
BMI Modifies Increased Mortality Risk of Post-PCI STEMI Patients with AKI
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. Data Collection and Definition
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
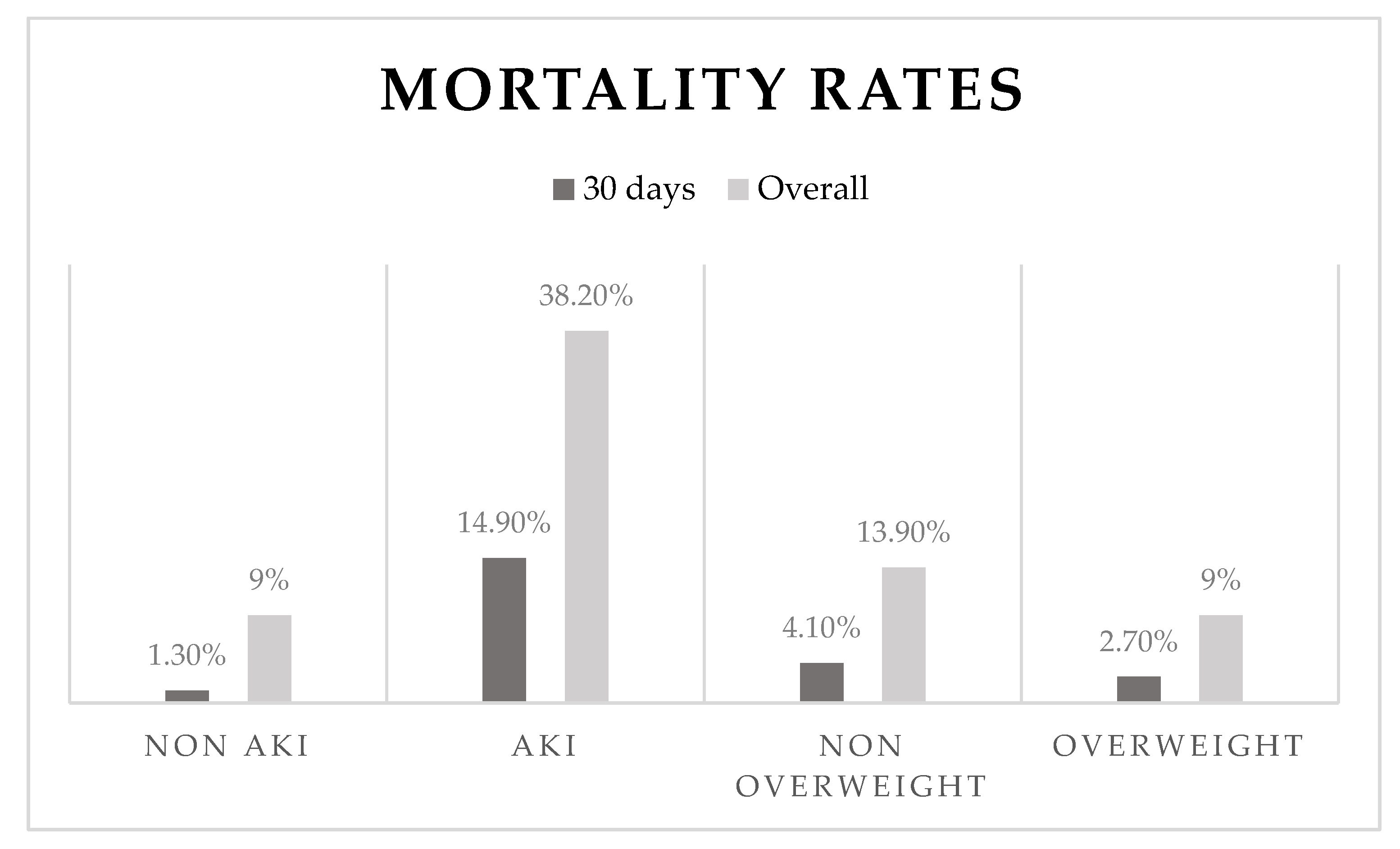
3.2. Primary Outcome
3.3. Multivariant Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Available online: https://www.who.int/data/gho/data/themes/topics/causes-of-death (accessed on 30 March 2021).
- Kolh, P.; Windecker, S.; Alfonso, F.; Collet, J.P.; Cremer, J.; Falk, V.; Filippatos, G.; Hamm, C.; Head, S.J.; Jüni, P. 2014 ESC/EACTS Guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur. Heart J. 2014, 35, 2541–2619. [Google Scholar]
- Goldberg, A.; Hammerman, H.; Petcherski, S.; Zdorovyak, A.; Yalonetsky, S.; Kapeliovich, M.; Agmon, Y.; Markiewicz, W.; Aronson, D. Inhospital and 1-year mortality of patients who develop worsening renal function following acute ST-elevation myocardial infarction. Am. Heart J. 2005, 150, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Moriyama, N.; Ishihara, M.; Noguchi, T.; Nakanishi, M.; Arakawa, T.; Asaumi, Y.; Kumasaka, L.; Kanaya, T.; Nagai, T.; Fujino, M.; et al. Early development of acute kidney injury is an independent predictor of in-hospital mortality in patients with acute myocardial infarction. J. Cardiol. 2016, 69, 79–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, C.S.; Muntner, P.; Chen, A.Y.; Alexander, K.P.; Roe, M.T.; Wiviott, S.D. Short-term Outcomes of Acute Myocardial Infarction in Patients with Acute Kidney Injury. Circulation 2012, 125, 497–504. [Google Scholar] [CrossRef] [Green Version]
- El-Ahmadi, A.; Abassi, M.S.; Andersson, H.B.; Engstrøm, T.; Clemmensen, P.; Helqvist, S.; Jørgensen, E.; Kelbæk, H.; Pedersen, F.; Saunamäki, K.; et al. Acute kidney injury—A frequent and serious complication after primary percutaneous coronary intervention in patients with ST-segment elevation myocardial infarction. PLoS ONE 2019, 14, e0226625. [Google Scholar] [CrossRef] [Green Version]
- Murphy, S.W.; Barrett, B.J.; Parfrey, P.S. Contrast Nephropathy. J. Am. Soc. Nephrol. 2000, 11, 177. [Google Scholar] [CrossRef]
- Fan, P.-C.; Chen, T.-H.; Lee, C.-C.; Tsai, T.-Y.; Chen, Y.-C.; Chang, C.-H. ADVANCIS Score Predicts Acute Kidney Injury after Percutaneous Coronary Intervention for Acute Coronary Syndrome. Int. J. Med. Sci. 2018, 15, 528–535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinkovič, A.; Masnik, K.; Mihevc, M. Predictors of acute kidney injury (AKI) in high-risk ST-elevation myocardial infarction (STEMI) patients: A single-center retrospective observational study. Bosn. J. Basic Med. Sci. 2019, 19, 101–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rana, J.S.; Mukamal, K.J.; Morgan, J.P.; Muller, J.E.; Mittleman, M.A. Obesity and the risk of death after acute myocardial infarction. Am. Heart J. 2004, 147, 841–846. [Google Scholar] [CrossRef] [PubMed]
- Doost Hosseiny, A.; Moloi, S.; Chandrasekhar, J.; Farshid, A. Mortality pattern and cause of death in a long-term follow-up of patients with STEMI treated with primary PCI. Open Heart 2016, 3, e000405. [Google Scholar] [CrossRef] [Green Version]
- Das, S.R.; Alexander, K.P.; Chen, A.Y.; Powell-Wiley, T.M.; Diercks, D.B.; Peterson, E.D.; Roe, M.T.; De Lemos, J.A. Impact of Body Weight and Extreme Obesity on the Presentation, Treatment, and in-Hospital Outcomes of 50,149 Patients with ST-Segment Elevation Myocardial Infarction. J. Am. Coll. Cardiol. 2011, 58, 2642–2650. [Google Scholar] [CrossRef] [PubMed]
- Prospective Studies Collaboration. Body-mass index and cause-specific mortality in 900,000 adults: Collaborative analyses of 57 prospective studies. Lancet 2009, 373, 1083–1096. [Google Scholar] [CrossRef] [Green Version]
- Kanic, V.; Vollrath, M.; Frank, B.; Kanic, Z. An obesity paradox in patients with myocardial infarction undergoing percutaneous intervention. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Adham, K.; Samiullah, A.; Sara, K.; Vedant, G. Explaining the BMI paradox in acute myocardial infraction. J. Am. Coll. Cardiol. 2021, 77, 171. [Google Scholar]
- Plečko, D.; Bennett, N.; Mårtensson, J.; Bellomo, R. The obesity paradox and hypoglycemia in critically ill patients. Crit. Care 2021, 25, 378. [Google Scholar] [CrossRef] [PubMed]
- Danziger, J.; Chen, K.; Lee, J.; Feng, M.; Mark, R.G.; Celi, L.A.; Mukamal, K.J. Obesity, Acute Kidney Injury, and Mortality in Critical Illness. Crit. Care Med. 2016, 44, 328–334. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://kdigo.org/guidelines/acute-kidney-injury/ (accessed on 30 March 2021).
- Kuźma, Ł.; Małyszko, J.; Kurasz, A.; Niwińska, M.M.; Zalewska-Adamiec, M.; Bachórzewska-Gajewska, H.; Dobrzycki, S. Impact of renal function on patients with acute coronary syndromes: 15,593 patient-years study. Ren. Fail. 2020, 42, 881–889. [Google Scholar] [CrossRef]
- Brown, J.R.; Malenka, D.J.; DeVries, J.T.; Robb, J.F.; Jayne, J.E.; Friedman, B.J.; Hettleman, B.D.; Niles, N.W.; Kaplan, A.V.; Schoolwerth, A.C.; et al. Transient and persistent renal dysfunction are predictors of survival after percutaneous coronary intervention: Insights from the Dartmouth Dynamic Registry. Catheter. Cardiovasc. Interv. 2008, 72, 347–354. [Google Scholar] [CrossRef]
- Amin, A.P.; Salisbury, A.C.; McCullough, P.A.; Gosch, K.; Spertus, J.A.; Venkitachalam, L.; Stolker, J.M.; Parikh, C.R.; Masoudi, F.A.; Jones, P.G.; et al. Trends in the Incidence of Acute Kidney Injury in Patients Hospitalized with Acute Myocardial Infarction. Arch. Intern. Med. 2012, 172, 246–253. [Google Scholar] [CrossRef] [Green Version]
- Schiffl, H. Obesity and the Survival of Critically Ill Patients with Acute Kidney Injury: A Paradox within the Paradox? Kidney Dis. 2020, 6, 13–21. [Google Scholar] [CrossRef]
- Kim, H.; Kim, J.; Seo, C.; Lee, M.; Cha, M.-U.; Jung, S.-Y.; Jhee, J.H.; Park, S.; Yun, H.-R.; Kee, Y.K.; et al. Body mass index is inversely associated with mortality in patients with acute kidney injury undergoing continuous renal replacement therapy. Kidney Res. Clin. Pract. 2017, 36, 39–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, S.Y.; Kim, W.; Kim, J.S.; Jeong, K.H.; Jeong, M.H.; Hwang, J.Y.; Hwang, H.S. Renal Function Effect on the Association between Body Mass Index and Mortality Risk after Acute Myocardial Infarction. Front. Cardiovasc. Med. 2021, 8, 765153. [Google Scholar] [CrossRef] [PubMed]
- Di Stefano, R.; Di Bello, V.; Barsotti, M.C.; Grigoratos, C.; Armani, C.; Dell’Omodarme, M.; Carpi, A.; Balbarini, A. Inflammatory markers and cardiac function in acute coronary syndrome: Difference in ST-segment elevation myocardial infarction (STEMI) and in non-STEMI models. Biomed. Pharmacother. 2009, 63, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Rabb, H.; Griffin, M.D.; McKay, D.B.; Swaminathan, S.; Pickkers, P.; Rosner, M.H.; Kellum, J.A.; Ronco, C. Inflammation in AKI: Current Understanding, Key Questions, and Knowledge Gaps. J. Am. Soc. Nephrol. 2016, 27, 371–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, W.-S.; Lee, W.-J.; Funahashi, T.; Tanaka, S.; Matsuzawa, Y.; Chao, C.-L.; Chen, C.-L.; Tai, T.-Y.; Chuang, L.-M. Plasma Adiponectin Levels in Overweight and Obese Asians. Obes. Res. 2002, 10, 1104–1110. [Google Scholar] [CrossRef] [PubMed]
- Rolland, Y.M.; Haren, M.T.; Patrick, P.; Banks, W.A.; Malmstrom, T.K.; Miller, D.K.; Morley, J.E. Adiponectin levels in obese and non-obese middle-aged African–American women. Obes. Res. Clin. Pract. 2007, 1, 27–37. [Google Scholar] [CrossRef] [Green Version]
- Natsukawa, T.; Maeda, N.; Fukuda, S.; Yamaoka, M.; Fujishima, Y.; Nagao, H.; Sato, F.; Nishizawa, H.; Sawano, H.; Hayashi, Y.; et al. Significant Association of Serum Adiponectin and Creatine Kinase-MB Levels in ST-Segment Elevation Myocardial Infarction. J. Atheroscler. Thromb. 2017, 24, 793–803. [Google Scholar] [CrossRef] [Green Version]
- Wolf, A.M.; Wolf, D.; Rumpold, H.; Enrich, B.; Tilg, H. Adiponectin induces the anti-inflammatory cytokines IL-10 and IL-1RA in human leukocytes. Biochem. Biophys. Res. Commun. 2004, 323, 630–635. [Google Scholar] [CrossRef]
- Ellulu, M.S.; Patimah, I.; KhazáAi, H.; Rahmat, A.; Abed, Y. Obesity and inflammation: The linking mechanism and the complications. Arch. Med. Sci. 2017, 13, 851–863. [Google Scholar] [CrossRef]
- Lafontan, M. FAT CELLS: Afferent and Efferent Messages Define New Approaches to Treat Obesity. Annu. Rev. Pharmacol. Toxicol. 2005, 45, 119–146. [Google Scholar] [CrossRef]
- Wang, C.-H.; Li, S.-H.; Weisel, R.D.; Fedak, P.; Dumont, A.S.; Szmitko, P.; Li, R.-K.; Mickle, D.A.G.; Verma, S. C-Reactive Protein Upregulates Angiotensin Type 1 Receptors in Vascular Smooth Muscle. Circulation 2003, 107, 1783–1790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheikh, A.; Yahya, S.; Sheikh, N.; Sheikh, A. C-reactive protein as a predictor of adverse outcome in patients with acute coronary syndrome. Heart Views 2012, 13, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Fang, L.; Moore, X.-L.; Dart, A.M.; Wang, L.-M. Systemic inflammatory response following acute myocardial infarction. J. Geriatr. Cardiol. 2015, 12, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Denis, G.V.; Obin, M.S. ‘Metabolically healthy obesity’: Origins and implications. Mol. Asp. Med. 2013, 34, 59–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coutinho, T.; Goel, K.; de Sá, D.C.; Kragelund, C.; Kanaya, A.M.; Zeller, M.; Park, J.-S.; Kober, L.; Torp-Pedersen, C.; Cottin, Y.; et al. Central Obesity and Survival in Subjects with Coronary Artery Disease: A Systematic Review of the Literature and Collaborative Analysis with Individual Subject Data. J. Am. Coll. Cardiol. 2011, 57, 1877–1886. [Google Scholar] [CrossRef] [Green Version]
- Canoy, D.; Boekholdt, S.M.; Wareham, N.; Luben, R.; Welch, A.; Bingham, S.; Buchan, I.; Day, N.; Khaw, K.T. Body fat distribution and risk of coronary heart disease in men and women in the European Prospective Investigation into Cancer and Nutrition in Norfolk cohort: A population-based prospective study. Circulation 2007, 116, 2933–2943. [Google Scholar] [CrossRef] [Green Version]
- Yusuf, S.; Hawken, S.; Ôunpuu, S.; Bautista, L.; Franzosi, M.G.; Commerford, P.; Lang, C.C.; Rumboldt, Z.; Onen, C.L.; Lisheng, L.; et al. Obesity and the risk of myocardial infarction in 27,000 participants from 52 countries: A case-control study. Lancet 2005, 366, 1640–1649. [Google Scholar] [CrossRef]
- Shahim, B.; Redfors, B.; Chen, S.; Thiele, H.; Eitel, I.; Gkargkoulas, F.; Crowley, A.; Ben-Yehuda, O.; Maehara, A.; Stone, G.W. BMI, Infarct Size, and Clinical Outcomes Following Primary PCI: Patient-Level Analysis From 6 Randomized Trials. JACC Cardiovasc. Interv. 2020, 13, 965–972. [Google Scholar] [CrossRef]
- Pingitore, A.; Di Bella, G.; Lombardi, M.; Iervasi, G.; Strata, E.; Aquaro, G.D.; Positano, V.; De Marchi, D.; Rossi, G.; L’Abbate, A.; et al. The obesity paradox and myocardial infarct size. J. Cardiovasc. Med. 2007, 8, 713–717. [Google Scholar] [CrossRef]
- Sohn, G.H.; Kim, E.K.; Hahn, J.-Y.; Bin Song, Y.; Yang, J.H.; Chang, S.-A.; Lee, S.-C.; Choe, Y.H.; Choi, S.-H.; Choi, J.-H.; et al. Impact of overweight on myocardial infarct size in patients undergoing primary percutaneous coronary intervention: A magnetic resonance imaging study. Atherosclerosis 2014, 235, 570–575. [Google Scholar] [CrossRef]
- Park, D.; Lee, J.; Han, S. Underweight: Another risk factor for cardiovascular disease?: A cross-sectional 2013 Behavioral Risk Factor Surveillance System (BRFSS) study of 491,773 individuals in the USA. Medicine 2017, 96, e8769. [Google Scholar] [CrossRef] [PubMed]
- Champney, K.P.; Frederick, P.; Bueno, H.; Parashar, S.; Foody, J.; Merz, C.N.B.; Canto, J.G.; Lichtman, J.H.; Vaccarino, V. For the NRMI Investigators The joint contribution of sex, age and type of myocardial infarction on hospital mortality following acute myocardial infarction. Heart 2009, 95, 895–899. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patients without AKI | N | Patients with AKI | N | p-Value | |
|---|---|---|---|---|---|
| N (1706) | 1528 (89.6%) | 178 (10.4%) | |||
| Age, yrs | 60.4 (±12.5) | 1528 | 70.8 (±13.1) | 178 | <0.001 |
| Gender (Female) | 18.7% | 1528 | 27% | 178 | 0.009 |
| BMI | 26.80 (±4.0) | 1093 | 27.1 (±4) | 130 | 0.98 |
| Smoker | 52.1% | 1528 | 33% | 178 | <0.001 |
| DM | 20.5% | 1528 | 32% | 178 | <0.001 |
| HTN | 40.1% | 1528 | 69% | 178 | <0.001 |
| HPL | 46.1% | 1528 | 55% | 178 | 0.20 |
| Past MI | 10.5% | 1528 | 14.5% | 178 | 0.09 |
| Cr (mg/dL) | 1.12 (±0.22) | 1528 | 1.31 (±0.43) | 178 | <0.001 |
| CRP (mg/L) | 3.8 (1.3–10.1) | 854 | 9.3 (2.3–20.4) | 97 | <0.001 |
| CPK (U/L) | 776 (313.5–1592.5) | 1497 | 918 (331–2468) | 172 | 0.04 |
| Hb (g/dL) | 14.4 (±1.5) | 1526 | 13.60 (±1.8) | 178 | 0.001 |
| Time to reperfusion (min) | 165 (105–390) | 1527 | 232.5 (120–765) | 178 | 0.001 |
| Contrast volume (ml) | 140 (115–175) | 383 | 140 (97–155) | 35 | 0.11 |
| Hemodynamic instability * | 2.20% | 1527 | 16.90% | 178 | <0.001 |
| CAD | 0–0.2%, 1–45.1%, 2–29.9%, 3≤–24.8% | 1524 | 0–0%, 1–36.5%, 2–27%, 3≤–36.5% | 178 | 0.008 |
| EF (%) | 50 (40–55) | 1505 | 45 (35–50) | 176 | <0.001 |
| Follow-up time (wks) | 45 (23–73) | 1500 | 45 (23–71) | 175 | 0.008 |
| Non-Overweight Patients | N | Overweight Patients | N | p-Value | |
|---|---|---|---|---|---|
| 560 (35%) | 1045 (65%) | ||||
| Age, yrs | 63.7 (±13.6) | 560 | 60.4 (±12.8) | 1044 | <0.001 |
| Gender (Female) | 41.90% | 560 | 58.10% | 1044 | 0.005 |
| Smoker | 53.90% | 560 | 51% | 1044 | 0.25 |
| DM | 17.10% | 560 | 26.70% | 1044 | <0.001 |
| HTN | 37.90% | 560 | 45% | 1044 | 0.006 |
| HPL | 41.40% | 560 | 49% | 1044 | 0.004 |
| Past MI | 14.60% | 560 | 14.60% | 1044 | 0.9 |
| Cr (mg/dL) | 1.10 (±0.36) | 559 | 1.10 (±0.33) | 1042 | 0.74 |
| CRP (mg/L) | 3 (0.95–9.5) | 419 | 5.4 (2.2–11.3) | 783 | <0.001 |
| CPK (U/L) | 885 (327–1707) | 551 | 837 (341–1772) | 1028 | 0.94 |
| Hb (g/dL) | 14.00 (±1.6) | 559 | 14.40 (±1.5) | 1043 | <0.001 |
| Time to reperfusion (min) | 90 (110–390) | 552 | 165 (105–420) | 1024 | 0.36 |
| Contrast volume (mL) | 136.5 (110.5–168.5) | 142 | 144.5 (117.7–176) | 238 | 0.15 |
| Hemodynamic instability * | 4.50% | 560 | 3.90% | 1043 | 0.60 |
| CAD | 0–0.4%, 1–46.7%, 2–23.4%, 3–29.5% | 555 | 0–0%, 1–40.2%, 2–32.2%, 3–27.6% | 1035 | 0.001 |
| EF (%) | 45 (40–50) | 556 | 45.90 (40–50) | 1029 | 0.09 |
| AKI | 9.80% | 429 | 11.10% | 778 | 0.49 |
| Follow-up time (wks) | 46 (24–75) | 545 | 45 (23–74) | 1032 | 0.46 |
| BMI Class | N | 30-Day Mortality p = 0.17 | N | Overall Mortality p = 0.02 |
|---|---|---|---|---|
| <18.5 | 14 | 2 (14%) | 14 | 4 (28.5%) |
| 18.6–24.9 | 541 | 21 (4%) | 546 | 74 (13.6%) |
| 25–29.9 | 725 | 19 (2.5%) | 730 | 68 (9.3%) |
| 30–34.9 | 245 | 7 (3%) | 246 | 21 (8.5%) |
| 35–39.9 | 53 | 2 (3.5%) | 56 | 4 (7%) |
| >40 | 12 | 0 | 12 | 1 (8.5%) |
| 30-Day Mortality N = 789 | p-Value | Overall Mortality N = 797 | p-Value | |
|---|---|---|---|---|
| Age, yrs | 1.08 (0.97–1.19) | 0.13 | 1.07 (1.04–1.11) | <0.001 |
| Gender (Female) | 0.00 (0–0.005) | 0.008 | 1.38 (0.64–2.95) | 0.40 |
| BMI | 0.40 (0.21–0.75) | 0.005 | 0.91 (0.84–0.99) | 0.04 |
| Smoker | 1.51 (0.19–11.8) | 0.69 | 2.65 (1.50–4.69) | 0.001 |
| DM | 5.69 (0.52–61.36) | 0.15 | 2.30 (0.85–6.19) | 0.09 |
| HTN | 2.04 (0.34–12.30) | 0.43 | 0.96 (0. 12–4.36) | 0.96 |
| HPL | 19.46 (0.003–136,010.27) | 0.51 | 0.74 (0.38–1.44) | 0.39 |
| Cr (mg/dL) | 0.00 (0.00–0.00) | 0.002 | 2.70 (0.002–4895.51) | 0.79 |
| CRP (mg/L) | 1.06 (1.03–1.10) | <0.001 | 1.01 (1.00–1.02) | 0.002 |
| CPK (U/L) | 1.0 (1.0–1.0) | 0.10 | 1.00 (1.00–1.00) | 0.93 |
| HB (g/dL) | 0.02 (0.002–0.22) | 0.002 | 0.27 (0.07–1.03) | 0.056 |
| Time to reperfusion (min) | 1.0 (0.99–1.002) | 0.58 | 1.00 (0.99–1.00) | 0.85 |
| CAD | 0.00 (0.00–0.07) | 0.008 | 0.979 (0.59–1.62) | 0.93 |
| Hemodynamic instability * | 247.02 (8.12–7512.77) | 0.09 | 23.72 (5.19–108.26) | <0.001 |
| EF (%) | 0.82 (0.73–0.93) | 0.002 | 0.61 (0.44–0.84) | 0.003 |
| AKI | 41.51 (3.99–431.13) | 0.002 | 2.91 (1.22–6.92) | 0.01 |
| 30-Day Survival N = 756 | p-Value | Overall Survival N = 781 | p-Value | |
|---|---|---|---|---|
| Age, yrs | 1.23 (0.99–1.52) | 0.05 | 1.06 (1.03–1.09) | <0.001 |
| Gender (Female) | 0.00 (0–0.001) | 0.003 | 490.15 (20.03–11,994.34) | <0.001 |
| BMI | 0.77 (0.64–0.94) | 0.01 | 0.93 (0.87–1.00) | 0.054 |
| Smoker | 0.87 (0.19–3.84) | 0.85 | 2.65 (1.50–4.69) | 0.001 |
| DM | 7.17 (1.24–41.40) | 0.02 | 28.67 (0.81–1009.09) | 0.06 |
| HTN | 0.02 (0.00–4.08) | 0.15 | 1.11 (0.62–1.96) | 0.71 |
| HPL | 0.69 (0.19–2.49) | 0.57 | 0.86 (0.48–1.51) | 0.60 |
| Cr (mg/dL) | 0.00 (0.00–0.11) | 0.03 | 1.54 (0.72–3.31) | 0.26 |
| CRP (mg/L) | 1.01 (1.004–1.03) | 0.009 | 1.01 (1.00–1.01) | <0.001 |
| CPK (U/L) | 1.0 (1.0–1.0) | 0.28 | 1.00 (1.00–1.00) | 0.90 |
| HB (g/dL) | 0.02 (0.002–0.18) | 0.001 | 1.03 (0.85–1.24) | 0.75 |
| Time to reperfusion | 1.0 (0.99–1.001) | 0.98 | 1.00 (0.99–1.00) | 0.16 |
| CAD | 0.76 (0.34–1.66) | 0.49 | 1.06 (0.76–1.48) | 0.71 |
| Hemodynamic instability * | 3.81 (0.78–18.54) | 0.09 | 43.04 (0.14–12,402.22) | 0.19 |
| EF (%) | 0.85 (0.79–0.92) | <0.001 | 1.01 (0.97–1.06) | 0.43 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schvartz, R.; Lupu, L.; Frydman, S.; Banai, S.; Shacham, Y.; Gal-Oz, A. BMI Modifies Increased Mortality Risk of Post-PCI STEMI Patients with AKI. J. Clin. Med. 2022, 11, 6104. https://doi.org/10.3390/jcm11206104
Schvartz R, Lupu L, Frydman S, Banai S, Shacham Y, Gal-Oz A. BMI Modifies Increased Mortality Risk of Post-PCI STEMI Patients with AKI. Journal of Clinical Medicine. 2022; 11(20):6104. https://doi.org/10.3390/jcm11206104
Chicago/Turabian StyleSchvartz, Reut, Lior Lupu, Shir Frydman, Shmuel Banai, Yacov Shacham, and Amir Gal-Oz. 2022. "BMI Modifies Increased Mortality Risk of Post-PCI STEMI Patients with AKI" Journal of Clinical Medicine 11, no. 20: 6104. https://doi.org/10.3390/jcm11206104