
Relation of Gender to the Occurrence of AKI in STEMI Patients

Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. AKI-Related Definitions
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics and Effect of Gender on AKI
3.2. Gender as an Independently Associated Factor for AKI
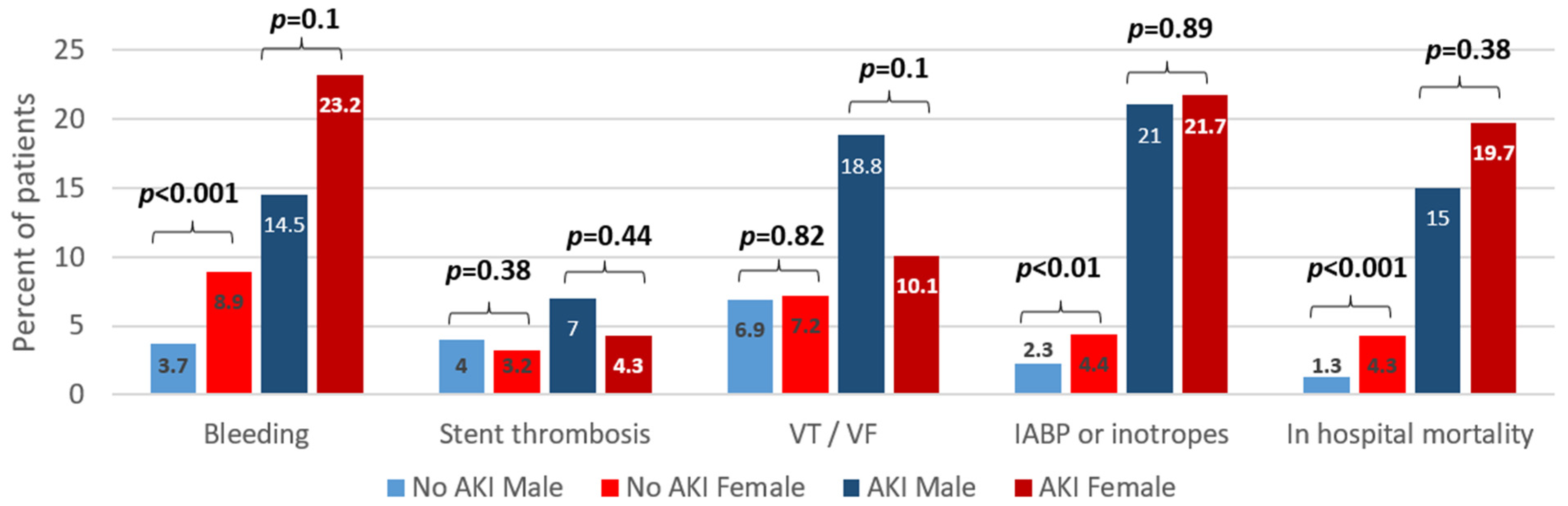
3.3. Effect of Gender and AKI on In-Hospital Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kutty, R.S.; Jones, N.; Moorjani, N. Mechanical Complications of Acute Myocardial Infarction. Cardiol. Clin. 2013, 31, 519–531. [Google Scholar] [CrossRef] [PubMed]
- Manoukian, S.V. Predictors and Impact of Bleeding Complications in Percutaneous Coronary Intervention, Acute Coronary Syndromes, and ST-Segment Elevation Myocardial Infarction. Am. J. Cardiol. 2009, 104 (Suppl. S5), 9C–15C. [Google Scholar] [CrossRef] [PubMed]
- Widimsky, P.; Wijns, W.; Fajadet, J.; De Belder, M.; Knot, J.; Aaberge, L.; Andrikopoulos, G.; Baz, J.A.; Betriu, A.; Claeys, M.; et al. Reperfusion Therapy for ST Elevation Acute Myocardial Infarction in Europe: Description of the Current Situation in 30 Countries. Eur. Heart J. 2010, 31, 943–957. [Google Scholar] [CrossRef] [Green Version]
- Busch, S.V.; Jensen, S.E.; Rosenberg, J.; Gögenur, I. Prevention of Contrast-Induced Nephropathy in STEMI Patients Undergoing Primary Percutaneous Coronary Intervention: A Systematic Review. J. Interv. Cardiol. 2013, 26, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Nanna, M.G.; Hajduk, A.M.; Krumholz, H.M.; Murphy, T.E.; Dreyer, R.P.; Alexander, K.P.; Geda, M.; Tsang, S.; Welty, F.K.; Safdar, B.; et al. Sex-Based Differences in Presentation, Treatment, and Complications Among Older Adults Hospitalized for Acute Myocardial Infarction. Circ. Cardiovasc. Qual. Outcomes 2019, 12, e005691. [Google Scholar] [CrossRef]
- Vaccarino, V.; Parsons, L.; Every, N.R.; Barron, H.V.; Krumholz, H.M. Sex-Based Differences in Early Mortality after Myocardial Infarction. N. Engl. J. Med. 1999, 341, 217–225. [Google Scholar] [CrossRef]
- Gan, S.C.; Beaver, S.K.; Houck, P.M.; MacLehose, R.F.; Lawson, H.W.; Chan, L. Treatment of Acute Myocardial Infarction and 30-Day Mortality among Women and Men. N. Engl. J. Med. 2000, 343, 8–15. [Google Scholar] [CrossRef]
- D’Ascenzo, F.; Gonella, A.; Quadri, G.; Longo, G.; Biondi-Zoccai, G.; Moretti, C.; Omedè, P.; Sciuto, F.; Gaita, F.; Sheiban, I. Comparison of Mortality Rates in Women Versus Men Presenting With ST-Segment Elevation Myocardial Infarction. Am. J. Cardiol. 2011, 107, 651–654. [Google Scholar] [CrossRef]
- Milcent, C.; Dormont, B.; Durand-Zaleski, I.; Steg, P.G. Gender Differences in Hospital Mortality and Use of Percutaneous Coronary Intervention in Acute Myocardial Infarction. Circulation 2007, 115, 833–839. [Google Scholar] [CrossRef] [Green Version]
- Berger, J.S.; Elliott, L.; Gallup, D.; Roe, M.; Granger, C.B.; Armstrong, P.W.; Simes, R.J.; White, H.D.; Van de Werf, F.; Topol, E.J.; et al. Sex Differences in Mortality Following Acute Coronary Syndromes. JAMA 2009, 302, 874–882. [Google Scholar] [CrossRef]
- Shacham, Y.; Topilsky, Y.; Leshem-Rubinow, E.; Laufer-Perl, M.; Keren, G.; Roth, A.; Steinvil, A.; Arbel, Y. Comparison of Left Ventricular Function Following First ST-Segment Elevation Myocardial Infarction Treated with Primary Percutaneous Coronary Intervention in Men Versus Women. Am. J. Cardiol. 2014, 113, 1941–1946. [Google Scholar] [CrossRef] [PubMed]
- Laufer-Perl, M.; Shacham, Y.; Letourneau-Shesaf, S.; Priesler, O.; Keren, G.; Roth, A.; Steinvil, A. Gender-Related Mortality and In-Hospital Complications Following ST-Segment Elevation Myocardial Infarction: Data from a Primary Percutaneous Coronary Intervention Cohort. Clin. Cardiol. 2015, 38, 145–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jneid, H.; Fonarow, G.; Cannon, C.P.; Hernandez, A.F.; Palacios, I.F.; Maree, A.; Wells, Q.; Bozkurt, B.; LaBresh, K.A.; Liang, L.; et al. Sex Differences in Medical Care and Early Death After Acute Myocardial Infarction. Circulation 2008, 118, 2803–2810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chertow, G.M.; Burdick, E.; Honour, M.; Bonventre, J.V.; Bates, D.W. Acute Kidney Injury, Mortality, Length of Stay, and Costs in Hospitalized Patients. JASN 2005, 16, 3365–3370. [Google Scholar] [CrossRef] [Green Version]
- Chawla, L.S.; Amdur, R.L.; Shaw, A.D.; Faselis, C.; Palant, C.E.; Kimmel, P.L. Association between AKI and Long-Term Renal and Cardiovascular Outcomes in United States Veterans. CJASN 2014, 9, 448–456. [Google Scholar] [CrossRef] [Green Version]
- Hayıroğlu, M.İ.; Bozbeyoglu, E.; Yıldırımtürk, Ö.; Tekkeşin, A.İ.; Pehlivanoğlu, S. Effect of acute kidney injury on long-term mortality in patients with ST-segment elevation myocardial infarction complicated by cardiogenic shock who underwent primary percutaneous coronary intervention in a high-volume tertiary center. Turk. Kardiyol. Dern. Ars. 2020, 48, 1–9. [Google Scholar] [CrossRef]
- Çinar, T.; Hayiroğlu, M.; Şeker, M.; Doğan, S.; Çiçek, V.; Öz, A.; Uzun, M.; Orhan, A.L. The predictive value of age, creatinine, ejection fraction score for in-hospital mortality in patients with cardiogenic shock. Coron. Artery Dis. 2019, 30, 569–574. [Google Scholar] [CrossRef]
- Schmucker, J.; Fach, A.; Becker, M.; Seide, S.; Bünger, S.; Zabrocki, R.; Fiehn, E.; Würmann-Busch, B.; Pohlabeln, H.; Günther, K.; et al. Predictors of acute kidney injury in patients admitted with ST-elevation myocardial infarction—Results from the Bremen STEMI-Registry. Eur. Heart J. Acute Cardiovasc. Care 2018, 7, 710–722. [Google Scholar] [CrossRef]
- Marenzi, G.; Cosentino, N.; Bartorelli, A.L. Acute kidney injury in patients with acute coronary syndromes. Heart 2015, 101, 1778–1785. [Google Scholar] [CrossRef]
- Shacham, Y.; Steinvil, A.; Arbel, Y. Acute kidney injury among ST elevation myocardial infarction patients treated by primary percutaneous coronary intervention: A multifactorial entity. J. Nephrol. 2016, 29, 169–174. [Google Scholar] [CrossRef]
- Güzel, C.; Yeşiltaş, S.; Daşkaya, H.; Uysal, H.; Sümer, I.; Türkay, M. The effect of gender on acute kidney injury developing in the intensive care unit. Hippokratia 2019, 23, 126–130. [Google Scholar] [PubMed]
- Loutradis, C.; Pickup, L.; Law, J.P.; Dasgupta, I.; Townend, J.N.; Cockwell, P.; Sharif, A.; Sarafidis, P.; Ferro, C.J. Acute kidney injury is more common in men than women after accounting for socioeconomic status, ethnicity, alcohol intake and smoking history. Biol. Sex Differ. 2021, 12, 30. [Google Scholar] [CrossRef] [PubMed]
- Ibanez, B.; James, S. The 2017 ESC STEMI Guidelines. Eur. Heart J. 2018, 39, 79–82. [Google Scholar] [CrossRef] [Green Version]
- Pugliese, G.; Solini, A.; Bonora, E.; Orsi, E.; Zerbini, G.; Giorgino, F.; Cavalot, F.; Pontiroli, A.E.; Baroni, M.G.; Morano, S.; et al. The Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation provides a better definition of cardiovascular burden associated with CKD than the Modification of Diet in Renal Disease (MDRD) Study formula in subjects with type 2 diabetes. Atherosclerosis 2011, 218, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Khwaja, A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin. Pract. 2012, 120, c179–c184. [Google Scholar] [CrossRef]
- Bhatraju, P.K.; Zelnick, L.R.; Chinchilli, V.M.; Moledina, D.G.; Coca, S.G.; Parikh, C.R.; Garg, A.X.; Hsu, C.-Y.; Go, A.S.; Liu, K.D.; et al. Association Between Early Recovery of Kidney Function After Acute Kidney Injury and Long-term Clinical Outcomes. JAMA Netw. Open 2020, 3, e202682. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H. Differences between men and women with chronic kidney disease. Nihon Rinsho Jpn. J. Clin. Med. 2015, 73, 629–633. [Google Scholar]
- Silbiger, S.R.; Neugarten, J. The Role of Gender in the Progression of Renal Disease. Adv. Ren. Replace. Ther. 2003, 10, 3–14. [Google Scholar] [CrossRef]
- Jousilahti, P.; Vartiainen, E.; Tuomilehto, J.; Puska, P. Sex, Age, Cardiovascular Risk Factors, and Coronary Heart Disease. Circulation 1999, 99, 1165–1172. [Google Scholar] [CrossRef] [Green Version]
- Neugarten, J.; Golestaneh, L. Female sex reduces the risk of hospital-associated acute kidney injury: A meta-analysis. BMC Nephrol. 2018, 19, 314. [Google Scholar] [CrossRef]
- Pickering, J.W.; Blunt, I.R.H.; Than, M.P. Acute Kidney Injury and mortality prognosis in Acute Coronary Syndrome patients: A meta-analysis. Nephrology 2018, 23, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Meng, Z.; Zhao, Y.; Zheng, X.; He, Y. The Relationship Between AKI in Patients with STEMI and Short-Term Mortality: A Propensity Score Matching Analysis. Angiology 2021, 72, 733–739. [Google Scholar] [CrossRef] [PubMed]
- Gnavi, R.; Rusciani, R.; Dalmasso, M.; Giammaria, M.; Anselmino, M.; Roggeri, D.P.; Roggeri, A. Gender, socioeconomic position, revascularization procedures and mortality in patients presenting with STEMI and NSTEMI in the era of primary PCI. Differences or inequities? Int. J. Cardiol. 2014, 176, 724–730. [Google Scholar] [CrossRef] [PubMed]
- Figtree, G.A.; Vernon, S.T.; Hadziosmanovic, N.; Sundström, J.; Alfredsson, J.; Arnott, C.; Delatour, V.; Leósdóttir, M.; Hagström, E. Mortality in STEMI patients without standard modifiable risk factors: A sex-disaggregated analysis of SWEDEHEART registry data. Lancet 2021, 397, 1085–1094. [Google Scholar] [CrossRef]
- Terkelsen, C.J.; Sørensen, J.T.; Maeng, M.; Jensen, L.O.; Tilsted, H.-H.; Trautner, S.; Vach, W.; Johnsen, S.P.; Thuesen, L.; Lassen, J.F. System Delay and Mortality Among Patients with STEMI Treated With Primary Percutaneous Coronary Intervention. JAMA 2010, 304, 763–771. [Google Scholar] [CrossRef] [Green Version]
- Granger, C.B.; Goldberg, R.J.; Dabbous, O.; Pieper, K.S.; Eagle, K.A.; Cannon, C.P.; Van de Werf, F.; Avezum, Á.; Goodman, S.G.; Flather, M.D.; et al. Predictors of Hospital Mortality in the Global Registry of Acute Coronary Events. Arch. Intern. Med. 2003, 163, 2345–2353. [Google Scholar] [CrossRef] [Green Version]
- Amin, S.T.; Morrow, D.A.; Braunwald, E.; Sloan, S.; Contant, C.; Murphy, S.; Antman, E.M. Dynamic TIMI Risk Score for STEMI. J. Am. Heart Assoc. 2013, 2, e003269. [Google Scholar] [CrossRef] [Green Version]
- Dai, X.; Kaul, P.; Smith, S.C.; Stouffer, G.A. Predictors, treatment, and outcomes of STEMI occurring in hospitalized patients. Nat. Rev. Cardiol. 2016, 13, 148–154. [Google Scholar] [CrossRef]
- Gevaert, S.A.; De Bacquer, D.; Evrard, P.; Convens, C.; Dubois, P.; Boland, J.; Renard, M.; Beauloye, C.; Coussement, P.; De Raedt, H.; et al. Gender, TIMI risk score and in-hospital mortality in STEMI patients undergoing primary PCI: Results from the Belgian STEMI registry. EuroIntervention 2014, 9, 1095–1101. [Google Scholar] [CrossRef] [Green Version]
- Stehli, J.; Martin, C.; Brennan, A.; Dinh, D.T.; Lefkovits, J.; Zaman, S. Sex Differences Persist in Time to Presentation, Revascularization, and Mortality in Myocardial Infarction Treated with Percutaneous Coronary Intervention. J. Am. Heart Assoc. 2019, 8, e012161. [Google Scholar] [CrossRef] [Green Version]
- Benamer, H.; Bataille, S.; Tafflet, M.; Jabre, P.; Dupas, F.; Laborne, F.X.; Lapostolle, F.; Lefort, H.; Juliard, J.-M.; Letarnec, J.-Y.; et al. Longer pre-hospital delays and higher mortality in women with STEMI: The e-MUST Registry. EuroIntervention 2016, 12, e542–e549. [Google Scholar] [CrossRef] [PubMed]
- Lawesson, S.S.; Alfredsson, J.; Fredrikson, M.; Swahn, E. A gender perspective on short- and long term mortality in ST-elevation myocardial infarction—A report from the SWEDEHEART register. Int. J. Cardiol. 2013, 168, 1041–1047. [Google Scholar] [CrossRef] [PubMed]
- Hayıroğlu, M.; Keskin, M.; Uzun, A.O.; Yıldırım, D.I.; Kaya, A.; Çinier, G.; Bozbeyoğlu, E.; Yıldırımtürk, Ö.; Kozan, Ö.; Pehlivanoğlu, S. Predictors of In-Hospital Mortality in Patients With ST-Segment Elevation Myocardial Infarction Complicated With Cardiogenic Shock. Heart Lung Circ. 2019, 28, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Hayıroğlu, M.İ.; Çanga, Y.; Yıldırımtürk, Ö.; Bozbeyoğlu, E.; Gümüşdağ, A.; Uzun, A.O.; Kalenderoğlu, K.; Keskin, M.; Çinier, G.; Acarel, M.; et al. Clinical characteristics and outcomes of acute coronary syndrome patients with intra-aortic balloon pump inserted in intensive cardiac care unit of a tertiary clinic. Turk. Kardiyol. Dern. Ars. 2018, 46, 10–17. [Google Scholar]


{kind=link}
| Variable | Male (n = 2400) | Female (n = 544) | Missing Data n (%) | p |
|---|---|---|---|---|
| Age | 60 (±12) | 69 (±13) | <0.001 | |
| Hyperlipidemia | 1150 (47.9) | 312 (57.4) | <0.001 | |
| Hypertension | 991 (41.3) | 342 (62.9) | <0.001 | |
| Diabetes | 552 (23) | 159 (29.2) | <0.001 | |
| Past Myocardial infarction | 404 (16.8) | 61 (11.2) | <0.001 | |
| Smoker | 1283 (53.3) | 201 (36.9) | <0.001 | |
| Chronic kidney disease | 463 (19.3) | 145 (26.7) | <0.001 | |
| Ejection fraction (%) | 47.4 (±8) | 46.4 (±8) | 0.02 | |
| Time to ER, min | 120 (60–360) | 180 (75–400) | 33 (1.1) | <0.001 |
| Door to balloon, min | 45 (30–60) | 45 (30–60) | 281 (9.5) | 0.36 |
| Time to reperfusion, min | 165 (105–450) | 240 (125–600) | 281 (9.5) | <0.001 |
| Coronary artery vessel disease | 27 (0.9) | <0.001 | ||
| 1 | 957 (40.2) | 264 (49.3) | ||
| 2 | 760 (31.9) | 127 (23.7) | ||
| 3 | 665 (27.9) | 144 (26.9) | ||
| Estimated GFR | 75.5 ± 20 | 75.8 ± 24 | 0.84 | |
| Creatinine, admission | 1.07 (0.95–1.22) | 0.95 (0.82–1.11) | <0.001 | |
| Creatinine, peak | 1.07 (0.96–1.24) | 0.96 (0.82–1.22) | <0.001 | |
| Troponin-I, admission | 0.91 (0.06–28.4) | 1.36 (0.09–19.3) | 694 (23.6) | 0.21 |
| Troponin-I, peak | 47 (7.4–299.6) | 30 (6–178.2) | 694 (23.6) | <0.01 |
| Variable | Male (n = 186) | Female (n = 69) | p |
|---|---|---|---|
| Acute kidney injury | 186 (7.8) | 69 (12.7) | <0.001 |
| Baseline Chronic kidney disease | 77 (48.7) | 39 (65) | 0.03 |
| Estimated GFR, admission | 58.5 ± 23 | 57.6 ± 25 | 0.80 |
| Creatinine, admission | 1.24 (1.05–1.55) | 1.10 (0.91–1.29) | <0.01 |
| Creatinine, peak | 1.81 (1.45–2.49) | 1.68 (1.44–2.28) | 0.24 |
| Severe AKI a | 27 (14.5) | 18 (26.1) | 0.031 |
| AKI early recovery b | 91 (48.9) | 33 (47.8) | 0.88 |
| AKI partial recovery c | 42 (22.6) | 10 (14.5) | 0.15 |
| AKI any recovery d | 133 (71.5) | 43 (62.3) | 0.16 |
| Variable | AOR | 95% CI | p |
|---|---|---|---|
| Female | 1.01 | 0.73–1.40 | 0.94 |
| Age | 1.04 | 1.02–1.05 | <0.001 |
| Hypertension | 2.02 | 1.48–2.75 | <0.001 |
| Diabetes | 1.26 | 0.94–1.69 | 0.12 |
| Chronic kidney disease | 2.37 | 1.71–3.30 | <0.001 |
| Variable | AOR | 95% CI | p |
|---|---|---|---|
| Female | 1.65 | 0.80–1.65 | 0.18 |
| Age | 1.03 | 0.99–1.06 | 0.09 |
| Hypertension | 1.13 | 0.48–2.61 | 0.78 |
| Diabetes | 1.73 | 0.88–3.38 | 0.11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frydman, S.; Freund, O.; Banai, A.; Zornitzki, L.; Banai, S.; Shacham, Y. Relation of Gender to the Occurrence of AKI in STEMI Patients. J. Clin. Med. 2022, 11, 6565. https://doi.org/10.3390/jcm11216565
Frydman S, Freund O, Banai A, Zornitzki L, Banai S, Shacham Y. Relation of Gender to the Occurrence of AKI in STEMI Patients. Journal of Clinical Medicine. 2022; 11(21):6565. https://doi.org/10.3390/jcm11216565
Chicago/Turabian StyleFrydman, Shir, Ophir Freund, Ariel Banai, Lior Zornitzki, Shmuel Banai, and Yacov Shacham. 2022. "Relation of Gender to the Occurrence of AKI in STEMI Patients" Journal of Clinical Medicine 11, no. 21: 6565. https://doi.org/10.3390/jcm11216565