
Buccolingual Inclination of Second Molars in Untreated Adolescents and Adults with Near Normal Occlusion: A CBCT Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Size Calculation
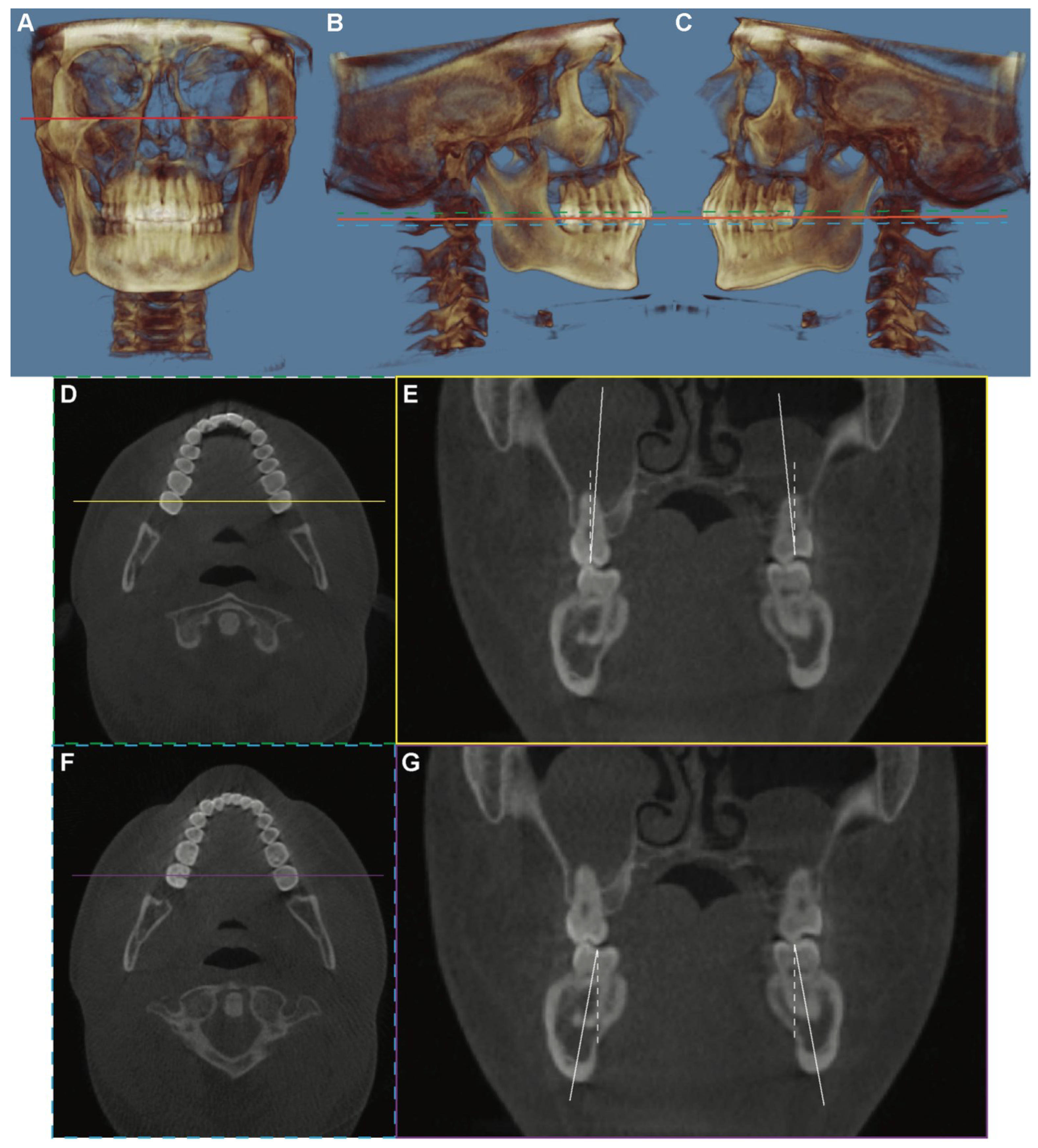
2.2. Imaging Analysis
2.3. Statistical Analysis
3. Results
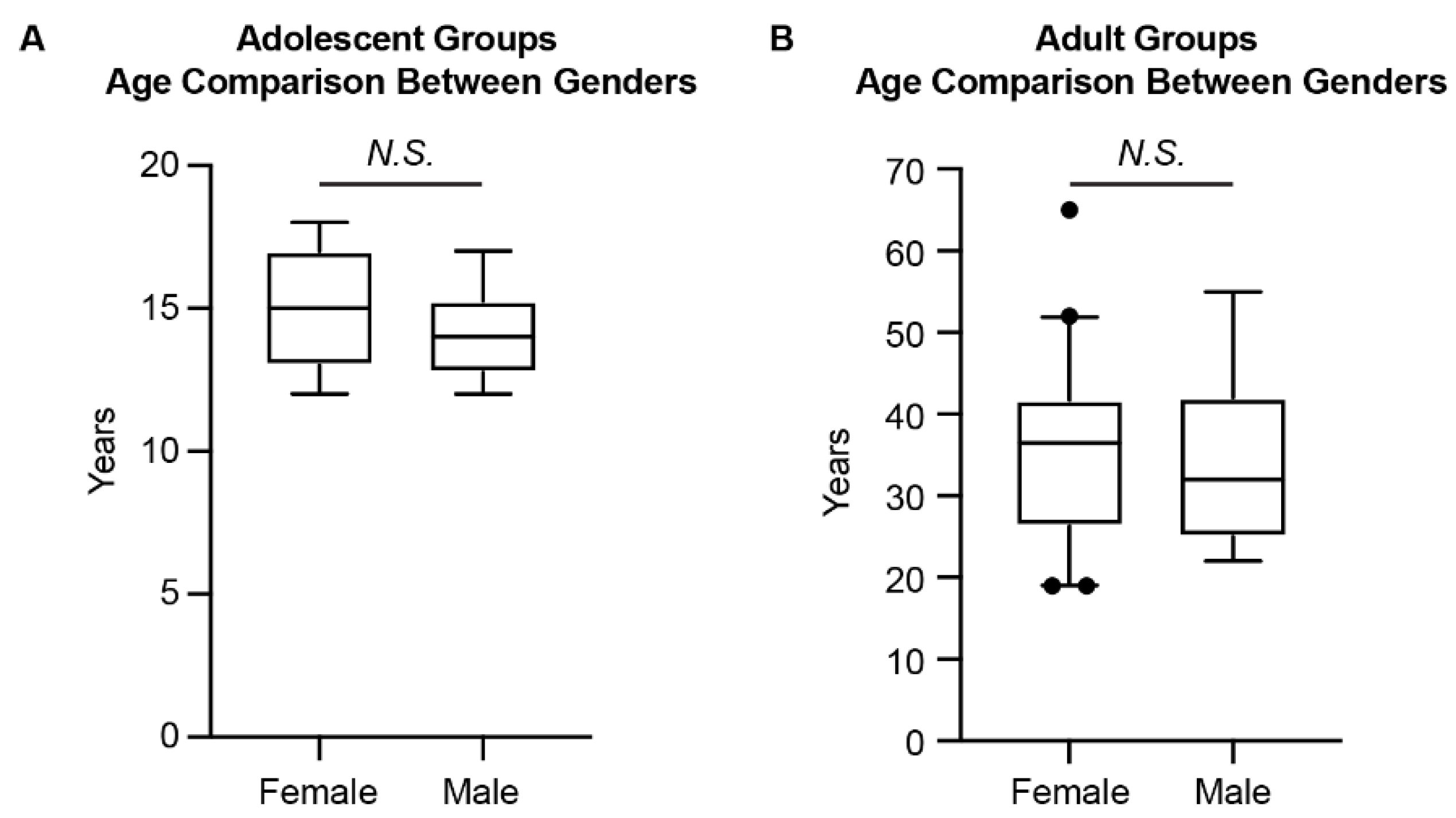
3.1. Patient Demographic Information
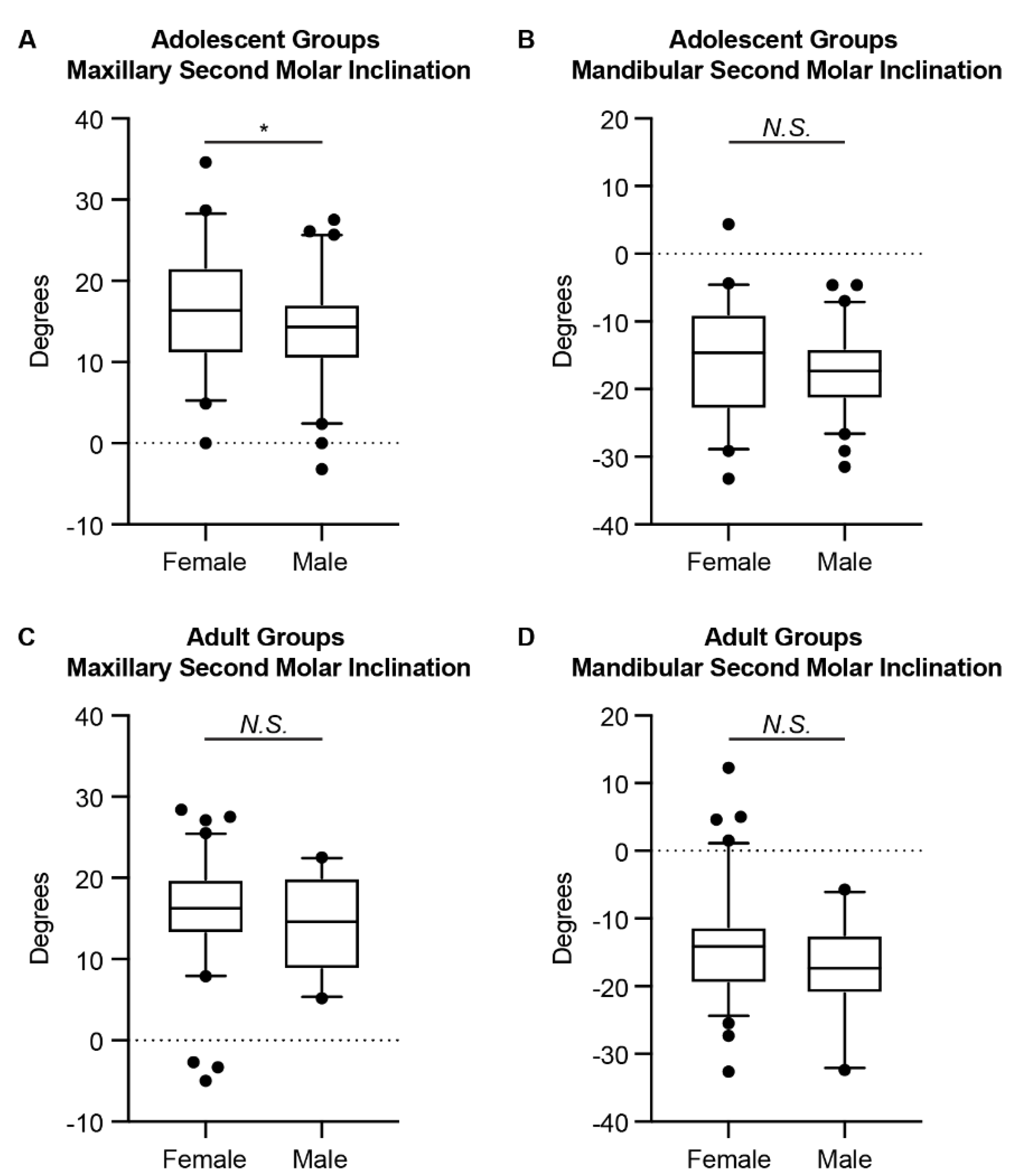
3.2. Differences in the Inclinations of the Second Molars between Genders
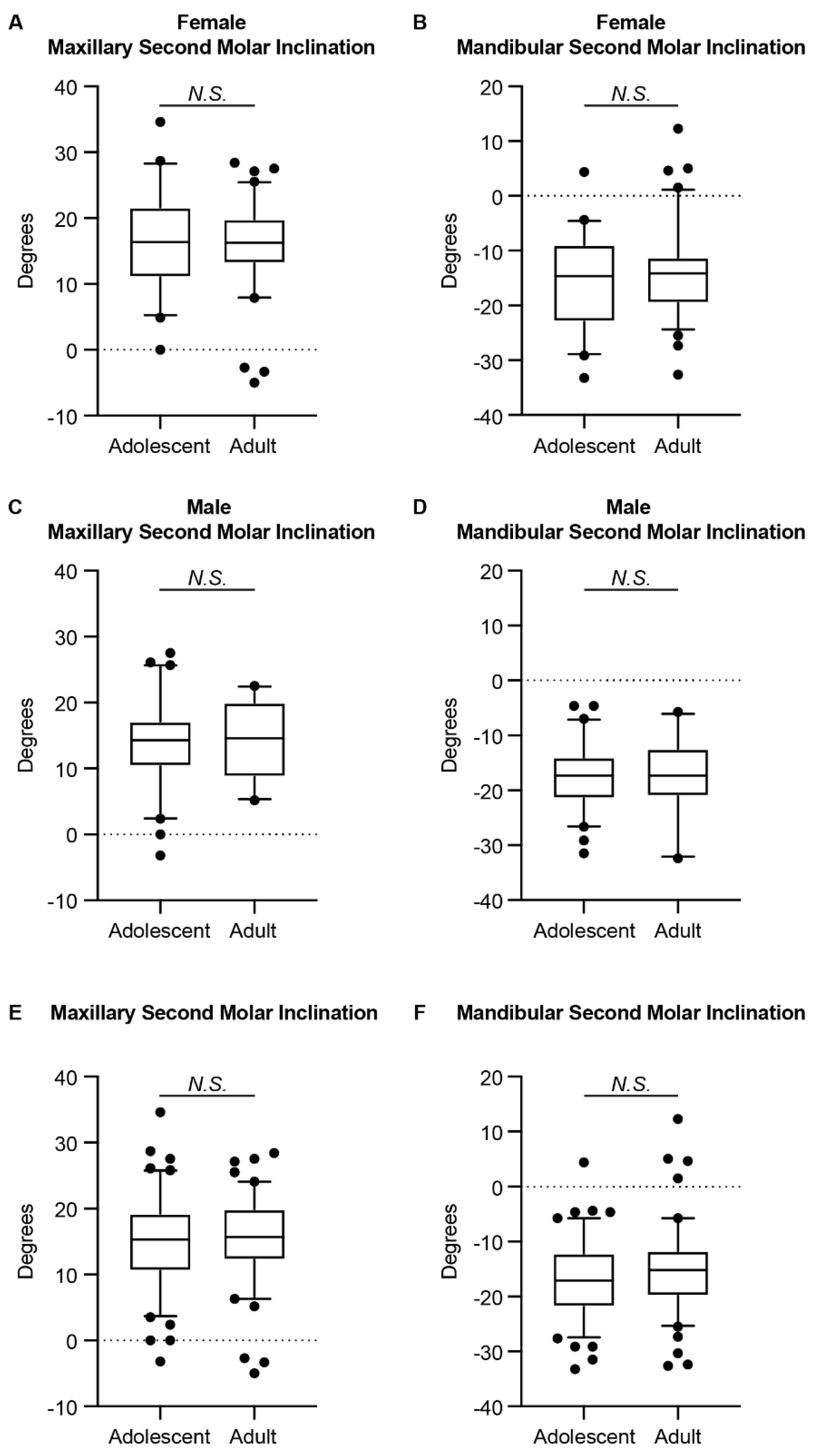
3.3. Differences in the Inclinations of the Second Molars between Adolescents and Adults
4. Discussion
5. Conclusions
- Maxillary second molars exhibited a buccal inclination of 15.30° in the Caucasian adolescent group and 15.70° in the Caucasian adult group.
- Mandibular second molars exhibited a lingual inclination of 17.05° in the Caucasian adolescent group and 15.20° in the Caucasian adult group.
- Female adolescents had more buccal inclination of the maxillary second molars and less lingual inclination of the mandibular second molars than male adolescents. There was no difference in the second molar inclinations between genders in adults.
- The amount of inclination of the second molars was similar in adolescent and adult groups.
- Clinically, a proper buccolingual inclination of the upper and lower second molars should be maintained.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wilson, G.H. A Manual of Dental Prosthetics; Lea & Febiger: Philaelphia, PA, USA, 1911. [Google Scholar]
- Dawson, P.E. Functional Occlusion: From TMJ to Smile Design; Elsevier Health Sciences: Amsterdam, The Netherlands, 2006. [Google Scholar]
- Okeson, J.P. Management of Temporomandibular Disorders and Occlusion—E-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Casko, J.S.; Vaden, J.L.; Kokich, V.G.; Damone, J.; James, R.D.; Cangialosi, T.J.; Riolo, M.L.; Owens, S.E., Jr.; Bills, E.D. Objective grading system for dental casts and panoramic radiographs. American Board of Orthodontics. Am. J. Orthod. Dentofac. Orthop. 1998, 114, 589–599. [Google Scholar] [CrossRef]
- Marshall, S.; Dawson, D.; Southard, K.A.; Lee, A.N.; Casko, J.S.; Southard, T.E. Transverse molar movements during growth. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 615–624. [Google Scholar] [CrossRef]
- Sayania, B.; Merchant, M.; Josephs, P.; Chung, C.H. Changes in the buccolingual inclination of first molars with growth in untreated subjects: A longitudinal study. Angle Orthod. 2017, 87, 681–687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Germane, N.; Bentley, B.E., Jr.; Isaacson, R.J. Three biologic variables modifying faciolingual tooth angulation by straight-wire appliances. Am. J. Orthod. Dentofac. Orthop 1989, 96, 312–319. [Google Scholar] [CrossRef]
- Li, C.; Lin, L.; Zheng, Z.; Chung, C.H. A User-Friendly Protocol for Mandibular Segmentation of CBCT Images for Superimposition and Internal Structure Analysis. J. Clin. Med. 2021, 10, 127. [Google Scholar] [CrossRef]
- Yang, B.; Chung, C.H. Buccolingual inclination of molars in untreated children and adults: A cone beam computed tomography study. Angle Orthod. 2019, 89, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Alkhatib, R.; Chung, C.H. Buccolingual inclination of first molars in untreated adults: A CBCT study. Angle Orthod. 2017, 87, 598–602. [Google Scholar] [CrossRef]
- Barrera, J.M.; Llamas, J.M.; Espinar, E.; Saenz-Ramirez, C.; Paredes, V.; Perez-Varela, J.C. Wilson maxillary curve analyzed by CBCT. A study on normocclusion and malocclusion individuals. Med. Oral Patol. Oral Cir. Bucal 2013, 18, e547–e552. [Google Scholar] [CrossRef]
- Kasai, K.; Kawamura, A. Correlation between buccolingual inclination and wear of mandibular teeth in ancient and modern Japanese. Arch. Oral Biol. 2001, 46, 269–273. [Google Scholar] [CrossRef]
- Aljarbou, F.A.; Aldosimani, M.; Althumairy, R.I.; Alhezam, A.A.; Aldawsari, A.I. An analysis of the first and second mandibular molar roots proximity to the inferior alveolar canal and cortical plates using cone beam computed tomography among the Saudi population. Saudi Med. J. 2019, 40, 189–194. [Google Scholar] [CrossRef]
- Saber, S.E.; Abu El Sadat, S.; Taha, A.; Nawar, N.N.; Abdel Azim, A. Anatomical Analysis of Mandibular Posterior Teeth using CBCT: An Endo-Surgical Perspective. Eur. Endod. J. 2021, 6, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Sendyk, M.; de Paiva, J.B.; Abrao, J.; Rino Neto, J. Correlation between buccolingual tooth inclination and alveolar bone thickness in subjects with Class III dentofacial deformities. Am. J. Orthod. Dentofac. Orthop. 2017, 152, 66–79. [Google Scholar] [CrossRef] [PubMed]
- Richman, C. Is gingival recession a consequence of an orthodontic tooth size and/or tooth position discrepancy? A paradigm shift. Compend. Contin. Educ. Dent. 2011, 32, e73–e79. [Google Scholar] [PubMed]
- Horiuchi, A.; Hotokezaka, H.; Kobayashi, K. Correlation between cortical plate proximity and apical root resorption. Am. J. Orthod. Dentofac. Orthop. 1998, 114, 311–318. [Google Scholar] [CrossRef]
- Janson, G.; Bombonatti, R.; Cruz, K.S.; Hassunuma, C.Y.; Del Santo, M., Jr. Buccolingual inclinations of posterior teeth in subjects with different facial patterns. Am. J. Orthod. Dentofac. Orthop. 2004, 125, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Shewinvanakitkul, W.; Hans, M.G.; Narendran, S.; Martin Palomo, J. Measuring buccolingual inclination of mandibular canines and first molars using CBCT. Orthod. Craniofac. Res. 2011, 14, 168–174. [Google Scholar] [CrossRef]
- Tsunori, M.; Mashita, M.; Kasai, K. Relationship between facial types and tooth and bone characteristics of the mandible obtained by CT scanning. Angle Orthod. 1998, 68, 557–562. [Google Scholar] [CrossRef]
- Golshah, A.; Rezaei, N.; Heshmati, S. Buccolingual Inclination of Canine and First and Second Molar Teeth and the Curve of Wilson in Different Sagittal Skeletal Patterns of Adults Using Cone-Beam Computed Tomography. Int. J. Dent. 2020, 2020, 8893778. [Google Scholar] [CrossRef]
- Hu, X.; Huang, X.; Gu, Y. Assessment of buccal and lingual alveolar bone thickness and buccolingual inclination of maxillary posterior teeth in patients with severe skeletal Class III malocclusion with mandibular asymmetry. Am. J. Orthod. Dentofac. Orthop. 2020, 157, 503–515. [Google Scholar] [CrossRef]
- Tong, H.; Kwon, D.; Shi, J.; Sakai, N.; Enciso, R.; Sameshima, G.T. Mesiodistal angulation and faciolingual inclination of each whole tooth in 3-dimensional space in patients with near-normal occlusion. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 604–617. [Google Scholar] [CrossRef]
- Tan, W.Y.; Ng, J.Z.L.; Ajit Bapat, R.; Vijaykumar Chaubal, T.; Kishor Kanneppedy, S. Evaluation of anatomic variations of mandibular lingual concavities from cone beam computed tomography scans in a Malaysian population. J. Prosthet. Dent. 2021, 125, 766.e1–766.e8. [Google Scholar] [CrossRef]
- Chang, C.; Liu, S.S.; Roberts, W.E. Primary failure rate for 1680 extra-alveolar mandibular buccal shelf mini-screws placed in movable mucosa or attached gingiva. Angle Orthod. 2015, 85, 905–910. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.J.; Choi, T.H.; Baik, H.S.; Park, Y.C.; Lee, K.J. Mandibular posterior anatomic limit for molar distalization. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Klinge, A.; Becktor, K.; Lindh, C.; Becktor, J.P. Craniofacial height in relation to cross-sectional maxillary and mandibular morphology. Prog. Orthod. 2017, 18, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, Y.; Penington, A.; Kilpatrick, N.; Hardiman, R.; Schneider, P.; Clement, J.; Claes, P.; Matthews, H. Quantification of mandibular sexual dimorphism during adolescence. J. Anat. 2019, 234, 709–717. [Google Scholar] [CrossRef]
- Vinay, G.; Mangala Gowri, S.R.; Anbalagan, J. Sex determination of human mandible using metrical parameters. J. Clin. Diagn. Res. 2013, 7, 2671–2673. [Google Scholar] [CrossRef]
- Ozturk, C.N.; Ozturk, C.; Bozkurt, M.; Uygur, H.S.; Papay, F.A.; Zins, J.E. Dentition, bone loss, and the aging of the mandible. Aesthet. Surg. J. 2013, 33, 967–974. [Google Scholar] [CrossRef] [Green Version]
- Cortella, S.; Shofer, F.S.; Ghafari, J. Transverse development of the jaws: Norms for the posteroanterior cephalometric analysis. Am. J. Orthod. Dentofac. Orthop. 1997, 112, 519–522. [Google Scholar] [CrossRef]
- Moyers, R.E.; van der Linden, F.P.G.M.; Riolo, M.L.; McNamara, J.A. Standards of Human Occlusal Development; Center for Human Growth and Development, University of Michigan: Ann Arbor, MI, USA, 1976. [Google Scholar]
- Okuyama, K.; Yanamoto, S.; Michi, Y.; Shibata, E.; Tsuchiya, M.; Yokokawa, M.; Naruse, T.; Tomioka, H.; Kuroshima, T.; Shimamoto, H.; et al. Multicenter retrospective analysis of clinicopathological features and prognosis of oral tongue squamous cell carcinoma in adolescent and young adult patients. Medicine 2021, 100, e27560. [Google Scholar] [CrossRef]
- Kim, Y.; Okuyama, K.; Michi, Y.; Ohyama, Y.; Uzawa, N.; Yamaguchi, S. Potential factors influencing the development of oral tongue squamous cell carcinoma in young mature patients: Lingual position of the mandibular second molar and narrow tongue space. Oncol. Lett. 2017, 14, 7339–7343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nanda, R. Biomechanics and Esthetic Strategies in Clinical Orthodontics; Elsevier Health Sciences: Amsterdam, The Netherlands, 2005. [Google Scholar]
- Ferrillo, M.; Curci, C.; Roccuzzo, A.; Migliario, M.; Invernizzi, M.; de Sire, A. Reliability of cervical vertebral maturation compared to hand-wrist for skeletal maturation assessment in growing subjects: A systematic review. J. Back Musculoskelet. Rehabil. 2021, 34, 925–936. [Google Scholar] [CrossRef] [PubMed]
- Szemraj, A.; Wojtaszek-Slominska, A.; Racka-Pilszak, B. Is the cervical vertebral maturation (CVM) method effective enough to replace the hand-wrist maturation (HWM) method in determining skeletal maturation?-A systematic review. Eur. J. Radiol. 2018, 102, 125–128. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Female | Male | Mann–Whitney U Test p-Value | |||||
|---|---|---|---|---|---|---|---|
| N | Median | Range (Min, Max) | N | Median | Range (Min, Max) | ||
| Adolescent (12–18 years) | 21 | 15.00 | (12, 18) | 30 | 14.00 | (12, 17) | 0.0525 |
| Adult (19–65 years) | 40 | 36.50 | (19, 65) | 11 | 32.00 | (22, 55) | 0.8081 |
| p-Value of Chi-Square Analysis for Gender Distribution | 0.0001 | ||||||
| Female | Male | Mann–Whitney U Test p-Value | ||||||
|---|---|---|---|---|---|---|---|---|
| N | Median | Range (Min, Max) | N | Median | Range (Min, Max) | |||
| Adolescent (12–18 years) | U7s | 42 | 16.35 | (0.00, 34.60) | 60 | 14.30 | (−3.20, 27.50) | 0.0354 |
| L7s | 42 | −14.65 | (−33.20, 4.40) | 60 | −17.30 | (−31.50, −4.60) | 0.0928 | |
| Adult (19–65 years) | U7s | 80 | 16.25 | (−5,00, 28.40) | 22 | 14.60 | (5.20, 22.50) | 0.1621 |
| L7s | 80 | −14.10 | (−32.60, 12.30) | 22 | −17.30 | (−32.40, −5.70) | 0.3615 | |
| Adolescent (12–18 Years) | Adult (19–65 Years) | Mann–Whitney U Test p-Value | ||||||
|---|---|---|---|---|---|---|---|---|
| N | Median | Range (Min, Max) | N | Median | Range (Min, Max) | |||
| Female | U7s | 42 | 16.35 | (0.00, 34.60) | 80 | 16.25 | (−5,00, 28.40) | 0.6376 |
| L7s | 42 | −14.65 | (−33.20, 4.40) | 80 | −14.10 | (−32.60, 12.30) | 0.8458 | |
| Male | U7s | 60 | 14.30 | (−3.20, 27.50) | 22 | 14.60 | (5.20, 22.50) | 0.8578 |
| L7s | 60 | −17.30 | (−31.50, −4.60) | 22 | −17.30 | (−32.40, −5.70) | 0.5763 | |
| Total | U7s | 102 | 15.30 | (−3.20, 34.60) | 102 | 15.70 | (-5.00, 28.40) | 0.3951 |
| L7s | 102 | −17.05 | (−33.20, 4.40) | 102 | −15.20 | (−32.60, 12.30) | 0.2218 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, C.; Dimitrova, B.; Boucher, N.S.; Chung, C.-H. Buccolingual Inclination of Second Molars in Untreated Adolescents and Adults with Near Normal Occlusion: A CBCT Study. J. Clin. Med. 2022, 11, 6629. https://doi.org/10.3390/jcm11226629
Li C, Dimitrova B, Boucher NS, Chung C-H. Buccolingual Inclination of Second Molars in Untreated Adolescents and Adults with Near Normal Occlusion: A CBCT Study. Journal of Clinical Medicine. 2022; 11(22):6629. https://doi.org/10.3390/jcm11226629
Chicago/Turabian StyleLi, Chenshuang, Boryana Dimitrova, Normand S. Boucher, and Chun-Hsi Chung. 2022. "Buccolingual Inclination of Second Molars in Untreated Adolescents and Adults with Near Normal Occlusion: A CBCT Study" Journal of Clinical Medicine 11, no. 22: 6629. https://doi.org/10.3390/jcm11226629