


Are Torque-Induced Bone Texture Alterations Related to Early Marginal Jawbone Loss?


Abstract
:1. Introduction
2. Materials and Methods
- MBL appearance (YES) if MLB is >0
- MBL appearance (NO) if MBL is =0
Statistical Analysis
3. Results
3.1. Marginal Bone Loss Statistical Evaluation
3.2. Torque Statistical Evaluation
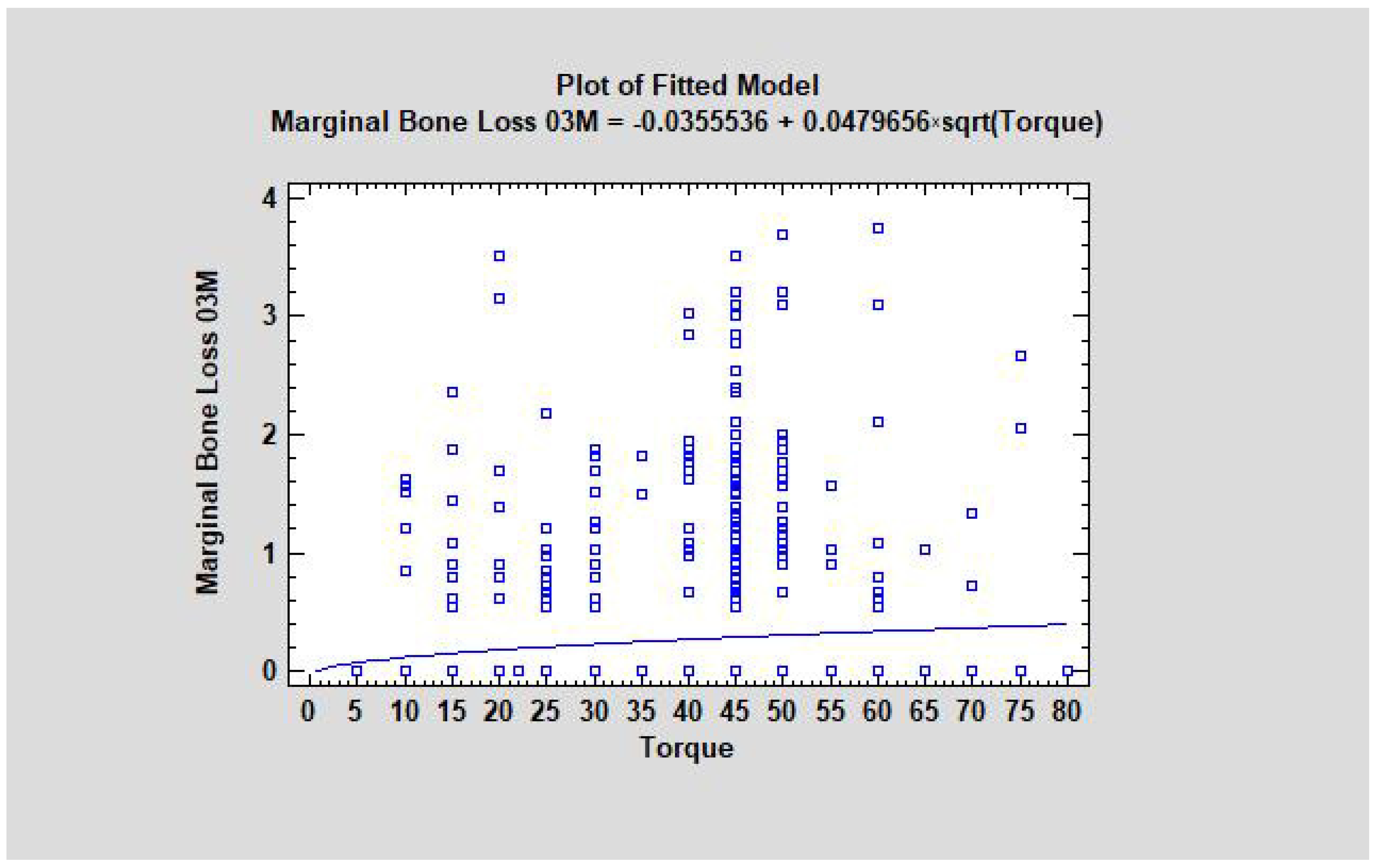
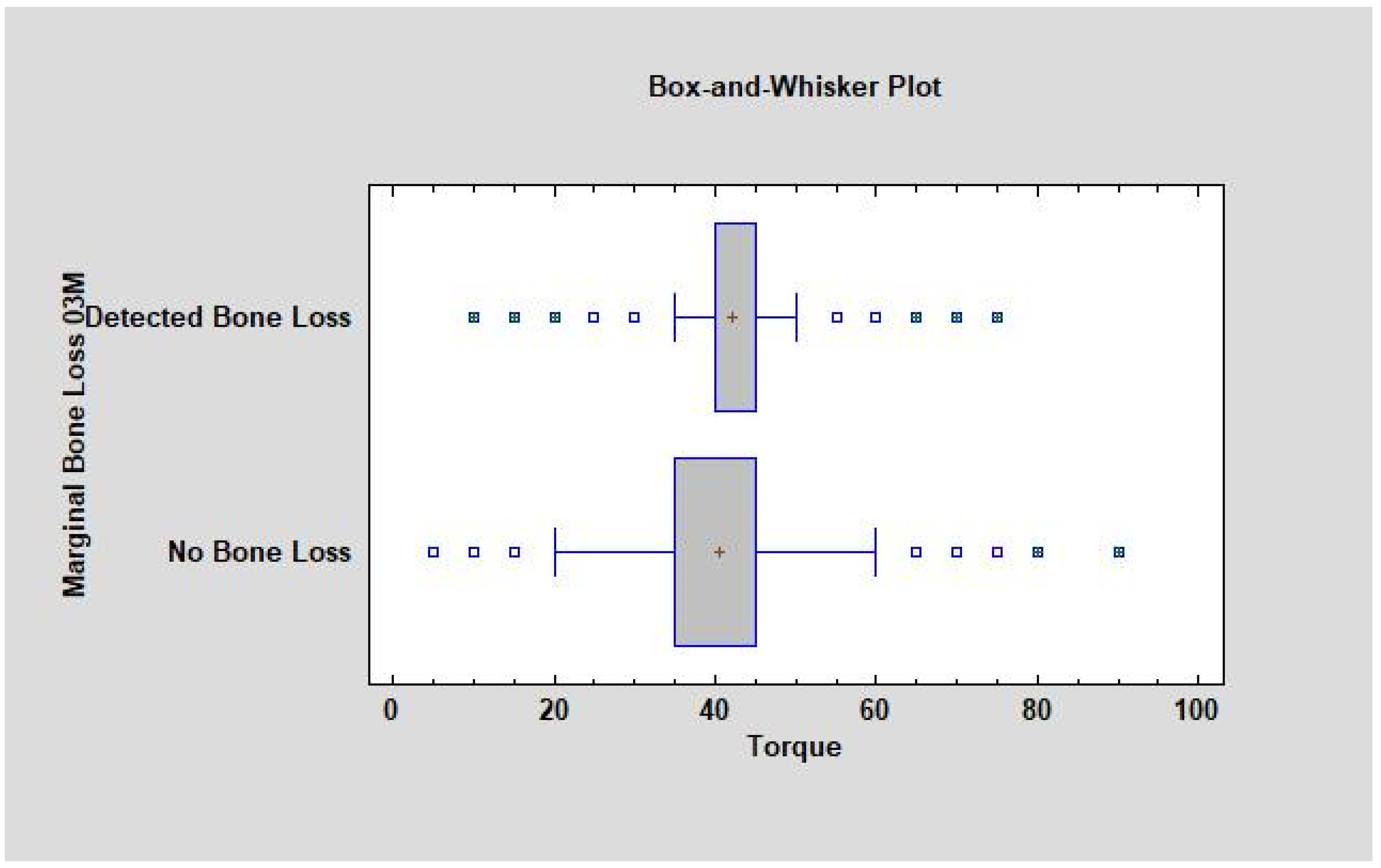
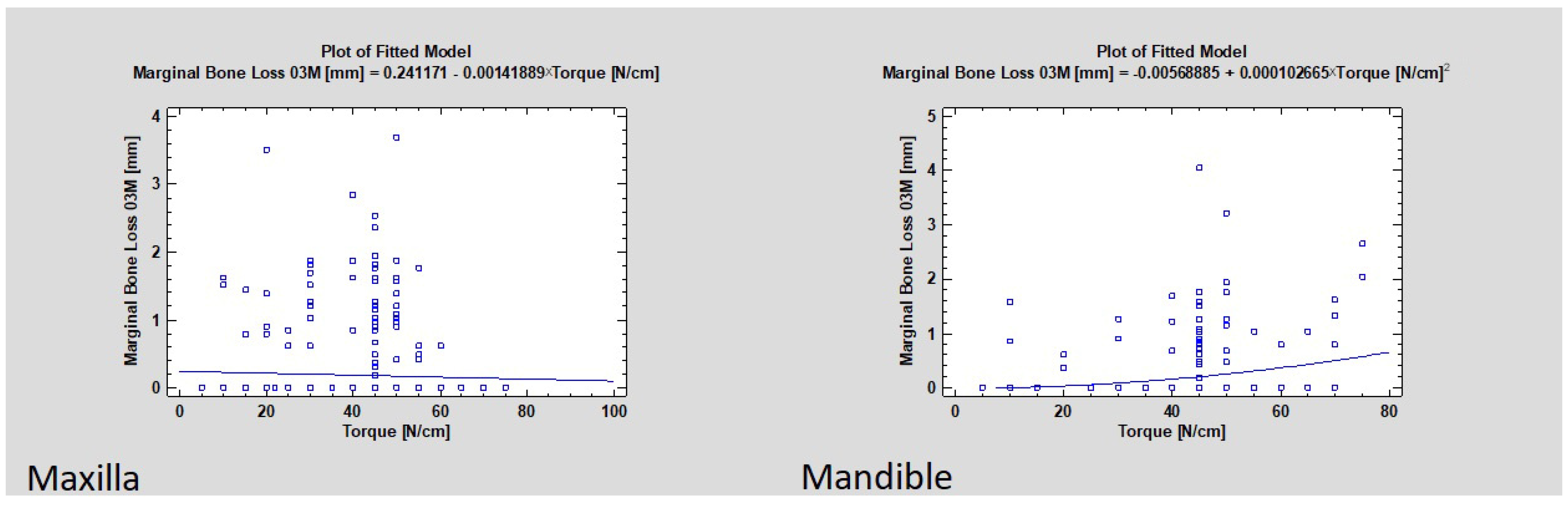
3.3. Torque Value and Marginal Bone Loss as a Dependency
3.4. Implant Placement Region in Jaw
- SumAverg,
- Entropy,
- DifEntr,
- LngREmph,
- ShrtREmph,
- Wavelets 4 and 5.
- SumOfSqrs,
- Wavelet 6—was not detected.
3.5. SumAverg Changes
3.6. Entropy Changes
3.7. DifEntr Changes
3.8. LngREmph Changes
3.9. ShrtREmph Changes
3.10. Wavelet Decomposition Changes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Çankaya, A.B.; Akçay, Ç.; Kahraman, N.; Köseoğlu, B.G. Oral surgical procedures under local anaesthesia in day surgery. BMC Oral Health 2018, 18, 4–7. [Google Scholar] [CrossRef] [PubMed]
- Wach, T.; Kozakiewicz, M. Comparison of two clinical procedures in patient affected with bone deficit in posterior mandible. Dent. Med. Probl. 2016, 53, 22–28. [Google Scholar] [CrossRef] [Green Version]
- Kowalski, J.; Lapinska, B.; Nissan, J.; Lukomska-Szymanska, M. Factors influencing marginal bone loss around dental implants: A narrative review. Coatings 2021, 11, 865. [Google Scholar] [CrossRef]
- Aldahlawi, S.; Demeter, A.; Irinakis, T. The effect of implant placement torque on crestal bone remodeling after 1 year of loading. Clin. Cosmet. Investig. Dent. 2018, 10, 203–209. [Google Scholar] [CrossRef] [Green Version]
- Kwiatek, J.; Jaroń, A.; Trybek, G. Impact of the 25-hydroxycholecalciferol concentration and vitamin d deficiency treatment on changes in the bone level at the implant site during the process of osseointegration: A prospective, randomized, controlled clinical trial. J. Clin. Med. 2021, 10, 526. [Google Scholar] [CrossRef]
- Sargolzaie, N.; Zarch, H.H.; Arab, H.; Koohestani, T.; Ramandi, M.F. Marginal bone loss around crestal or subcrestal dental implants: Prospective clinical study. J. Korean Assoc. Oral Maxillofac. Surg. 2022, 48, 159–166. [Google Scholar] [CrossRef]
- Attanasio, F.; Antonelli, A.; Brancaccio, Y.; Averta, F.; Figliuzzi, M.M.; Fortunato, L.; Giudice, A. Primary Stability of Three Different Osteotomy Techniques in Medullary Bone: An in Vitro Study. Dent. J. 2020, 8, 21. [Google Scholar] [CrossRef] [Green Version]
- Di Domênico, M.B.; Collares, K.F.; Bergoli, C.D.; Dos Santos, M.B.F.; Corazza, P.H.; Özcan, M. Factors related to early marginal bone loss in dental implants—A multicentre observational clinical study. Appl. Sci. 2021, 11, 11197. [Google Scholar] [CrossRef]
- Gehrke, S.A.; Júnior, J.A.; Treichel, T.L.E.; do Prado, T.D.; Dedavid, B.A.; de Aza, P.N. Effects of insertion torque values on the marginal bone loss of dental implants installed in sheep mandibles. Sci. Rep. 2022, 12, 538. [Google Scholar] [CrossRef]
- Raz, P.; Meir, H.; Levartovsky, S.; Sebaoun, A.; Beitlitum, I. Primary Implant Stability Analysis of Different Dental Implant Connections and Designs-An In Vitro Comparative Study. Materials 2022, 15, 3072. [Google Scholar] [CrossRef]
- Kołaciński, M.; Kozakiewicz, M.; Materka, A. Textural entropy as a potential feature for quantitative assessment of jaw bone healing process. Arch. Med. Sci. 2015, 11, 78–84. [Google Scholar] [CrossRef]
- Kozakiewicz, M.; Wach, T. New oral surgery materials for bone reconstruction-a comparison of five bone substitute materials for dentoalveolar augmentation. Materials 2020, 13, 2935. [Google Scholar] [CrossRef] [PubMed]
- Wach, T.; Kozakiewicz, M. Are recent available blended collagen-calcium phosphate better than collagen alone or crystalline calcium phosphate? Radiotextural analysis of a 1-year clinical trial. Clin. Oral Investig. 2021, 25, 3711–3718. [Google Scholar] [CrossRef] [PubMed]
- Wach, T.; Kozakiewicz, M. Fast-versus slow-resorbable calcium phosphate bone substitute materials-texture analysis after 12 months of observation. Materials 2020, 13, 3854. [Google Scholar] [CrossRef] [PubMed]
- Kozakiewicz, M.; Bogusiak, K.; Hanclik, M.; Denkowski, M.; Arkuszewski, P. Noise in subtraction images made from pairs of intraoral radiographs: A comparison between four methods of geometric alignment. Dentomaxillofacial Radiol. 2008, 37, 40–46. [Google Scholar] [CrossRef]
- Szczypiński, P.M.; Strzelecki, M.; Materka, A.; Klepaczko, A. MaZda—A software package for image texture analysis. Comput. Methods Programs Biomed. 2009, 94, 66–76. [Google Scholar] [CrossRef]
- Hof, M.; Pommer, B.; Strbac, G.D.; Vasak, C.; Agis, H.; Zechner, W. Impact of insertion torque and implant neck design on peri-implant bone level: A randomized split-mouth trial. Clin. Implant Dent. Relat. Res. 2014, 16, 668–674. [Google Scholar] [CrossRef]
- Ajanović, M.; Hamzić, A.; Redžepagić, S.; Kamber-Ćesir, A.; Kazazić, L.; Tosum, S. Radiografska procjena gubitka alveolarne kosti oko zubnih implantata u maksili i mandibuli: Jednogodišnje prospektivno kliničko istraživanje. Acta Stomatol. Croat. 2015, 49, 128–136. [Google Scholar] [CrossRef]
- Gheisari, R.; Eatemadi, H.; Alavian, A. Comparison of the Marginal Bone Loss in One-stage versus Two-stage Implant Surgery. J. Dent. 2017, 18, 272–276. [Google Scholar]
- Comparison, L.T.; Beta, T.; Phosphates, T.; Surgery, O. Long Term Comparison of Application of Two Beta—Tricalcium Phosphates in Oral Surgery Porównanie odległych wyników leczenia z zastosowaniem. Dent. Med. Probl. 2009, 46, 384–388. [Google Scholar]
- Kozakiewicz, M.; Skorupska, M. What Does Bone Corticalization around Dental Implants Mean in Light of Ten Years of Follow-Up? J. Clin. Med. 2022, 11, 3545. [Google Scholar] [CrossRef] [PubMed]
- Marcin Kozakiewicz, K.G. Zastosowanie dyskretnej transformacji falkowej do matematycznego opisu radiotekstury kości żuchwy po zabiegach implantologicznych. Mag. Stomatol. 2009, 19, 90–93. [Google Scholar]
- Patil, Y.B.; Asopa, S.J.; Deepa, D.; Goel, A.; Jyoti, D.; Somayaji, N.S.; Sabharwal, R. Influence of Implant Neck Design on Crestal Bone Loss: A Comparative Study. Niger. J. Surg. Off. Publ. Niger. Surg. Res. Soc. 2020, 26, 22–27. [Google Scholar]
- Lovatto, S.T.; Bassani, R.; Sarkis-Onofre, R.; dos Santos, M.B.F. Influence of Different Implant Geometry in Clinical Longevity and Maintenance of Marginal Bone: A Systematic Review. J. Prosthodont. 2019, 28, e713–e721. [Google Scholar] [CrossRef]
- Valderrama, P.; Bornstein, M.M.; Jones, A.A.; Wilson, T.G.; Higginbottom, F.L.; Cochran, D.L. Effects of implant design on marginal bone changes around early loaded, chemically modified, sandblasted Acid-etched-surfaced implants: A histologic analysis in dogs. J. Periodontol. 2011, 82, 1025–1034. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Implant Name | Titanium Alloy No. | Insertion Level | Connection Type | Connection Shape | Neck Shape | Neck Microthreads | Body Shape | Body Threads | Apex Shape | Apex Hole | Apex Groove |
|---|---|---|---|---|---|---|---|---|---|---|---|
| AB Dental Devices I5 | Grade 5 | Bone level | Internal | Hexagon | Straight | No | Tapered | Square | Flat | No hole | Yes |
| ADIN Dental Implants Touareg | Grade 5 | Bone level | Internal | Hexagon | Straight | Yes | Tapered | Square | Flat | No hole | Yes |
| Alpha Bio ATI | Grade 5 | Bone level | Internal | Hexagon | Straight | Yes | Straight | Square | Flat | No hole | Yes |
| Alpha Bio OCI | Grade 5 | Bone level | Internal | Hexagon | Straight | No | Straight | No Threads | Dome | Round | No |
| Alpha Bio DFI | Grade 5 | Bone level | Internal | Hexagon | Straight | Yes | Tapered | Square | Flat | No hole | Yes |
| Alpha Bio SFB | Grade 5 | Bone level | Internal | Hexagon | Straight | No | Tapered | V-shaped | Flat | No hole | Yes |
| Alpha Bio SPI | Grade 5 | Bone level | Internal | Hexagon | Straight | Yes | Tapered | Square | Flat | No hole | Yes |
| Argon Medical Prod. K3pro Rapid | Grade 4 | Subcrestal | Internal | Conical | Straight | Yes | Tapered | V-shaped | Dome | No hole | Yes |
| Bego Semados RI | Grade 4 | Bone level | Internal | Hexagon | Straight | Yes | Tapered | Reverse buttress | Cone | No hole | Yes |
| Dentium Super Line | Grade 5 | Bone level | Internal | Conical | Straight | No | Tapered | Buttress | Dome | No hole | Yes |
| Friadent Ankylos C/X | Grade 4 | Subcrestal | Internal | Conical | Straight | No | Tapered | V-shaped | Dome | No hole | Yes |
| Implant Direct InterActive | Grade 5 | Bone level | Internal | Conical | Straight | Yes | Tapered | Reverse buttress | Dome | No hole | Yes |
| Implant Direct Legacy 3 | Grade 5 | Bone level | Internal | Hexagon | Straight | Yes | Tapered | Reverse buttress | Dome | No hole | Yes |
| MIS BioCom M4 | Grade 5 | Bone level | Internal | Hexagon | Straight | No | Straight | V-shaped | Flat | No hole | Yes |
| MIS C1 | Grade 5 | Bone level | Internal | Conical | Straight | Yes | Tapered | Reverse buttress | Dome | No hole | Yes |
| MIS Seven | Grade 5 | Bone level | Internal | Hexagon | Straight | Yes | Tapered | Reverse buttress | Dome | No hole | Yes |
| Osstem Implant Company GS III | Grade 5 | Bone level | Internal | Conical | Straight | Yes | Tapered | V-shaped | Dome | No hole | Yes |
| SGS Dental P7N | Grade 5 | Bone level | Internal | Hexagon | Straight | Yes | Tapered | V-shaped | Flat | No hole | Yes |
| TBR Implanté | Grade 5 | Bone level | Internal | Octagon | Straight | No | Straight | No threads | Flat | Round | Yes |
| Wolf Dental Conical Screw-Type | Grade 4 | Bone level | Internal | Hexagon | Straight | No | Tapered | V-shaped | Cone | No Hole | Yes |
| Feature | Marginal Bone Loss | p-Value for MBL | Torque | p-Value for Torque |
|---|---|---|---|---|
| Mandible | 0.29 mm ± 0.98 | p < 0.01 | 42.5 ± 12.67 | p < 0.01 |
| Maxilla | 0.23 mm ± 0.91 | p < 0.01 | 41.04 ± 12.7 | p > 0.05 |
| Anterior | 0.32 mm ± 1 | p < 0.01 | 43.15 ± 11.31 | p < 0.01 |
| Posterior | 0.22 mm ± 0.91 | p < 0.01 | 41.08 ± 13.07 | p < 0.01 |
| Texture Feature | Value | p-Value | Reference |
|---|---|---|---|
| SumAverg | 63.22 ± 2.32 | p < 0.05 | Trabecular Bone |
| Entropy | 2.70 ± 0.24 | p < 0.05 | Trabecular Bone |
| DifEntr | 1.25 ± 0.12 | p < 0.05 | Trabecular Bone |
| LngREmph | 1.53 ± 0.75 | p < 0.05 | Trabecular Bone |
| ShrtREmph | 0.90 ± 0.05 | p < 0.05 | Trabecular Bone |
| WavEnLH_s-4 | 131.03 ± 94.39 | p < 0.05 | Trabecular Bone |
| WavEnLH_s-5 | 313.35 ± 213.69 | p < 0.05 | Trabecular Bone |
| WavEnHH_s-5 | 42.36 ± 44.35 | p < 0.05 | Trabecular Bone |
| Texture Feature | Value at 00M | p-Value 00M | Value at 03M for the Area with MBL | Value at 03M for the Area without MBL | p-Value 03M | Reference Value for Trabecular Bone |
|---|---|---|---|---|---|---|
| SumAverg | 64.21 ± 2.9 | p > 0.05 | 64.35 ± 3.54 | 64.16 ± 3.85 | p < 0.05 | 63.22 ± 2.32 |
| Entropy | 2.58 ± 0.19 | p > 0.05 | 2.47 ± 0.21 | 2.52 ± 0.20 | p < 0.01 | 2.70 ± 0.24 |
| DifEntr | 1.11 ± 0.16 | p > 0.05 | 1.01 ± 0.15 | 1.04 ± 0.16 | p < 0.01 | 1.25 ± 0.12 |
| LngREmph | 1.71 ± 0.57 | p > 0.05 | 2.01 ± 0.55 | 1.97 ± 0.75 | p < 0.01 | 1.53 ± 0.75 |
| ShrtREmph | 0.88 ± 0.05 | p > 0.05 | 0.84 ± 0.05 | 0.85 ± 0.06 | p < 0.01 | 0.90 ± 0.05 |
| Texture Feature | Maxilla at 03M with MBL | Maxilla at 03M without MBL | p-Value for Maxilla | Mandible at 03M with | Mandible at 03M without | p-Value for Mandible |
|---|---|---|---|---|---|---|
| SumAverg | 64.42 ± 0.91 | 64.37 ± 1.20 | p > 0.05 | 64.76 ± 0.78 | 64.67 ± 0.89 | p > 0.05 |
| Entropy | 2.52 ± 0.16 | 2.57 ± 0.14 | p > 0.05 | 2.42 ± 0.16 | 2.50 ± 0.18 | p < 0.01 |
| DifEntr | 1.05 ± 0.16 | 1.08 ± 0.15 | p > 0.05 | 0.95 ± 0.14 | 1.01 ± 0.15 | p < 0.05 |
| LngREmph | 1.89 ± 0.43 | 1.84 ± 0.48 | p > 0.05 | 2.20 ± 0.68 | 2.11 ± 0.75 | p > 0.05 |
| ShrtREmph | 0.85 ± 0.05 | 0.86 ± 0.05 | p > 0.05 | 0.83 ± 0.6 | 0.84 ± 0.06 | p > 0.05 |
| WavEnLH_s-4 | 118.04 ± 87.24 | 122.93 ± 79.40 | p < 0.01 | 112.18 ± 116.14 | 120.90 ± 74.04 | p < 0.05 |
| WavEnLH_s-5 | 304.59 ± 208.42 | 308.534 ± 268.32 | p > 0.05 | 212.15 ± 185.22 | 287.54 ± 209.37 | p < 0.05 |
| WavEnHH_s-5 | 73.10 ± 65.97 | 63.89 ± 66.59 | p > 0.05 | 35.75 ± 38.44 | 63.21 ± 73.00 | p < 0.05 |
| Texture Feature | Maxilla at 00M before MBL Did Not Occur | Maxilla at 00M before MBL Occurred | Mandible at 00M before MBL Did Not Occur | Mandible at 00M before MBL Occurred |
|---|---|---|---|---|
| SumAverg | 64.14 ± 0.15 | 64.16 ± 1.22 | 64.52 ± 0.94 | 64.71 ± 1.14 |
| Entropy | 2.61 ± 0.14 | 2.58 ± 0.12 | 2.56 ± 0.14 | 2.58 ± 0.14 |
| DifEntr | 1.15 ± 0.15 | 1.13 ± 0.12 | 1.07 ± 0.14 | 1.07 ± 0.15 |
| LngREmph | 1.68 ± 0.41 | 1.75 ± 0.52 | 1.77 ± 0.42 | 1.74 ± 0.64 |
| ShrtREmph | 0.88 ± 0.05 | 0.87 ± 0.05 | 0.87 ± 0.5 | 0.88 ± 0.6 |
| WavEnLH_s-4 | 138.15 ± 94.13 | 142.92 ± 111.54 | 133.22 ± 86.73 | 134.35 ± 86.67 |
| WavEnLH_s-5 | 331.45 ± 283.28 | 339.16 ± 300.11 | 324.12 ± 222.26 | 345.23 ± 203.47 |
| WavEnHH_s-5 | 68.31 ± 88.00 | 69.94 ± 61.29 | 68.59 ± 75.42 | 61.28 ± 65.77 |
| Compared Implant Design Feature | MBL | p-Value |
|---|---|---|
| Bone-level implant | 0.26 ± 0.97 mm | p < 0.05 |
| Subcrestal implant | 0.09 ± 0.51 mm | |
| Neck microthreads | 0.25 ± 0.94 mm | p < 0.05 |
| Without neck microthreads | 0.31 ± 0.92 mm | |
| Without body threads | 0.99 ± 0.77 mm | p < 0.05 |
| V-shaped threads | 0.15 ± 0.64 mm | |
| Square threads | 0.28 ± 0.93 mm | |
| Buttress threads | 0.67 ± 1.75 mm | |
| Reverse buttress threads | 0.25 ± 0.97 mm |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wach, T.; Skorupska, M.; Trybek, G. Are Torque-Induced Bone Texture Alterations Related to Early Marginal Jawbone Loss? J. Clin. Med. 2022, 11, 6158. https://doi.org/10.3390/jcm11206158
Wach T, Skorupska M, Trybek G. Are Torque-Induced Bone Texture Alterations Related to Early Marginal Jawbone Loss? Journal of Clinical Medicine. 2022; 11(20):6158. https://doi.org/10.3390/jcm11206158
Chicago/Turabian StyleWach, Tomasz, Małgorzata Skorupska, and Grzegorz Trybek. 2022. "Are Torque-Induced Bone Texture Alterations Related to Early Marginal Jawbone Loss?" Journal of Clinical Medicine 11, no. 20: 6158. https://doi.org/10.3390/jcm11206158