
New Targeted Agents in Myasthenia Gravis and Future Therapeutic Strategies
 , , ,
, , ,
Abstract
:1. Introduction
2. Pathophysiology of Myasthenia Gravis
3. New Therapeutic Strategies in Myasthenia Gravis
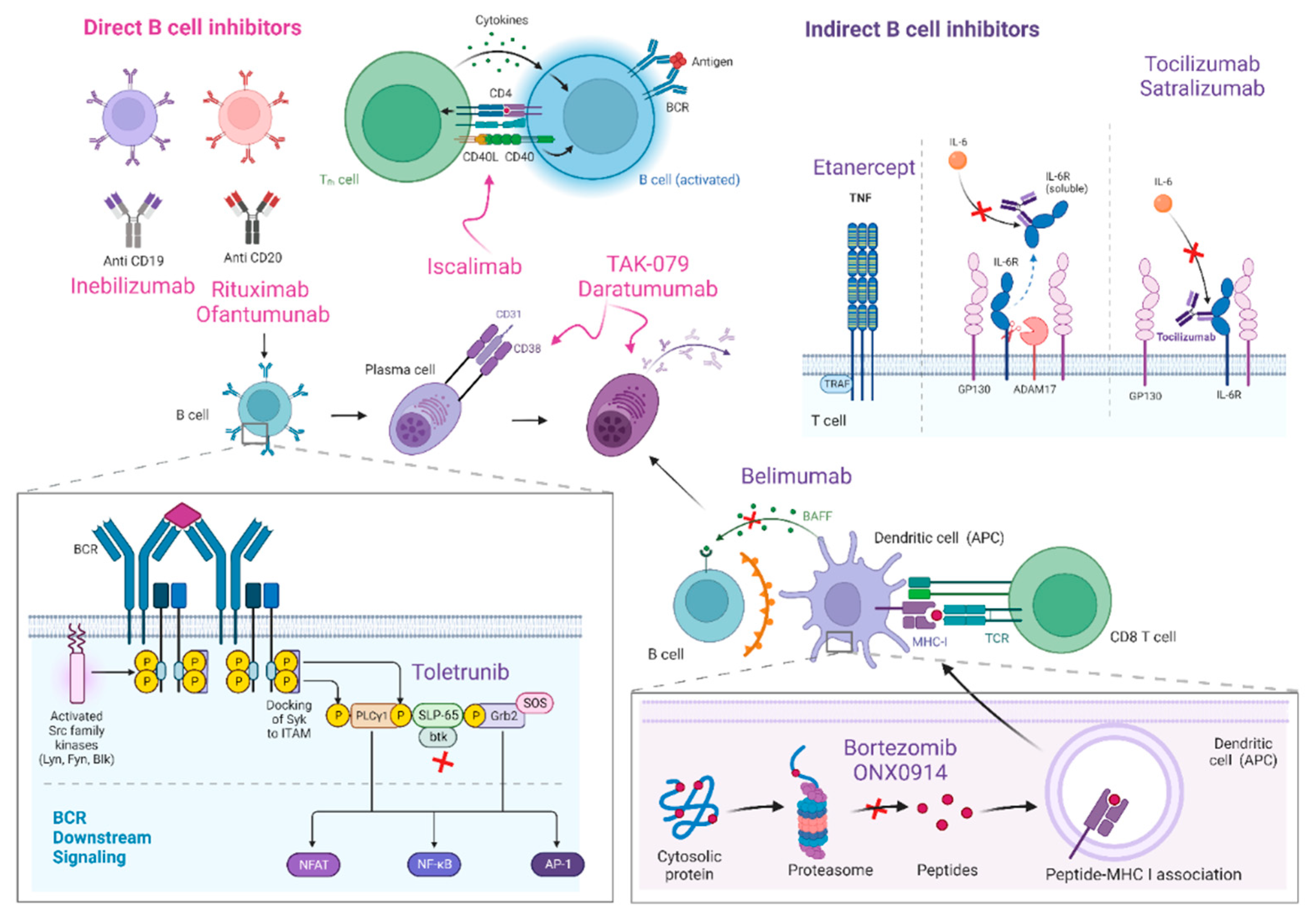
3.1. B-Cell Inhibitors
3.1.1. Direct B-Cell Inhibitors
- Rituximab (RTX)
- 2.
- Other B-cell inhibitors
- 3.
- Drugs targeting plasma cells
- Proteasome inhibitors
- b.
- Biologic drugs targeting plasma cells

3.1.2. Indirect B-Cell Inhibitors
- Cytokines, interleukins, and other immune mediators
- 2.
- B-cell-activating factor
- 3.
- Bruton’s tyrosine kinase
3.2. Complement Inhibitors
- Eculizumab
- 2.
- Ravulizumab
- 3.
- Zilucoplan

3.3. FcRn Inhibitors
3.3.1. Efgartigimod
3.3.2. Rozanolixizumab
3.3.3. Nipocalimab
3.3.4. Batoclimab
3.3.5. Other FcRn Antagonists and Related Drugs

4. Discussion and Conclusions

{kind=link}
{kind=link}
{kind=link}
| Drug | Target | Product | Type of Study † | MG Population | Study Code | Results ђ | Reference φ |
|---|---|---|---|---|---|---|---|
| B-cell inhibitors | |||||||
| Direct B-cell inhibitors | |||||||
| Rituximab | CD20 | Murine-human chimeric IgG1k mAb | Phase 2 Phase 3 Non-randomized observational | AChR-MG AChR and seronegative MG MuSK-MG and AChR-MG | NCT02110706 NCT02950155 | Controversial in AChR-MG Positive in AChR-MG, single dose of 500 mg rituximab Positive in MuSK-MG | Nowak et al., 2022 [46] Piehl et al., 2022 [47] Beecher et al., 2018: Topakian et al., 2019; Dos Santos et al., 2020; Brauner et al., 2020; Choi et al. 2019; Lu et al., 2020; Li et al., 2021; Hehir et al. 2017; Cortés-Vicente et al. 2018 [34,35,36,37,38,39,40,41,42,44]. |
| Ofatumumab | CD20 | Fully human IgG1k mAb | Non-randomized, single case report | AChR-MG, refractory, previously treated with rituximab | NA | Not applicable | Waters et al., 2019 [52] |
| Inebilizumab | CD19 | Humanized, afucosylated IgG1k mAb | Phase 3 | AChR-gMG | NCT04524273 | Pending | ct.gov [55] |
| Iscalimab (CFZ533) | CD145-CD40 | Fully human, Fc-silenced, IgG1 mAb | Phase 3 | AChR-gMG | NCT02565576 | Pending | ct.gov [57] |
| Drugs targeting plasma cells | |||||||
| Proteasome inhibitors | |||||||
| Bortezomib | Proteasome | Non-randomized clinical trial | Antibody-mediated AIDs, including MG | NA | Not completed, neurotoxicity | Kohler et al., 2019 [60] | |
| ONX0914 | Proteasome | Pre-clinical | EAMG models only | NA | Positive | Liu et al., 2017 [62] | |
| Biologic drugs against plasma-cells | |||||||
| Mezagitamab (TAK-079) | CD38 | Phase 2 | AChR-gMG MuSK-MG | NCT04159805/EudraCT:2019-003383-47 | Pending | ct.gov [65] | |
| Daratumumab | CD38 | Human IgG1k mAb | Non-randomized, retrospective, single-centre study | n = 7, 1 MG | NA | Positive | Scheibe et al., 2022 [66] |
| Indirect B-cell inhibitors | |||||||
| Tocilizumab | IL-6 | Phase 2 | AChR-gMG | NCT05067348 | Pending start | ct.gov [70] | |
| Satralizumab | IL-6 | Phase 3 | AChR-gMG | NCT04963270 | Pending, recruiting | ct.gov [71] | |
| Etanercept | TNF | Non-randomized, prospective (pilot) | AChR-gMG, corticosteroid-dependent | NA | Controversial, toxicity | Pelechas et al., 2020 [72] | |
| Belimumab | BAFF | Phase 2 | AChR- gMG | NCT01480596 | Negative | Hewett et al. 2018 [76] | |
| Tolebrutinib | BTK | Phase 3 | AChR- gMG | NCT05132569/EudraCT: 2021-003898 | Pending, halted recruitment | ct.gov [80] | |
| Complement inhibitors | |||||||
| Eculizumab | C5 | Phase 3 and OLE | AChR-gMG, refractory | NCT01997229 and NCT02301624 | Approved for the treatment of refractory anti-AChR+ gMG (Solaris®) Phase 3: 900 mg intravenous on days 1 and at weeks 1, 2, and 3, followed by 1200 mg at week 4 and 1200 mg every 2 weeks as a maintenance dose. Primary endpoint not met (change in MG-ADL from baseline to week 26). Significant differences in secondary endpoints (changes in QMG, MG Composite, and MG-QOL15 scores). OLE: all patients received eculizumab maintenance therapy (1200 mg every 2 weeks), 90% patients improved, 60% remission | Howard et al., 2017 [89] | |
| Ravulizumab | C5 | Phase 3 | AChR-gMG | NCT03920293 | Positive Patients receive a loading dose on day 1, followed by maintenance doses on day 15 and every 8 weeks thereafter. Loading dose: 40 to <60 kg: 2400 mg IV; 60 to <100 kg: 2700 mg IV; ≥100 kg: 3000 mg IV Maintenance IV dose: 40 to <60 kg: 3000 mg IV; Q8W; 60 to <100 kg: 3300 mg IV Q8W; ≥100 kg: 3600 mg IV Q8W | Tuan et al., 2022 [94] | |
| Zilucoplan | C5 | Phase 3 | AChR-gMG | NCT04115293 | Pending phase 3 results, preliminary positive (press release) | ct.gov [96] | |
| FcRn inhibitors | |||||||
| Efgartigimod | FcRn | Human FcRn mAb | Phase 3 | AChR-gMG MuSK-MG | NCT04735432 | Approved in the US and Europe for the treatment anti-AChR+ gMG (Vyvgart®). 68% MG-ADL responders and 34% MG-ADL 0-1 (minimal symptom) by the end of first in the first treatment cycle. Higher MG-ADL early-responder (2 weeks) proportion vs placebo group. Improvement in QMG, MGC, MG-QoL15 at 7 weeks after first infusion. | Howard et al., 2021 [105] |
| Rozanolixizumab | FcRn | Humanized, high-affinity, human IgG4 anti-FcRn mAb | Phase 3 | AChR-gMG MuSK-MG | NCT04124965 | Pending publication phase 3, positive results (press release) Primary and all secondary endpoints with statistical significance and no safety or tolerance concerns | Bril et al., 2021 [112] |
| Nipocalimab (M281) | FcRn | Fully human alpha-deglycosylated IgG1 anti-FcRn mAb | Phase 3 | AChR-gMG MuSK-MG | NCT04951622 | Positive phase 2, pending phase 3 results | ct.gov [117] |
| Batoclimab (RVT-1401 or HL161) | FcRn | Human recombinant anti-FcRn mAb | Phase 3 | AChR-gMG MuSK-MG | NCT05403541 | Pending phase 3, recruiting | ct.gov [121] |
| Oralinomab (SYNT001 or ALX1830) | FcRn | Human recombinant IgG4 anti-FcRn mAb | No trials in MG | NA | Phase 1/2 in wAIHA (NCT03075878) and chronic pemphigus (NCT03075904) | Not applicable to MG | ct.gov [123]; Werth et al., 2021 [124] |
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Jaretzki, A.; Barohn, R.J.; Ernstoff, R.M.; Kaminski, H.J.; Keesey, J.C.; Penn, A.S.; Sanders, D.B. Myasthenia Gravis: Recommendations for Clinical Research Standards. Neurology 2000, 55, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Narayanaswami, P.; Sanders, D.B.; Wolfe, G.; Benatar, M.; Cea, G.; Evoli, A.; Gilhus, N.E.; Illa, I.; Kuntz, N.L.; Massey, J.; et al. International Consensus Guidance for Management of Myasthenia Gravis: 2020 Update. Neurology 2021, 96, 114–122. [Google Scholar] [CrossRef]
- Law, C.; Flaherty, C.V.; Bandyopadhyay, S. A Review of Psychiatric Comorbidity in Myasthenia Gravis. Cureus 2020, 12, e9184. [Google Scholar] [CrossRef] [PubMed]
- Cutter, G.; Xin, H.; Aban, I.; Burns, T.M.; Allman, P.H.; Farzaneh-Far, R.; Duda, P.W.; Kaminski, H.J. Cross-Sectional Analysis of the Myasthenia Gravis Patient Registry: Disability and Treatment. Muscle Nerve 2019, 60, 707–715. [Google Scholar] [CrossRef] [PubMed]
- Bacci, E.D.; Coyne, K.S.; Poon, J.L.; Harris, L.; Boscoe, A.N. Understanding Side Effects of Therapy for Myasthenia Gravis and Their Impact on Daily Life. BMC Neurol. 2019, 19, 335. [Google Scholar] [CrossRef]
- Berrih-Aknin, S.; Claeys, K.G.; Law, N.; Mantegazza, R.; Murai, H.; Saccà, F.; Dewilde, S.; Janssen, M.F.; Bagshaw, E.; Kousoulakou, H.; et al. Patient-Reportedimpact of Myasthenia Gravis in the Real World: Protocol for a Digital Observational Study (MyRealWorld MG). BMJ Open 2021, 11, e048198. [Google Scholar] [CrossRef]
- Law, N.; Davio, K.; Blunck, M.; Lobban, D.; Seddik, K. The Lived Experience of Myasthenia Gravis: A Patient-Led Analysis. Neurol. Ther. 2021, 10, 1103–1125. [Google Scholar] [CrossRef] [PubMed]
- Gelinas, D.; Parvin-Nejad, S.; Phillips, G.; Cole, C.; Hughes, T.; Silvestri, N.; Govindarajan, R.; Jefferson, M.; Campbell, J.; Burnett, H. The Humanistic Burden of Myasthenia Gravis: A Systematic Literature Review. J. Neurol. Sci. 2022, 437, 120268. [Google Scholar] [CrossRef]
- Yang, Y.; Zhang, M.; Guo, J.; Ma, S.; Fan, L.; Wang, X.; Li, C.; Guo, P.; Wang, J.; Li, H.; et al. Quality of Life in 188 Patients with Myasthenia Gravis in China. Int. J. Neurosci. 2016, 126, 455–462. [Google Scholar] [CrossRef]
- Blum, S.; Lee, D.; Gillis, D.; McEniery, D.F.; Reddel, S.; McCombe, P. Clinical Features and Impact of Myasthenia Gravis Disease in Australian Patients. J. Clin. Neurosci. 2015, 22, 1164–1169. [Google Scholar] [CrossRef]
- Schneider-Gold, C.; Hagenacker, T.; Melzer, N.; Ruck, T. Understanding the Burden of Refractory Myasthenia Gravis. Ther. Adv. Neurol. Disord. 2019, 12, 1756286419832242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xin, H.; Harris, L.A.; Aban, I.B.; Cutter, G. Examining the Impact of Refractory Myasthenia Gravis on Healthcare Resource Utilization in the United States: Analysis of a Myasthenia Gravis Foundation of America Patient Registry Sample. J. Clin. Neurol. 2019, 15, 376–385. [Google Scholar] [CrossRef]
- Salvado, M.; Caro, J.L.; Garcia, C.; Rudilla, F.; Zalba-Jadraque, L.; Lopez, E.; Sanjuan, E.; Gamez, J.; Vidal-Taboada, J.M. HLA-DQB1*05:02, *05:03, and *03:01 Alleles as Risk Factors for Myasthenia Gravis in a Spanish Cohort. Neurol. Sci. 2022, 43, 5057–5065. [Google Scholar] [CrossRef] [PubMed]
- Dalakas, M.C. Immunotherapy in Myasthenia Gravis in the Era of Biologics. Nat. Rev. Neurol. 2019, 15, 113–124. [Google Scholar] [CrossRef] [PubMed]
- Thiruppathi, M.; Rowin, J.; Li Jiang, Q.; Sheng, J.R.; Prabhakar, B.S.; Meriggioli, M.N. Functional Defect in Regulatory T Cells in Myasthenia Gravis. Ann. N. Y. Acad. Sci. 2012, 1274, 68–76. [Google Scholar] [CrossRef] [Green Version]
- Dominguez-Villar, M.; Hafler, D.A. Regulatory T Cells in Autoimmune Disease. Nat. Immunol. 2018, 19, 665–673. [Google Scholar] [CrossRef]
- Sudres, M.; Verdier, J.; Truffault, F.; Le Panse, R.; Berrih-Aknin, S. Pathophysiological Mechanisms of Autoimmunity. Ann. N. Y. Acad. Sci. 2018, 1413, 59–68. [Google Scholar] [CrossRef]
- Berrih-Aknin, S.; Le Panse, R. Myasthenia Gravis: A Comprehensive Review of Immune Dysregulation and Etiological Mechanisms. J. Autoimmun. 2014, 52, 90–100. [Google Scholar] [CrossRef]
- Meriggioli, M.N.; Sanders, D.B. Muscle Autoantibodies in Myasthenia Gravis: Beyond Diagnosis? Expert Rev. Clin. Immunol. 2012, 8, 427–438. [Google Scholar] [CrossRef] [Green Version]
- Gilhus, N.E.; Tzartos, S.; Evoli, A.; Palace, J.; Burns, T.M.; Verschuuren, J.J.G.M. Myasthenia Gravis. Nat. Rev. Dis. Prim. 2019, 5, 30. [Google Scholar] [CrossRef]
- Leite, M.I.; Jacob, S.; Viegas, S.; Cossins, J.; Clover, L.; Morgan, B.P.; Beeson, D.; Willcox, N.; Vincent, A. IgG1 Antibodies to Acetylcholine Receptors in “seronegative” Myasthenia Gravis. Brain 2008, 131, 1940–1952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacob, S.; Viegas, S.; Leite, M.I.; Webster, R.; Cossins, J.; Kennett, R.; Hilton-Jones, D.; Morgan, B.P.; Vincent, A. Presence and Pathogenic Relevance of Antibodies to Clustered Acetylcholine Receptor in Ocular and Generalized Myasthenia Gravis. Arch. Neurol. 2012, 69, 994–1001. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, S.; Harms, L.; Schuelke, M.; Rückert, J.C.; Goebel, H.H.; Stenzel, W.; Meisel, A. Complement Deposition at the Neuromuscular Junction in Seronegative Myasthenia Gravis. Acta Neuropathol. 2020, 139, 1119–1122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koneczny, I.; Herbst, R. Myasthenia Gravis: Pathogenic Effects of Autoantibodies on Neuromuscular Architecture. Cells 2019, 8, 671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takamori, M. Myasthenia Gravis: From the Viewpoint of Pathogenicity Focusing on Acetylcholine Receptor Clustering, Trans-Synaptic Homeostasis and Synaptic Stability. Front. Mol. Neurosci. 2020, 13, 86. [Google Scholar] [CrossRef]
- Lazaridis, K.; Tzartos, S.J. Autoantibody Specificities in Myasthenia Gravis; Implications for Improved Diagnostics and Therapeutics. Front. Immunol. 2020, 11, 212. [Google Scholar] [CrossRef] [Green Version]
- Koneczny, I.; Cossins, J.; Waters, P.; Beeson, D.; Vincent, A. MuSK Myasthenia Gravis IgG4 Disrupts the Interaction of LRP4 with MuSK but Both IgG4 and IgG1-3 Can Disperse Preformed Agrin-Independent AChR Clusters. PLoS ONE 2013, 8, e80695. [Google Scholar] [CrossRef] [Green Version]
- Koneczny, I.; Stevens, J.A.A.; De Rosa, A.; Huda, S.; Huijbers, M.G.; Saxena, A.; Maestri, M.; Lazaridis, K.; Zisimopoulou, P.; Tzartos, S.; et al. IgG4 Autoantibodies against Muscle-Specific Kinase Undergo Fab-Arm Exchange in Myasthenia Gravis Patients. J. Autoimmun. 2017, 77, 104–115. [Google Scholar] [CrossRef]
- Dalakas, M.C. IgG4-Mediated Neurologic Autoimmunities: Understanding the Pathogenicity of IgG4, Ineffectiveness of IVIg, and Long-Lasting Benefits of Anti-B Cell Therapies. Neurol. Neuroimmunol. Neuroinflamm. 2022, 9. [Google Scholar] [CrossRef]
- Higuchi, O.; Hamuro, J.; Motomura, M.; Yamanashi, Y. Autoantibodies to Low-Density Lipoprotein Receptor-Related Protein 4 in Myasthenia Gravis. Ann. Neurol. 2011, 69, 418–422. [Google Scholar] [CrossRef]
- Yi, J.S.; Guptill, J.T.; Stathopoulos, P.; Nowak, R.J.; O’Connor, K.C. B Cells in the Pathophysiology of Myasthenia Gravis. Muscle Nerve 2018, 57, 172–184. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, K.; Clauder, A.K.; Manz, R.A. Targeting B Cells and Plasma Cells in Autoimmune Diseases. Front. Immunol. 2018, 9, 835. [Google Scholar] [CrossRef] [PubMed]
- Sellebjerg, F.; Blinkenberg, M.; Sorensen, P.S. Anti-CD20 Monoclonal Antibodies for Relapsing and Progressive Multiple Sclerosis. CNS Drugs 2020, 34, 269–280. [Google Scholar] [CrossRef]
- Lee, D.S.W.; Rojas, O.L.; Gommerman, J.L. B Cell Depletion Therapies in Autoimmune Disease: Advances and Mechanistic Insights. Nat. Rev. Drug Discov. 2021, 20, 179–199. [Google Scholar] [CrossRef]
- Dalakas, M.C. B Cells as Therapeutic Targets in Autoimmune Neurological Disorders. Nat. Clin. Pract. Neurol. 2008, 4, 557–567. [Google Scholar] [CrossRef] [PubMed]
- Leandro, M.J. B-Cell Subpopulations in Humans and Their Differential Susceptibility to Depletion with Anti-CD20 Monoclonal Antibodies. Arthritis Res. Ther. 2013, 15, S3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tandan, R.; Hehir, M.K.; Waheed, W.; Howard, D.B. Rituximab Treatment of Myasthenia Gravis: A Systematic Review. Muscle Nerve 2017, 56, 185–196. [Google Scholar] [CrossRef]
- Beecher, G.; Anderson, D.; Siddiqi, Z.A. Rituximab in Refractory Myasthenia Gravis: Extended Prospective Study Results. Muscle Nerve 2018, 58, 452–455. [Google Scholar] [CrossRef]
- Topakian, R.; Zimprich, F.; Iglseder, S.; Embacher, N.; Guger, M.; Stieglbauer, K.; Langenscheidt, D.; Rath, J.; Quasthoff, S.; Simschitz, P.; et al. High Efficacy of Rituximab for Myasthenia Gravis: A Comprehensive Nationwide Study in Austria. J. Neurol. 2019, 266, 699–706. [Google Scholar] [CrossRef]
- Nowak, R.; Coffey, C.; Goldstein, J.; Yankey, J.; Uribe, L.; Dimachkie, M.; Benatar, M.; Wolfe, G.; Burns, T.; O’Connor, K.; et al. Rituximab in Patients with Moderate to Severe Myasthenia Gravis: A Subgroup Analysis of the BeatMG Study. AANEM Annual Meeting Abstract Guide Austin, TX, October 16–19, 2019. Muscle Nerve 2019, 60, S139. [Google Scholar] [CrossRef]
- Dos Santos, A.; Noury, J.B.; Genestet, S.; Nadaj-Pakleza, A.; Cassereau, J.; Baron, C.; Videt, D.; Michel, L.; Pereon, Y.; Wiertlewski, S.; et al. Efficacy and Safety of Rituximab in Myasthenia Gravis: A French Multicentre Real-Life Study. Eur. J. Neurol. 2020, 27, 2277–2285. [Google Scholar] [CrossRef] [PubMed]
- Brauner, S.; Eriksson-Dufva, A.; Hietala, M.A.; Frisell, T.; Press, R.; Piehl, F. Comparison between Rituximab Treatment for New-Onset Generalized Myasthenia Gravis and Refractory Generalized Myasthenia Gravis. JAMA Neurol. 2020, 77, 974–981. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.; Hong, Y.H.; Ahn, S.H.; Baek, S.H.; Kim, J.S.; Shin, J.Y.; Sung, J.J. Repeated Low-Dose Rituximab Treatment Based on the Assessment of Circulating B Cells in Patients with Refractory Myasthenia Gravis. Ther. Adv. Neurol. Disord. 2019, 12, 1756286419871187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, J.; Zhong, H.; Jing, S.; Wang, L.; Xi, J.; Lu, J.; Zhou, L.; Zhao, C. Low-Dose Rituximab Every 6 Months for the Treatment of Acetylcholine Receptor–Positive Refractory Generalized Myasthenia Gravis. Muscle Nerve 2020, 61, 311–315. [Google Scholar] [CrossRef]
- Li, T.; Zhang, G.Q.; Li, Y.; Dong, S.A.; Wang, N.; Yi, M.; Qi, Y.; Zhai, H.; Yang, L.; Shi, F.D.; et al. Efficacy and Safety of Different Dosages of Rituximab for Refractory Generalized AChR Myasthenia Gravis: A Meta-Analysis. J. Clin. Neurosci. 2021, 85, 6–12. [Google Scholar] [CrossRef]
- Hehir, M.K.; Hobson-Webb, L.D.; Benatar, M.; Barnett, C.; Silvestri, N.J.; Howard, J.F.; Howard, D.; Visser, A.; Crum, B.A.; Nowak, R.; et al. Rituximab as Treatment for Anti-MuSK Myasthenia Gravis. Neurology 2017, 89, 1069–1077. [Google Scholar] [CrossRef]
- Marino, M.; Basile, U.; Spagni, G.; Napodano, C.; Iorio, R.; Gulli, F.; Todi, L.; Provenzano, C.; Bartoccioni, E.; Evoli, A. Long-Lasting Rituximab-Induced Reduction of Specific—But Not Total—IgG4 in MuSK-Positive Myasthenia Gravis. Front. Immunol. 2020, 11, 613. [Google Scholar] [CrossRef]
- Cortés-Vicente, E.; Rojas-Garcia, R.; Díaz-Manera, J.; Querol, L.; Casasnovas, C.; Guerrero-Sola, A.; Muñoz-Blanco, J.L.; Bárcena-Llona, J.E.; Márquez-Infante, C.; Pardo, J.; et al. The Impact of Rituximab Infusion Protocol on the Long-Term Outcome in Anti-MuSK Myasthenia Gravis. Ann. Clin. Transl. Neurol. 2018, 5, 710–716. [Google Scholar] [CrossRef]
- Stathopoulos, P.; Kumar, A.; Heiden, J.A.V.; Pascual-Goñi, E.; Nowak, R.J.; O’Connor, K.C. Mechanisms Underlying B Cell Immune Dysregulation and Autoantibody Production in MuSK Myasthenia Gravis. Ann. N. Y. Acad. Sci. 2018, 1412, 154–165. [Google Scholar] [CrossRef]
- Nowak, R.J.; Coffey, C.S.; Goldstein, J.M.; Dimachkie, M.M.; Benatar, M.; Kissel, J.T.; Wolfe, G.I.; Burns, T.M.; Freimer, M.L.; Nations, S.; et al. Phase 2 Trial of Rituximab in Acetylcholine Receptor Antibody-Positive Generalized Myasthenia Gravis: The BeatMG Study. Neurology 2022, 98, e376–e389. [Google Scholar] [CrossRef]
- Piehl, F.; Eriksson-Dufva, A.; Budzianowska, A.; Feresiadou, A.; Hansson, W.; Hietala, M.A.; Håkansson, I.; Johansson, R.; Jons, D.; Kmezic, I.; et al. Efficacy and Safety of Rituximab for New-Onset Generalized Myasthenia Gravis: The RINOMAX Randomized Clinical Trial. JAMA Neurol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Zhao, C.; Pu, M.; Chen, D.; Shi, J.; Li, Z.; Guo, J.; Zhang, G. Effectiveness and Safety of Rituximab for Refractory Myasthenia Gravis: A Systematic Review and Single-Arm Meta-Analysis. Front. Neurol. 2021, 12, 736190. [Google Scholar] [CrossRef] [PubMed]
- Caballero-Ávila, M.; Álvarez-Velasco, R.; Moga, E.; Rojas-Garcia, R.; Turon-Sans, J.; Querol, L.; Olivé, M.; Reyes-Leiva, D.; Illa, I.; Gallardo, E.; et al. Rituximab in Myasthenia Gravis: Efficacy, Associated Infections and Risk of Induced Hypogammaglobulinemia. Neuromuscul. Disord. 2022, 32, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Whittam, D.H.; Tallantyre, E.C.; Jolles, S.; Huda, S.; Moots, R.J.; Kim, H.J.; Robertson, N.P.; Cree, B.A.C.; Jacob, A. Rituximab in Neurological Disease: Principles, Evidence and Practice. Pract. Neurol. 2019, 19, 5–20. [Google Scholar] [CrossRef] [Green Version]
- Stathopoulos, P.; Dalakas, M.C. Evolution of Anti-B Cell Therapeutics in Autoimmune Neurological Diseases. Neurotherapeutics 2022, 19, 691–710. [Google Scholar] [CrossRef]
- Beecher, G.; Putko, B.N.; Wagner, A.N.; Siddiqi, Z.A. Therapies Directed Against B-Cells and Downstream Effectors in Generalized Autoimmune Myasthenia Gravis: Current Status. Drugs 2019, 79, 353–364. [Google Scholar] [CrossRef]
- Waters, M.J.; Field, D.; Ravindran, J. Refractory Myasthenia Gravis Successfully Treated with Ofatumumab. Muscle Nerve 2019, 60, E45–E47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, D.; Gallagher, S.; Monson, N.L.; Herbst, R.; Wang, Y. Inebilizumab, a B Cell-Depleting Anti-CD19 Antibody for the Treatment of Autoimmune Neurological Diseases: Insights from Preclinical Studies. J. Clin. Med. 2016, 5, 107. [Google Scholar] [CrossRef] [Green Version]
- Frampton, J.E. Inebilizumab: First Approval. Drugs 2020, 80, 1259–1264. [Google Scholar] [CrossRef]
- A Randomized, Double-Blind, Multicenter, Placebo-Controlled Phase 3 Study With Open-Label Period to Evaluate the Efficacy and Safety of Inebilizumab in Adults With Myasthenia Gravis. Available online: https://clinicaltrials.gov/ct2/show/nct04524273 (accessed on 31 August 2022).
- Alabbad, S.; AlGaeed, M.; Sikorski, P.; Kaminski, H.J. Monoclonal Antibody-Based Therapies for Myasthenia Gravis. BioDrugs 2020, 34, 557–566. [Google Scholar] [CrossRef]
- A Multi-Centre, Randomized, Double- Blind, Placebo-Controlled, Parallel Group Study to Preliminarily Evaluate the Safety, Tolerability, Pharmacokinetics and Efficacy of CFZ533 in Patients With Moderate to Severe Myasthenia Gravis. Available online: https://clinicaltrials.gov/ct2/show/results/nct02565576 (accessed on 31 August 2022).
- Field-Smith, A.; Morgan, G.J.; Davies, F.E. Bortezomib (Velcadetrade Mark) in the Treatment of Multiple Myeloma. Ther. Clin. Risk Manag. 2006, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomez, A.M.; Vrolix, K.; Martínez-Martínez, P.; Molenaar, P.C.; Phernambucq, M.; van der Esch, E.; Duimel, H.; Verheyen, F.; Voll, R.E.; Manz, R.A.; et al. Proteasome Inhibition with Bortezomib Depletes Plasma Cells and Autoantibodies in Experimental Autoimmune Myasthenia Gravis. J. Immunol. 2011, 186, 2503–2513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohler, S.; Märschenz, S.; Grittner, U.; Alexander, T.; Hiepe, F.; Meisel, A. Bortezomib in Antibody-Mediated Autoimmune Diseases (TAVAB): Study Protocol for a Unicentric, Non-Randomised, Non-Placebo Controlled Trial. BMJ Open 2019, 9, e024523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alé, A.; Bruna, J.; Navarro, X.; Udina, E. Neurotoxicity Induced by Antineoplastic Proteasome Inhibitors. Neurotoxicology 2014, 43, 28–35. [Google Scholar] [CrossRef]
- Liu, Z.J.; Lin, H.X.; Liu, G.L.; Tao, Q.Q.; Ni, W.; Xiao, B.G.; Wu, Z.Y. The Investigation of Genetic and Clinical Features in Chinese Patients with Juvenile Amyotrophic Lateral Sclerosis. Clin. Genet. 2017, 92, 267–273. [Google Scholar] [CrossRef]
- Tenca, C.; Merlo, A.; Zarcone, D.; Saverino, D.; Bruno, S.; De Santanna, A.; Ramarli, D.; Fabbi, M.; Pesce, C.; Deaglio, S.; et al. Death of T Cell Precursors in the Human Thymus: A Role for CD38. Int. Immunol. 2003, 15, 1105–1116. [Google Scholar] [CrossRef] [Green Version]
- Bonello, F.; Rocchi, S.; Barilà, G.; Sandrone, M.; Talarico, M.; Zamagni, E.; Scaldaferri, M.; Vedovato, S.; Bertiond, C.; Pavan, L.; et al. Safety of Rapid Daratumumab Infusion: A Retrospective, Multicenter, Real-Life Analysis on 134 Patients With Multiple Myeloma. Front. Oncol. 2022, 12, 851864. [Google Scholar] [CrossRef]
- A Phase 2, Randomized, Placebo-Controlled Study to Evaluate Safety, Tolerability, and Efficacy of TAK-079 in Patients With Generalized Myasthenia Gravis. Available online: https://clinicaltrials.gov/ct2/show/nct04159805 (accessed on 31 August 2022).
- Scheibe, F.; Ostendorf, L.; Prüss, H.; Radbruch, H.; Aschman, T.; Hoffmann, S.; Blau, I.W.; Meisel, C.; Alexander, T.; Meisel, A. Daratumumab for Treatment-Refractory Antibody-Mediated Diseases in Neurology. Eur. J. Neurol. 2022, 29, 1847–1854. [Google Scholar] [CrossRef]
- Aricha, R.; Mizrachi, K.; Fuchs, S.; Souroujon, M.C. Blocking of IL-6 Suppresses Experimental Autoimmune Myasthenia Gravis. J. Autoimmun. 2011, 36, 135–141. [Google Scholar] [CrossRef]
- Jonsson, D.I.; Pirskanen, R.; Piehl, F. Beneficial Effect of Tocilizumab in Myasthenia Gravis Refractory to Rituximab. Neuromuscul. Disord. 2017, 27, 565–568. [Google Scholar] [CrossRef]
- Anand, P.; Slama, M.C.C.; Kaku, M.; Ong, C.; Cervantes-Arslanian, A.M.; Zhou, L.; David, W.S.; Guidon, A.C. COVID-19 in Patients with Myasthenia Gravis. Muscle Nerve 2020, 62, 254–258. [Google Scholar] [CrossRef] [PubMed]
- A Multi-Center, Randomized, Double-Blind, Placebo-Controlled Clinical Trial of the Efficacy and Safety of Tocilizumab in the Treatment of Generalized Myasthenia Gravis. Available online: https://clinicaltrials.gov/ct2/show/nct05067348 (accessed on 31 August 2022).
- A Phase III, Randomized, Double-Blind, Placebo-Controlled, Multicenter Study To Evaluate Efficacy, Safety, Pharmacokinetics, And Pharmacodynamics Of Satralizumab In Patients With Generalized Myasthenia Gravis. Available online: https://clinicaltrials.gov/ct2/show/nct04963270 (accessed on 4 September 2022).
- Pelechas, E.; Memi, T.; Markatseli, T.E.; Voulgari, P.V.; Drosos, A.A. Adalimumab-Induced Myasthenia Gravis: Case-Based Review. Rheumatol. Int. 2020, 40, 1891–1894. [Google Scholar] [CrossRef] [PubMed]
- Nicocia, G.; Bonanno, C.; Lupica, A.; Toscano, A.; Rodolico, C. Myasthenia Gravis after Etanercept and Ustekinumab Treatment for Psoriatic Arthritis: A Case Report. Neuromuscul. Disord. 2020, 30, 246–249. [Google Scholar] [CrossRef] [PubMed]
- Davidson, A. Targeting BAFF in Autoimmunity. Curr. Opin. Immunol. 2010, 22, 732–739. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.Y.; Kang, C.H.; Lee, K.H. B-Cell–Activating Factor Is Elevated in Serum of Patients with Myasthenia Gravis. Muscle Nerve 2016, 54, 1030–1033. [Google Scholar] [CrossRef] [Green Version]
- Hewett, K.; Sanders, D.B.; Grove, R.A.; Broderick, C.L.; Rudo, T.J.; Bassiri, A.; Zvartau-Hind, M.; Bril, V. Randomized Study of Adjunctive Belimumab in Participants with Generalized Myasthenia Gravis. Neurology 2018, 90, e1425–e1434. [Google Scholar] [CrossRef] [Green Version]
- Mohamed, A.J.; Yu, L.; Bäckesjö, C.M.; Vargas, L.; Faryal, R.; Aints, A.; Christensson, B.; Berglöf, A.; Vihinen, M.; Nore, B.F.; et al. Bruton’s Tyrosine Kinase (Btk): Function, Regulation, and Transformation with Special Emphasis on the PH Domain. Immunol. Rev. 2009, 228, 58–73. [Google Scholar] [CrossRef]
- Estupiñán, H.Y.; Berglöf, A.; Zain, R.; Smith, C.I.E. Comparative Analysis of BTK Inhibitors and Mechanisms Underlying Adverse Effects. Front. Cell Dev. Biol. 2021, 9, 630942. [Google Scholar] [CrossRef]
- Reich, D.S.; Arnold, D.L.; Vermersch, P.; Bar-Or, A.; Fox, R.J.; Matta, A.; Turner, T.; Wallström, E.; Zhang, X.; Mareš, M.; et al. Safety and Efficacy of Tolebrutinib, an Oral Brain-Penetrant BTK Inhibitor, in Relapsing Multiple Sclerosis: A Phase 2b, Randomised, Double-Blind, Placebo-Controlled Trial. Lancet Neurol. 2021, 20, 729–738. [Google Scholar] [CrossRef]
- A Phase 3, Randomized, Double-Blind, Placebo-Controlled, Parallel-Group Study to Evaluate the Efficacy and Safety of Tolebrutinib (SAR442168) in Adults With Generalized Myasthenia Gravis (MG). Available online: https://clinicaltrials.gov/ct2/show/nct05132569 (accessed on 31 August 2022).
- Sahashi, K.; Engel, A.G.; Lindstrom, J.M.; Lambert, E.H.; Lennon, V.A. Ultrastructural Localization of Immune Complexes (IgG and C3) at the End-Plate in Experimental Autoimmune Myasthenia Gravis. J. Neuropathol. Exp. Neurol. 1978, 37, 212–223. [Google Scholar] [CrossRef]
- Kusner, L.L.; Sengupta, M.; Kaminski, H.J. Acetylcholine Receptor Antibody-Mediated Animal Models of Myasthenia Gravis and the Role of Complement. Ann. N. Y. Acad. Sci. 2018, 1413, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Nakano, S.; Engel, A.G. Myasthenia Gravis: Quantitative Immunocytochemical Analysis of Inflammatory Cells and Detection of Complement Membrane Attack Complex at the End-Plate in 30 Patients. Neurology 1993, 43, 1167–1172. [Google Scholar] [CrossRef] [PubMed]
- Basta, M.; Illa, I.; Dalakas, M.C. Increased in Vitro Uptake of the Complement C3b in the Serum of Patients with Guillain-Barré Syndrome, Myasthenia Gravis and Dermatomyositis. J. Neuroimmunol. 1996, 71, 227–229. [Google Scholar] [CrossRef]
- Romi, F.; Kristoffersen, E.K.; Aarli, J.A.; Gilhus, N.E. The Role of Complement in Myasthenia Gravis: Serological Evidence of Complement Consumption in Vivo. J. Neuroimmunol. 2005, 158, 191–194. [Google Scholar] [CrossRef]
- Toyka, K.V.; Drachman, D.B.; Griffin, D.E.; Pestronk, A.; Winkelstein, J.A.; Fischbeck, K.H.; Kao, I. Myasthenia Gravis. Study of Humoral Immune Mechanisms by Passive Transfer to Mice. N. Engl. J. Med. 1977, 296, 125–131. [Google Scholar] [CrossRef]
- Lennon, V.A. The Immunopathology of Myasthenia Gravis. Hum. Pathol. 1978, 9, 541–551. [Google Scholar] [CrossRef]
- Menon, D.; Bril, V. Pharmacotherapy of Generalized Myasthenia Gravis with Special Emphasis on Newer Biologicals. Drugs 2022, 82, 865–887. [Google Scholar] [CrossRef]
- Howard, J.F.; Utsugisawa, K.; Benatar, M.; Murai, H.; Barohn, R.J.; Illa, I.; Jacob, S.; Vissing, J.; Burns, T.M.; Kissel, J.T.; et al. Safety and Efficacy of Eculizumab in Anti-Acetylcholine Receptor Antibody-Positive Refractory Generalised Myasthenia Gravis (REGAIN): A Phase 3, Randomised, Double-Blind, Placebo-Controlled, Multicentre Study. Lancet Neurol. 2017, 16, 976–986. [Google Scholar] [CrossRef]
- Muppidi, S.; Utsugisawa, K.; Benatar, M.; Murai, H.; Barohn, R.J.; Illa, I.; Jacob, S.; Vissing, J.; Burns, T.M.; Kissel, J.T.; et al. Long-Term Safety and Efficacy of Eculizumab in Generalized Myasthenia Gravis. Muscle Nerve 2019, 60, 14–24. [Google Scholar] [CrossRef] [Green Version]
- Nowak, R.J.; Muppidi, S.; Beydoun, S.R.; O’Brien, F.L.; Yountz, M.; Howard, J.F. Concomitant Immunosuppressive Therapy Use in Eculizumab-Treated Adults With Generalized Myasthenia Gravis During the REGAIN Open-Label Extension Study. Front. Neurol. 2020, 11, 556104. [Google Scholar] [CrossRef]
- Dalakas, M.C. Role of Complement, Anti-Complement Therapeutics, and Other Targeted Immunotherapies in Myasthenia Gravis. Expert Rev. Clin. Immunol. 2022, 18, 691–701. [Google Scholar] [CrossRef] [PubMed]
- Sheridan, D.; Yu, Z.X.; Zhang, Y.; Patel, R.; Sun, F.; Lasaro, M.A.; Bouchard, K.; Andrien, B.; Marozsan, A.; Wang, Y.; et al. Design and Preclinical Characterization of ALXN1210: A Novel Anti-C5 Antibody with Extended Duration of Action. PLoS ONE 2018, 13, e0195909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vu, T.; Meisel, A.; Mantegazza, R.; Annane, D.; Katsuno, M.; Aguzzi, R.; Enayetallah, A.; Beasley, K.N.; Rampal, N.; Howard, J.F., Jr. Terminal Complement Inhibitor Ravulizumab in Generalized Myasthenia Gravis. NEJM Evid. 2022, 1, EVIDoa2100066. [Google Scholar] [CrossRef]
- Howard, J.F.; Nowak, R.J.; Wolfe, G.I.; Freimer, M.L.; Vu, T.H.; Hinton, J.L.; Benatar, M.; Duda, P.W.; MacDougall, J.E.; Farzaneh-Far, R.; et al. Clinical Effects of the Self-Administered Subcutaneous Complement Inhibitor Zilucoplan in Patients with Moderate to Severe Generalized Myasthenia Gravis: Results of a Phase 2 Randomized, Double-Blind, Placebo-Controlled, Multicenter Clinical Trial. JAMA Neurol. 2020, 77, 582–592. [Google Scholar] [CrossRef] [Green Version]
- A Phase 3, Multicenter, Randomized, Double Blind, Placebo-Controlled Study to Confirm the Safety, Tolerability, and Efficacy of Zilucoplan in Subjects With Generalized Myasthenia Gravis. Available online: https://clinicaltrials.gov/ct2/show/nct04115293 (accessed on 31 August 2022).
- Club, B.; Business, F.A.Q.; Bureau, G.D.; Investigate, T.V. UCB Announces Positive Data in Myasthenia Gravis with Zilucoplan Phase 3 Study Results|UCB. Available online: https://www.14news.com/prnewswire/2022/02/04/ucb-announces-positive-data-myasthenia-gravis-with-zilucoplan-phase-3-study-results/?outputType=amp (accessed on 4 September 2022).
- Kang, T.H.; Jung, S.T. Boosting Therapeutic Potency of Antibodies by Taming Fc Domain Functions. Exp. Mol. Med. 2019, 51, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Patel, D.D.; Bussel, J.B. Neonatal Fc Receptor in Human Immunity: Function and Role in Therapeutic Intervention. J. Allergy Clin. Immunol. 2020, 146, 467–478. [Google Scholar] [CrossRef]
- Sesarman, A.; Vidarsson, G.; Sitaru, C. The Neonatal Fc Receptor as Therapeutic Target in IgG-Mediated Autoimmune Diseases. Cell. Mol. Life Sci. 2010, 67, 2533–2550. [Google Scholar] [CrossRef] [PubMed]
- Habib, A.A.; Ahmadi Jazi, G.; Mozaffar, T. Update on Immune-Mediated Therapies for Myasthenia Gravis. Muscle Nerve 2020, 62, 579–592. [Google Scholar] [CrossRef]
- Huda, R. New Approaches to Targeting B Cells for Myasthenia Gravis Therapy. Front. Immunol. 2020, 11, 240. [Google Scholar] [CrossRef] [Green Version]
- Ulrichts, P.; Guglietta, A.; Dreier, T.; Van Bragt, T.; Hanssens, V.; Hofman, E.; Vankerckhoven, B.; Verheesen, P.; Ongenae, N.; Lykhopiy, V.; et al. Neonatal Fc Receptor Antagonist Efgartigimod Safely and Sustainably Reduces IgGs in Humans. J. Clin. Investig. 2018, 128, 4372–4386. [Google Scholar] [CrossRef]
- Howard, J.F.; Bril, V.; Burns, T.M.; Mantegazza, R.; Bilinska, M.; Szczudlik, A.; Beydoun, S.; Garrido, F.J.R.D.R.; Piehl, F.; Rottoli, M.; et al. Randomized Phase 2 Study of FcRn Antagonist Efgartigimod in Generalized Myasthenia Gravis. Neurology 2019, 92, e2661–e2673. [Google Scholar] [CrossRef]
- Howard, J.F.; Bril, V.; Vu, T.; Karam, C.; Peric, S.; Margania, T.; Murai, H.; Bilinska, M.; Shakarishvili, R.; Smilowski, M.; et al. Safety, Efficacy, and Tolerability of Efgartigimod in Patients with Generalised Myasthenia Gravis (ADAPT): A Multicentre, Randomised, Placebo-Controlled, Phase 3 Trial. Lancet Neurol. 2021, 20, 526–536. [Google Scholar] [CrossRef]
- Evaluating the Pharmacodynamic Noninferiority of Efgartigimod PH20 SC Administered Subcutaneously as Compared to Efgartigimod Administered Intravenously in Patients with Generalized Myasthenia Gravis (ADAPTsc). Available online: https://clinicaltrials.gov/ct2/show/nct04735432 (accessed on 31 August 2022).
- Evaluating the Long-Term Safety and Tolerability of Efgartigimod PH20 SC Administered Subcutaneously in Patients with Generalized Myasthenia Gravis (ADAPTsc+). Available online: https://clinicaltrials.gov/ct2/Show/nct04818671 (accessed on 31 August 2022).
- FDA Approves New Treatment for Myasthenia Gravis. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-new-treatment-myasthenia-gravis (accessed on 31 August 2022).
- European Medicines Agency Authorization for Vyvgart (Efgartigimod) in Myasthenia Gravis. Available online: https://www.ema.europa.eu/en/medicines/human/epar/vyvgart#authorisation-details-section (accessed on 4 September 2022).
- Efgartigimod Expanded Access for Generalized Myasthenia Gravis. Available online: https://clinicaltrials.gov/ct2/show/nct04777734 (accessed on 31 August 2022).
- Smith, B.; Kiessling, A.; Lledo-Garcia, R.; Dixon, K.L.; Christodoulou, L.; Catley, M.C.; Atherfold, P.; D’Hooghe, L.E.; Finney, H.; Greenslade, K.; et al. Generation and Characterization of a High Affinity Anti-Human FcRn Antibody, Rozanolixizumab, and the Effects of Different Molecular Formats on the Reduction of Plasma IgG Concentration. MAbs 2018, 10, 1111–1130. [Google Scholar] [CrossRef] [PubMed]
- Bril, V.; Benatar, M.; Andersen, H.; Vissing, J.; Brock, M.; Greve, B.; Kiessling, P.; Woltering, F.; Griffin, L.; van den Bergh, P. Efficacy and Safety of Rozanolixizumab in Moderate to Severe Generalized Myasthenia Gravis: A Phase 2 Randomized Control Trial. Neurology 2021, 96, e853–e865. [Google Scholar] [CrossRef] [PubMed]
- An Open-Label Extension Study to Evaluate Rozanolixizumab in Study Participants with Generalized Myasthenia Gravis. Available online: https://clinicaltrials.gov/ct2/show/nct04650854 (accessed on 31 August 2022).
- Ling, L.E.; Hillson, J.L.; Tiessen, R.G.; Bosje, T.; van Iersel, M.P.; Nix, D.J.; Markowitz, L.; Cilfone, N.A.; Duffner, J.; Streisand, J.B.; et al. M281, an Anti-FcRn Antibody: Pharmacodynamics, Pharmacokinetics, and Safety Across the Full Range of IgG Reduction in a First-in-Human Study. Clin. Pharmacol. Ther. 2019, 105, 1031–1039. [Google Scholar] [CrossRef] [Green Version]
- Guptill, J.; Antozzi, C.; Bril, V.; Gamez, J.; Meuth, S.G.; Muñoz Blanco, J.L.; Nowak, R.J.; Quan, D.; Sevilla, T.; Szczudlik, A.; et al. Vivacity-MG: A Phase 2, Multicenter, Randomized, Double-Blind, Placebo-Controlled Study to Evaluate the Safety, Tolerability, Efficacy, Pharmacokinetics, Pharmacodynamics, and Immunogenicity of Nipocalimab Administered to Adults with Generalized Myasthenia Gravis. Neurol. 2021, 96 (Suppl. 15), 2157. [Google Scholar]
- A Study of Nipocalimab Administered to Adults with Generalized Myasthenia Gravis. Available online: https://clinicaltrials.gov/ct2/show/nct04951622 (accessed on 31 August 2022).
- Post-Trial Access for Nipocalimab in Participants with Warm Autoimmune Hemolytic Anemia (WAIHA). Available online: https://clinicaltrials.gov/ct2/show/nct05221619 (accessed on 31 August 2022).
- Zuercher, A.W.; Spirig, R.; Baz Morelli, A.; Rowe, T.; Käsermann, F. Next-Generation Fc Receptor–Targeting Biologics for Autoimmune Diseases. Autoimmun. Rev. 2019, 18, 102366. [Google Scholar] [CrossRef]
- Yan, C.; Duan, R.S.; Yang, H.; Li, H.F.; Zou, Z.; Zhang, H.; Zhou, H.; Li, X.L.; Zhou, H.; Jiao, L.; et al. Therapeutic Effects of Batoclimab in Chinese Patients with Generalized Myasthenia Gravis: A Double-Blinded, Randomized, Placebo-Controlled Phase II Study. Neurol. Ther. 2022, 11, 815–834. [Google Scholar] [CrossRef]
- Phase 3 Study to Assess the Efficacy and Safety of Batoclimab as Induction and Maintenance Therapy in Adult Participants with Generalized Myasthenia Gravis. Available online: https://clinicaltrials.gov/ct2/show/nct05403541 (accessed on 31 August 2022).
- Blumberg, L.J.; Humphries, J.E.; Jones, S.D.; Pearce, L.B.; Holgate, R.; Hearn, A.; Cheung, J.; Mahmood, A.; Del Tito, B.; Graydon, J.S.; et al. Blocking FcRn in Humans Reduces Circulating IgG Levels and Inhibits IgG Immune Complex-Mediated Immune Responses. Sci. Adv. 2019, 5, eaax9586. [Google Scholar] [CrossRef] [Green Version]
- A Safety Study of SYNT001 in Subjects with Chronic, Stable Warm Autoimmune Hemolytic Anemia (WAIHA). Available online: https://clinicaltrials.gov/ct2/show/nct03075878 (accessed on 31 August 2022).
- Werth, V.P.; Culton, D.A.; Concha, J.S.S.; Graydon, J.S.; Blumberg, L.J.; Okawa, J.; Pyzik, M.; Blumberg, R.S.; Hall, R.P. Safety, Tolerability, and Activity of ALXN1830 Targeting the Neonatal Fc Receptor in Chronic Pemphigus. J. Investig. Dermatol. 2021, 141, 2858–2865.e4. [Google Scholar] [CrossRef]
- Affibody Announces Termination of ABY-039 (FcRn) Program. Available online: https://www.affibody.se/affibody-announces-termination-of-aby-039-fcrn-program/#:~:text=aby-039%20is%20a%20bivalent%20antibody-mimetic%20that%20targets%20the,in%20patients%20with%20myasthenia%20gravis%20in%20Phase%203. (accessed on 31 August 2022).
- A Study to Investigate the Safety, Tolerability and Pharmacokinetics of ABY-039. Available online: https://clinicaltrials.gov/ct2/show/nct03502954 (accessed on 31 August 2022).
- Seijsing, J.; Lindborg, M.; Höidén-Guthenberg, I.; Bönisch, H.; Guneriusson, E.; Frejd, F.Y.; Abrahmsén, L.; Ekblad, C.; Löfblom, J.; Uhlén, M.; et al. An Engineered Affibody Molecule with PH-Dependent Binding to FcRN Mediates Extended Circulatory Half-Life of a Fusion Protein. Proc. Natl. Acad. Sci. USA 2014, 111, 17110–17115. [Google Scholar] [CrossRef] [PubMed]
- Sabre, L.; Punga, T.; Punga, A.R. Circulating MiRNAs as Potential Biomarkers in Myasthenia Gravis: Tools for Personalized Medicine. Front. Immunol. 2020, 11, 213. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Tejerina, D.; Sotoca, J.; Llaurado, A.; López-Diego, V.; Juntas-Morales, R.; Salvado, M. New Targeted Agents in Myasthenia Gravis and Future Therapeutic Strategies. J. Clin. Med. 2022, 11, 6394. https://doi.org/10.3390/jcm11216394
Sánchez-Tejerina D, Sotoca J, Llaurado A, López-Diego V, Juntas-Morales R, Salvado M. New Targeted Agents in Myasthenia Gravis and Future Therapeutic Strategies. Journal of Clinical Medicine. 2022; 11(21):6394. https://doi.org/10.3390/jcm11216394
Chicago/Turabian StyleSánchez-Tejerina, Daniel, Javier Sotoca, Arnau Llaurado, Veronica López-Diego, Raul Juntas-Morales, and Maria Salvado. 2022. "New Targeted Agents in Myasthenia Gravis and Future Therapeutic Strategies" Journal of Clinical Medicine 11, no. 21: 6394. https://doi.org/10.3390/jcm11216394