
The Effects of Device-Based Cardiac Contractility Modulation Therapy on Left Ventricle Global Longitudinal Strain and Myocardial Mechano-Energetic Efficiency in Patients with Heart Failure with Reduced Ejection Fraction
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
- (1)
- left ventricular ejection fraction ≤ 40%,
- (2)
- New York Heart Association Class (NYHA) II-IV,
- (3)
- Persistence of HF-related symptoms and/or >2 unplanned HF-related visits or hospitalization in the last 12 months despite optimal medical therapy (OMT),
- (4)
- QRS duration < 120 ms.
- (1)
- acute coronary syndrome in the previous three months,
- (2)
- cardiac resynchronization therapy device implantation in the previous 12 months,
- (3)
- absence of aortic stenosis or left ventricular outflow tract (LVOT) obstruction,
- (4)
- non-target dose of OMT for HFrEF,
- (5)
- end-stage kidney disease required renal replacement therapy.
2.2. Echocardiography
2.3. MEE Evaluation
2.4. Statistical Analysis
3. Results
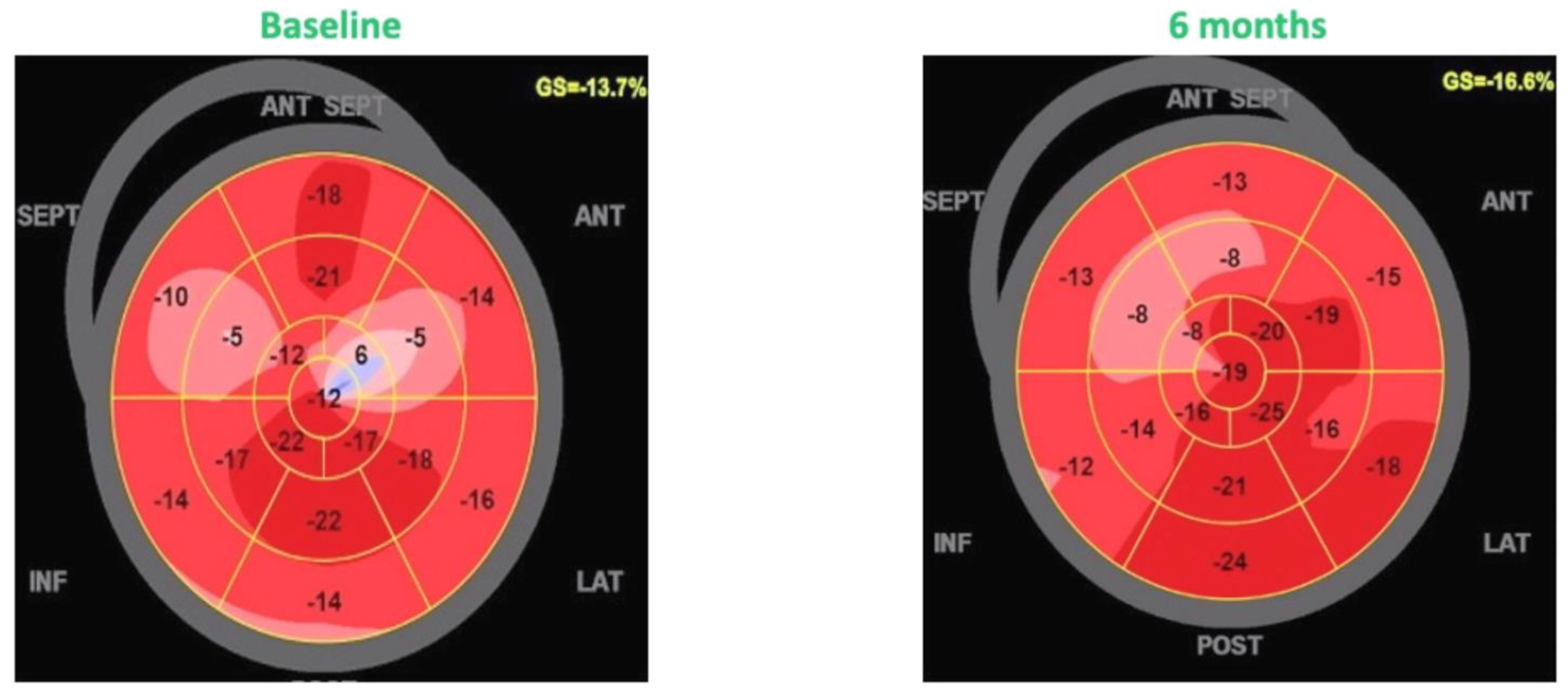
3.1. Effects of CCM Therapy on Left Ventricular Function
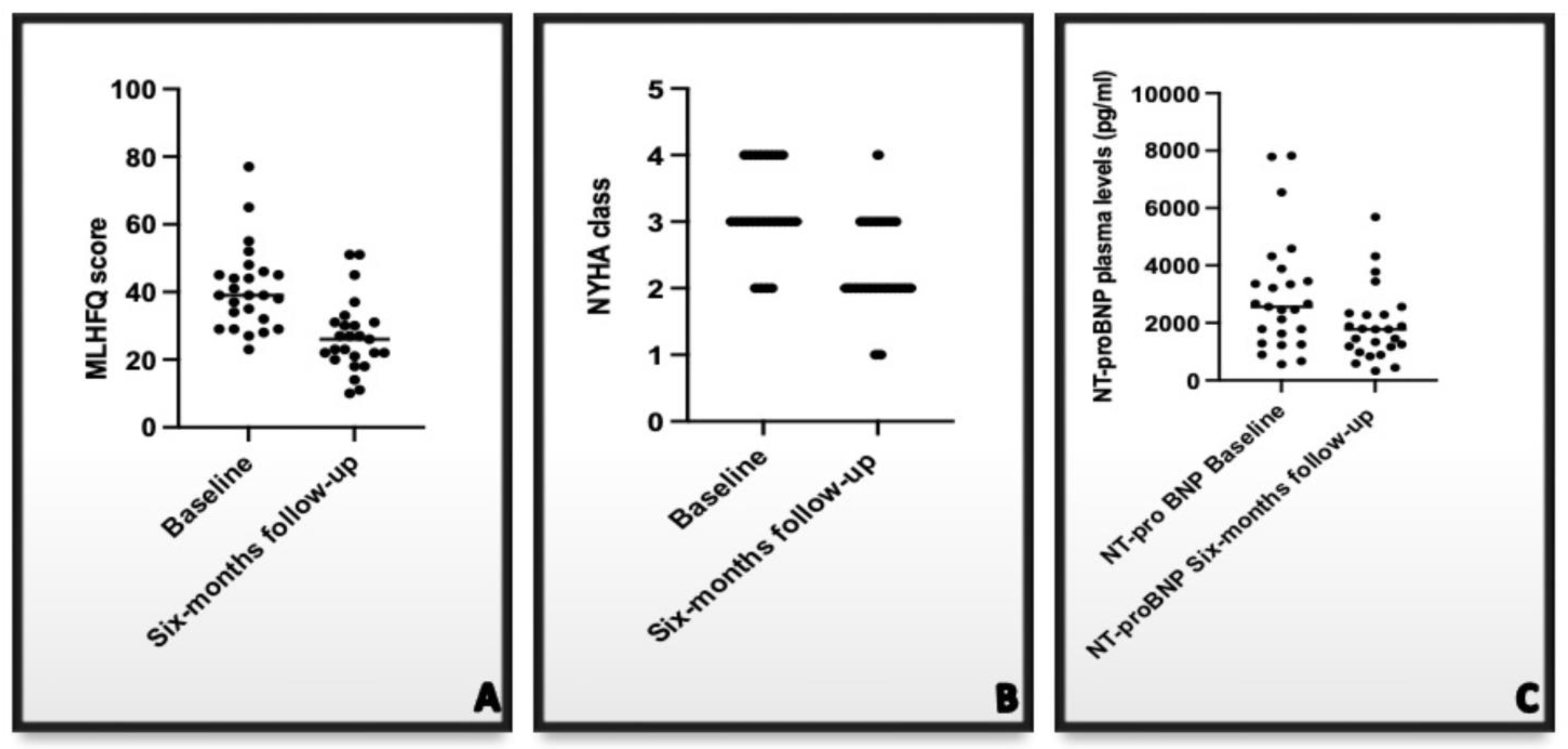
3.2. Effects of CCM Therapy on Natriuretic Peptides, NYHA Class, and Quality of Life
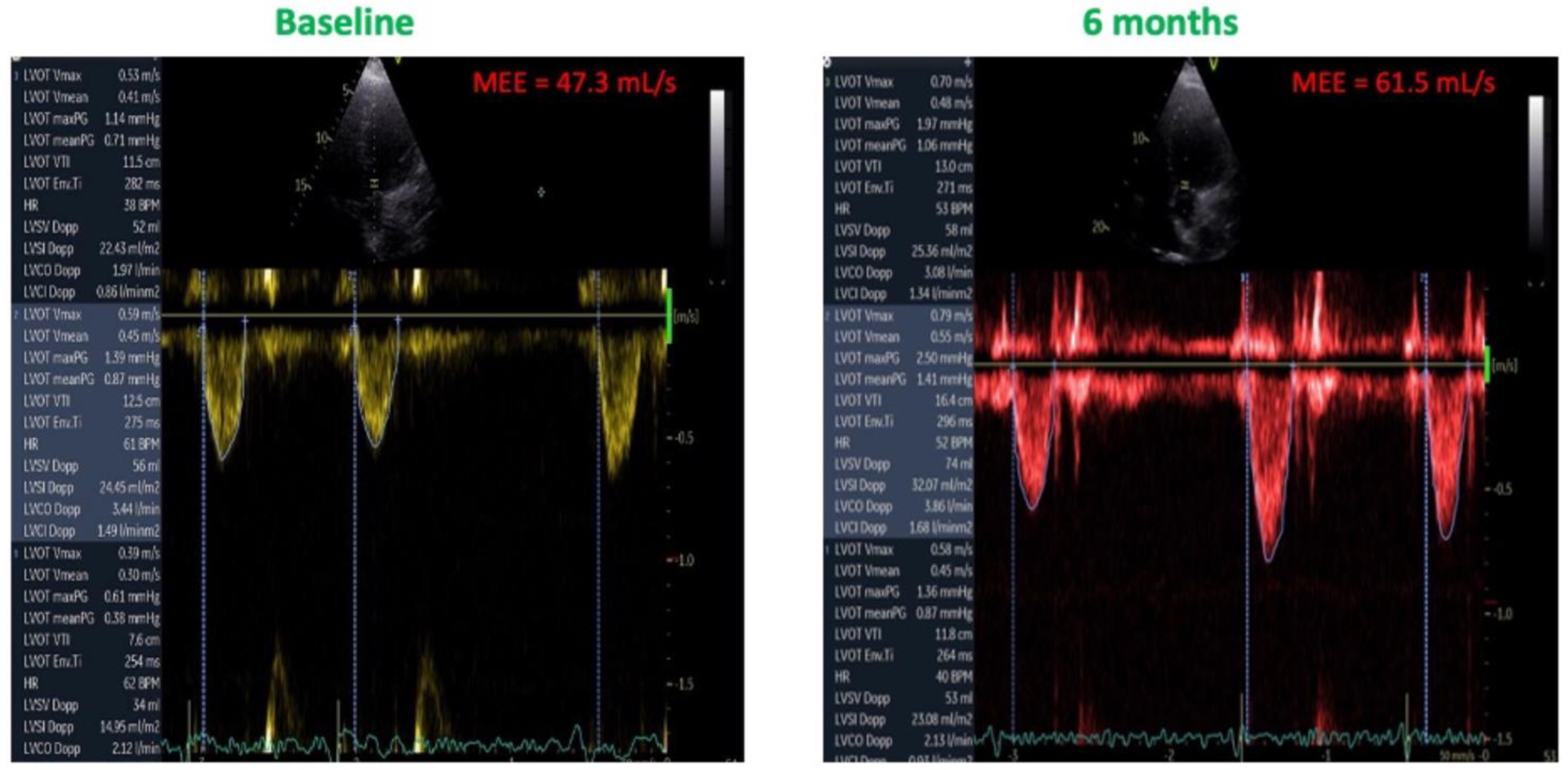
3.3. Effects of CCM on MEE
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferrara, F.; Capone, V.; Cademartiri, F.; Vriz, O.; Cocchia, R.; Ranieri, B.; Franzese, M.; Castaldo, R.; D’Andrea, A.; Citro, R.; et al. Physiologic Range of Myocardial Mechano-Energetic Efficiency among Healthy Subjects: Impact of Gender and Age. J. Pers. Med. 2022, 12, 996. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.S.; Izawa, H.; Sobue, T.; Ishihara, H.; Somura, F.; Nishizawa, T.; Nagata, K.; Iwase, M.; Yokota, M. Prognostic value of mechanical efficiency in ambulatory patients with idiopathic dilated cardiomyopathy in sinus rhythm. J. Am. Coll. Cardiol. 2002, 39, 1264–1268. [Google Scholar] [CrossRef] [Green Version]
- Knaapen, P.; Germans, T.; Knuuti, J.; Paulus, W.J.; Dijkmans, P.A.; Allaart, C.P.; Lammertsma, A.A.; Visser, F.C. Myocardial energetics and efficiency: Current status of the noninvasive approach. Circulation 2007, 115, 918–927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Losi, M.A.; Izzo, R.; Mancusi, C.; Wang, W.; Roman, M.J.; Lee, E.T.; Howard, B.V.; Devereux, R.B.; de Simone, G. Depressed Myocardial Energetic Efficiency Increases Risk of Incident Heart Failure: The Strong Heart Study. J. Clin. Med. 2019, 8, 1044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manzi, M.V.; Mancusi, C.; Lembo, M.; Esposito, G.; Rao, M.A.; de Simone, G.; Morisco, C.; Trimarco, V.; Izzo, R.; Trimarco, B. Low mechano-energetic efficiency is associated with future left ventricular systolic dysfunction in hypertensives. ESC Heart Fail. 2022, 9, 2291–2300. [Google Scholar] [CrossRef]
- Patel, P.A.; Nadarajah, R.; Ali, N.; Gierula, J.; Witte, K.K. Cardiac contractility modulation for the treatment of heart failure with reduced ejection fraction. Heart Fail Rev. 2021, 26, 217–226. [Google Scholar] [CrossRef]
- Gupta, R.C.; Mishra, S.; Rastogi, S.; Wang, M.; Rousso, B.; Mika, Y.; Remppis, A.; Sabbah, H.N. Ca(2+)-binding proteins in dogs with heart failure: Effects of cardiac contractility modulation electrical signals. Clin. Transl. Sci. 2009, 2, 211–215. [Google Scholar] [CrossRef] [Green Version]
- Rastogi, S.; Mishra, S.; Zacà, V.; Mika, Y.; Rousso, B.; Sabbah, H.N. Effects of chronic therapy with cardiac contractility modulation electrical signals on cytoskeletal proteins and matrix metalloproteinases in dogs with heart failure. Cardiology 2008, 110, 230–237. [Google Scholar] [CrossRef]
- Butter, C.; Rastogi, S.; Minden, H.H.; Meyhöfer, J.; Burkhoff, D.; Sabbah, H.N. Cardiac contractility modulation electrical signals improve myocardial gene expression in patients with heart failure. J. Am. Coll Cardiol. 2008, 51, 1784–1789. [Google Scholar] [CrossRef] [Green Version]
- Tschöpe, C.; Kherad, B.; Klein, O.; Lipp, A.; Blaschke, F.; Gutterman, D.; Burkhoff, D.; Hamdani, N.; Spillmann, F.; Van Linthout, S. Cardiac contractility modulation: Mechanisms of action in heart failure with reduced ejection fraction and beyond. Eur. J. Heart Fail. 2019, 21, 14–22. [Google Scholar] [CrossRef]
- Ning, B.; Zhang, F.; Song, X.; Hao, Q.; Li, Y.; Li, R.; Dang, Y. Cardiac contractility modulation attenuates structural and electrical remodeling in a chronic heart failure rabbit model. J. Int. Med. Res. 2020, 48, 300060520962910. [Google Scholar] [CrossRef] [PubMed]
- Giallauria, F.; Cuomo, G.; Parlato, A.; Raval, N.Y.; Kuschyk, J.; Stewart Coats, A.J. A comprehensive individual patient data meta-analysis of the effects of cardiac contractility modulation on functional capacity and heart failure-related quality of life. ESC Heart Fail. 2020, 7, 2922–2932. [Google Scholar] [CrossRef] [PubMed]
- Anker, S.D.; Borggrefe, M.; Neuser, H.; Ohlow, M.-A.; Röger, S.; Goette, A.; Remppis, B.A.; Kuck, K.; Najarian, K.B.; Gutterman, D.D.; et al. Cardiac contractility modulation improves long-term survival and hospitalizations in heart failure with reduced ejection fraction. Eur. J. Heart Fail. 2019, 21, 1103–1111. [Google Scholar] [CrossRef]
- Yücel, G.; Fastner, C.; Hetjens, S.; Toepel, M.; Schmiel, G.; Yazdani, B.; Husain-Syed, F.; Liebe, V.; Rudic, B.; Akin, I.; et al. Impact of baseline left ventricular ejection fraction on long-term outcomes in cardiac contractility modulation therapy. Pacing Clin. Electrophysiol. 2022, 45, 639–648. [Google Scholar] [CrossRef]
- Contaldi, C.; De Vivo, S.; Martucci, M.L.; D’Onofrio, A.; Ammendola, E.; Nigro, G.; Errigo, V.; Pacileo, G.; Masarone, D. Effects of Cardiac Contractility Modulation Therapy on Right Ventricular Function: An Echocardiographic Study. Appl. Sci. 2022, 2, 7917. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [Green Version]
- Quiñones, M.A.; Otto, C.M.; Stoddard, M.; Waggoner, A.; Zoghbi, W.A. Doppler Quantification Task Force of the Nomenclature and Standards Committee of the American Society of Echocardiography. Recommendations for quantification of Doppler echocardiography: A report from the Doppler Quantification Task Force of the Nomenclature and Standards Committee of the American Society of Echocardiography. J. Am. Soc Echocardiogr. 2002, 15, 167–184. [Google Scholar]
- Mitchell, C.; Rahko, P.S.; Blauwet, L.A.; Canaday, B.; Finstuen, J.A.; Foster, M.C.; Horton, K.; Ogunyankin, K.O.; Palma, R.A.; Velazquez, E.J. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2019, 32, 1–64. [Google Scholar] [CrossRef] [PubMed]
- Sattin, M.; Burhani, Z.; Jaidka, A.; Millington, S.J.; Arntfield, R.T. Stroke Volume Determination by Echocardiography. Chest 2022, 161, 1598–1605. [Google Scholar] [CrossRef] [PubMed]
- Tran, P.; Maddock, H.; Banerjee, P. Myocardial Fatigue: A Mechano-energetic Concept in Heart Failure. Curr. Cardiol. Rep. 2022, 24, 711–730. [Google Scholar] [CrossRef]
- Juszczyk, A.; Jankowska, K.; Zawiślak, B.; Surdacki, A.; Chyrchel, B. Depressed Cardiac Mechanical Energetic Efficiency: A Contributor to Cardiovascular Risk in Common Metabolic Diseases-From Mechanisms to Clinical Applications. J. Clin. Med. 2020, 9, 2681. [Google Scholar] [CrossRef]
- Ong, G.; Yan, A.T.; Connelly, K.A. Clinical application of echocardiographic-derived myocardial strain imaging in subclinical disease: A primer for cardiologists. Curr. Opin. Cardiol. 2019, 34, 147–155. [Google Scholar] [CrossRef]
- Haji, K.; Marwick, T.H. Clinical Utility of Echocardiographic Strain and Strain Rate Measurements. Curr. Cardiol. Rep. 2021, 23, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Tops, L.F.; Delgado, V.; Marsan, N.A.; Bax, J.J. Myocardial strain to detect subtle left ventricular systolic dysfunction. Eur. J. Heart Fail. 2017, 19, 307–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russo, C.; Jin, Z.; Elkind, M.S.; Rundek, T.; Homma, S.; Sacco, R.L.; Di Tullio, M.R. Prevalence and prognostic value of subclinical left ventricular systolic dysfunction by global longitudinal strain in a community-based cohort. Eur. J. Heart Fail. 2014, 16, 1301–1309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunckhorst, C.B.; Shemer, I.; Mika, Y.; Ben-Haim, S.A.; Burkhoff, D. Cardiac contractility modulation by non-excitatory currents: Studies in isolated cardiac muscle. Eur. J. Heart Fail. 2006, 8, 7–15. [Google Scholar] [CrossRef]
- Burkhoff, D.; Shemer, I.; Felzen, B.; Shimizu, J.; Mika, Y.; Dickstein, M.; Prutchi, D.; Darvish, N.; Ben-Haim, S.A. Electric currents applied during the refractory period can modulate cardiac contractility in vitro and in vivo. Heart Fail. Rev. 2001, 6, 27–34. [Google Scholar] [CrossRef]
- Endo, M. Calcium-induced calcium release in skeletal muscle. Physiol. Rev. 2009, 89, 1153–1176. [Google Scholar] [CrossRef] [Green Version]
- Imai, M.; Rastogi, S.; Gupta, R.C.; Mishra, S.; Sharov, V.G.; Stanley, W.C.; Mika, Y.; Rousso, B.; Burkhoff, D.; Ben-Haim, S.; et al. Therapy with cardiac contractility modulation electrical signals improves left ventricular function and remodeling in dogs with chronic heart failure. J. Am. Coll. Cardiol. 2007, 49, 2120–2128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smart, N.; Haluska, B.; Leano, R.; Case, C.; Mottram, P.M.; Marwick, T.H. Determinants of functional capacity in patients with chronic heart failure: Role of filling pressure and systolic and diastolic function. Am. Heart J. 2005, 149, 152–158. [Google Scholar] [CrossRef]
- Terzi, S.; Sayar, N.; Bilsel, T.; Enc, Y.; Yildirim, A.; Ciloğlu, F.; Yesilcimen, K. Tissue Doppler imaging adds incremental value in predicting exercise capacity in patients with congestive heart failure. Heart Vessel. 2007, 22, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Daullxhiu, I.; Haliti, E.; Poniku, A.; Ahmeti, A.; Hyseni, V.; Olloni, R.; Vela, Z.; Elezi, S.; Bajraktari, G.; Daullxhiu, T.; et al. Predictors of exercise capacity in patients with chronic heart failure. J. Cardiovasc. Med. 2011, 12, 223–225. [Google Scholar] [CrossRef] [PubMed]
- Bussoni, M.F.; Guirado, G.N.; Roscani, M.G.; Polegato, B.F.; Matsubara, L.S.; Bazan, S.G.; Matsubara, B. Diastolic function is associated with quality of life and exercise capacity in stable heart failure patients with reduced ejection fraction. Braz. J. Med. Biol. Res. 2013, 46, 803–838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohri, S.; He, K.L.; Dickstein, M.; Mika, Y.; Shimizu, J.; Shemer, I.; Yi, G.H.; Wang, J.; Ben-Haim, S.; Burkhoff, D. Cardiac contractility modulation by electric currents applied during the refractory period. Am. J. Physiol. Heart Circ. Physiol. 2002, 282, 1642–1647. [Google Scholar] [CrossRef] [Green Version]
- Butter, C.; Wellnhofer, E.; Schlegl, M.; Winbeck, G.; Fleck, E.; Sabbah, H.N. Enhanced inotropic state of the failing left ventricle by cardiac contractility modulation electrical signals is not associated with increased myocardial oxygen consumption. J. Card. Fail. 2007, 13, 137–142. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Overall Population (25) |
|---|---|
| Age (mean ± SD) | 62.8 ± 9.7 years |
| Female sex (n,%) | 3 (12%) |
| Ischemic etiology (n%) | 13 (52%) |
| Hypertension (n, %) | 12 (48%) |
| Diabetes (n,%) | 9 (36%) |
| COPD (n,%) | 7 (28%) |
| NYHA class II (n,%) | 4 (16%) |
| NYHA class III (n,%) | 13 (52%) |
| NYHA class IV (n, %) | 8 (32%) |
| ICD-DR (n,%) | 16 (64%) |
| S-ICD | 2 (8%) |
| CRT-D | 7 (28%) |
| SBP (mean ± SD) | 101 ± 11 mmHg |
| DBP (mean ± SD) | 72 ± 6 mmHg |
| NT-pro BNP (mean ± SD) | 2185 ± 1738 pg/mL |
| e-GFR (CKD-EPI) | 62.3 ± 12 ml/min/1.73 m2 |
| BUN/Creatinine | 18.4 ± 9.7 mg/dL |
| Atrial fibrillation | 9 (36%) |
| LVEDV (mean ± SD) | 208.2 ± 73.2 mL |
| LVESV (mean ± SD) | 125.3 ± 43.5 mL |
| LVEF (mean ± SD) | 32.8 ± 7.1% |
| LAVi | 41.9 ± 4.3 mL/m2 |
| E/e’ ratio | 16.3 ± 7.5 cm/sec |
| Loop diuretic (n,%) | 16 (64%) |
| Beta-Blockers (n,%) | 25 (100%) |
| ARNI (n%) | 25 (100%) |
| MRA (n,%) | 18 (72%) |
| Variable | Baseline | 6 Months Follow-Up | p-Value |
|---|---|---|---|
| LVEDV (mL) | 211.8 ± 45.8 | 188.3 ± 38.5 | 0.041 |
| LVESV (mL) | 141.8 ± 51.5 | 119.6 ± 49.7 | 0.024 |
| LVEF (%) | 32.8 ± 7.1 | 36.1 ± 6.9 | 0.032 |
| GLS (%) | −10.3 ± −2.7 | −12.9 ± −4.2 | 0.018 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masarone, D.; Kittleson, M.M.; De Vivo, S.; D’Onofrio, A.; Ammendola, E.; Nigro, G.; Contaldi, C.; Martucci, M.L.; Errigo, V.; Pacileo, G. The Effects of Device-Based Cardiac Contractility Modulation Therapy on Left Ventricle Global Longitudinal Strain and Myocardial Mechano-Energetic Efficiency in Patients with Heart Failure with Reduced Ejection Fraction. J. Clin. Med. 2022, 11, 5866. https://doi.org/10.3390/jcm11195866
Masarone D, Kittleson MM, De Vivo S, D’Onofrio A, Ammendola E, Nigro G, Contaldi C, Martucci ML, Errigo V, Pacileo G. The Effects of Device-Based Cardiac Contractility Modulation Therapy on Left Ventricle Global Longitudinal Strain and Myocardial Mechano-Energetic Efficiency in Patients with Heart Failure with Reduced Ejection Fraction. Journal of Clinical Medicine. 2022; 11(19):5866. https://doi.org/10.3390/jcm11195866
Chicago/Turabian StyleMasarone, Daniele, Michelle M. Kittleson, Stefano De Vivo, Antonio D’Onofrio, Ernesto Ammendola, Gerardo Nigro, Carla Contaldi, Maria L. Martucci, Vittoria Errigo, and Giuseppe Pacileo. 2022. "The Effects of Device-Based Cardiac Contractility Modulation Therapy on Left Ventricle Global Longitudinal Strain and Myocardial Mechano-Energetic Efficiency in Patients with Heart Failure with Reduced Ejection Fraction" Journal of Clinical Medicine 11, no. 19: 5866. https://doi.org/10.3390/jcm11195866