
The Use of Aspirin Increases the Risk of Major Adverse Cardiac and Cerebrovascular Events in Hypertensive Patients with Obstructive Sleep Apnea for the Primary Prevention of Cardiovascular Disease: A Real-World Cohort Study
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
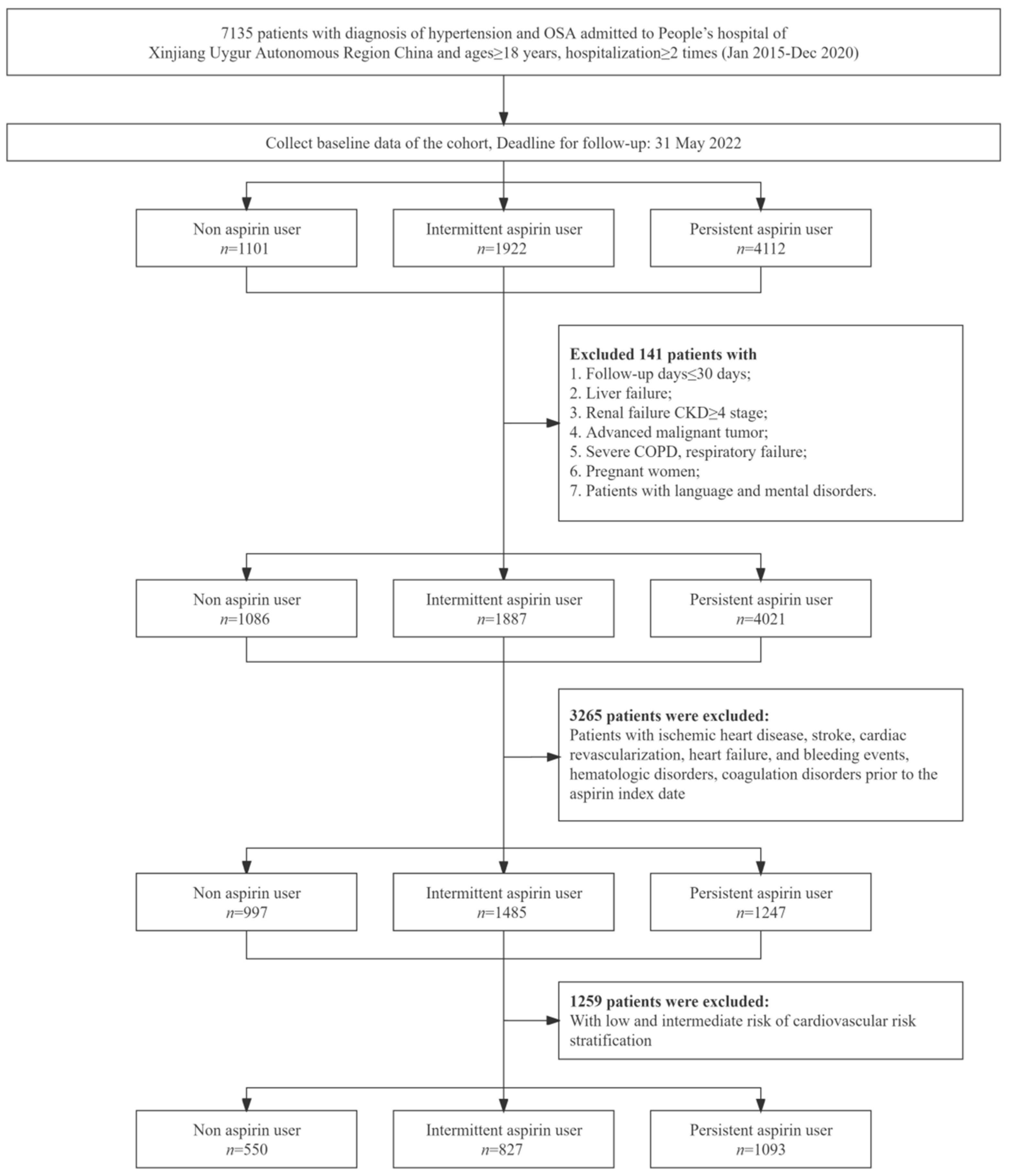
2.2. Study Population
2.3. Data Collection and Definition
2.4. Follow-Up and Results
2.5. Statistical Analysis
3. Result
3.1. Baseline Characteristics of the Participants
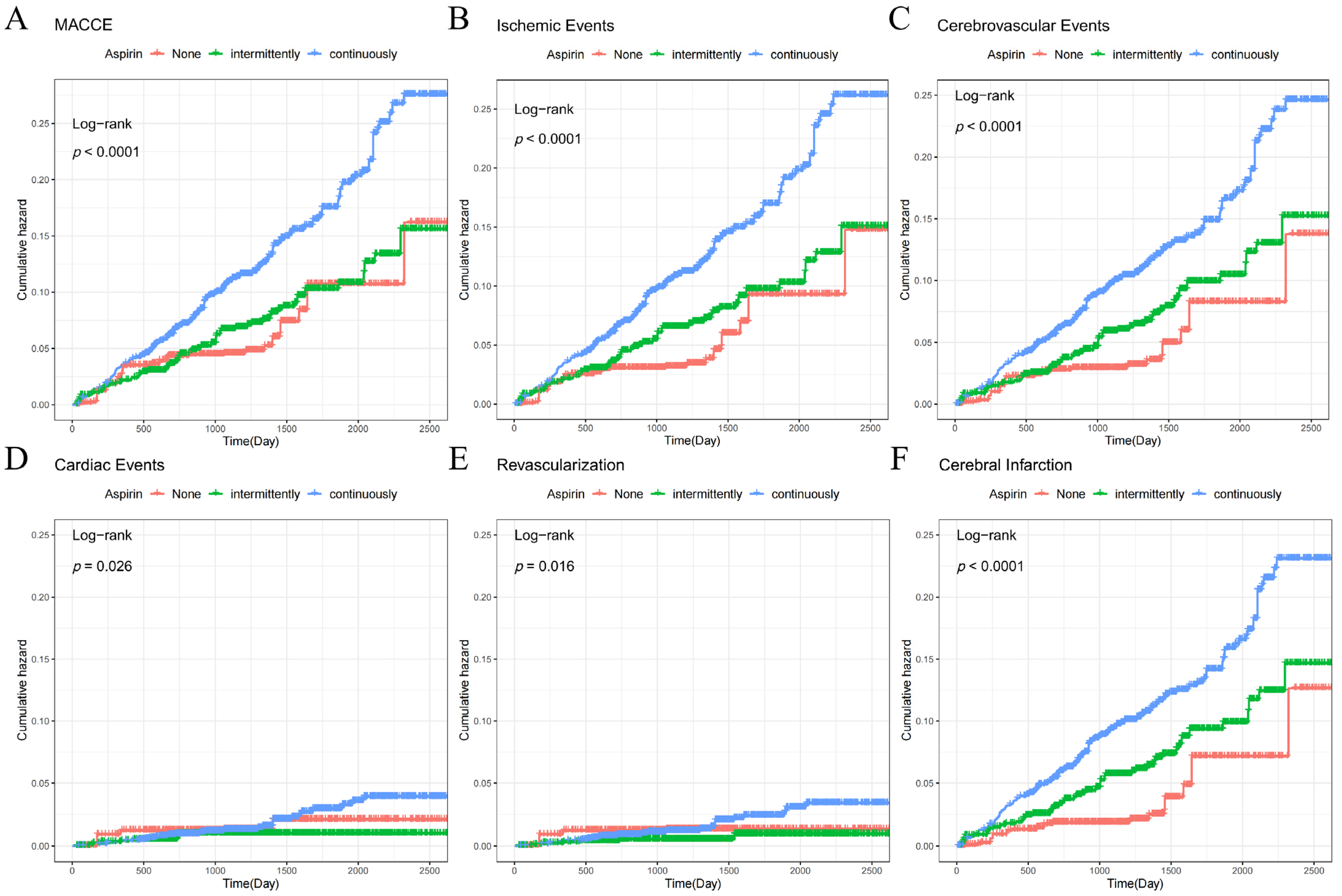
3.2. Relationship between Aspirin and Endpoint Events
3.3. The Relationship between Aspirin and Hemorrhagic Stroke and Gastrointestinal Bleeding
3.4. Relationship between Aspirin Use and Endpoint Events in Patients with Different Grades of OSA
3.5. Sensitivity and Stratified Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- The Writing Committee of the Report on Cardiovascular Health and Diseases in China. Report on Cardiovascular Health and Diseases in China 2021: An Updated Summary. Biomed. Environ. Sci. BES 2022, 35, 573–603. [Google Scholar] [CrossRef]
- Zapater, A.; Sánchez-de-la-Torre, M.; Benítez, I.; Targa, A.; Bertran, S.; Torres, G.; Aldomà, A.; De Batlle, J.; Abad, J.; Duran-Cantolla, J.; et al. The Effect of Sleep Apnea on Cardiovascular Events in Different Acute Coronary Syndrome Phenotypes. Am. J. Respir. Crit. Care Med. 2020, 202, 1698–1706. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, F.; Whelton, P. High Blood Pressure and Cardiovascular Disease. Hypertension 2020, 75, 285–292. [Google Scholar] [CrossRef]
- Torres, G.; Sánchez-de-la-Torre, M.; Barbé, F. Relationship Between OSA and Hypertension. Chest 2015, 148, 824–832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rothwell, P.M.; Algra, A.; Chen, Z.; Diener, H.C.; Norrving, B.; Mehta, Z. Effects of aspirin on risk and severity of early recurrent stroke after transient ischaemic attack and ischaemic stroke: Time-course analysis of randomised trials. Lancet 2016, 388, 365–375. [Google Scholar] [CrossRef] [Green Version]
- Bibbins-Domingo, K. Aspirin Use for the Primary Prevention of Cardiovascular Disease and Colorectal Cancer: U.S. Preventive Services Task Force Recommendation Statement. Ann. Intern. Med. 2016, 164, 836–845. [Google Scholar] [CrossRef] [Green Version]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts)Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef] [PubMed]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef] [PubMed]
- Mahady, S.E.; Margolis, K.L.; Chan, A.; Polekhina, G.; Woods, R.L.; Wolfe, R.; Nelson, M.R.; Lockery, J.E.; Wood, E.M.; Reid, C.; et al. Major GI bleeding in older persons using aspirin: Incidence and risk factors in the ASPREE randomised controlled trial. Gut 2021, 70, 717–724. [Google Scholar] [CrossRef] [PubMed]
- Sugawara, M.; Goto, Y.; Yamazaki, T.; Teramoto, T.; Oikawa, S.; Shimada, K.; Uchiyama, S.; Ando, K.; Ishizuka, N.; Murata, M.; et al. Low-Dose Aspirin for Primary Prevention of Cardiovascular Events in Elderly Japanese Patients with Atherosclerotic Risk Factors: Subanalysis of a Randomized Clinical Trial (JPPP-70). Am. J. Cardiovasc. Drugs Drugs Devices Other Interv. 2019, 19, 299–311. [Google Scholar] [CrossRef] [Green Version]
- Carrick, D.; Haig, C.; Maznyczka, A.M.; Carberry, J.; Mangion, K.; Ahmed, N.; Yue May, V.T.; McEntegart, M.; Petrie, M.C.; Eteiba, H.; et al. Hypertension, Microvascular Pathology, and Prognosis After an Acute Myocardial Infarction. Hypertension 2018, 72, 720–730. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, J.A.; Veasey, S.C.; Morgan, B.J.; Morgan, B.J.; O’Donnell, C.P.; O’Donnell, C.P. Pathophysiology of sleep apnea. Physiol. Rev. 2010, 90, 47–112. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Q.; Heizhati, M.; Lin, M.; Wang, M.; Yao, X.; Gan, L.; Luo, Q.; Zhang, W.; Hong, J.; Yue, N.; et al. Higher Plasma Aldosterone Concentrations Are Associated With Elevated Risk of Aortic Dissection and Aneurysm: A Case-Control Study. Hypertension 2022, 79, 736–746. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.S. 2010 Chinese guidelines for the management of hypertension. Zhonghua Xin Xue Guan Bing Za Zhi 2011, 39, 579–615. [Google Scholar] [PubMed]
- Pishgar, F.; Greifer, N.; Leyrat, C.; Stuart, E. MatchThem:: Matching and Weighting after Multiple Imputation. R J. 2021, 13, 228. [Google Scholar] [CrossRef]
- Leyrat, C.; Seaman, S.R.; White, I.R.; Douglas, I.; Smeeth, L.; Kim, J.; Resche-Rigon, M.; Carpenter, J.R.; Williamson, E.J. Propensity score analysis with partially observed covariates: How should multiple imputation be used? Stat. Methods Med. Res. 2019, 28, 3–19. [Google Scholar] [CrossRef] [PubMed]
- Mathur, M.B.; Ding, P.; Riddell, C.A.; Riddell, C.A.; VanderWeele, T.J.; VanderWeele, T.J. Web Site and R Package for Computing E-values. Epidemiology 2018, 29, e45–e47. [Google Scholar] [CrossRef] [PubMed]
- VanderWeele, T.J.; Ding, P. Sensitivity Analysis in Observational Research: Introducing the E-Value. Ann. Intern. Med. 2017, 167, 268–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davidson, K.W.; Barry, M.J.; Mangione, C.M.; Cabana, M.; Chelmow, D.; Coker, T.R.; Davis, E.M.; Donahue, K.E.; Jaén, C.R.; Krist, A.H.; et al. Aspirin Use to Prevent Cardiovascular Disease: US Preventive Services Task Force Recommendation Statement. Jama 2022, 327, 1577–1584. [Google Scholar] [CrossRef] [PubMed]
- Krieger, A.C.; Anand, R.; Hernandez-Rosa, E.; Maidman, A.; Milrad, S.; DeGrazia, M.Q.; Choi, A.J.; Oromendia, C.; Marcus, A.J.; Drosopoulos, J.H.F. Increased platelet activation in sleep apnea subjects with intermittent hypoxemia. Sleep Breath. 2020, 24, 1537–1547. [Google Scholar] [CrossRef]
- von Känel, R.; Malan, N.T.; Hamer, M.; Lambert, G.W.; Schlaich, M.; Reimann, M.; Malan, L. Three-year changes of prothrombotic factors in a cohort of South Africans with a high clinical suspicion of obstructive sleep apnea. Thromb. Haemost. 2016, 115, 63–72. [Google Scholar] [CrossRef]
- Doyle, A.E. Hypertension and vascular disease. Am. J. Hypertens. 1991, 4, 103s–106s. [Google Scholar] [CrossRef] [PubMed]
- Gong, W.; Wang, X.; Fan, J.; Nie, S.; Wei, Y. Impact of Obstructive Sleep Apnea on Platelet Function Profiles in Patients with Acute Coronary Syndrome Taking Dual Antiplatelet Therapy. J. Am. Heart Assoc. 2018, 7, e008808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, X.M.; Qian, X.S.; Gao, X.F.; Ge, Z.; Tian, N.L.; Kan, J.; Zhang, J.J. Obstructive Sleep Apnea Affecting Platelet Reactivity in Patients Undergoing Percutaneous Coronary Intervention. Chin. Med. J. 2018, 131, 1023–1029. [Google Scholar] [CrossRef] [PubMed]
- Scinico, M.; Sostin, O.V.; Agarwal, R.; Kapoor, A.D.; Petrini, J.R.; Mendez, J.L. A Pilot Study Of Aspirin Resistance In Obstructive Sleep Apnea Patients. Clin. Investig. Med. Med. Clin. Exp. 2021, 44, E55–E63. [Google Scholar] [CrossRef] [PubMed]
- Valles, J.; Santos, M.T.; Aznar, J.; Osa, A.; Lago, A.; Cosin, J.; Sanchez, E.; Broekman, M.J.; Marcus, A.J. Erythrocyte promotion of platelet reactivity decreases the effectiveness of aspirin as an antithrombotic therapeutic modality: The effect of low-dose aspirin is less than optimal in patients with vascular disease due to prothrombotic effects of erythrocytes on platelet reactivity. Circulation 1998, 97, 350–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, D.; Griendling, K.K.; Landmesser, U.; Landmesser, U.; Hornig, B.; Hornig, B.; Drexler, H.; Drexler, H. Role of oxidative stress in atherosclerosis. Am. J. Cardiol. 2003, 91, 7A–11A. [Google Scholar] [CrossRef] [PubMed]
- Crescente, M.; Armstrong, P.C.; Kirkby, N.S.; Edin, M.L.; Chan, M.V.; Lih, F.B.; Jiao, J.; Maffucci, T.; Allan, H.E.; Mein, C.A.; et al. Profiling the eicosanoid networks that underlie the anti- and pro-thrombotic effects of aspirin. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2020, 34, 10027–10040. [Google Scholar] [CrossRef] [PubMed]
- Krieger, J.; Benzoni, D.; Sforza, E.; Sassard, J. Urinary excretion of prostanoids during sleep in obstructive sleep apnoea patients. Clin. Exp. Pharm. Physiol. 1991, 18, 551–555. [Google Scholar] [CrossRef] [PubMed]
- Francois, H.; Athirakul, K.; Howell, D.; Dash, R.; Mao, L.; Kim, H.-S.; Rockman, H.A.; Fitzgerald, G.A.; Koller, B.H.; Coffman, T.M. Prostacyclin protects against elevated blood pressure and cardiac fibrosis. Cell Metab. 2005, 2, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikeda, Y.; Shimada, K.; Teramoto, T.; Uchiyama, S.; Yamazaki, T.; Oikawa, S.; Sugawara, M.; Ando, K.; Murata, M.; Yokoyama, K.; et al. Low-dose aspirin for primary prevention of cardiovascular events in Japanese patients 60 years or older with atherosclerotic risk factors: A randomized clinical trial. JAMA 2014, 312, 2510–2520. [Google Scholar] [CrossRef] [PubMed]
- Gaziano, J.M.; Brotons, C.; Coppolecchia, R.; Cricelli, C.; Darius, H.; Gorelick, P.B.; Howard, G.; Pearson, T.A.; Rothwell, P.M.; Ruilope, L.M.; et al. Use of aspirin to reduce risk of initial vascular events in patients at moderate risk of cardiovascular disease (ARRIVE): A randomised, double-blind, placebo-controlled trial. Lancet 2018, 392, 1036–1046. [Google Scholar] [CrossRef] [PubMed]
- Mochol, J.; Gawrys, J.; Gajecki, D.; Szahidewicz-Krupska, E.; Martynowicz, H.; Doroszko, A. Cardiovascular Disorders Triggered by Obstructive Sleep Apnea-A Focus on Endothelium and Blood Components. Int. J. Mol. Sci. 2021, 22, 5139. [Google Scholar] [CrossRef]
- Alonso-Fernández, A.; Toledo-Pons, N.; García-Río, F. Obstructive sleep apnea and venous thromboembolism: Overview of an emerging relationship. Sleep Med. Rev. 2020, 50, 101233. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All | Non-Users | Intermittent Users | Persistent Users | p before IPTW | p after IPTW | |
|---|---|---|---|---|---|---|
| n = 2470 | n = 550 | n = 827 | n = 1093 | |||
| Gender | 0.829 | 0.528 | ||||
| Female | 558 (22.6%) | 125 (22.7%) | 192 (23.2%) | 241 (22.0%) | ||
| Male | 1912 (77.4%) | 425 (77.3%) | 635 (76.8%) | 852 (78.0%) | ||
| Age, y | 48.1 (9.8) | 43.7 (10.1) | 47.8 (9.8) | 50.6 (8.9) | <0.001 | 0.758 |
| Duration of hypertension, y | 5.8 (3.1) | 5.3 (3.1) | 5.7 (3.1) | 6.1 (3.1) | <0.001 | 0.953 |
| Duration of hypertension groups | <0.001 | 0.345 | ||||
| ≤4 years | 735 (29.8%) | 200 (36.4%) | 258 (31.2%) | 277 (25.3%) | ||
| >4 years, ≤8 years | 994 (40.2%) | 218 (39.6%) | 313 (37.8%) | 463 (42.4%) | ||
| >8 years | 741 (30.0%) | 132 (24.0%) | 256 (31.0%) | 353 (32.3%) | ||
| Smoke (ever) | 1209 (48.9%) | 267 (48.5%) | 395 (47.8%) | 547 (50.0%) | 0.598 | 0.199 |
| Drink (ever) | 1108 (44.9%) | 240 (43.6%) | 360 (43.5%) | 508 (46.5%) | 0.353 | 0.966 |
| Baseline DBP, mmHg | 92.9 (15.2) | 94.5 (15.8) | 94.0 (14.8) | 91.3 (15.0) | <0.001 | 0.611 |
| Baseline SBP, mmHg | 149 (21.5) | 149 (21.6) | 149 (21.3) | 148 (21.6) | 0.518 | 0.683 |
| BMI, kg/m2 | 28.9 (4.5) | 29.2 (5.3) | 29.1 (4.7) | 28.5 (3.7) | 0.001 | 0.733 |
| BMI groups | 0.472 | 0.440 | ||||
| <28 kg/m2 | 1114 (45.1%) | 242 (44.0%) | 364 (44.0%) | 508 (46.5%) | ||
| ≥28 kg/m2 | 1356 (54.9%) | 308 (56.0%) | 463 (56.0%) | 585 (53.5%) | ||
| Waist, cm | 102 (11.8) | 103 (13.7) | 103 (12.1) | 102 (10.5) | 0.047 | 0.855 |
| OSA grade | 0.281 | 0.540 | ||||
| Mild | 862 (34.9%) | 204 (37.1%) | 292 (35.3%) | 366 (33.5%) | ||
| Moderate | 764 (30.9%) | 160 (29.1%) | 242 (29.3%) | 362 (33.1%) | ||
| Severe | 844 (34.2%) | 186 (33.8%) | 293 (35.4%) | 365 (33.4%) | ||
| Baseline DM | 639 (25.9%) | 123 (22.4%) | 195 (23.6%) | 321 (29.4%) | 0.002 | 0.826 |
| ALT, U/L | 26.0 [18.0; 39.0] | 26.0 [18.7; 41.9] | 26.0 [17.9; 40.0] | 25.2 [18.0; 38.0] | 0.228 | 0.777 |
| AST, U/L | 19.0 [16.0; 25.0] | 19.9 [16.0; 25.0] | 19.0 [15.5; 24.0] | 19.0 [16.0; 25.0] | 0.534 | 0.788 |
| Crea, μmol/L | 68.1 [58.7; 78.4] | 69.5 [58.6; 78.7] | 67.9 [59.0; 78.4] | 67.7 [58.7; 78.0] | 0.243 | 0.856 |
| BUN, mmol/L | 5.0 [4.2; 5.9] | 5.0 [4.2; 5.9] | 4.9 [4.1; 5.9] | 5.0 [4.2; 5.9] | 0.745 | 0.895 |
| UA, μmol/L | 369 [309; 431] | 377 [320; 441] | 370 [307; 431] | 366 [307; 428] | 0.062 | 0.973 |
| TC, mmol/L | 4.5 [3.9; 5.1] | 4.4 [3.8; 5.1] | 4.5 [3.9; 5.1] | 4.5 [3.9; 5.2] | 0.116 | 0.723 |
| TG, mmol/L | 1.8 [1.3; 2.6] | 1.9 [1.3; 2.8] | 1.8 [1.3; 2.6] | 1.8 [1.7; 2.6] | 0.060 | 0.931 |
| HDLC, mmol/L | 0.9 [0.8; 1.1] | 0.9 [0.8; 1.0] | 0.9 [0.8; 1.1] | 0.9 [0.8; 1.1] | <0.001 | 0.958 |
| LDLC, mmol/L | 2.7 [2.2; 3.3] | 2.6 [2.2; 3.2] | 2.7 [2.2; 3.2] | 2.7 [2.2; 3.3] | 0.184 | 0.920 |
| Hypoglycemic drugs | 1461 (59.1%) | 249 (45.3%) | 475 (57.4%) | 737 (67.4%) | <0.001 | 0.862 |
| Lipid-lowering drugs | 2041 (82.6%) | 346 (62.9%) | 648 (78.4%) | 1047 (95.8%) | <0.001 | 0.912 |
| ACEI/ARB | 1926 (78.0%) | 350 (63.6%) | 614 (74.2%) | 962 (88.0%) | <0.001 | 0.731 |
| β | 1298 (52.6%) | 189 (34.4%) | 415 (50.2%) | 694 (63.5%) | <0.001 | 0.989 |
| CCBs | 2068 (83.7%) | 397 (72.2%) | 663 (80.2%) | 1008 (92.2%) | <0.001 | 0.520 |
| Diuretic | 1332 (53.9%) | 232 (42.2%) | 401 (48.5%) | 699 (64.0%) | <0.001 | 0.834 |
| Unadjusted Model | Model 1 * | Model 2 † | With IPTW ‡ | |||||
|---|---|---|---|---|---|---|---|---|
| HR (95%CI) | p | aHR (95%CI) | p | aHR (95%CI) | p | aHR (95%CI) § | p || | |
| MACCE | ||||||||
| Intermittent users | 1.40 (0.88–2.22) | 0.156 | 1.17 (0.74–1.86) | 0.503 | 1.13 (0.71–1.80) | 0.614 | 1.21 (0.68–2.14) | 0.522 |
| Persistent users | 2.79 (1.84–4.22) | <0.001 | 2.09 (1.37–3.18) | 0.001 | 1.95 (1.26–3.03) | 0.003 | 2.11 (1.23–3.63) | 0.007 |
| Ischemic events | ||||||||
| Intermittent users | 1.65 (1.00–2.72) | 0.052 | 1.37 (0.83–2.26) | 0.224 | 1.34 (0.80–2.22) | 0.266 | 1.46 (0.78–2.73) | 0.239 |
| Persistent users | 3.34 (2.12–5.27) | <0.001 | 2.47 (1.56–3.92) | <0.001 | 2.38 (1.47–3.84) | <0.001 | 2.58 (1.42–4.69) | 0.002 |
| Cerebrovascular events | ||||||||
| Intermittent users | 1.55 (0.94–2.57) | 0.088 | 1.28 (0.77–2.14) | 0.335 | 1.25 (0.75–2.09) | 0.398 | 1.50 (0.82–2.75) | 0.193 |
| Persistent users | 3.02 (1.91–4.78) | <0.001 | 2.26 (1.42–3.59) | 0.001 | 2.11 (1.30–3.42) | 0.002 | 2.55 (1.44–4.51) | 0.001 |
| Cerebral hemorrhage | ||||||||
| Intermittent users | 0.76 (0.20–2.83) | 0.682 | 0.79 (0.21–3.03) | 0.736 | 0.61 (0.15–2.44) | 0.484 | 0.48 (0.10–2.29) | 0.359 |
| Persistent users | 0.53 (0.14–1.99) | 0.351 | 0.58 (0.15–2.33) | 0.446 | 0.36 (0.09–1.54) | 0.170 | 0.33 (0.07–1.51) | 0.152 |
| Cerebral infarction | ||||||||
| Intermittent users | 1.81 (1.05–3.14) | 0.034 | 1.48 (0.85–2.57) | 0.168 | 1.46 (0.83–2.54) | 0.188 | 1.83 (0.95–3.52) | 0.072 |
| Persistent users | 3.58 (2.16–5.93) | <0.001 | 2.63 (1.58–4.38) | <0.001 | 2.52 (1.49–4.27) | 0.001 | 3.14 (1.69–5.84) | <0.001 |
| Cardiac events | ||||||||
| Intermittent users | 1.21 (0.37–4.03) | 0.751 | 1.15 (0.35–3.85) | 0.816 | 0.99 (0.29–3.34) | 0.984 | 0.64 (0.15–2.80) | 0.550 |
| Persistent users | 2.80 (0.98–8.04) | 0.055 | 2.38 (0.81–6.94) | 0.113 | 2.04 (0.65–6.34) | 0.220 | 1.43 (0.38–5.45) | 0.600 |
| MI | ||||||||
| Intermittent users | 1.75 (0.18–16.87) | 0.626 | 1.71 (0.18–16.62) | 0.645 | 1.67 (0.17–16.74) | 0.661 | 1.15 (0.11–12.45) | 0.910 |
| Persistent users | 3.73 (0.47–29.42) | 0.212 | 3.36 (0.41–27.18) | 0.256 | 3.73 (0.42–33.17) | 0.237 | 2.54 (0.31–20.53) | 0.383 |
| Revascularization | ||||||||
| Intermittent users | 1.22 (0.31–4.88) | 0.778 | 1.16 (0.29–4.67) | 0.834 | 0.96 (0.24–3.94) | 0.959 | 0.58 (0.10–3.29) | 0.536 |
| Persistent users | 3.33 (1.00–11.08) | 0.050 | 2.88 (0.85–9.81) | 0.090 | 2.33 (0.64–8.51) | 0.201 | 1.66 (0.35–7.82) | 0.523 |
| All-causer death | ||||||||
| Intermittent users | 0.59 (0.04–9.44) | 0.709 | 0.42 (0.03–6.95) | 0.546 | 0.53 (0.03–9.26) | 0.662 | 0.40 (0.01–10.73) | 0.583 |
| Persistent users | 1.56 (0.17–13.99) | 0.692 | 0.83 (0.09–7.88) | 0.872 | 1.50 (0.11–20.32) | 0.762 | 1.02 (0.06–16.17) | 0.991 |
| Gastrointestinal bleeding | ||||||||
| Intermittent users | 0.27 (0.09–0.77) | 0.014 | 0.24 (0.08–0.70) | 0.009 | 0.25 (0.09–0.74) | 0.013 | 0.31 (0.08–1.16) | 0.083 |
| Persistent users | 0.63 (0.30–1.35) | 0.235 | 0.53 (0.24–1.16) | 0.112 | 0.57 (0.24–1.34) | 0.194 | 0.66 (0.23–1.86) | 0.431 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, N.; Wen, W.; Cai, X.; Zhu, Q.; Hu, J.; Heizhati, M.; Yuan, Y.; Gan, L.; Dang, Y.; Yang, W.; et al. The Use of Aspirin Increases the Risk of Major Adverse Cardiac and Cerebrovascular Events in Hypertensive Patients with Obstructive Sleep Apnea for the Primary Prevention of Cardiovascular Disease: A Real-World Cohort Study. J. Clin. Med. 2022, 11, 7066. https://doi.org/10.3390/jcm11237066
Li N, Wen W, Cai X, Zhu Q, Hu J, Heizhati M, Yuan Y, Gan L, Dang Y, Yang W, et al. The Use of Aspirin Increases the Risk of Major Adverse Cardiac and Cerebrovascular Events in Hypertensive Patients with Obstructive Sleep Apnea for the Primary Prevention of Cardiovascular Disease: A Real-World Cohort Study. Journal of Clinical Medicine. 2022; 11(23):7066. https://doi.org/10.3390/jcm11237066
Chicago/Turabian StyleLi, Nanfang, Wen Wen, Xintian Cai, Qing Zhu, Junli Hu, Mulalibieke Heizhati, Yujuan Yuan, Lin Gan, Yujie Dang, Wenbo Yang, and et al. 2022. "The Use of Aspirin Increases the Risk of Major Adverse Cardiac and Cerebrovascular Events in Hypertensive Patients with Obstructive Sleep Apnea for the Primary Prevention of Cardiovascular Disease: A Real-World Cohort Study" Journal of Clinical Medicine 11, no. 23: 7066. https://doi.org/10.3390/jcm11237066