., et al., 2008 [21] | 49 | 3rd generation Cephalosporin and Aminoglycoside | 3 weeks | 6 month, NLS 63% 2 year, NLS 31% |
| Lee J Y., et al., 2014 [12] | 27 | Ampicillin, Gentamycin, and Metronidazole or Unasyn | 14 days | - |
| Lien T., et al., 2015 [40] | 20 | Ceftriaxone | 14 days | - |
| Chiang L.W., et al., 2017 [41] | 58 | Ceftriaxone 100 mg/kg/day or Piperacilline–Tazobactam 320 mg/kg/day recently | - | Overall NLS, 48.3% 2 year NLS, 72% 5 year NLS, 45.7% |
| Lee W.S., et al., 2017 [34] | 52 | - | 10–14 days | NLS, 37% |
| Li Z., et al., 2017 [42] | 80 | Meropenem or Cefoperazone | - | - |
| Li D., et al., 2018 [5] | 113 | Meropenem 20 mg/kg 3×/j | 5 days | - |
| Calinescu A.M., et al., 2019 [43] | 62 | Piperacillin–Tazobactam | 3 weeks | 4 year NLS for cholangitis patients, 36% |
| Ramachandran P., et al., 2019 [36] | 62 | Piperacillin–Tazobactam | - | 1 year NLS for cholangitis patients, 33% |
| Chung P.H.Y., et al., 2020 [44] | 128 | Meropenem Cefoperazone | 2 weeks 2 weeks | 1 year NLS, 85.7% 1 year NLS, 69% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calinescu, A.M.; Madadi-Sanjani, O.; Mack, C.; Schreiber, R.A.; Superina, R.; Kelly, D.; Petersen, C.; Wildhaber, B.E. Cholangitis Definition and Treatment after Kasai Hepatoportoenterostomy for Biliary Atresia: A Delphi Process and International Expert Panel. J. Clin. Med. 2022, 11, 494. https://doi.org/10.3390/jcm11030494
Calinescu AM, Madadi-Sanjani O, Mack C, Schreiber RA, Superina R, Kelly D, Petersen C, Wildhaber BE. Cholangitis Definition and Treatment after Kasai Hepatoportoenterostomy for Biliary Atresia: A Delphi Process and International Expert Panel. Journal of Clinical Medicine. 2022; 11(3):494. https://doi.org/10.3390/jcm11030494
Chicago/Turabian StyleCalinescu, Ana M., Omid Madadi-Sanjani, Cara Mack, Richard A. Schreiber, Riccardo Superina, Deirdre Kelly, Claus Petersen, and Barbara E. Wildhaber. 2022. "Cholangitis Definition and Treatment after Kasai Hepatoportoenterostomy for Biliary Atresia: A Delphi Process and International Expert Panel" Journal of Clinical Medicine 11, no. 3: 494. https://doi.org/10.3390/jcm11030494