
Adjuvant Therapy with Budesonide Post-Kasai Reduces the Need for Liver Transplantation in Biliary Atresia

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Diagnostics and Treatment
2.2. Patients and Data Management
2.3. Statistics
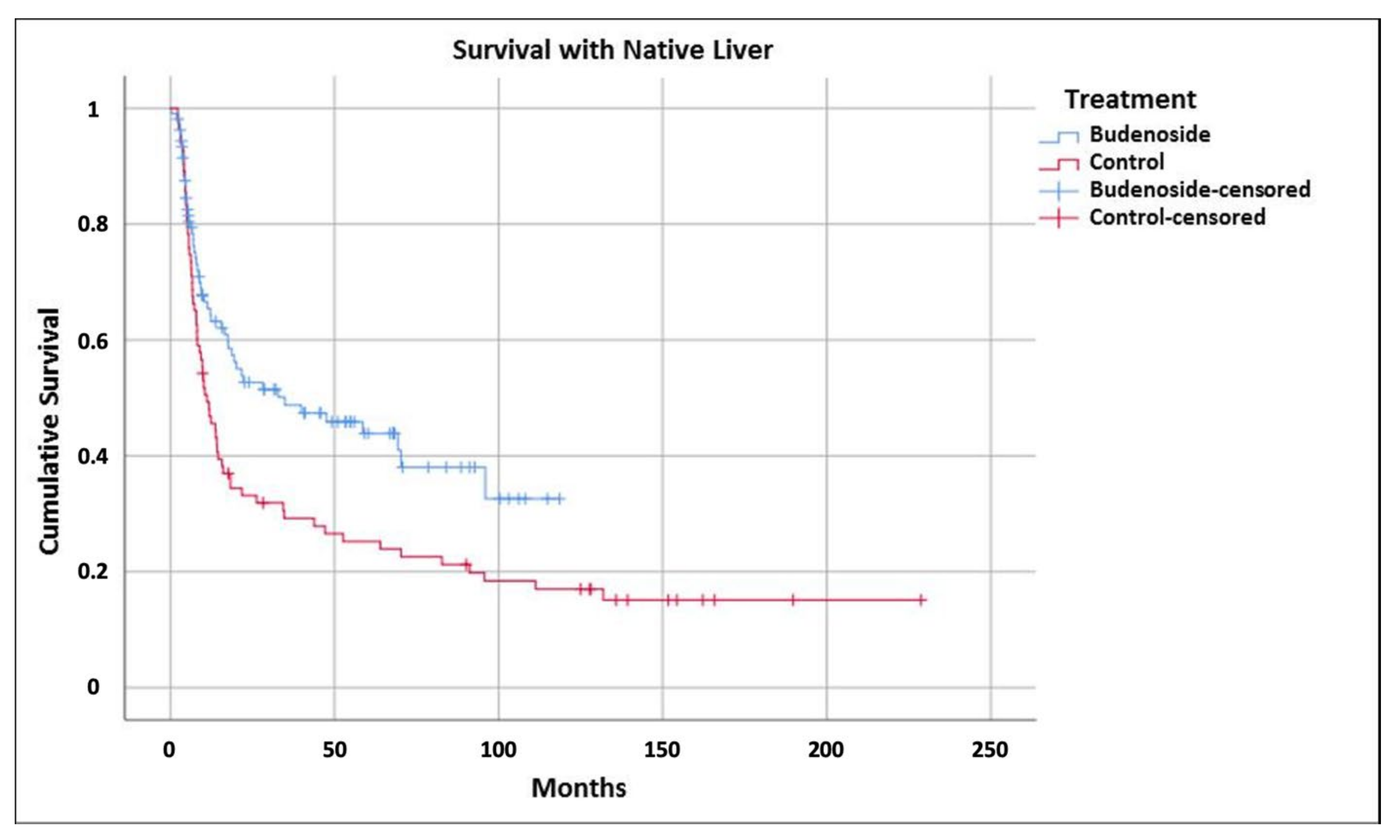
3. Results
4. Discussion
5. Conclusions and Perspectives
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AIH | Autoimmune Hepatitis |
| ALT | Alanine Aminotransferase |
| ASD | Atrial Septal Defect |
| AST | Aspartate Aminotransferase |
| BA | Biliary Atresia |
| BARD | Biliary Atresia and Related Diseases |
| CG | Control Group |
| CMV | Cytomegalovirus |
| EBAR | European Biliary Atresia Registry |
| ERC | Endoscopic Retrograde Cholangiography |
| GGT | Gamma Glutamyl Transferase |
| jfSNL | Jaundice-free Survival with Native Liver |
| KPE | Kasai Portoenterostomy |
| LTx | Liver Transplantation |
| PBC | Primary Biliary Cholangitis |
| SG | Study Group |
| SNL | Survival with Native Liver |
| SSSE | Systemic Steroid Specific Side Effects |
References
- Verkade, H.J.; Bezerra, J.A.; Davenport, M.; Schreiber, R.A.; Mieli-Vergani, G.; Hulscher, J.B.; Sokol, R.J.; Kelly, D.A.; Ure, B.; Whitington, P.F.; et al. Biliary atresia and other cholestatic childhood diseases: Advances and future challenges. J. Hepatol. 2016, 65, 631–642. [Google Scholar] [CrossRef] [Green Version]
- Fanna, M.; Masson, G.; Capito, C.; Girard, M.; Guerin, F.; Hermeziu, B.; Lachaux, A.; Roquelaure, B.; Gottrand, F.; Broue, P.; et al. Management of Biliary Atresia in France 1986 to 2015: Long-term Results. J. Pediatr. Gastroenterol. Nutr. 2019, 69, 416–424. [Google Scholar] [CrossRef] [PubMed]
- Parolini, F.; Boroni, G.; Milianti, S.; Tonegatti, L.; Armellini, A.; Magne, M.G.; Pedersini, P.; Torri, F.; Orizio, P.; Benvenuti, S.; et al. Biliary atresia: 20–40-year follow-up with native liver in an Italian centre. J. Pediatr. Surg. 2019, 54, 1440–1444. [Google Scholar] [CrossRef] [PubMed]
- Petersen, C.; Davenport, M. Aetiology of biliary atresia: What is actually known? Orphanet J. Rare Dis. 2013, 8, 128. [Google Scholar] [CrossRef] [Green Version]
- Mack, C.L. What Causes Biliary Atresia? Unique Aspects of the Neonatal Immune System Provide Clues to Disease Pathogenesis. Cell. Mol. Gastroenterol. Hepatol. 2015, 1, 267–274. [Google Scholar] [CrossRef] [Green Version]
- Kilgore, A.; Mack, C.L. Update on investigations pertaining to the pathogenesis of biliary atresia. Pediatr. Surg. Int. 2017, 33, 1233–1241. [Google Scholar] [CrossRef] [Green Version]
- Klemann, C.; Schröder, A.; Dreier, A.; Möhn, N.; Dippel, S.; Winterberg, T.; Wilde, A.; Yu, Y.; Thorenz, A.; Gueler, F.; et al. Interleukin 17, Produced by gammadelta T Cells, Contributes to Hepatic Inflammation in a Mouse Model of Biliary Atresia and Is Increased in Livers of Patients. Gastroenterology 2016, 150, 229–241. [Google Scholar] [CrossRef] [Green Version]
- Burns, J.; Davenport, M. Adjuvant treatments for biliary atresia. Transl. Pediatr. 2020, 9, 253–265. [Google Scholar] [CrossRef]
- Pietrobattista, A.; Mosca, A.; Liccardo, D.; Alterio, T.; Grimaldi, C.; Basso, M.; Saffioti, M.C.; Della Corte, C.; Spada, M.; Candusso, M. Does the Treatment After Kasai Procedure Influence Biliary Atresia Outcome and Native Liver Survival? J. Pediatr. Gastroenterol. Nutr. 2020, 71, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.Z.; Xun, P.C.; He, K.; Cai, W. Adjuvant steroid treatment following Kasai portoenterostomy and clinical outcomes of biliary atresia patients: An updated meta-analysis. World J. Pediatr. 2016, 13, 20–26. [Google Scholar] [CrossRef]
- Manns, M.P.; Woynarowski, M.; Kreisel, W.; Lurie, Y.; Rust, C.; Zuckerman, E.; Bahr, M.J.; Günther, R.; Hultcrantz, R.W.; Spengler, U.; et al. Budesonide induces remission more effectively than prednisone in a controlled trial of patients with autoimmune hepatitis. Gastroenterology 2010, 139, 1198–1206. [Google Scholar] [CrossRef]
- Manns, M.P.; Jaeckel, E.; Taubert, R. Budesonide in Autoimmune Hepatitis: The Right Drug at the Right Time for the Right Patient. Clin. Gastroenterol. Hepatol. 2017, 16, 186–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peiseler, M.; Liebscher, T.; Sebode, M.; Zenouzi, R.; Hartl, J.; Ehlken, H.; Pannicke, N.; Weiler-Normann, C.; Lohse, A.W.; Schramm, C. Efficacy and Limitations of Budesonide as a Second-Line Treatment for Patients With Autoimmune Hepatitis. Clin. Gastroenterol. Hepatol. 2018, 16, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Leuschner, M.; Maier, K.P.; Schlichting, J.; Strahl, S.; Herrmann, G.; Dahm, H.H.; Ackermann, H.; Happ, J.; Leuschne, U. Oral budesonide and ursodeoxycholic acid for treatment of primary biliary cirrhosis: Results of a prospective double-blind trial. Gastroenterology 1999, 117, 918–925. [Google Scholar] [CrossRef]
- Rautiainen, H.; Kärkkäinen, P.; Karvonen, A.-L.; Nurmi, H.; Pikkarainen, P.; Nuutinen, H.; Färkkilä, M. Budesonide combined with UDCA to improve liver histology in primary biliary cirrhosis: A three-year randomized trial. Hepatology 2005, 41, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Hirschfield, G.M.; Beuers, U.; Kupcinskas, L.; Ott, P.; Bergquist, A.; Färkkilä, M.; Manns, M.P.; Parés, A.; Spengler, U.; Stiess, M.; et al. A placebo-controlled randomised trial of budesonide for PBC following an insufficient response to UDCA. J. Hepatol. 2021, 74, 321–329. [Google Scholar] [CrossRef]
- Petersen, C.; Meier, P.N.; Schneider, A.; Turowski, C.; Pfister, E.D.; Manns, M.P.; Ure, B.M.; Wedemeyer, J. Endoscopic retrograde cholangiopancreaticography prior to explorative laparotomy avoids unnecessary surgery in patients suspected for biliary atresia. J. Hepatol. 2009, 51, 1055–1060. [Google Scholar] [CrossRef]
- Petersen, C.; Madadi-Sanjani, O. Registries for Biliary Atresia and Related Disorders. Eur. J. Pediatr. Surg. 2015, 25, 469–473. [Google Scholar] [PubMed]
- Petersen, C.M.; Harder, D.; Melter, M.; Becker, T.; Von Wasielewski, R.; Leonhardt, J.; Ure, B.M. Postoperative high-dose steroids do not improve mid-term survival with native liver in biliary atresia. Am. J. Gastroenterol. 2008, 103, 712–719. [Google Scholar] [CrossRef]
- Ure, B.M.; Kuebler, J.F.; Schukfeh, N.; Engelmann, C.; Dingemann, J.; Petersen, C. Survival with the native liver after laparoscopic versus conventional kasai portoenterostomy in infants with biliary atresia: A prospective trial. Ann. Surg. 2011, 253, 826–830. [Google Scholar] [CrossRef]
- Tyraskis, A.; Parsons, C.; Davenport, M. Glucocorticosteroids for infants with biliary atresia following Kasai portoenterostomy. Cochrane Database Syst. Rev. 2016, 5. [Google Scholar] [CrossRef]
- Karrer, F.; Lilly, J.R. Corticosteroid therapy in biliary atresia. J. Pediatr. Surg. 1985, 20, 693–695. [Google Scholar] [CrossRef]
- Petersen, C. Biliary atresia: Unity in diversity. Pediatr. Surg. Int. 2017, 33, 1255–1261. [Google Scholar] [CrossRef]
- Jee, J.; Mourya, R.; Shivakumar, P.; Fei, L.; Wagner, M.; Bezerra, J.A. Cxcr2 signaling and the microbiome suppress inflammation, bile duct injury, and the phenotype of experimental biliary atresia. PLoS ONE 2017, 12, e0182089. [Google Scholar] [CrossRef] [Green Version]
- Tessier, M.E.M.; Cavallo, L.; Yeh, J.; Harpavat, S.; Hoffman, K.L.; Petrosino, J.F.; Shneider, B.L. The Fecal Microbiome in Infants With Biliary Atresia Associates With Bile Flow After Kasai Portoenterostomy. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Han, M.; Heinrich, B.; Fu, Q.; Zhang, Q.; Sandhu, M.; Agdashian, D.; Terabe, M.; Berzofsky, J.A.; Fako, V.; et al. Gut microbiome-mediated bile acid metabolism regulates liver cancer via NKT cells. Science 2018, 360, eaan5931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albillos, A.; de Gottardi, A.; Rescigno, M. The gut-liver axis in liver disease: Pathophysiological basis for therapy. J. Hepatol. 2020, 72, 558–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krogsgaard, L.R.; Munck, L.K.; Bytzer, P.; Wildt, S. An altered composition of the microbiome in microscopic colitis is driven towards the composition in healthy controls by treatment with budesonide. Scand. J. Gastroenterol. 2019, 54, 446–452. [Google Scholar] [CrossRef] [PubMed]
- Nunez, G.J.; Johnstone, T.B.; Corpuz, M.L.; Kazarian, A.G.; Mohajer, N.N.; Tliba, O. Glucocorticoids rapidly activate cAMP production via G αs to initiate non-genomic signaling that contributes to one-third of their canonical genomic effects. FASEB J. 2020, 34, 2882–2895. [Google Scholar] [CrossRef] [Green Version]
- Zimmermann, C.; van Waterschoot, R.A.B.; Harmsen, S.; Maier, A.; Gutmann, H.; Schinkel, A.H. PXR-mediated induction of human CYP3A4 and mouse Cyp3a11 by the glucocorticoid budesonide. Eur. J. Pharm. Sci. 2009, 36, 565–571. [Google Scholar] [CrossRef]
- Goldsetin, J.; Levy, C. Novel and emerging therapies for cholestatic liver diseases. Liver Int. 2018, 38, 1520–1535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dindia, L.; Murray, J.; Faught, E.; Davis, T.L.; Leonenko, Z.; Vijayan, M.M. Novel nongenomic signaling by glucocorticoid may involve changes to liver membrane order in rainbow trout. PLoS ONE 2012, 7, e46859. [Google Scholar]
- Alonso, E.M.; Ye, W.; Hawthorne, K.; Venkat, V.; Loomes, K.M.; Mack, C.L.; Hertel, P.M.; Karpen, S.J.; Kerkar, N.; Molleston, J.P.; et al. Impact of Steroid Therapy on Early Growth in Infants with Biliary Atresia: The Multicenter Steroids in Biliary Atresia Randomized Trial. J. Pediatr. 2018, 202, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Tamura, T.; Kobayashi, H.; Yamataka, A.; Lane, G.J.; Koga, H.; Miyano, T. Inchin-ko-to prevents medium-term liver fibrosis in postoperative biliary atresia patients. Pediatr. Surg. Int. 2007, 23, 343–347. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study/ Control Group | SOA | p-Value n.s. | SNL | p-Value n.s. | jfSNL | p-Value | |
|---|---|---|---|---|---|---|---|
| 6 months post KPE N = 176 | SG | 99% (94/95) | n.s. | 78% (74/95) | n.s. | 55% (52/95) | n.s. |
| CG | 100% (81/81) | 73% (60/81) | 35% (29/81) | ||||
| 2 years post KPE N = 176 | SG | 92% (87/95) | n.s. | 54% (51/95) | p < 0.001 | 45% (43/95) | p < 0.001 |
| CG | 88% (73/81) | 32% (26/81) | 28% (23/81) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuebler, J.F.; Madadi-Sanjani, O.; Pfister, E.D.; Baumann, U.; Fortmann, D.; Leonhardt, J.; Ure, B.M.; Manns, M.P.; Taubert, R.; Petersen, C. Adjuvant Therapy with Budesonide Post-Kasai Reduces the Need for Liver Transplantation in Biliary Atresia. J. Clin. Med. 2021, 10, 5758. https://doi.org/10.3390/jcm10245758
Kuebler JF, Madadi-Sanjani O, Pfister ED, Baumann U, Fortmann D, Leonhardt J, Ure BM, Manns MP, Taubert R, Petersen C. Adjuvant Therapy with Budesonide Post-Kasai Reduces the Need for Liver Transplantation in Biliary Atresia. Journal of Clinical Medicine. 2021; 10(24):5758. https://doi.org/10.3390/jcm10245758
Chicago/Turabian StyleKuebler, Joachim F., Omid Madadi-Sanjani, Eva D. Pfister, Ulrich Baumann, David Fortmann, Johannes Leonhardt, Benno M. Ure, Michael P. Manns, Richard Taubert, and Claus Petersen. 2021. "Adjuvant Therapy with Budesonide Post-Kasai Reduces the Need for Liver Transplantation in Biliary Atresia" Journal of Clinical Medicine 10, no. 24: 5758. https://doi.org/10.3390/jcm10245758