
Dose Optimization of Meropenem in Patients on Veno-Arterial Extracorporeal Membrane Oxygenation in Critically Ill Cardiac Patients: Pharmacokinetic/Pharmacodynamic Modeling
 and
and
Abstract
:1. Introduction
2. Methods
Ethical Aspects
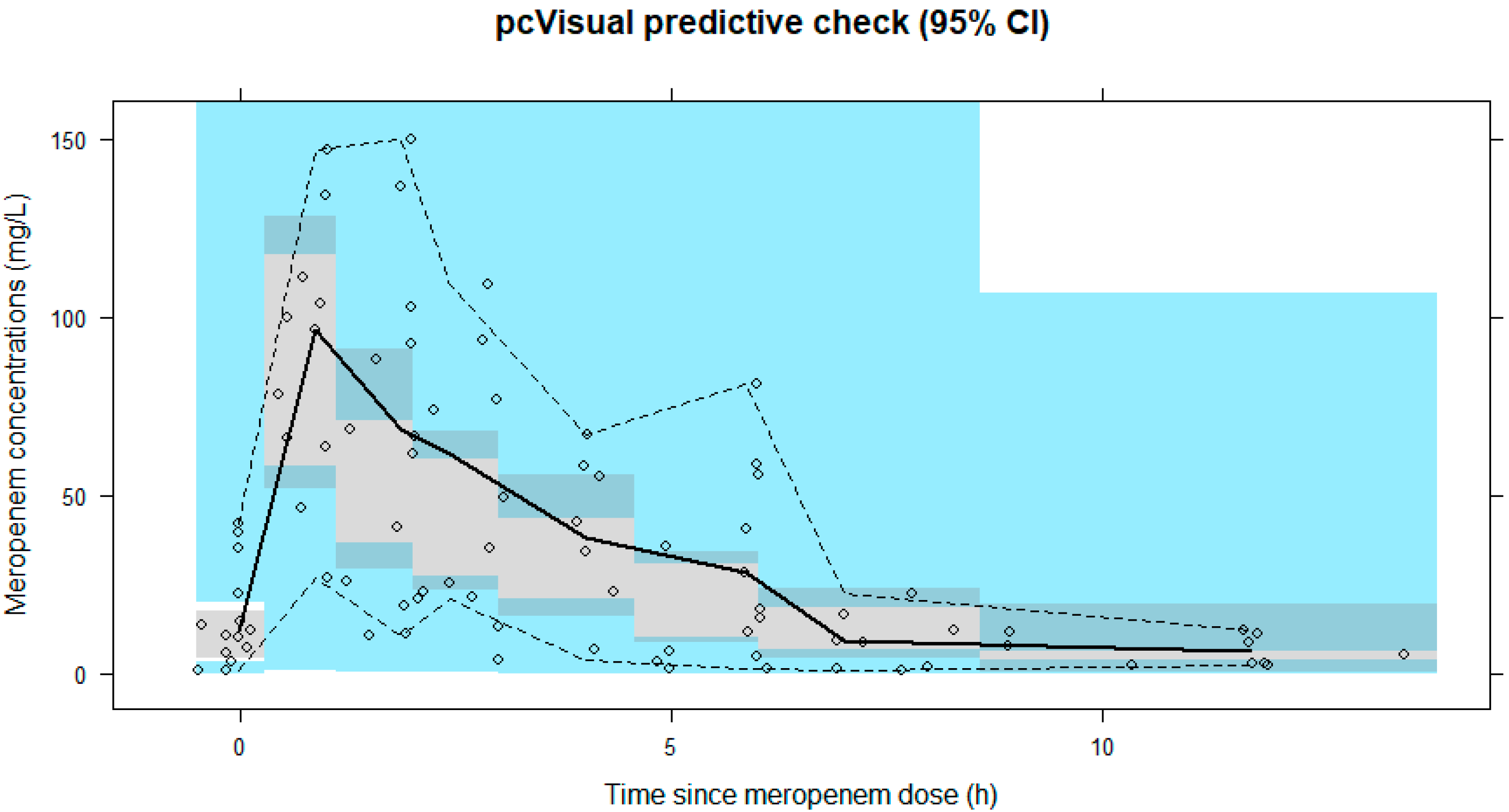
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Ouweneel, D.M.; Schotborgh, J.V.; Limpens, J.; Sjauw, K.D.; Engström, A.E.; Lagrand, W.K.; Cherpanath, T.G.V.; Driessen, A.H.G.; de Mol, B.; Henriques, J.P.S. Extracorporeal life support during cardiac arrest and cardiogenic shock: A systematic review and meta-analysis. Intensive Care Med. 2016, 42, 1922–1934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thiagarajan, R.R.; Barbaro, R.P.; Rycus, P.T.; McMullan, D.M.; Conrad, S.A.; Fortenberry, J.D.; Paden, M.L. Extracorporeal Life Support Organization Registry International Report 2016. ASAIO J. 2017, 63, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Loforte, A.; Marinelli, G.; Musumeci, F.; Folesani, G.; Pilato, E.; Martin Suarez, S.; Montalto, A.; Lilla Della Monica, P.; Grigioni, F.; Frascaroli, G.; et al. Extracorporeal membrane oxygenation support in refractory cardiogenic shock: Treatment strategies and analysis of risk factors. Artif. Organs 2014, 38, E129–E141. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Park, S.; Ko, H.H.; Ha, S.O.; Lee, S.H.; Kim, Y.K. Different characteristics of bloodstream infection during venoarterial and venovenous extracorporeal membrane oxygenation in adult patients. Sci. Rep. 2021, 11, 9498. [Google Scholar] [CrossRef] [PubMed]
- Aubron, C.; Cheng, A.C.; Pilcher, D.; Leong, T.; Magrin, G.; Cooper, D.J.; Scheinkestel, C.; Pellegrino, V. Infections acquired by adults who receive extracorporeal membrane oxygenation: Risk factors and outcome. Infect. Control. Hosp. Epidemiol. 2013, 34, 24–30. [Google Scholar] [CrossRef] [Green Version]
- Sherwin, J.; Heath, T.; Watt, K. Pharmacokinetics and Dosing of Anti-infective Drugs in Patients on Extracorporeal Membrane Oxygenation: A Review of the Current Literature. Clin. Ther. 2016, 38, 1976–1994. [Google Scholar] [CrossRef] [Green Version]
- Hahn, J.; Choi, J.H.; Chang, M.J. Pharmacokinetic changes of antibiotic, antiviral, antituberculosis and antifungal agents during extracorporeal membrane oxygenation in critically ill adult patients. J. Clin. Pharm. Ther. 2017, 42, 661–671. [Google Scholar] [CrossRef] [Green Version]
- Ha, M.A.; Sieg, A.C. Evaluation of Altered Drug Pharmacokinetics in Critically Ill Adults Receiving Extracorporeal Membrane Oxygenation. Pharmacotherapy 2017, 37, 221–235. [Google Scholar] [CrossRef]
- Shekar, K.; Roberts, J.A.; McDonald, C.I.; Ghassabian, S.; Anstey, C.; Wallis, S.C.; Mullany, D.V.; Fung, Y.L.; Fraser, J.F. Protein-bound drugs are prone to sequestration in the extracorporeal membrane oxygenation circuit: Results from an ex vivo study. Crit. Care 2015, 19, 164. [Google Scholar] [CrossRef] [Green Version]
- Shekar, K.; Roberts, J.A.; McDonald, C.I.; Fisquet, S.; Barnett, A.G.; Mullany, D.V.; Ghassabian, S.; Wallis, S.C.; Fung, Y.L.; Smith, M.T.; et al. Sequestration of drugs in the circuit may lead to therapeutic failure during extracorporeal membrane oxygenation. Crit. Care 2012, 16, R194. [Google Scholar] [CrossRef]
- Mousavi, S.; Levcovich, B.; Mojtahedzadeh, M. A systematic review on pharmacokinetic changes in critically ill patients: Role of extracorporeal membrane oxygenation. DARU 2011, 19, 312–321. [Google Scholar]
- Thiele, H.; Ohman, E.M.; de Waha-Thiele, S.; Zeymer, U.; Desch, S. Management of cardiogenic shock complicating myocardial infarction: An update 2019. Eur. Heart J. 2019, 40, 2671–2683. [Google Scholar] [CrossRef] [Green Version]
- Cheng, V.; Abdul-Aziz, M.H.; Roberts, J.A.; Shekar, K. Optimising drug dosing in patients receiving extracorporeal membrane oxygenation. J. Thorac. Dis. 2018, 10, S629–S641. [Google Scholar] [CrossRef]
- Abdul-Aziz, M.H.; Roberts, J.A. Antibiotic dosing during extracorporeal membrane oxygenation: Does the system matter? Curr. Opin. Anaesthesiol. 2020, 33, 71–82. [Google Scholar] [CrossRef]
- Hahn, J.; Min, K.L.; Kang, S.; Yang, S.; Park, M.S.; Wi, J.; Chang, M.J. Population Pharmacokinetics and Dosing Optimization of Piperacillin-Tazobactam in Critically Ill Patients on Extracorporeal Membrane Oxygenation and the Influence of Concomitant Renal Replacement Therapy. Microbiol. Spectr. 2021, 9, e0063321. [Google Scholar] [CrossRef]
- Hanberg, P.; Öbrink-Hansen, K.; Thorsted, A.; Bue, M.; Tøttrup, M.; Friberg, L.E.; Hardlei, T.F.; Søballe, K.; Gjedsted, J. Population Pharmacokinetics of Meropenem in Plasma and Subcutis from Patients on Extracorporeal Membrane Oxygenation Treatment. Antimicrob. Agents Chemother. 2018, 62, e02390-17. [Google Scholar] [CrossRef] [Green Version]
- Shekar, K.; Fraser, J.F.; Taccone, F.S.; Welch, S.; Wallis, S.C.; Mullany, D.V.; Lipman, J.; Roberts, J.A. The combined effects of extracorporeal membrane oxygenation and renal replacement therapy on meropenem pharmacokinetics: A matched cohort study. Crit. Care 2014, 18, 565. [Google Scholar] [CrossRef] [Green Version]
- Post, T.M.; Freijer, J.I.; Ploeger, B.A.; Danhof, M. Extensions to the visual predictive check to facilitate model performance evaluation. J. Pharmacokinet. Pharmacodyn. 2008, 35, 185–202. [Google Scholar] [CrossRef] [Green Version]
- Dosne, A.G.; Bergstrand, M.; Karlsson, M.O. An automated sampling importance resampling procedure for estimating parameter uncertainty. J. Pharmacokinet. Pharmacodyn. 2017, 44, 509–520. [Google Scholar] [CrossRef] [Green Version]
- Shekar, K.; Fraser, J.F.; Smith, M.T.; Roberts, J.A. Pharmacokinetic changes in patients receiving extracorporeal membrane oxygenation. J. Crit. Care 2012, 27, 741.e9–741.e18. [Google Scholar] [CrossRef]
- Wishart, D.S.; Feunang, Y.D.; Guo, A.C.; Lo, E.J.; Marcu, A.; Grant, J.R.; Sajed, T.; Johnson, D.; Li, C.; Sayeeda, Z.; et al. DrugBank 5.0: A major update to the DrugBank database for 2018. Nucleic Acids Res. 2018, 46, D1074–D1082. [Google Scholar] [CrossRef] [PubMed]
- Donadello, K.; Antonucci, E.; Cristallini, S.; Roberts, J.A.; Beumier, M.; Scolletta, S.; Jacobs, F.; Rondelet, B.; de Backer, D.; Vincent, J.L.; et al. β-Lactam pharmacokinetics during extracorporeal membrane oxygenation therapy: A case-control study. Int. J. Antimicrob. Agents 2015, 45, 278–282. [Google Scholar] [CrossRef] [PubMed]
- Kois, A.K.; Gluck, J.A.; Nicolau, D.P.; Kuti, J.L. Pharmacokinetics and Time above the MIC Exposure of Cefepime in Critically Ill Patients Receiving Extracorporeal Membrane Oxygenation (ECMO). Int. J. Antimicrob. Agents 2022, 60, 106603. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Jang, J.Y.; Hahn, J.; Kim, D.; Lee, J.Y.; Min, K.L.; Yang, S.; Wi, J.; Chang, M.J. Dose Optimization of Cefpirome Based on Population Pharmacokinetics and Target Attainment during Extracorporeal Membrane Oxygenation. Antimicrob. Agents Chemother. 2020, 64, e00249-20. [Google Scholar] [CrossRef] [PubMed]
- Cheng, V.; Abdul-Aziz, M.H.; Burrows, F.; Buscher, H.; Cho, Y.J.; Corley, A.; Gilder, E.; Kim, H.S.; Lim, S.Y.; McGuinness, S.; et al. Population Pharmacokinetics and Dosing Simulations of Ceftriaxone in Critically Ill Patients Receiving Extracorporeal Membrane Oxygenation (An ASAP ECMO Study). Clin. Pharmacokinet. 2022, 61, 847–856. [Google Scholar] [CrossRef]
- Craig, W.A. Interrelationship between pharmacokinetics and pharmacodynamics in determining dosage regimens for broad-spectrum cephalosporins. Diagn. Microbiol. Infect. Dis. 1995, 22, 89–96. [Google Scholar] [CrossRef]
- Nielsen, E.I.; Cars, O.; Friberg, L.E. Pharmacokinetic/pharmacodynamic (PK/PD) indices of antibiotics predicted by a semimechanistic PKPD model: A step toward model-based dose optimization. Antimicrob. Agents Chemother. 2011, 55, 4619–4630. [Google Scholar] [CrossRef] [Green Version]
- Onufrak, N.J.; Forrest, A.; Gonzalez, D. Pharmacokinetic and Pharmacodynamic Principles of Anti-infective Dosing. Clin. Ther. 2016, 38, 1930–1947. [Google Scholar] [CrossRef] [Green Version]
- Kristoffersson, A.N.; David-Pierson, P.; Parrott, N.J.; Kuhlmann, O.; Lave, T.; Friberg, L.E.; Nielsen, E.I. Simulation-Based Evaluation of PK/PD Indices for Meropenem Across Patient Groups and Experimental Designs. Pharm. Res. 2016, 33, 1115–1125. [Google Scholar] [CrossRef]
- Drusano, G.L. Prevention of resistance: A goal for dose selection for antimicrobial agents. Clin. Infect. Dis. 2003, 36, S42–S50. [Google Scholar] [CrossRef]
- Li, C.; Du, X.; Kuti, J.L.; Nicolau, D.P. Clinical pharmacodynamics of meropenem in patients with lower respiratory tract infections. Antimicrob. Agents Chemother. 2007, 51, 1725–1730. [Google Scholar] [CrossRef]
- Roberts, J.A.; Paul, S.K.; Akova, M.; Bassetti, M.; De Waele, J.J.; Dimopoulos, G.; Kaukonen, K.M.; Koulenti, D.; Martin, C.; Montravers, P.; et al. DALI: Defining antibiotic levels in intensive care unit patients: Are current β-lactam antibiotic doses sufficient for critically ill patients? Clin. Infect. Dis. 2014, 58, 1072–1083. [Google Scholar] [CrossRef]
- Huttner, A.; Harbarth, S.; Hope, W.W.; Lipman, J.; Roberts, J.A. Therapeutic drug monitoring of the β-lactam antibiotics: What is the evidence and which patients should we be using it for? J. Antimicrob. Chemother. 2015, 70, 3178–3183. [Google Scholar] [CrossRef] [Green Version]
- Roberts, J.A.; Ulldemolins, M.; Roberts, M.S.; McWhinney, B.; Ungerer, J.; Paterson, D.L.; Lipman, J. Therapeutic drug monitoring of beta-lactams in critically ill patients: Proof of concept. Int. J. Antimicrob. Agents 2010, 36, 332–339. [Google Scholar] [CrossRef]
- Mouton, J.W.; Vinks, A.A. Continuous infusion of beta-lactams. Curr. Opin. Crit. Care 2007, 13, 598–606. [Google Scholar] [CrossRef]
- Mohd Hafiz, A.A.; Staatz, C.E.; Kirkpatrick, C.M.; Lipman, J.; Roberts, J.A. Continuous infusion vs. bolus dosing: Implications for beta-lactam antibiotics. Minerva Anestesiol. 2012, 78, 94–104. [Google Scholar]
- Bauer, K.A.; West, J.E.; O’Brien, J.M.; Goff, D.A. Extended-infusion cefepime reduces mortality in patients with Pseudomonas aeruginosa infections. Antimicrob. Agents Chemother. 2013, 57, 2907–2912. [Google Scholar] [CrossRef] [Green Version]
- Kuti, J.L.; Nightingale, C.H.; Knauft, R.F.; Nicolau, D.P. Pharmacokinetic properties and stability of continuous-infusion meropenem in adults with cystic fibrosis. Clin. Ther. 2004, 26, 493–501. [Google Scholar] [CrossRef]
- Roberts, J.A.; Kirkpatrick, C.M.; Roberts, M.S.; Robertson, T.A.; Dalley, A.J.; Lipman, J. Meropenem dosing in critically ill patients with sepsis and without renal dysfunction: Intermittent bolus versus continuous administration? Monte Carlo dosing simulations and subcutaneous tissue distribution. J. Antimicrob. Chemother. 2009, 64, 142–150. [Google Scholar] [CrossRef] [Green Version]
- Berthoin, K.; Le Duff, C.S.; Marchand-Brynaert, J.; Carryn, S.; Tulkens, P.M. Stability of meropenem and doripenem solutions for administration by continuous infusion. J. Antimicrob. Chemother. 2010, 65, 1073–1075. [Google Scholar] [CrossRef] [Green Version]
- Patel, P.R.; Cook, S.E. Stability of meropenem in intravenous solutions. Am. J. Health Syst. Pharm. 1997, 54, 412–421. [Google Scholar] [CrossRef] [PubMed]
- Viaene, E.; Chanteux, H.; Servais, H.; Mingeot-Leclercq, M.P.; Tulkens, P.M. Comparative stability studies of antipseudomonal beta-lactams for potential administration through portable elastomeric pumps (home therapy for cystic fibrosis patients) and motor-operated syringes (intensive care units). Antimicrob. Agents Chemother. 2002, 46, 2327–2332. [Google Scholar] [CrossRef] [PubMed]
- Venugopalan, V.; Manigaba, K.; Borgert, S.J.; Cope, J.; Peloquin, C.A.; Klinker, K.P. Training a Drug to Do New Tricks: Insights on Stability of Meropenem Administered as a Continuous Infusion. Microbiol. Insights 2018, 11, 1178636118804549. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| ECMO | Patient No. * | Age Range (yr) | Sex | Wt (kg) | Ht (m) | Diagnosis | SCr (mg/dL) | CRRT | eGFR (mL/min/1.73 m2) | APACHE II Score | Length of Hospital Stay (Days) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| On | 1 | 45–49 | M | 74.6 | 1.73 | Acute MI | na # | yes | na # | 34 | 15 |
| 2 | 50–54 | M | 74.6 | 1.70 | Acute MI, | na # | yes | na # | 32 | 27 | |
| 3 | 50–54 | M | 82.9 | 1.68 | Acute MI | na # | yes | na # | 44 | 40 | |
| 4 | 55–59 | F | 69.9 | 1.64 | Acute MI | na # | yes | na # | 30 | 200 | |
| 5 | 70–74 | M | 93.3 | 1.70 | Acute MI | na # | yes | na # | 36 | 21 | |
| 6 | 50–59 | M | 53.1 | 1.68 | Acute MI | 1.06 | no | 76.5 | 29 | 36 | |
| Off | 4 * | 55–59 | F | 67.4 | 1.64 | 1.2 | no | 49.6 | 30 | 200 | |
| 6 * | 55–59 | M | 53.1 | 1.68 | 0.88 | no | 94.9 | 29 | 36 | ||
| 7 | 50–54 | F | 48.2 | 1.46 | Acute MI | na # | yes | na # | 37 | 75 | |
| 8 | 75–79 | M | 53.9 | 1.60 | Acute MI | na # | yes | na # | 40 | 75 | |
| 9 | 45–49 | M | 61.1 | 1.72 | Acute MI | 1.3 | no | 64.3 | 22 | 21 | |
| 10 | 55–59 | F | 60.0 | 1.62 | VF arrest | 0.5 | no | 127.3 | 30 | 29 | |
| 11 | 55–59 | M | 77.5 | 1.68 | Acute MI, VF arrest | 2.0 | no | 36.5 | 28 | 37 | |
| 12 | 50–54 | M | 63.0 | 1.62 | VF arrest | 0.7 | no | 120.4 | 26 | 36 | |
| 13 | 65–69 | M | 67.4 | 1.68 § | Acute MI | 1.3 | no | 60.3 | 14 | 23 | |
| 55 (53–58) | 67.4 (57–74.6) | 1.68 (1.63–1.70) | 1.2 (0.7–1.56) | 70.4 (57.6–101.3) | 30 (28.5–35) | 36 (25–57.5) |
| Parameter | Base Model | Final Model | |
|---|---|---|---|
| Population Estimate (RSE) | Population Estimate (RSE) | SIR Median (2.5th–97.5th Percentile) | |
| Fixed effects (θ) | |||
| CL (L/h) | 2.65 (32%) | 3.79 (26%) | 3.77 (2.69–5.37) |
| Central volume of distribution, V1 (L) | 2.53 (21%) | 2.4 (38%) | 2.76 (0.59–4.84) |
| Peripheral volume of distribution, V2 (L) | 9.61 (38%) | 8.56 (22%) | 8.36 (5.59–12.93) |
| Intercompartmental clearance, Q (L/h) | 20.8 (9%) | 21.3 (17%) | 19.94 (9.37–33.41) |
| θCRRT on CL | - | 0.44 (30%) | 0.45 (0.29–0.62) |
| Random effects (% CV) | |||
| Interindividual variability (ω2) | |||
| CL | 69.4 (36%) | 47.1 (49%) | 49.2 (32.2–74.2) |
| V2 | 61 (103%) | 44 (154%) | 51.1 (7.7–108) |
| Residual unexplained variability (σ2) | 49.7 (18%) | 47.3 (21%) | 49.0 (40.9–60.2) |
| Target | Normal Therapy (40% fT > MIC) | More Aggressive Therapy (100% fT > MIC) | ||
|---|---|---|---|---|
| For Susceptible Pathogens (MIC = 2 mg/L) | For Resistant Pathogens (MIC = 8 mg/L) | For Susceptible Pathogens (MIC = 2 mg/L) | For resistant Pathogens (MIC = 8 mg/L) | |
| without CRRT | 1–2 g q8h II 0.5 g q8h EIs or CI | 1–2 g q8h II 0.5 g q8h EIs or CI | 1–2 g q8h EIs or CI | 2 g q8h EI over 6 h or CI |
| with CRRT | 1 g q12h II 0.5 g q8h II 0.5 g q8h EIs or CI | 1 g q12h II 0.5 g q8h II 0.5 g q8h EIs or CI | 1 g q12h II 0.5 g q8h II 0.5 g q8h EIs or CI | 1 g q8h EIs 0.5–1 g q8h CI |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, S.; Yang, S.; Hahn, J.; Jang, J.Y.; Min, K.L.; Wi, J.; Chang, M.J. Dose Optimization of Meropenem in Patients on Veno-Arterial Extracorporeal Membrane Oxygenation in Critically Ill Cardiac Patients: Pharmacokinetic/Pharmacodynamic Modeling. J. Clin. Med. 2022, 11, 6621. https://doi.org/10.3390/jcm11226621
Kang S, Yang S, Hahn J, Jang JY, Min KL, Wi J, Chang MJ. Dose Optimization of Meropenem in Patients on Veno-Arterial Extracorporeal Membrane Oxygenation in Critically Ill Cardiac Patients: Pharmacokinetic/Pharmacodynamic Modeling. Journal of Clinical Medicine. 2022; 11(22):6621. https://doi.org/10.3390/jcm11226621
Chicago/Turabian StyleKang, Soyoung, Seungwon Yang, Jongsung Hahn, June Young Jang, Kyoung Lok Min, Jin Wi, and Min Jung Chang. 2022. "Dose Optimization of Meropenem in Patients on Veno-Arterial Extracorporeal Membrane Oxygenation in Critically Ill Cardiac Patients: Pharmacokinetic/Pharmacodynamic Modeling" Journal of Clinical Medicine 11, no. 22: 6621. https://doi.org/10.3390/jcm11226621