
Core Lab Adjudication of the ACURATE neo2 Hemodynamic Performance Using Computed-Tomography-Corrected Left Ventricular Outflow Tract Area
 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Definition of Prosthesis Patient Mismatch (PPM)
- For patients with BMI < 30 kg/cm2; PPM is:
- -
- Hemodynamically insignificant if the indexed EOA is >0.85 cm2/m2.
- -
- Moderate if between 0.66 and 0.85 cm2/m2.
- -
- Severe if ≤0.65 cm2/m2.
- For obese patients with BMI ≥ 30 kg/m2; PPM is:
- -
- Hemodynamically insignificant if the indexed EOA is >0.70 cm2/m2.
- -
- Moderate if between 0.56 and 0.70 cm2/m2.
- -
- Severe if ≤0.55 cm2/m2.
2.2. Echocardiography
2.3. Multidetector Computerized Tomography (MDCT)
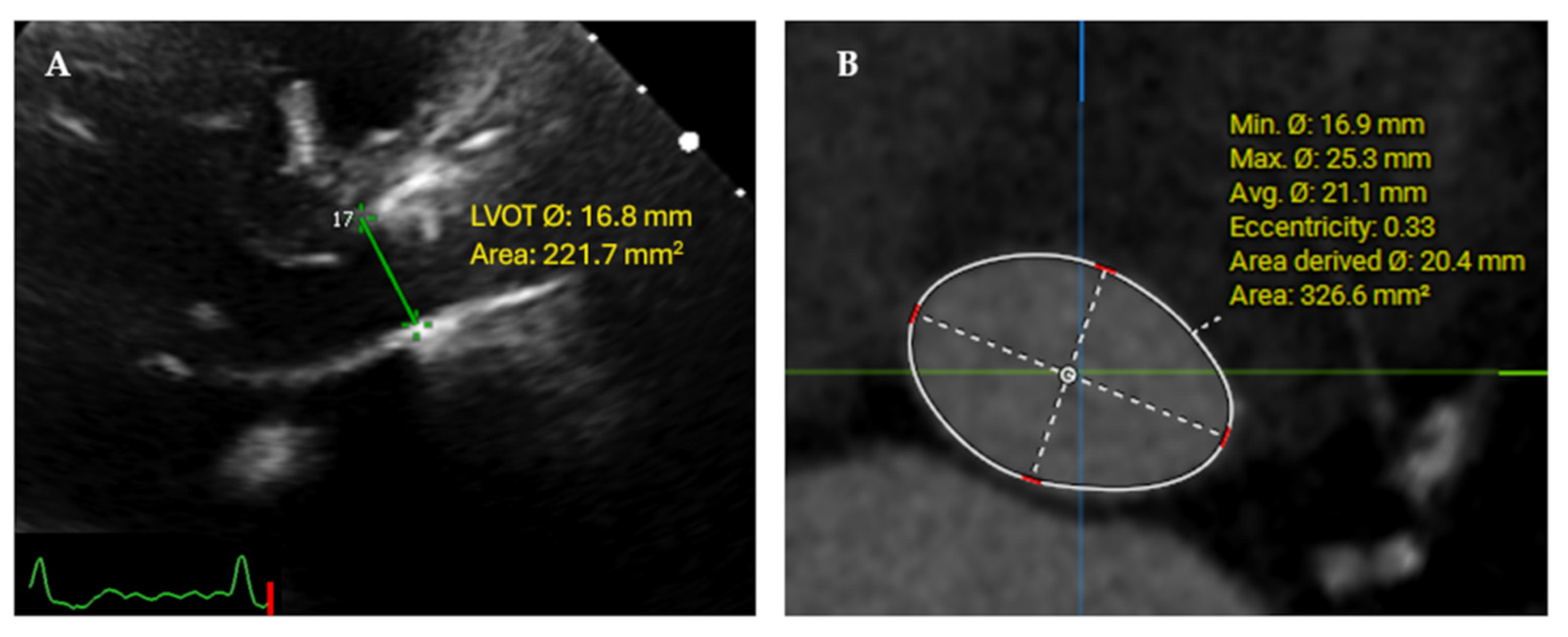
2.4. Corrected Continuity and Flow Equations
2.5. Statistical Analysis
3. Results
3.1. Hemodynamic Outcomes (Conventional 2D TTE and MSCT-Corrected Parameters)
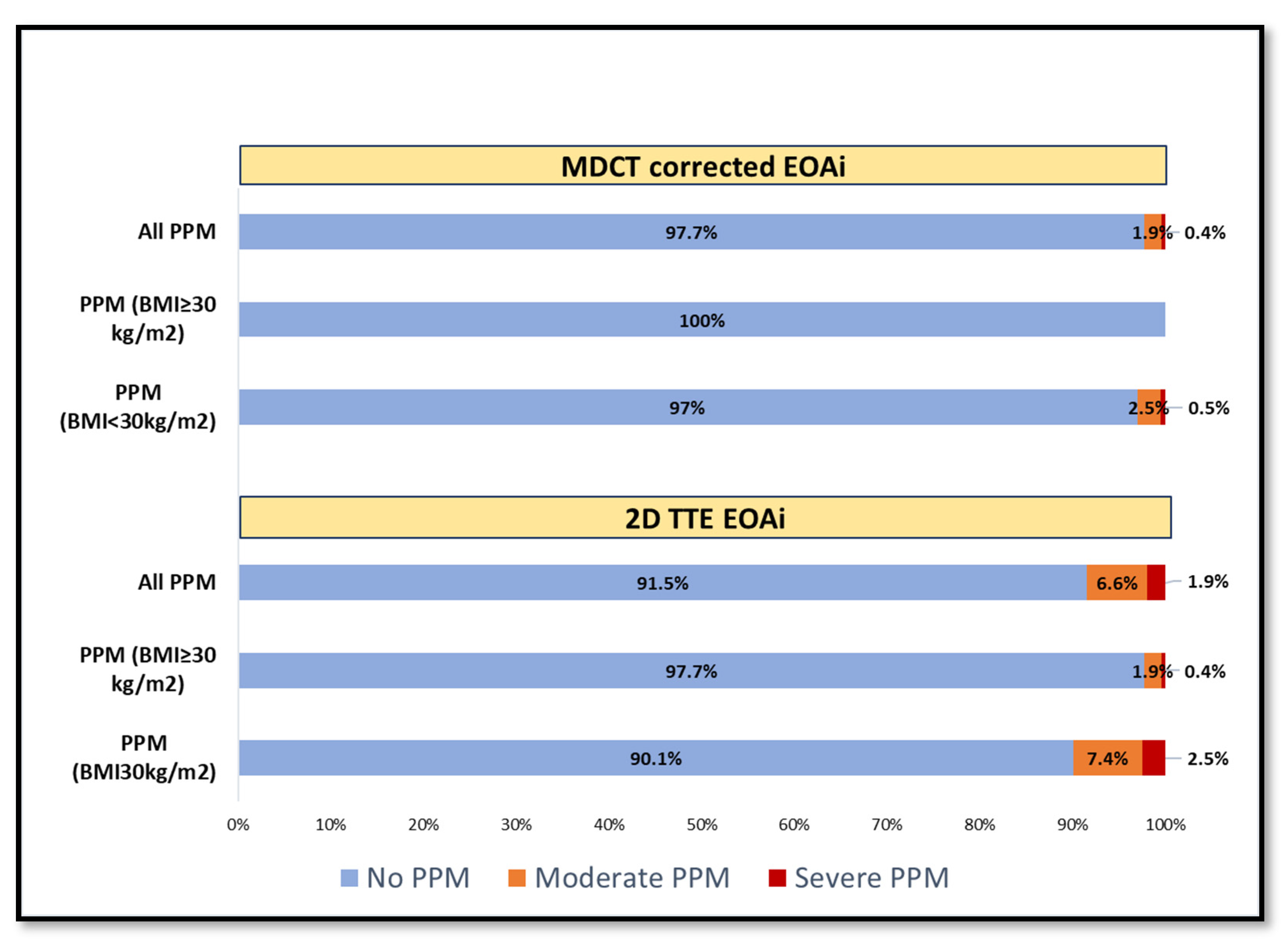
3.2. Prosthesis-Patient Mismatch (PPM) Incidence and Reclassification
3.3. Stroke Volume Index Changes in Patients with Low EF%
3.4. Inter Valve Size Differences in Hemodynamic Performance and Incidence of PPM
3.5. Intra-Observer and Inter-Observer Reliability
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2021, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2021, 77, e25–e197. [Google Scholar] [CrossRef] [PubMed]
- Lancellotti, P.; Pibarot, P.; Chambers, J.; Edvardsen, T.; Delgado, V.; Dulgheru, R.; Pepi, M.; Cosyns, B.; Dweck, M.R.; Garbi, M.; et al. Recommendations for the imaging assessment of prosthetic heart valves: A report from the European Association of Cardiovascular Imaging endorsed by the Chinese Society of Echocardiography, the Inter-American Society of Echocardiography, and the Brazilian Department of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 589–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- VARC-3 WRITING COMMITTEE; Genereux, P.; Piazza, N.; Alu, M.C.; Nazif, T.; Hahn, R.T.; Pibarot, P.; Bax, J.J.; Leipsic, J.A.; Blanke, P.; et al. Valve Academic Research Consortium 3: Updated endpoint definitions for aortic valve clinical research. Eur. Heart J. 2021, 42, 1825–1857. [Google Scholar] [CrossRef]
- Zoghbi, W.A.; Chambers, J.B.; Dumesnil, J.G.; Foster, E.; Gottdiener, J.S.; Grayburn, P.A.; Khandheria, B.K.; Levine, R.A.; Marx, G.R.; Miller, F.A., Jr.; et al. Recommendations for evaluation of prosthetic valves with echocardiography and doppler ultrasound: A report From the American Society of Echocardiography’s Guidelines and Standards Committee and the Task Force on Prosthetic Valves, developed in conjunction with the American College of Cardiology Cardiovascular Imaging Committee, Cardiac Imaging Committee of the American Heart Association, the European Association of Echocardiography, a registered branch of the European Society of Cardiology, the Japanese Society of Echocardiography and the Canadian Society of Echocardiography, endorsed by the American College of Cardiology Foundation, American Heart Association, European Association of Echocardiography, a registered branch of the European Society of Cardiology, the Japanese Society of Echocardiography, and Canadian Society of Echocardiography. J. Am. Soc. Echocardiogr. 2009, 22, 975–1014. [Google Scholar] [CrossRef]
- Zoghbi, W.A.; Asch, F.M.; Bruce, C.; Gillam, L.D.; Grayburn, P.A.; Hahn, R.T.; Inglessis, I.; Islam, A.M.; Lerakis, S.; Little, S.H.; et al. Guidelines for the Evaluation of Valvular Regurgitation After Percutaneous Valve Repair or Replacement: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Angiography and Interventions, Japanese Society of Echocardiography, and Society for Cardiovascular Magnetic Resonance. J. Am. Soc. Echocardiogr. 2019, 32, 431–475. [Google Scholar] [CrossRef]
- Baumgartner, H.; Hung, J.; Bermejo, J.; Chambers, J.B.; Edvardsen, T.; Goldstein, S.; Lancellotti, P.; LeFevre, M.; Miller, F., Jr.; Otto, C.M. Recommendations on the Echocardiographic Assessment of Aortic Valve Stenosis: A Focused Update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2017, 30, 372–392. [Google Scholar] [CrossRef]
- Maes, F.; Pierard, S.; de Meester, C.; Boulif, J.; Amzulescu, M.; Vancraeynest, D.; Pouleur, A.C.; Pasquet, A.; Gerber, B.; Vanoverschelde, J.L. Impact of left ventricular outflow tract ellipticity on the grading of aortic stenosis in patients with normal ejection fraction. J. Cardiovasc. Magn. Reson. 2017, 19, 37. [Google Scholar] [CrossRef] [Green Version]
- Mollmann, H.; Holzhey, D.M.; Hilker, M.; Toggweiler, S.; Schafer, U.; Treede, H.; Joner, M.; Sondergaard, L.; Christen, T.; Allocco, D.J.; et al. The ACURATE neo2 valve system for transcatheter aortic valve implantation: 30-day and 1-year outcomes. Clin. Res. Cardiol. 2021, 110, 1912–1920. [Google Scholar] [CrossRef]
- Rück, A.; Kim, W.-K.; Kawashima, H.; Abdelshafy, M.; Elkoumy, A.; Elzomor, H.; Wang, R.; Meduri, C.U.; Verouhis, D.; Saleh, N.; et al. Paravalvular Aortic Regurgitation Severity Assessed by Quantitative Aortography: ACURATE neo2 versus ACURATE neo Transcatheter Aortic Valve Implantation. J. Clin. Med. 2021, 10, 4627. [Google Scholar] [CrossRef]
- Blanke, P.; Weir-McCall, J.R.; Achenbach, S.; Delgado, V.; Hausleiter, J.; Jilaihawi, H.; Marwan, M.; Norgaard, B.L.; Piazza, N.; Schoenhagen, P.; et al. Computed tomography imaging in the context of transcatheter aortic valve implantation (TAVI)/transcatheter aortic valve replacement (TAVR): An expert consensus document of the Society of Cardiovascular Computed Tomography. J. Cardiovasc. Comput. Tomogr. 2019, 13, 1–20. [Google Scholar] [CrossRef]
- Fukui, M.; Garcia, S.; Lesser, J.R.; Gossl, M.; Tang, L.; Caye, D.; Newell, M.; Hashimoto, G.; Lopes, B.B.C.; Stanberry, L.I.; et al. Prosthesis-patient mismatch defined by cardiac computed tomography versus echocardiography after transcatheter aortic valve replacement. J. Cardiovasc. Comput. Tomogr. 2021, 15, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Churchill, J.; Hua, L.; Zeng, X.; Rhoades, V.; Namasivayam, M.; Baliyan, V.; Ghoshhajra, B.B.; Dong, T.; Dal-Bianco, J.P.; et al. Direct Planimetry of Left Ventricular Outflow Tract Area by Simultaneous Biplane Imaging: Challenging the Need for a Circular Assumption of the Left Ventricular Outflow Tract in the Assessment of Aortic Stenosis. J. Am. Soc. Echocardiogr. 2020, 33, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Weber, M.; Jaenisch, M.; Spilker, M.; Pingel, S.; Schueler, R.; Stundl, A.; Sedaghat, A.; Hammerstingl, C.; Mellert, F.; Grube, E.; et al. TAVR outcome after reclassification of aortic valve stenosis by using a hybrid continuity equation that combines computed tomography and echocardiography data. Catheter. Cardiovasc. Interv. 2020, 96, 958–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doddamani, S.; Bello, R.; Friedman, M.A.; Banerjee, A.; Bowers, J.H., Jr.; Kim, B.; Vennalaganti, P.R.; Ostfeld, R.J.; Gordon, G.M.; Malhotra, D.; et al. Demonstration of left ventricular outflow tract eccentricity by real time 3D echocardiography: Implications for the determination of aortic valve area. Echocardiography 2007, 24, 860–866. [Google Scholar] [CrossRef]
- Poh, K.K.; Levine, R.A.; Solis, J.; Shen, L.; Flaherty, M.; Kang, Y.J.; Guerrero, J.L.; Hung, J. Assessing aortic valve area in aortic stenosis by continuity equation: A novel approach using real-time three-dimensional echocardiography. Eur. Heart J. 2008, 29, 2526–2535. [Google Scholar] [CrossRef]
- Gaspar, T.; Adawi, S.; Sachner, R.; Asmer, I.; Ganaeem, M.; Rubinshtein, R.; Shiran, A. Three-dimensional imaging of the left ventricular outflow tract: Impact on aortic valve area estimation by the continuity equation. J. Am. Soc. Echocardiogr. 2012, 25, 749–757. [Google Scholar] [CrossRef]
- Mooney, J.; Sellers, S.L.; Blanke, P.; Pibarot, P.; Hahn, R.T.; Dvir, D.; Douglas, P.S.; Weissman, N.J.; Kodali, S.K.; Thourani, V.H.; et al. CT-Defined Prosthesis-Patient Mismatch Downgrades Frequency and Severity, and Demonstrates No Association With Adverse Outcomes after Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2017, 10, 1578–1587. [Google Scholar] [CrossRef]
- He, S.; Fang, Z. Incidence, predictors, and outcome of prosthesis-patient mismatch after transcatheter aortic valve replacement: A meta-analysis. Medicine 2020, 99, e20717. [Google Scholar] [CrossRef]
- Miyasaka, M. Prosthesis-patient mismatch after transcatheter aortic valve implantation. Cardiovasc. Interv. Ther. 2022, 37, 615–625. [Google Scholar] [CrossRef]
- Leone, P.P.; Regazzoli, D.; Pagnesi, M.; Sanz-Sanchez, J.; Chiarito, M.; Cannata, F.; Van Mieghem, N.M.; Barbanti, M.; Tamburino, C.; Teles, R.; et al. Predictors and Clinical Impact of Prosthesis-Patient Mismatch after Self-Expandable TAVR in Small Annuli. JACC Cardiovasc. Interv. 2021, 14, 1218–1228. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | n = 258 |
|---|---|
| Age | 81.6 (6.1) |
| Women | 168 (65%) |
| Body surface area, m2 | 1.8 [1.7–2.0] |
| Body mass index, kg/m2 Body mass index < 30 kg/m2 Body mass index ≥ 30 kg/m2 | 26 [23.7–29.3] 204 (79%) 54 (21%) |
| Euroscore II, % | 3.34 [2.15–3.5] |
| Hypertension | 212 (82.2%) |
| Diabetes mellitus Type I Diabetes mellitus Type II | 32 (12.4%) 49 (19%) |
| Baseline creatinine, mg/dL | 1.0 [0.8–1.3] |
| Prior Atrial fibrillation | 102 (39.5%) |
| Chronic lung obstructive disease | 39 (15.1%) |
| Prior stroke or TIA | 33 (12.8%) |
| Peripheral arterial disease | 30 (11.6) |
| Prior permanent pacemaker implantation | 26 (10.1%) |
| Previous cardiac surgery | 30 (11.6%) |
| Previous CABG | 15 (5.8%) |
| Previous PCI | 51 (19.8) |
| New York Heart Association (NYHA) class | |
| Class II Class III Class IV | 86 (33.3%) 141 (54.7%) 25 (9.7%) |
| Valve-in-Valve procedure (TAVI-in-SAVR) | 6 (2.3%) |
| Preprocedural 2D-TTE characteristics | |
| LV Ejection fraction, % | 60 [55–65] |
| Aortic valve maximum velocity, m/s | 4.29 (0.56) |
| Mean pressure gradient, mmHg | 43.6 [35–52] |
| Aortic valve effective orifice area, cm2 | 0.7 [0.6–0.8] |
| Moderate-severe aortic regurgitation | 28 (10.9%) |
| Moderate-severe mitral regurgitation | 38 (14.8%) |
| Moderate-severe tricuspid regurgitation | 21 (8.2%) |
| Pre-procedural MDCT characteristics | |
| Bicuspid Aortic Valve (Type I) | 8 (3.1%) |
| Native aortic annulus area, mm2 | 430.2 (62.9) |
| MDCT-derived LVOT measurements | |
| Minimum diameter, mm Maximum diameter, mm LVOT area, mm2 | 19.03 (2.55) 26.92 (2.43) 405.22 (81.32) |
| n (%) | |
|---|---|
| Vascular access | |
| Transfemoral | 258 (100%) |
| Balloon pre-dilatation | 211 (81.8%) |
| ACURATEneo2 size | |
| Small {23 mm} Medium {25 mm} Large {27 mm} | 59 (22.9%) 101 (39.1%) 98 (38%) |
| Balloon post-dilatation | 106 (41.1%) |
| Valve embolization | 1 (0.4%) |
| Need for second valve implantation | 1 (0.4%) |
| Annular injury (rupture) | 0 |
| Cardiac tamponade | 0 |
| Procedural death | 0 |
| Coronary obstruction | 0 |
| New postoperative permanent pacemaker | 18 (7%) |
| Major vascular complications | 4 (1.6%) |
| Major bleeding | 4 (1.6%) |
| Life-threatening bleeding | 3 (1.2%) |
| In-hospital stroke | 7 (2.7%) |
| Conversion to surgery | 0 |
| New dialysis | 0 |
| All-cause mortality | 0 |
| TTE (n = 258) | |
|---|---|
| LV ejection fraction, % | 58.9 (9.8) |
| AV maximum velocity, m/s | 1.98 (0.44) |
| AV mean pressure gradient, mmHg | 7.22 (3.11) |
| Dimensionless velocity index | 0.64 (0.13) |
| Systolic pulmonary artery pressure, mmHg | 36.8 [29.5–44.1] |
| Post-TAVI aortic regurgitation | |
| None/trace Mild Moderate | 154 (59.7%) 94 (36.4%) 5 (1.9%) |
| Moderate–severe mitral regurgitation | 36 (15.2%) |
| Moderate–severe tricuspid regurgitation | 49 (24.5%) |
| TTE | MSCT | 95% CrI of Difference | |
|---|---|---|---|
| LVOT diameter, mm | 21.03 (1.9) | Minimum diameter 19.03 (2.55) | [1.7, 2.31] |
| Maximum diameter 26.92 (2.43) | [−6.2, −5.58] | ||
| LVOT area, mm2 | 350.4 (62.04) | 405.22 (81.32) | [−55.15, −36.09] |
| EOA, cm2 | 2.25 (0.59) | 2.58 (0.63) | [−0.85, −0.43] |
| EOA index, cm2/m2 | 1.20 (0.32) | 1.41 (0.34) | [−0.207, −0.136] |
| LVOT SV, mL | 73.88 (21.41) | 84.47 (22.66) | [−14.45, −0.14] |
| LVOT SV index, mL/m2 | 41.0 (12.6) | 46.14 (12) | [−0.207, −0.136] |
Prosthesis-Patient Mismatch (PPM)
| 22 (8.52%) | 6 (2.32%) | |
| BMI < 30 kg/m2 | |||
| Moderate PPM | 15 (7.3%) | 5 (2.5%) | |
| Severe PPM | 5 (2.5%) | 1 (0.5%) | |
| BMI ≥ 30 kg/m2 | |||
| Moderate PPM | 2 (3.7%) | 0 | |
| Severe PPM | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elkoumy, A.; Rück, A.; Kim, W.-K.; Abdel-Wahab, M.; Abdelshafy, M.; De Backer, O.; Elzomor, H.; Hengstenberg, C.; Mohamed, S.K.; Saleh, N.; et al. Core Lab Adjudication of the ACURATE neo2 Hemodynamic Performance Using Computed-Tomography-Corrected Left Ventricular Outflow Tract Area. J. Clin. Med. 2022, 11, 6103. https://doi.org/10.3390/jcm11206103
Elkoumy A, Rück A, Kim W-K, Abdel-Wahab M, Abdelshafy M, De Backer O, Elzomor H, Hengstenberg C, Mohamed SK, Saleh N, et al. Core Lab Adjudication of the ACURATE neo2 Hemodynamic Performance Using Computed-Tomography-Corrected Left Ventricular Outflow Tract Area. Journal of Clinical Medicine. 2022; 11(20):6103. https://doi.org/10.3390/jcm11206103
Chicago/Turabian StyleElkoumy, Ahmed, Andreas Rück, Won-Keun Kim, Mohamed Abdel-Wahab, Mahmoud Abdelshafy, Ole De Backer, Hesham Elzomor, Christian Hengstenberg, Sameh K. Mohamed, Nawzad Saleh, and et al. 2022. "Core Lab Adjudication of the ACURATE neo2 Hemodynamic Performance Using Computed-Tomography-Corrected Left Ventricular Outflow Tract Area" Journal of Clinical Medicine 11, no. 20: 6103. https://doi.org/10.3390/jcm11206103