
Myocardial Injury in Hospitalized Patients with Myasthenia Gravis
 ,
,
Abstract
:1. Introduction
2. Methods
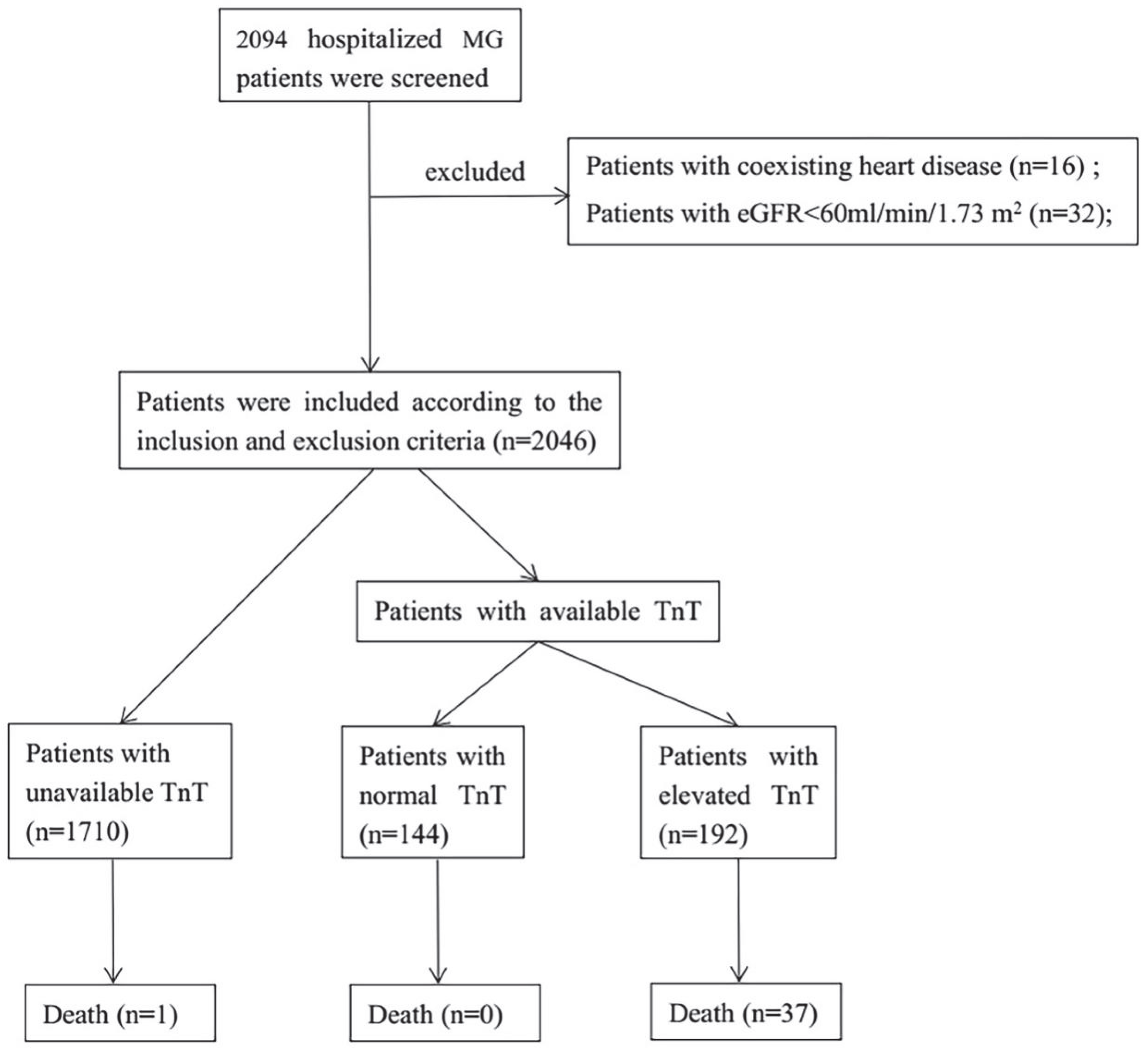
2.1. Study Design and Patient Selection
2.2. Data Acquisition
2.3. Statistical Analyses
3. Results
3.1. Baseline Characteristics
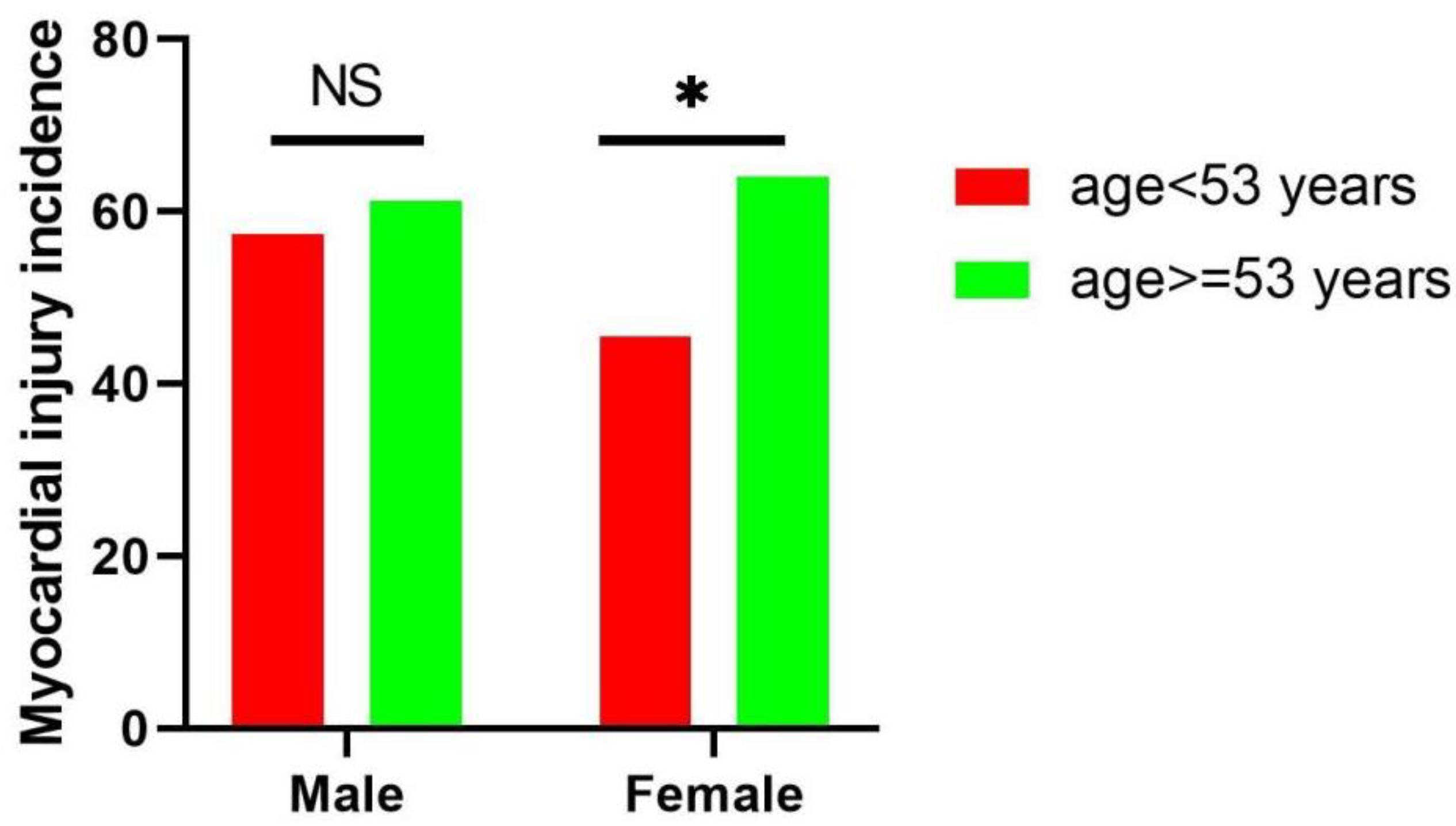
3.2. Myocardial Injury Examinations of Patients with MG
3.3. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gilhus, N.E. Myasthenia Gravis. N. Engl. J. Med. 2016, 375, 2570–2581. [Google Scholar] [CrossRef] [PubMed]
- Peric, S.; Rakocevic-Stojanovic, V.; Nisic, T.; Pavlovic, S.; Basta, I.; Popovic, S.; Damjanovic, S.; Lavrnic, D. Cardiac autonomic control in patients with myasthenia gravis and thymoma. J. Neurol. Sci. 2011, 307, 30–33. [Google Scholar] [CrossRef]
- Rzepiński, Ł.; Zawadka-Kunikowska, M.; Newton, J.; Zalewski, P. Cardiac Autonomic Dysfunction in Myasthenia Gravis and Relapsing-Remitting Multiple Sclerosis—A Pilot Study. J. Clin. Med. 2021, 10, 2173. [Google Scholar] [CrossRef] [PubMed]
- Zawadka-Kunikowska, M.; Rzepiński, Ł.; Tafil-Klawe, M.; Klawe, J.J.; Zalewski, P.; Słomko, J. Association of Cardiac Autonomic Responses with Clinical Outcomes of Myasthenia Gravis: Short-Term Analysis of the Heart-Rate and Blood Pressure Variability. J. Clin. Med. 2022, 11, 3697. [Google Scholar] [CrossRef] [PubMed]
- Cheng, W.; Sun, T.; Liu, C.; Zhou, Z.; Duan, J.; Zhao, Y.; Yang, M.; Chen, P. Author response for “A systematic review of myasthenia gravis complicated with myocarditis”. Brain Behav. 2021, 11, e2242. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A. Fourth Universal Definition of Myocardial Infarction. Circulation 2018, 138, e618–e651. [Google Scholar] [CrossRef]
- Ammirati, E.; Frigerio, M.; Adler, E.D.; Basso, C.; Birnie, D.H.; Brambatti, M. Management of Acute Myocarditis and Chronic Inflammatory Cardiomyopathy: An Expert Consensus Document. Circ. Heart Fail. 2020, 13, e007405. [Google Scholar] [CrossRef]
- Yin, Y.J.; Zeng, S.L.; Li, Y.W.; Wu, Z.; Huang, D.J.; Tang, H.Z. The effect of coenzyme Q10 plus trimetazidine on acute viral myocarditis treatment. Am. J. Transl. Res. 2021, 13, 13854–13861. [Google Scholar]
- du Fay de Lavallaz, J.; Prepoudis, A.; Wendebourg, M.J.; Kesenheimer, E.; Kyburz, D.; Daikeler, T.; Haaf, P.; Wanschitz, J.; Löscher, W.N.; Schreiner, B.; et al. Skeletal Muscle Disorders: A Non-cardiac Source of Cardiac Troponin T. Circulation 2022, 145, 1764–1779. [Google Scholar] [CrossRef]
- Thygesen, K.; Mair, J.; Giannitsis, E.; Mueller, C.; Lindahl, B.; Blankenberg, S.; Huber, K.; Plebani, M.; Biasucci, L.M.; Tubaro, M.; et al. How to use high-sensitivity cardiac troponins in acute cardiac care. Eur. Heart J. 2012, 33, 2252–2257. [Google Scholar] [CrossRef] [Green Version]
- Giustino, G.; Croft, L.B.; Stefanini, G.G.; Bragato, R.; Silbiger, J.J.; Vicenzi, M.; Danilov, T.; Kukar, N.; Shaban, N.; Kini, A.; et al. Characterization of Myocardial Injury in Patients With COVID-19. J. Am. Coll. Cardiol. 2020, 76, 2043–2055. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Utsugisawa, K.; Yoshikawa, H.; Motomura, M.; Matsubara, S.; Yokoyama, K.; Nagane, Y.; Maruta, T.; Satoh, T.; Sato, H.; et al. Autoimmune Targets of Heart and Skeletal Muscles in Myasthenia Gravis. Arch. Neurol. 2009, 66, 1334–1338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, E.; Coutinho, E.; da Silva, A.M.; Marinho, A.; Vasconcelos, C.; Taipa, R.; Pires, M.M.; Gonçalves, G.; Lopes, C.; Leite, M.I. Inflammatory myopathy associated with myasthenia gravis with and without thymic pathology: Report of four cases and literature review. Autoimmun. Rev. 2017, 16, 644–649. [Google Scholar] [CrossRef]
- Suzuki, S.; Utsugisawa, K.; Nagane, Y.; Suzuki, N. Three Types of Striational Antibodies in Myasthenia Gravis. Autoimmune Dis. 2011, 2011, 740583. [Google Scholar] [CrossRef] [Green Version]
- Grandi, E.; Sanguinetti, M.C.; Bartos, D.C.; Bers, D.M.; Chen-Izu, Y.; Chiamvimonvat, N.; Colecraft, H.M.; Delisle, B.P.; Heijman, J.; Navedo, M.F.; et al. Potassium channels in the heart: Structure, function and regulation. J. Physiol. 2016, 595, 2209–2228. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, S.; Baba, A.; Kaida, K.; Utsugisawa, K.; Kita, Y.; Tsugawa, J.; Ogawa, G.; Nagane, Y.; Kuwana, M.; Suzuki, N. Cardiac involvements in myasthenia gravis associated with anti-Kv1.4 antibodies. Eur. J. Neurol. 2013, 21, 223–230. [Google Scholar] [CrossRef]
- Álvarez-Velasco, R.; Gutiérrez-Gutiérrez, G.; Trujillo, J.C.; Martínez, E.; Segovia, S.; Arribas-Velasco, M. Clinical characteristics and outcomes of thymoma-associated myasthenia gravis. Eur. J. Neurol. 2021, 28, 2083–2091. [Google Scholar] [CrossRef]
- Westerberg, E.; Punga, A.R. Mortality rates and causes of death in Swedish Myasthenia Gravis patients. Neuromuscul. Disord. 2020, 30, 815–824. [Google Scholar] [CrossRef]
- Neumann, B.; Angstwurm, K.; Mergenthaler, P.; Kohler, S.; Schönenberger, S.; Bösel, J. Myasthenic crisis demanding mechanical ventilation: A multicenter analysis of 250 cases. Neurology 2020, 94, e299–e313. [Google Scholar] [CrossRef]
- Tschöpe, C.; Ammirati, E.; Bozkurt, B.; Caforio, A.L.P.; Cooper, L.T.; Felix, S.B.; Hare, J.M.; Heidecker, B.; Heymans, S.; Hübner, N.; et al. Myocarditis and inflammatory cardiomyopathy: Current evidence and future directions. Nat. Rev. Cardiol. 2020, 18, 169–193. [Google Scholar] [CrossRef] [PubMed]
- Desai, R.; Abbas, S.A.; Fong, H.K.; Lodhi, M.U.; Doshi, R.; Savani, S.; Gangani, K.; Sachdeva, R.; Kumar, G. Burden and impact of takotsubo syndrome in myasthenic crisis: A national inpatient perspective on the under-recognized but potentially fatal association. Int. J. Cardiol. 2019, 299, 63–66. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male | p Value | Female | p Value | |||
|---|---|---|---|---|---|---|
| Normal TnT | Elevated TnT | Normal TnT | Elevated TnT | |||
| Number | 60 | 88 | 84 | 104 | ||
| Age, mean (SD), years | 51.9 (16.6) | 54.7 (17.1) | 0.324 | 49.2 (17.2) | 56.0 (16.6) | 0.007 |
| Infection, n (%) | 18 (30) | 50 (56.8) | 0.001 | 27 (32.1) | 68 (65.4) | <0.001 |
| Myasthenic crisis, n (%) | 8 (13.3) | 33 (37.5) | 0.001 | 15 (17.9) | 35 (33.6) | 0.015 |
| Classification | ||||||
| Available, n | 59 | 86 | 83 | 100 | ||
| Generalized MG, n (%) | 42 (71.2) | 71 (82.6) | 0.105 | 68 (81.9) | 91 (91.0) | 0.070 |
| Ocular MG, n (%) | 17 (28.8) | 15 (17.4) | 15 (18.1) | 9 (9.0) | ||
| Thymoma, n (%) | 17 (28.3) | 30 (34.1) | 0.460 | 14 (16.7) | 40 (38.5) | 0.001 |
| Atrial fibrillation | 0 | 1 (1.1) | 0.407 | 0 | 4 (3.9) | 0.069 |
| ICI therapy, n (%) | 1 (1.7) | 3 (3.4) | 0.521 | 0 | 3 (2.9) | 0.117 |
| Outcome | ||||||
| Death, n (%) | 0 | 21 (23.9) | <0.001 | 0 | 16 (15.4) | <0.001 |
| Male | p Value | Female | p Value | |||
|---|---|---|---|---|---|---|
| Normal TnT | Elevated TnT | Normal TnT | Elevated TnT | |||
| LAD | 31.8 (4.8) | 31.1 (6.9) | 0.618 | 29.4 (7.4) | 28.4 (9.3) | 0.579 |
| LVEDD | 46.1 (3.6) | 46.6 (3.7) | 0.591 | 44.6 (3.2) | 42.9 (3.4) | 0.017 |
| RVEDD | 20.7 (4.3) | 20.6 (4.3) | 0.916 | 19.3 (4.7) | 18.9 (3.6) | 0.678 |
| RAD | 32.5 (6.7) | 30.9 (8.6) | 0.394 | 28.4 (10.6) | 28.7 (10.3) | 0.902 |
| IVS | 10.2 (2.7) | 10.5 (2.4) | 0.664 | 8.9 (2.1) | 9.7 (3.4) | 0.219 |
| LVPW | 8.8 (1.9) | 8.8 (2.3) | 0.999 | 7.8 (2.2) | 8.4 (2.7) | 0.269 |
| LVEF | 67.0 (5.5) | 65.7 (8.6) | 0.462 | 64.6 (14.6) | 68.2 (4.2) | 0.127 |
| Unadjusted | Adjusted | |||
|---|---|---|---|---|
| Coefficient (95% CI) | p | Coefficient (95% CI) | p | |
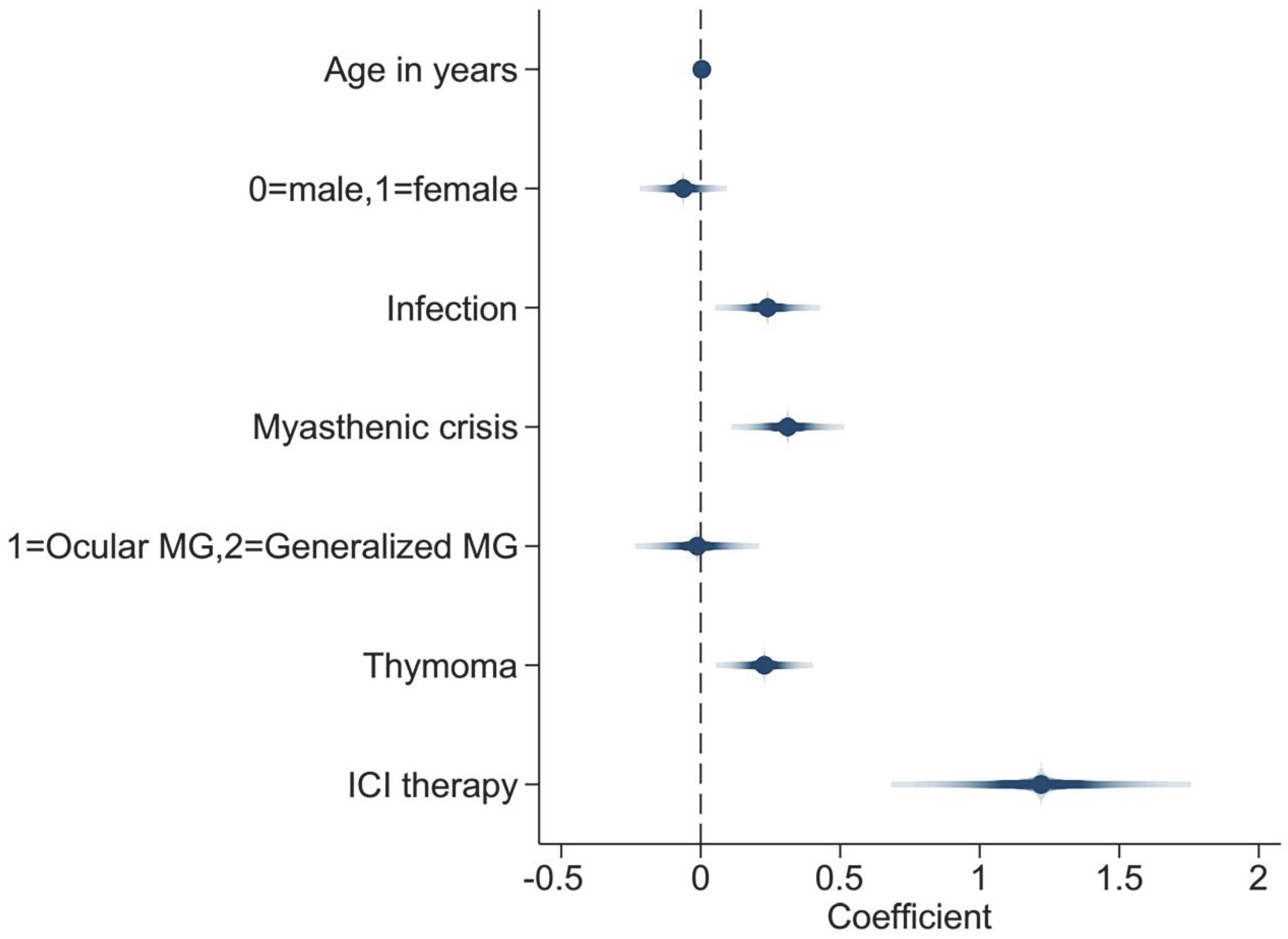
| Age | 0.004 (0.000, 0.008) | 0.029 | 0.004 (0.000, 0.007) | 0.034 |
| Female | −0.073 (−0.206, 0.059) | 0.278 | −0.063 (−0.182, 0.056) | 0.301 |
| Infection | 0.371 (0.245, 0.497) | <0.001 | 0.240 (0.097, 0.382) | 0.001 |
| Myasthenic crisis | 0.453 (0.312, 0.593) | <0.001 | 0.312 (0.158, 0.466) | <0.001 |
| Generalized MG | 0.249 (0.072, 0.425) | 0.006 | −0.012 (−0.181, 0.158) | 0.888 |
| Thymoma | 0.206 (0.064, 0.348) | 0.005 | 0.228 (0.097, 0.360) | 0.001 |
| ICI therapy | 1.218 (0.775, 1.662) | <0.001 | 1.220 (0.812, 1.628) | <0.001 |
| Dead Patients | Surviving Patients | p | |
|---|---|---|---|
| Number | 37 | 299 | -- |
| Female, n (%) | 16 (43.2) | 172 (57.5) | 0.099 |
| Age, mean(SD), years | 58.2 (16.0) | 52.6 (17.1) | 0.060 |
| Infection, n (%) | 34 (91.9) | 129 (43.1) | <0.001 |
| Thymoma, n (%) | 19 (51.4) | 82 (27.4) | 0.003 |
| ICI therapy, n (%) | 2 (5.4) | 5 (1.7) | 0.134 |
| Myasthenic crisis, n (%) | 37 (100.0) | 54 (18.1) | <0.001 |
| Classification | |||
| Available, n | 37 | 291 | -- |
| Generalized MG, n (%) | 37 (100.0) | 235 (80.8) | 0.003 |
| Ocular MG, n (%) | 0 | 56 (19.2) | -- |
| Unadjusted | Adjusted | |||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p | |
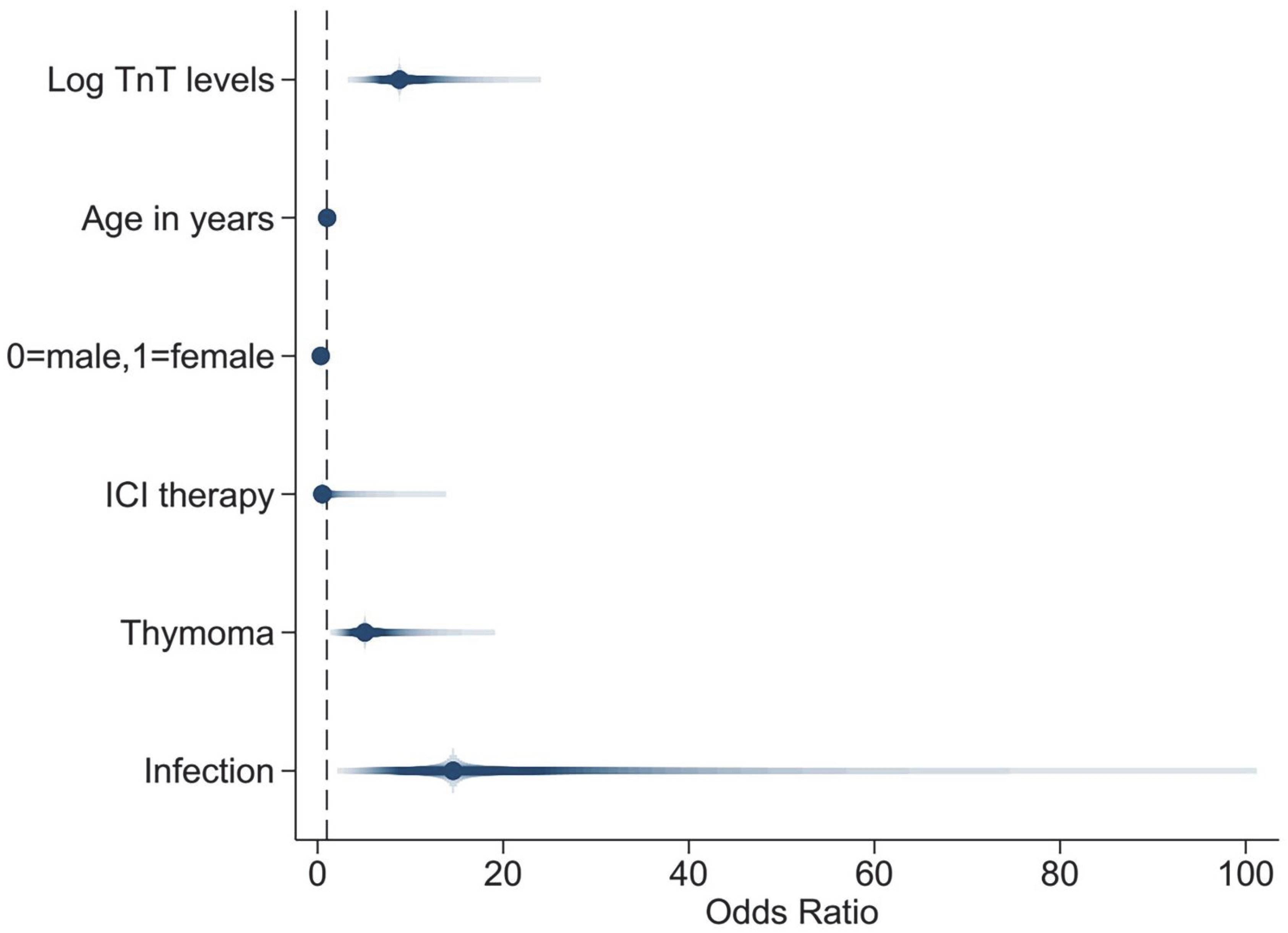
| Log TnT levels | 7.928 (4.388, 14.325) | <0.001 | 8.818 (4.107, 18.934) | <0.001 |
| Age | 1.020 (0.999, 1.042) | 0.062 | 1.028 (0.994, 1.063) | 0.112 |
| Female | 0.562 (0.282, 1.121) | 0.102 | 0.346 (0.139, 0.862) | 0.023 |
| ICI therapy | 3.360 (0.628, 17.972) | 0.157 | 0.514 (0.042, 6.308) | 0.603 |
| Thymoma | 2.793 (1.397, 5.585) | 0.004 | 5.092 (1.861, 13.938) | 0.002 |
| Infection | 14.935 (4.488, 49.708) | <0.001 | 14.597 (3.345, 63.700) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, H.; Kong, L.; Zhang, Y.; Lin, X.; Shi, Z.; Du, Q.; Wang, X.; Lang, Y.; Cai, L.; Mou, Z.; et al. Myocardial Injury in Hospitalized Patients with Myasthenia Gravis. J. Clin. Med. 2022, 11, 7106. https://doi.org/10.3390/jcm11237106
Chen H, Kong L, Zhang Y, Lin X, Shi Z, Du Q, Wang X, Lang Y, Cai L, Mou Z, et al. Myocardial Injury in Hospitalized Patients with Myasthenia Gravis. Journal of Clinical Medicine. 2022; 11(23):7106. https://doi.org/10.3390/jcm11237106
Chicago/Turabian StyleChen, Hongxi, Lingyao Kong, Ying Zhang, Xue Lin, Ziyan Shi, Qin Du, Xiaofei Wang, Yanlin Lang, Linjun Cai, Zichao Mou, and et al. 2022. "Myocardial Injury in Hospitalized Patients with Myasthenia Gravis" Journal of Clinical Medicine 11, no. 23: 7106. https://doi.org/10.3390/jcm11237106