
Pulmonary Embolism in the Cancer Associated Thrombosis Landscape
 , , , and
, , , and
Abstract
:1. Introduction
2. Epidemiology
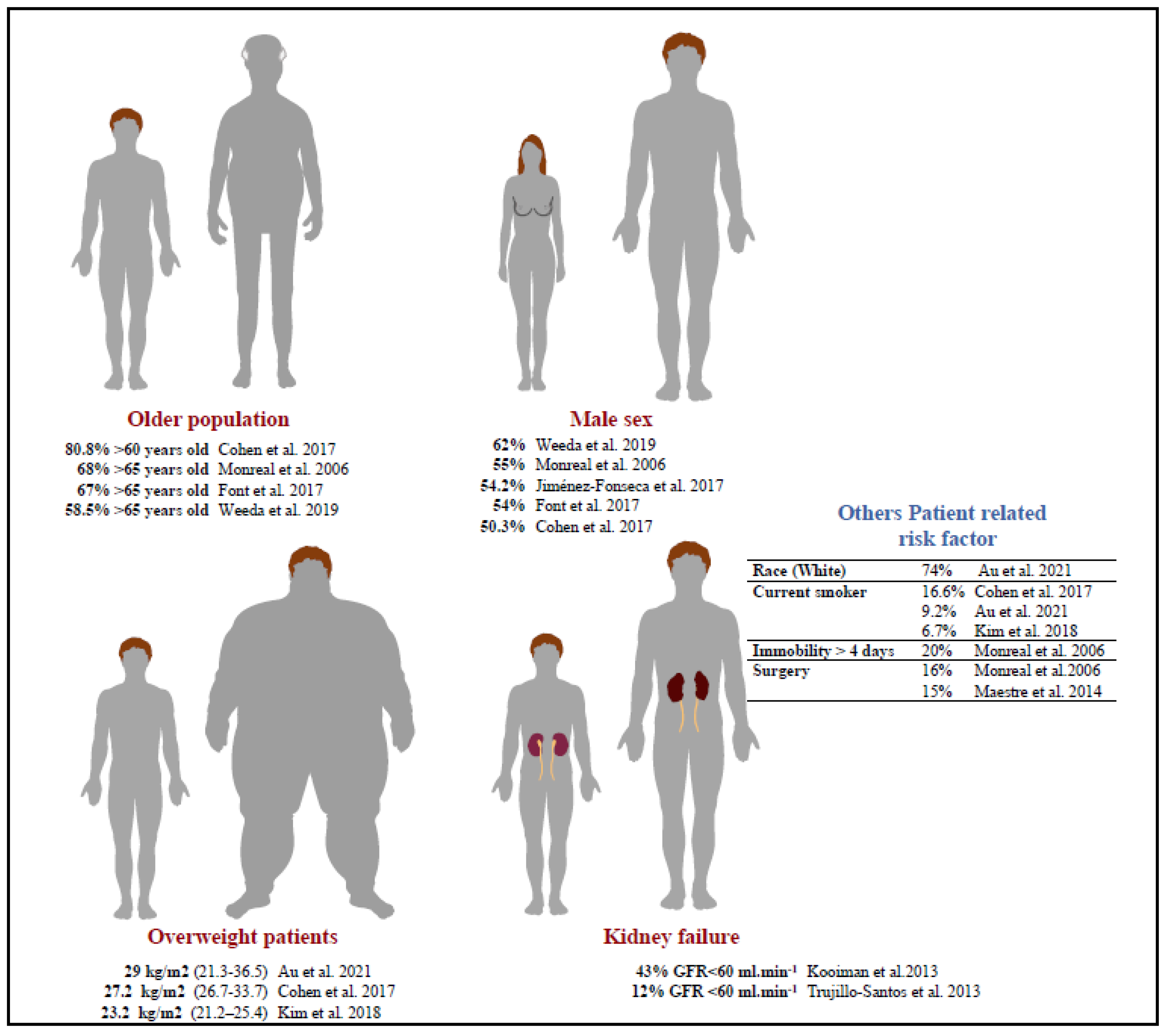
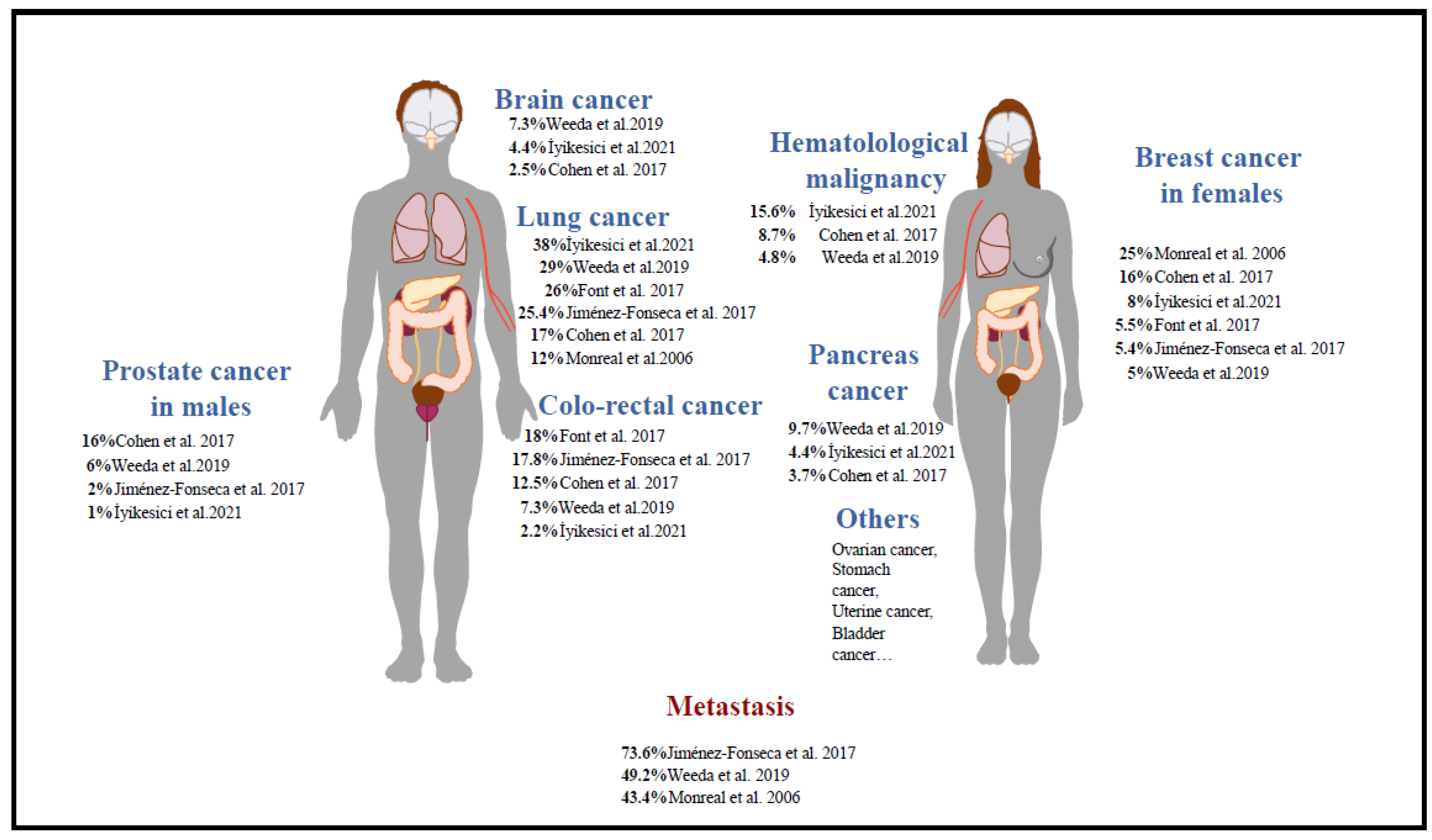
2.1. Demographic Characteristics
2.2. Demographic Characteristics
2.3. Risk of Recurrent PE in Cancer Patients
3. Diagnosis and Prognosis of PE in Cancer Patients
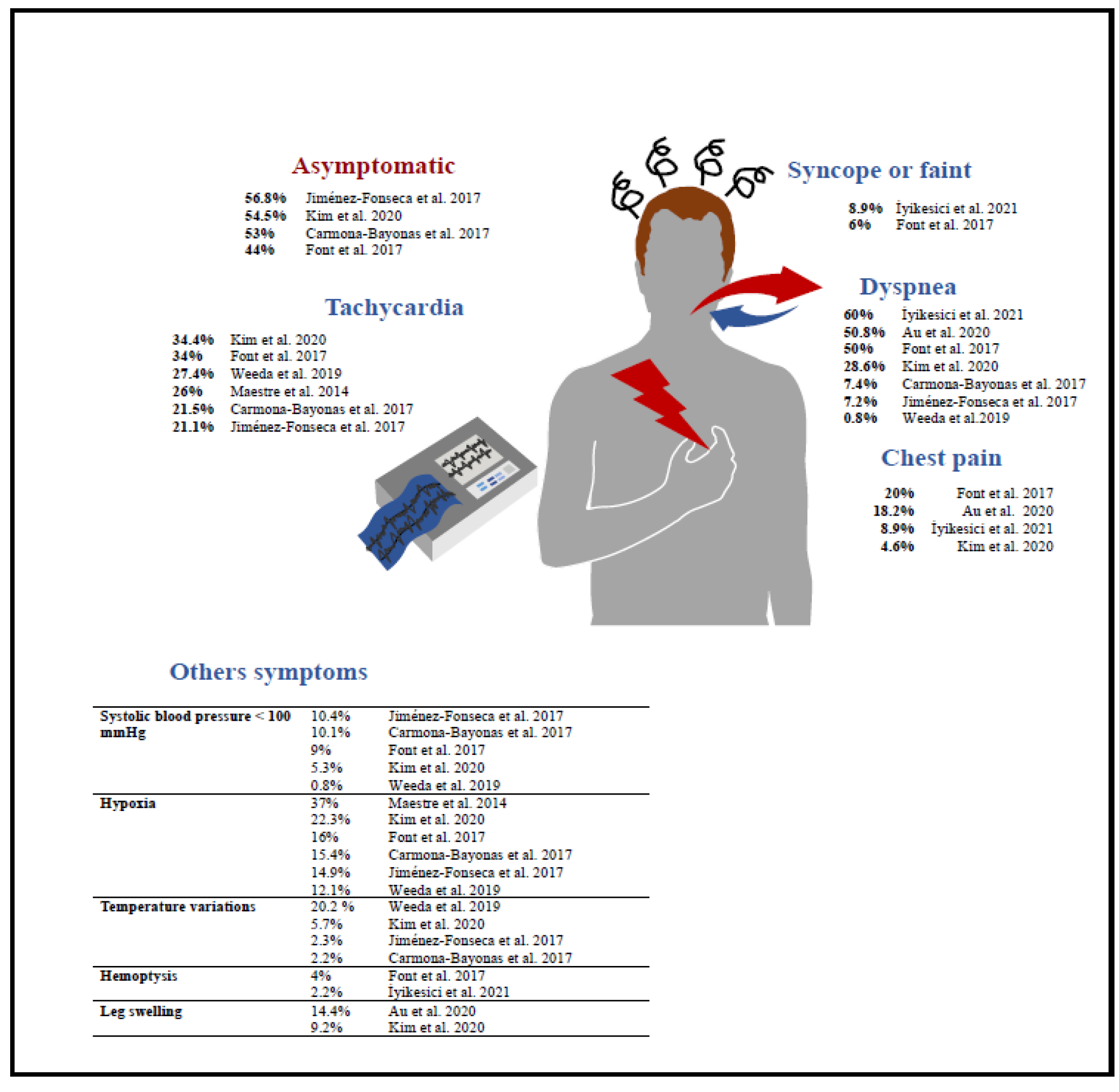
3.1. Symptomatic PE in Cancer Patients
3.2. Unsuspected PE in Cancer Patients
3.3. Subsegmental PE in Cancer Patients
3.4. Central Venous Catheter-Related Pulmonary Embolism in Cancer Patients
3.5. How to Assess the Risk of Mortality in PE Cancer Patients
4. Management of Cancer Patients with PE
4.1. Anticoagulation
4.2. Other Available Treatments of Pulmonary Embolism in Cancer Patients
5. What Are the Remaining Unmet Needs in Cancer Patients with PE?
5.1. How to Predict Better the Bleeding Risk in Cancer Patient with PE?
5.2. What Is the Best Secondary Prevention for the Management of PE in Cancer?
5.3. How to Screen for Post-PE Syndrome in Cancer Patients?
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Agnelli, G.; Verso, M. Management of venous thromboembolism in patients with cancer: Management of VTE in cancer patients. J. Thromb. Haemost. 2011, 9, 316–324. [Google Scholar] [CrossRef]
- Carson, J.L.; Kelley, M.A.; Duff, A.; Weg, J.G.; Fulkerson, W.J.; Palevsky, H.I.; Schwartz, J.S.; Thompson, B.T.; Popovich, J.; Hobbins, T.E. The Clinical Course of Pulmonary Embolism. N. Engl. J. Med. 1992, 326, 1240–1245. [Google Scholar] [CrossRef] [PubMed]
- Cai, B.; Bedayat, A.; George, E.; Hunsaker, A.R.; Dill, K.E.; Rybicki, F.J.; Kumamaru, K.K. Malignancy and Acute Pulmonary Embolism: Risk Stratification Including the Right to Left Ventricle Diameter Ratio in 1596 Subjects. J. Thorac. Imaging 2013, 28, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.T.; Katholing, A.; Rietbrock, S.; Bamber, L.; Martinez, C. Epidemiology of first and recurrent venous thromboembolism in patients with active cancer: A population-based cohort study. Thromb. Haemost. 2017, 117, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Au, C.; Gupta, E.; Khaing, P.; Dibello, J.; Chengsupanimit, T.; Mitchell, E.P.; West, F.M.; Baram, M.; Alwsare, B.K.; Kane, G.C. Clinical presentations and outcomes in pulmonary embolism patients with cancer. J. Thromb. Thrombolysis 2021, 51, 430–436. [Google Scholar] [CrossRef]
- Kim, M.S.; Chang, H.; Lee, S.Y.; Shin, S.H.; Park, H.; Chang, S.-A.; Park, T.K.; Kim, D.-K.; Kim, E.K. Differential clinical manifestations and clinical outcome of cancer-related pulmonary embolism. Korean J. Intern. Med. 2020, 35, 360–368. [Google Scholar] [CrossRef]
- Khorana, A.A.; Connolly, G.C. Assessing Risk of Venous Thromboembolism in the Patient with Cancer. J. Clin. Oncol. 2009, 27, 4839–4847. [Google Scholar] [CrossRef]
- Blom, J.W. Malignancies, Prothrombotic Mutations, and the Risk of Venous Thrombosis. JAMA 2005, 293, 715. [Google Scholar] [CrossRef]
- Monreal, M.; Falgá, C.; Valdés, M.; Suárez, C.; Gabriel, F.; Tolosa, C.; Montes, J.; Riete Investigators. Fatal pulmonary embolism and fatal bleeding in cancer patients with venous thromboembolism: Findings from the RIETE registry. J. Thromb. Haemost. 2006, 4, 1950–1956. [Google Scholar] [CrossRef]
- Font, C.; Carmona-Bayonas, A.; Beato, C.; Reig, Ò.; Sáez, A.; Jiménez-Fonseca, P.; Plasencia, J.M.; Calvo-Temprano, D.; Sanchez, M.; Benegas, M.; et al. Clinical features and short-term outcomes of cancer patients with suspected and unsuspected pulmonary embolism: The EPIPHANY study. Eur. Respir. J. 2017, 49, 1600282. [Google Scholar] [CrossRef] [Green Version]
- Jiménez-Fonseca, P.; Carmona-Bayonas, A.; Font, C.; Plasencia-Martínez, J.; Calvo-Temprano, D.; Otero, R.; Beato, C.; Biosca, M.; Sánchez, M.; Benegas, M.; et al. The prognostic impact of additional intrathoracic findings in patients with cancer-related pulmonary embolism. Clin. Transl. Oncol. 2018, 20, 230–242. [Google Scholar] [CrossRef] [PubMed]
- Weeda, E.R.; Hakamiun, K.M.; Leschorn, H.X.; Tran, E. Comorbid cancer and use of thrombolysis in acute pulmonary embolism. J. Thromb. Thrombolysis 2019, 47, 324–327. [Google Scholar] [CrossRef] [PubMed]
- Kooiman, J.; Den Exter, P.L.; Cannegieter, S.C.; Le Cessie, S.; Del Toro, J.; Sahuquillo, J.C.; Pedrajas, J.M.; Huisman, M.V. Impact of chronic kidney disease on the risk of clinical outcomes in patients with cancer-associated venous thromboembolism during anticoagulant treatment. J. Thromb. Haemost. 2013, 11, 1968–1976. [Google Scholar] [CrossRef] [PubMed]
- Trujillo-Santos, J.; Schellong, S.; Falga, C.; Zorrilla, V.; Gallego, P.; Barrón, M.; Monreal, M.; RIETE investigators. Low-molecular-weight or Unfractionated Heparin in Venous Thromboembolism: The Influence of Renal Function. Am. J. Med. 2013, 126, 425–434. [Google Scholar] [CrossRef]
- Maestre, A.; Trujillo-Santos, J.; Visoná, A.; Lobo, J.L.; Grau, E.; Malý, R.; Duce, R.; Monreal, M. D-dimer levels and 90-day outcome in patients with acute pulmonary embolism with or without cancer. Thromb. Res. 2014, 133, 384–389. [Google Scholar] [CrossRef]
- İyikesici, F.; Bozkurt Babuş, S.; Köse, A.; Erdoğan, S.; Balcı, Y. Analysis of Clinical and Radiological Findings in Oncology Patients Undergoing Thoracic Tomography for Suspected Pulmonary Embolism. Cardiovasc. Toxicol. 2021, 21, 927–935. [Google Scholar] [CrossRef]
- Bikdeli, B.; Jimenez, D.; Hawkins, M.; Ortíz, S.; Prandoni, P.; Brenner, B.; Decousus, H.; Masoudi, F.A.; Trujillo-Santos, J.; Krumholz, H.M.; et al. Rationale, Design and Methodology of the Computerized Registry of Patients with Venous Thromboembolism (RIETE). Thromb. Haemost. 2018, 118, 214–224. [Google Scholar] [CrossRef]
- Delluc, A.; Tromeur, C.; Le Ven, F.; Gouillou, M.; Paleiron, N.; Bressollette, L.; Nonent, M.; Salaun, P.Y.; Lacut, K.; Leroyer, C.; et al. Current incidence of venous thromboembolism and comparison with 1998: A community-based study in Western France. Thromb. Haemost. 2016, 116, 967–974. [Google Scholar] [CrossRef]
- Khorana, A.A.; Kuderer, N.M.; Culakova, E.; Lyman, G.H.; Francis, C.W. Development and validation of a predictive model for chemotherapy-associated thrombosis. Blood 2008, 111, 4902–4907. [Google Scholar] [CrossRef]
- Ay, C.; Dunkler, D.; Marosi, C.; Chiriac, A.L.; Vormittag, R.; Simanek, R.; Quehenberger, P.; Zielinski, C.; Pabinger, I. Prediction of venous thromboembolism in cancer patients. Blood 2010, 116, 5377–5382. [Google Scholar] [CrossRef]
- Moik, F.; Ay, C.; Pabinger, I. Risk prediction for cancer-associated thrombosis in ambulatory patients with cancer: Past, present and future. Thromb. Res. 2020, 191, S3–S11. [Google Scholar] [CrossRef]
- Carmona-Bayonas, A.; Gómez, D.; de Castro, E.M.; Segura, P.P.; Langa, J.M.; Jimenez-Fonseca, P.; Cánovas, M.S.; Moran, L.O.; Escobar, I.G.; Blanco, A.B.; et al. A snapshot of cancer-associated thromboembolic disease in 2018–2019: First data from the TESEO prospective registry. Eur. J. Intern. Med. 2020, 78, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Mulder, F.I.; Horvàth-Puhó, E.; van Es, N.; Van Laarhoven, H.W.; Pedersen, L.; Moik, F.; Ay, C.; Büller, H.R.; Sørensen, H.T. Venous thromboembolism in cancer patients: A population-based cohort study. Blood 2021, 137, 1959–1969. [Google Scholar] [CrossRef] [PubMed]
- Carrier, M.; Lazo-Langner, A.; Shivakumar, S.; Tagalakis, V.; Zarychanski, R.; Solymoss, S.; Routhier, N.; Douketis, J.; Danovitch, K.; Lee, A.Y.; et al. Screening for Occult Cancer in Unprovoked Venous Thromboembolism. N. Engl. J. Med. 2015, 373, 697–704. [Google Scholar] [CrossRef]
- Robin, P.; Le Roux, P.-Y.; Planquette, B.; Accassat, S.; Roy, P.-M.; Couturaud, F.; Ghazzar, N.; Prevot-Bitot, N.; Couturier, O.; Delluc, A.; et al. Limited screening with versus without 18F-fluorodeoxyglucose PET/CT for occult malignancy in unprovoked venous thromboembolism: An open-label randomised controlled trial. Lancet Oncol. 2016, 17, 193–199. [Google Scholar] [CrossRef]
- van Es, N.; Le Gal, G.; Otten, H.M.; Robin, P.; Piccioli, A.; Lecumberri, R.; Jara-Palomares, L.; Religa, P.; Rieu, V.; Rondina, M.; et al. Screening for Occult Cancer in Patients with Unprovoked Venous Thromboembolism: A Systematic Review and Meta-analysis of Individual Patient Data. Ann. Intern. Med. 2017, 167, 410. [Google Scholar] [CrossRef]
- Delluc, A.; Antic, D.; Lecumberri, R.; Ay, C.; Meyer, G.; Carrier, M. Occult cancer screening in patients with venous thromboembolism: Guidance from the SSC of the ISTH. J. Thromb. Haemost. 2017, 15, 2076–2079. [Google Scholar] [CrossRef]
- Farge, D.; Trujillo-Santos, J.; Debourdeau, P.; Bura-Riviere, A.; Rodriguez-Beltrán, E.M.; Nieto, J.A.; Peris, M.L.; Zeltser, D.; Mazzolai, L.; Hij, A.; et al. Fatal Events in Cancer Patients Receiving Anticoagulant Therapy for Venous Thromboembolism. Medicine 2015, 94, e1235. [Google Scholar] [CrossRef]
- Gussoni, G.; Frasson, S.; La Regina, M.; Di Micco, P.; Monreal, M. Three-month mortality rate and clinical predictors in patients with venous thromboembolism and cancer. Findings from the RIETE registry. Thromb. Res. 2012, 131, 24–30. [Google Scholar] [CrossRef]
- Shalaby, K.; Kahn, A.; Silver, E.S.; Kim, M.J.; Balakumaran, K.; Kim, A.S. Outcomes of acute pulmonary embolism in hospitalized patients with cancer. BMC Pulm. Med. 2022, 22, 11. [Google Scholar] [CrossRef]
- Kabrhel, C.; Okechukwu, I.; Hariharan, P.; Takayesu, J.K.; MacMahon, P.; Haddad, F.; Chang, Y. Factors associated with clinical deterioration shortly after PE. Thorax 2014, 69, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Alotaibi, G.; Wu, C.; Senthilselvan, A.; McMurtry, M.S. Short- and long-term mortality after pulmonary embolism in patients with and without cancer. Vasc. Med. 2018, 23, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Gimbel, I.A.; Mulder, F.I.; Bosch, F.T.M.; Freund, J.E.; Guman, N.; van Es, N.; Kamphuisen, P.W.; Büller, H.R.; Middeldorp, S. Pulmonary embolism at autopsy in cancer patients. J. Thromb. Haemost. 2021, 19, 1228–1235. [Google Scholar] [CrossRef] [PubMed]
- Svendsen, E.; Karwinski, B. Prevalence of pulmonary embolism at necropsy in patients with cancer. J. Clin. Pathol. 1989, 42, 805–809. [Google Scholar] [CrossRef] [PubMed]
- Sakuma, M.; Fukui, S.; Nakamura, M.; Takahashi, T.; Kitamukai, O.; Yazu, T.; Yamada, N.; Ota, M.; Kobayashi, T.; Nakano, T. Cancer and Pulmonary Embolism Thrombotic Embolism, Tumor Embolism, and Tumor Invasion into a Large Vein: Thrombotic Embolism, Tumor Embolism, and Tumor Invasion into a Large Vein. Circ. J. 2006, 70, 744–749. [Google Scholar] [CrossRef]
- Ögren, M.; Bergqvist, D.; Wåhlander, K.; Eriksson, H.; Sternby, N. Trousseau’s syndrome—What is the evidence?: A population-based autopsy study. Thromb. Haemost. 2006, 95, 541–545. [Google Scholar]
- Valerio, L.; Turatti, G.; Klok, F.A.; Konstantinides, S.V.; Kucher, N.; Roncon, L.; Zuin, M.; Barco, S. Prevalence of pulmonary embolism in 127 945 autopsies performed in cancer patients in the United States between 2003 and 2019. J. Thromb. Haemost. 2021, 19, 1591–1593. [Google Scholar] [CrossRef]
- Tritschler, T.; Kraaijpoel, N.; Girard, P.; Büller, H.R.; Langlois, N.; Righini, M.; Schulman, S.; Segers, A.; Le Gal, G.; Subcommittee on Predictive and Diagnostic Variables in Thrombotic Disease. Definition of pulmonary embolism-related death and classification of the cause of death in venous thromboembolism studies: Communication from the SSC of the ISTH. J. Thromb. Haemost. 2020, 18, 1495–1500. [Google Scholar] [CrossRef]
- Lyman, G.H.; Carrier, M.; Ay, C.; Di Nisio, M.; Hicks, L.K.; Khorana, A.A.; Leavitt, A.D.; Lee, A.Y.Y.; Macbeth, F.; Morgan, R.L.; et al. American Society of Hematology 2021 guidelines for management of venous thromboembolism: Prevention and treatment in patients with cancer. Blood Adv. 2021, 5, 927–974. [Google Scholar] [CrossRef]
- Kearon, C.; Akl, E.A.; Ornelas, J.; Blaivas, A.; Jimenez, D.; Bounameaux, H.; Huisman, M.; King, C.S.; Morris, T.A.; Sood, N.; et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest 2016, 149, 315–352. [Google Scholar] [CrossRef]
- Louzada, M.L.; Carrier, M.; Lazo-Langner, A.; Dao, V.; Kovacs, M.J.; Ramsay, T.O.; Rodger, M.A.; Zhang, J.; Lee, A.Y.; Meyer, G.; et al. Development of a Clinical Prediction Rule for Risk Stratification of Recurrent Venous Thromboembolism in Patients with Cancer-Associated Venous Thromboembolism. Circulation 2012, 126, 448–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delluc, A.; Miranda, S.; Exter, P.D.; Louzada, M.; Alatri, A.; Ahn, S.; Monreal, M.; Khorana, A.; Huisman, M.V.; Wells, P.S.; et al. Accuracy of the Ottawa score in risk stratification of recurrent venous thromboembolism in patients with cancer-associated venous thromboembolism: A systematic review and meta-analysis. Haematologica 2020, 105, 1436–1442. [Google Scholar] [CrossRef] [PubMed]
- Girard, P.; Laporte, S.; Chapelle, C.; Falvo, N.; Falchero, L.; Cloarec, N.; Monnet, I.; Burnod, A.; Tomasini, P.; Boulon, C.; et al. Failure of the Ottawa Score to Predict the Risk of Recurrent Venous Thromboembolism in Cancer Patients: The Prospective PREDICARE Cohort Study. Thromb. Haemost. 2022, 122, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Hyers, T.M. Venous Thromboembolism. Am. J. Respir. Crit. Care Med. 1999, 159, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Weeda, E.R.; Caranfa, J.T.; Lyman, G.H.; Kuderer, N.M.; Nguyen, E.; Coleman, C.I.; Kohn, C.G. External validation of three risk stratification rules in patients presenting with pulmonary embolism and cancer. Support. Care Cancer 2019, 27, 921–925. [Google Scholar] [CrossRef]
- Wells, P.S.; Anderson, D.R.; Rodger, M.; Stiell, I.; Dreyer, J.F.; Barnes, D.; Forgie, M.; Kovacs, G.; Ward, J.; Kovacs, M.J. Excluding Pulmonary Embolism at the Bedside without Diagnostic Imaging: Management of Patients with Suspected Pulmonary Embolism Presenting to the Emergency Department by Using a Simple Clinical Model and d-dimer. Ann. Intern. Med. 2001, 135, 98–107. [Google Scholar] [CrossRef]
- Blondon, M.; Le Gal, G.; Meyer, G.; Righini, M.; Robert-Ebadi, H. Age-adjusted D-dimer cutoff for the diagnosis of pulmonary embolism: A cost-effectiveness analysis. J. Thromb. Haemost. 2020, 18, 865–875. [Google Scholar] [CrossRef]
- Schutgens, R.; Beckers, M.M.J.; Haas, F.J.L.M.; Biesma, U.H. The predictive value of D-dimer measurement for cancer in patients with deep vein thrombosis. Haematologica 2005, 90, 214–219. [Google Scholar]
- LE Gal, G.; De Lucia, S.; Roy, P.-M.; Meyer, G.; Aujesky, D.; Bounameaux, H.; Perrier, A.; Righini, M. Clinical usefulness of D-dimer testing in cancer patients with suspected pulmonary embolism. Thromb. Haemost. 2006, 95, 715–719. [Google Scholar] [CrossRef]
- Righini, M.; Van Es, J.; Den Exter, P.L.; Roy, P.M.; Verschuren, F.; Ghuysen, A.; Rutschmann, O.T.; Sanchez, O.; Jaffrelot, M.; Trinh-Duc, A.; et al. Age-Adjusted D-Dimer Cutoff Levels to Rule Out Pulmonary Embolism: The ADJUST-PE Study. JAMA 2014, 311, 1117. [Google Scholar] [CrossRef]
- Wilts, I.; Le Gal, G.; Exter, P.D.; Van Es, J.; Carrier, M.; Planquette, B.; Büller, H.; Righini, M.; Huisman, M.; Kamphuisen, P. Performance of the age-adjusted cut-off for D-dimer in patients with cancer and suspected pulmonary embolism. Thromb. Res. 2017, 152, 49–51. [Google Scholar] [CrossRef] [PubMed]
- van der Hulle, T.; Cheung, W.Y.; Kooij, S.; Beenen, L.F.; van Bemmel, T.; van Es, J.; Faber, L.M.; Hazelaar, G.M.; Heringhaus, C.; Hofstee, H.; et al. Faculty Opinions recommendation of Simplified diagnostic management of suspected pulmonary embolism (the YEARS study): A prospective, multicentre, cohort study. Lancet 2017, 390, 289–297. [Google Scholar] [CrossRef]
- Stals, M.A.M.; Klok, E.; Huisman, M.V. Diagnostic management of acute pulmonary embolism in special populations. Expert Rev. Respir. Med. 2020, 14, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Callejas, M.F.; Errázuriz, J.I.; Castillo, F.; Otárola, C.; Riquelme, C.; Ortega, C.; Huete, Á.; Bächler, P. Incidental venous thromboembolism detected by PET-CT in patients with cancer: Prevalence and impact on survival rate. Thromb. Res. 2014, 133, 750–755. [Google Scholar] [CrossRef]
- Kline, J.A.; Jiménez, D.; Courtney, D.M.; Ianus, J.; Cao, L.; Lensing, A.W.; Prins, M.H.; Wells, P.S. Comparison of Four Bleeding Risk Scores to Identify Rivaroxaban-treated Patients with Venous Thromboembolism at Low Risk for Major Bleeding. Acad. Emerg. Med. 2016, 23, 144–150. [Google Scholar] [CrossRef]
- Liebman, H.A.; O’Connell, C. Incidental venous thromboembolic events in cancer patients: What we know in 2016. Thromb. Res. 2016, 140, S18–S20. [Google Scholar] [CrossRef]
- Kraaijpoel, N.; Bleker, S.M.; Meyer, G.; Mahé, I.; Muñoz, A.; Bertoletti, L.; Bartels-Rutten, A.; Beyer-Westendorf, J.; Porreca, E.; Boulon, C.; et al. Treatment and Long-Term Clinical Outcomes of Incidental Pulmonary Embolism in Patients with Cancer: An International Prospective Cohort Study. J Clin Oncol. 2019, 37, 1713–1720. [Google Scholar] [CrossRef]
- Chang, H.; Kim, M.S.; Lee, S.Y.; Shin, S.H.; Park, H.Y.; Chang, S.A.; Park, T.K.; Kim, D.K.; Kim, E.K. Does anticoagulation needed for distally located incidental pulmonary thromboembolism in patients with active cancer? PLoS ONE. 2019, 14, e0222149. [Google Scholar] [CrossRef]
- Sun, J.-M.; Kim, T.S.; Lee, J.; Park, Y.H.; Ahn, J.S.; Kim, H.; Kwon, O.J.; Lee, K.S.; Park, K.; Ahn, M.-J. Unsuspected pulmonary emboli in lung cancer patients: The impact on survival and the significance of anticoagulation therapy. Lung Cancer 2010, 69, 330–336. [Google Scholar] [CrossRef]
- den Exter, P.L.; Hooijer, J.; Dekkers, O.M.; Huisman, M.V. Risk of recurrent venous thromboembolism and mortality in patients with cancer incidentally diagnosed with pulmonary embolism: A comparison with symptomatic patients. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29, 2405–2409. [Google Scholar] [CrossRef]
- Abdel-Razeq, H.N.; Mansour, A.H.; Ismael, Y.M. Incidental pulmonary embolism in cancer patients: Clinical characteristics and outcome—A comprehensive cancer center experience. Vasc. Health Risk Manag. 2011, 7, 153–158. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, C.; Razavi, P.; Ghalichi, M.; Boyle, S.; Vasan, S.; Mark, L.; Caton, A.; Duddalwar, V.; Boswell, W.; Grabow, K.; et al. Unsuspected pulmonary emboli adversely impact survival in patients with cancer undergoing routine staging multi-row detector computed tomography scanning. J. Thromb. Haemost. 2011, 9, 305–311. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, C.L.; Razavi, P.A.; Liebman, H.A. Symptoms Adversely Impact Survival Among Patients with Cancer and Unsuspected Pulmonary Embolism. J. Clin. Oncol. 2011, 29, 4208–4209. [Google Scholar] [CrossRef] [PubMed]
- Dentali, F.; Ageno, W.; Giorgi Pierfranceschi, M.; Imberti, D.; Malato, A.; Nitti, C.; Salvi, A.; Siragusa, S.; Squizzato, A.; Vitale, J.; et al. Prognostic relevance of an asymptomatic venous thromboembolism in patients with cancer. J. Thromb. Haemost. JTH 2011, 9, 1081–1083. [Google Scholar] [CrossRef]
- Sahut D’Izarn, M.; Caumont Prim, A.; Planquette, B.; Revel, M.P.; Avillach, P.; Chatellier, G.; Sanchez, O.; Meyer, G. Risk factors and clinical outcome of unsuspected pulmonary embolism in cancer patients: A case-control study: Unsuspected pulmonary embolism. J. Thromb. Haemost. 2012, 10, 2032–2038. [Google Scholar] [CrossRef]
- van der Hulle, T.; Den Exter, P.L.; Planquette, B.; Meyer, G.; Soler, S.; Monreal, M.; Jiménez, D.; Portillo, A.K.; O’Connell, C.; Liebman, H.A.; et al. Risk of recurrent venous thromboembolism and major hemorrhage in cancer-associated incidental pulmonary embolism among treated and untreated patients: A pooled analysis of 926 patients. J. Thromb. Haemost. 2016, 14, 105–113. [Google Scholar] [CrossRef]
- Peris, M.; Jiménez, D.; Maestre, A.; Font, C.; Tafur, A.J.; Mazzolai, L.; Xifre, B.; Skride, A.; Dentali, F.; Monreal, M. Outcome during and after anticoagulant therapy in cancer patients with incidentally found pulmonary embolism. Eur. Respir. J. 2016, 48, 1360–1368. [Google Scholar] [CrossRef]
- Myat Moe, M.M.; Redla, S. Incidental pulmonary embolism in oncology patients with current macroscopic malignancy: Incidence in different tumour type and impact of delayed treatment on survival outcome. Br. J. Radiol. 2018, 10, 20170806. [Google Scholar] [CrossRef]
- Bozas, G.; Jeffery, N.; Ramanujam-Venkatachala, D.; Avery, G.; Stephens, A.; Moss, H.; Palmer, J.; Elliott, M.; Maraveyas, A. Prognostic assessment for patients with cancer and incidental pulmonary embolism. Thromb. J. 2018, 16, 8. [Google Scholar] [CrossRef]
- Ahn, S.; Cooksley, T.; Banala, S.; Buffardi, L.; Rice, T.W. Validation of the EPIPHANY index for predicting risk of serious complications in cancer patients with incidental pulmonary embolism. Support. Care Cancer 2018, 26, 3601–3607. [Google Scholar] [CrossRef]
- Muñoz Martín, A.J.; Ruiz Zamorano, M.C.; Viñuela Benéitez, M.C.; Ortega Morán, L.; García Pérez, Á.; Martín Jiménez, M. Outpatient management of incidental pulmonary embolism in cancer patient. Clin. Transl. Oncol. 2020, 22, 612–615. [Google Scholar] [CrossRef] [PubMed]
- Qdaisat, A.; Kamal, M.; Al-Breiki, A.; Goswami, B.; Wu, C.C.; Zhou, S.; Rice, T.W.; Alagappan, K.; Yeung, S.C. Clinical characteristics, management, and outcome of incidental pulmonary embolism in cancer patients. Blood Adv. 2020, 4, 1606–1614. [Google Scholar] [CrossRef] [PubMed]
- Maraveyas, A.; Kraaijpoel, N.; Bozas, G.; Huang, C.; Mahé, I.; Bertoletti, L.; Bartels-Rutten, A.; Beyer-Westendorf, J.; Constans, J.; Iosub, D.; et al. The prognostic value of respiratory symptoms and performance status in ambulatory cancer patients and unsuspected pulmonary embolism; analysis of an international, prospective, observational cohort study. J. Thromb. Haemost. 2021, 19, 2791–2800. [Google Scholar] [CrossRef] [PubMed]
- Peris, M.; López-Nuñez, J.J.; Maestre, A.; Jimenez, D.; Muriel, A.; Bikdeli, B.; Weinberg, I.; Ay, C.; Mazzolai, L.; Lorenzo, A.; et al. Clinical characteristics and 3-month outcomes in cancer patients with incidental versus clinically suspected and confirmed pulmonary embolism. Eur. Respir. J. 2021, 58, 2002723. [Google Scholar] [CrossRef]
- Eyer, B.A.; Goodman, L.R.; Washington, L. Clinicians’ Response to Radiologists’ Reports of Isolated Subsegmental Pulmonary Embolism or Inconclusive Interpretation of Pulmonary Embolism Using MDCT. Am. J. Roentgenol. 2005, 184, 623–628. [Google Scholar] [CrossRef]
- Carrier, M.; Righini, M.; Wells, P.S.; Perrier, A.; Anderson, D.R.; Rodger, M.A.; Pleasance, S.; Le Gal, G. Subsegmental pulmonary embolism diagnosed by computed tomography: Incidence and clinical implications. A systematic review and meta-analysis of the management outcome studies: Subsegmental pulmonary embolism diagnosed by computed tomography. J. Thromb. Haemost. 2010, 8, 1716–1722. [Google Scholar] [CrossRef]
- Le Roux, P.Y.; Burbury, K.; Hofman, M.S.; Hicks, R.J. Short and long-term prognostic implications of a low embolic burden in oncology patients diagnosed with symptomatic pulmonary embolism. Ann. Hematol. 2016, 95, 651–652. [Google Scholar] [CrossRef]
- Key, N.S.; Khorana, A.A.; Kuderer, N.M.; Bohlke, K.; Lee, A.Y.; Arcelus, J.I.; Wong, S.L.; Balaban, E.P.; Flowers, C.R.; Francis, C.W.; et al. Venous Thromboembolism Prophylaxis and Treatment in Patients with Cancer: ASCO Clinical Practice Guideline Update. J. Clin. Oncol. 2020, 38, 496–520. [Google Scholar] [CrossRef]
- Witt, D.M.; Nieuwlaat, R.; Clark, N.P.; Ansell, J.; Holbrook, A.; Skov, J.; Shehab, N.; Mock, J.; Myers, T.; Dentali, F.; et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: Optimal management of anticoagulation therapy. Blood Adv. 2018, 2, 3257–3291. [Google Scholar] [CrossRef]
- Farge, D.; Frere, C.; Connors, J.M.; Ay, C.; Khorana, A.A.; Munoz, A.; Brenner, B.; Kakkar, A.; Rafii, H.; Solymoss, S.; et al. 2019 international clinical practice guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer. Lancet Oncol. 2019, 20, e566–e581. [Google Scholar] [CrossRef]
- Flinterman, L.E.; Van Der Meer, F.J.M.; Rosendaal, F.R.; Doggen, C.J.M. Current perspective of venous thrombosis in the upper extremity. J. Thromb. Haemost. 2008, 6, 1262–1266. [Google Scholar] [CrossRef] [PubMed]
- Decousus, H.; Bourmaud, A.; Fournel, P.; Bertoletti, L.; Labruyère, C.; Presles, E.; Merah, A.; Laporte, S.; Stefani, L.; Del Piano, F.; et al. Cancer-associated thrombosis in patients with implanted ports: A prospective multicenter French cohort study (ONCOCIP). Blood 2018, 132, 707–716. [Google Scholar] [CrossRef] [PubMed]
- Kreuziger, L.B.; Cote, L.; Verhamme, P.; Greenberg, S.; Caprini, J.; Muñoz, F.J.; Valle, R.; Bosch, M.M.; Monreal, M.; Decousus, H.; et al. A RIETE registry analysis of recurrent thromboembolism and hemorrhage in patients with catheter-related thrombosis. J. Vasc. Surg. Venous Lymphat Disord. 2015, 3, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, Y.; Morimoto, T.; Amano, H.; Takase, T.; Hiramori, S.; Kim, K.; Oi, M.; Akao, M.; Kobayashi, Y.; Toyofuku, M.; et al. Usefulness of Simplified Pulmonary Embolism Severity Index Score for Identification of Patients with Low-Risk Pulmonary Embolism and Active Cancer: From the COMMAND VTE Registry. Chest 2020, 157, 636–644. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.Y.; Levine, M.N.; Baker, R.I.; Bowden, C.; Kakkar, A.K.; Prins, M.; Rickles, F.R.; Julian, J.A.; Haley, S.; Kovacs, M.J.; et al. Low-Molecular-Weight Heparin versus a Coumarin for the Prevention of Recurrent Venous Thromboembolism in Patients with Cancer. N. Engl. J. Med. 2003, 349, 146–153. [Google Scholar] [CrossRef] [PubMed]
- van Es, N.; Di Nisio, M.; Bleker, S.M.; Segers, A.; Mercuri, M.F.; Schwocho, L.; Kakkar, A.; Weitz, J.I.; Beyer-Westendorf, J.; Boda, Z.; et al. Edoxaban for treatment of venous thromboembolism in patients with cancer: Rationale and design of the Hokusai VTE-cancer study. Thromb. Haemost. 2015, 114, 1268–1276. [Google Scholar] [PubMed]
- McBane, R.D.; Wysokinski, W.E.; Le-Rademacher, J.G.; Zemla, T.; Ashrani, A.; Tafur, A.; Perepu, U.; Anderson, D.; Gundabolu, K.; Kuzma, C.; et al. Apixaban and dalteparin in active malignancy-associated venous thromboembolism: The ADAM VTE trial. J. Thromb. Haemost. 2020, 18, 411–421. [Google Scholar] [CrossRef]
- Agnelli, G.; Becattini, C.; Meyer, G.; Muñoz, A.; Huisman, M.V.; Connors, J.M.; Cohen, A.; Bauersachs, R.; Brenner, B.; Torbicki, A.; et al. Apixaban for the Treatment of Venous Thromboembolism Associated with Cancer. N. Engl. J. Med. 2020, 382, 1599–1607. [Google Scholar] [CrossRef]
- Riess, H.; Sinn, M.; Kreher, S. CONKO-011: Evaluation der Patientenzufriedenheit bei der Behandlung akuter venöser Thromboembolien mit Rivaroxaban oder niedermolekularem Heparin bei Krebspatienten. DMW-Dtsch. Med. Wochenschr. 2015, 140, S22–S23. [Google Scholar] [CrossRef]
- Young, A.M.; Marshall, A.; Thirlwall, J.; Chapman, O.; Lokare, A.; Hill, C.; Hale, D.; Dunn, J.A.; Lyman, G.H.; Hutchinson, C.; et al. Comparison of an Oral Factor Xa Inhibitor with Low Molecular Weight Heparin in Patients with Cancer with Venous Thromboembolism: Results of a Randomized Trial (SELECT-D). J. Clin. Oncol. 2018, 36, 2017–2023. [Google Scholar] [CrossRef]
- Planquette, B.; Bertoletti, L.; Charles-Nelson, A.; Laporte, S.; Grange, C.; Mahé, I.; Pernod, G.; Elias, A.; Couturaud, F.; Falvo, N.; et al. Rivaroxaban vs Dalteparin in Cancer-Associated Thromboembolism. Chest 2022, 161, 781–790. [Google Scholar] [CrossRef] [PubMed]
- Jara-Palomares, L.; Jiménez, D.; Bikdeli, B.; Muriel, A.; Rali, P.; Yamashita, Y.; Morimoto, T.; Kimura, T.; Le Mao, R.; Riera-Mestre, A.; et al. Derivation and validation of a clinical prediction rule for thrombolysis-associated major bleeding in patients with acute pulmonary embolism: The BACS score. Eur. Respir. J. 2020, 56, 2002336. [Google Scholar] [CrossRef] [PubMed]
- Iskandar, J.-P.; Hariri, E.; Kanaan, C.; Kassis, N.; Kamran, H.; Sese, D.; Wright, C.; Marinescu, M.; Cameron, S.J. The safety and efficacy of systemic versus catheter-based therapies: Application of a prognostic model by a pulmonary embolism response team. J. Thromb. Thrombolysis 2022, 53, 616–625. [Google Scholar] [CrossRef] [PubMed]
- Mismetti, P.; Laporte, S.; Pellerin, O.; Ennezat, P.V.; Couturaud, F.; Elias, A.; Falvo, N.; Meneveau, N.; Quere, I.; Roy, P.M.; et al. Effect of a Retrievable Inferior Vena Cava Filter Plus Anticoagulation vs Anticoagulation Alone on Risk of Recurrent Pulmonary Embolism: A Randomized Clinical Trial. JAMA 2015, 313, 1627. [Google Scholar] [CrossRef]
- Olin, J.W.; Young, J.R.; Graor, R.A.; Ruschhaupt, W.F.; Beven, E.G.; Bay, J.W. Treatment of deep vein thrombosis and pulmonary emboli in patients with primary and metastatic brain tumors. Anticoagulants or inferior vena cava filter? Arch. Intern. Med. 1987, 147, 2177–2179. [Google Scholar] [CrossRef]
- Cohen, J.R.; Tenenbaum, N.; Citron, M. Greenfield filter as primary therapy for deep venous thrombosis and/or pulmonary embolism in patients with cancer. Surgery 1991, 109, 12–15. [Google Scholar]
- Cohen, J.R.; Grella, L.; Citron, M. Greenfield filter instead of heparin as primary treatment for deep venous thrombosis or pulmonary embolism in patients with cancer. Cancer. 1992, 70, 1993–1996. [Google Scholar] [CrossRef]
- Hubbard, K.P.; Roehm, J.O.; Abbruzzese, J.L. The Bird’s Nest Filter. An alternative to long-term oral anticoagulation in patients with advanced malignancies. Am. J. Clin. Oncol. 1994, 17, 115–117. [Google Scholar] [CrossRef]
- Schwarz, R.E.; Marrero, A.M.; Conlon, K.C.; Burt, M. Inferior vena cava filters in cancer patients: Indications and outcome. J. Clin. Oncol. 1996, 14, 652–657. [Google Scholar] [CrossRef]
- Greenfield, L. Clinical results of Greenfield filter use in patients with cancer. Cardiovasc. Surg. 1997, 5, 145–149. [Google Scholar] [CrossRef]
- Barginear, M.F.; Gralla, R.J.; Bradley, T.P.; Ali, S.S.; Shapira, I.; Greben, C.; Nier-Shoulson, N.; Akerman, M.; Lesser, M.; Budman, D.R. Investigating the benefit of adding a vena cava filter to anticoagulation with fondaparinux sodium in patients with cancer and venous thromboembolism in a prospective randomized clinical trial. Support. Care Cancer 2012, 20, 2865–2872. [Google Scholar] [CrossRef] [PubMed]
- Brunson, A.; Ho, G.; White, R.; Wun, T. Inferior vena cava filters in patients with cancer and venous thromboembolism (VTE): Patterns of use and outcomes. Thromb. Res. 2016, 140, S132–S141. [Google Scholar] [CrossRef]
- Stein, P.D.; Matta, F.; Lawrence, F.R.; Hughes, M.J. Inferior Vena Cava Filters in Patients with Acute Pulmonary Embolism and Cancer. Am. J. Med. 2018, 131, 442.e9. [Google Scholar] [CrossRef] [PubMed]
- Balabhadra, S.; Kuban, J.D.; Lee, S.; Yevich, S.; Metwalli, Z.; McCarthy, C.J.; Huang, S.Y.; Tam, A.; Gupta, S.; Sheth, S.A.; et al. Association of Inferior Vena Cava Filter Placement with Rates of Pulmonary Embolism in Patients with Cancer and Acute Lower Extremity Deep Venous Thrombosis. JAMA Netw. Open 2020, 3, e2011079. [Google Scholar] [CrossRef] [PubMed]
- Edupuganti, S.; Li, M.; Wu, Z.; Basu, T.; Barnes, G.D.; Carrier, M.; Sood, S.L.; Griggs, J.J.; Schaefer, J.K. Factors Associated with Inferior Vena Cava Filter Placement and Retrieval for Patients with Cancer-Associated Thrombosis. Am. J. Med. 2022, 135, 478–487. [Google Scholar] [CrossRef]
- Kucher, N.; Boekstegers, P.; Müller, O.J.; Kupatt, C.; Beyer-Westendorf, J.; Heitzer, T.; Tebbe, U.; Horstkotte, J.; Müller, R.; Blessing, E.; et al. Randomized, Controlled Trial of Ultrasound-Assisted Catheter-Directed Thrombolysis for Acute Intermediate-Risk Pulmonary Embolism. Circulation 2014, 129, 479–486. [Google Scholar] [CrossRef]
- Piazza, G.; Hohlfelder, B.; Jaff, M.R.; Ouriel, K.; Engelhardt, T.C.; Sterling, K.M.; Jones, N.J.; Gurley, J.C.; Bhatheja, R.; Kennedy, R.J.; et al. A Prospective, Single-Arm, Multicenter Trial of Ultrasound-Facilitated, Catheter-Directed, Low-Dose Fibrinolysis for Acute Massive and Submassive Pulmonary Embolism. JACC Cardiovasc. Interv. 2015, 8, 1382–1392. [Google Scholar] [CrossRef]
- Kuo, W.T.; Banerjee, A.; Kim, P.S.; DeMarco, F.J., Jr.; Levy, J.R.; Facchini, F.R.; Unver, K.; Bertini, M.J.; Sista, A.; Hall, M.J.; et al. Pulmonary Embolism Response to Fragmentation, Embolectomy, and Catheter Thrombolysis (PERFECT)Initial Results from a Prospective Multicenter Registry. Chest 2015, 148, 667–673. [Google Scholar] [CrossRef]
- Weitz, J.I.; Prandoni, P.; Verhamme, P. Anticoagulation for Patients with Venous Thromboembolism: When is Extended Treatment Required? TH Open. 2020, 4, e446–56. [Google Scholar] [CrossRef]
- Ageno, W.; Vedovati, M.C.; Cohen, A.; Huisman, M.; Bauersachs, R.; Gussoni, G.; Becattini, C.; Agnelli, G. Bleeding with Apixaban and Dalteparin in Patients with Cancer-Associated Venous Thromboembolism: Results from the Caravaggio Study. Thromb. Haemost. 2021, 121, 616–624. [Google Scholar] [CrossRef]
- Poénou, G.; Tolédano, E.; Helfer, H.; Plaisance, L.; Happe, F.; Versini, E.; Diab, N.; Djennaoui, S.; Mahé, I. In Search of the Appropriate Anticoagulant-Associated Bleeding Risk Assessment Model for Cancer-Associated Thrombosis Patients. Cancers 2022, 14, 1937. [Google Scholar] [CrossRef] [PubMed]
- de Winter, M.A.; Dorresteijn, J.A.N.; Ageno, W.; Ay, C.; Beyer-Westendorf, J.; Coppens, M.; Erik, K.; Fares, M.; Nicoletta, R.; Thomas, V.; et al. Estimating Bleeding Risk in Patients with Cancer-Associated Thrombosis: Evaluation of Existing Risk Scores and Development of a New Risk Score. Thromb Haemost. 2021, 122, 818–829. [Google Scholar] [CrossRef] [PubMed]
- Poenou, G.; Dimitru, T.D.; Lafaie, L.; Mismetti, V.; Heestermans, M.; Bertoletti, L. Factor XI Inhibition for the Prevention of Venous Thromboembolism: An Update on Current Evidence and Future perspectives. Vasc. Health Risk Manag. 2022, 18, 359–373. [Google Scholar] [CrossRef] [PubMed]
- Mahé, I.; Agnelli, G.; Ay, C.; Bamias, A.; Becattini, C.; Carrier, M.; Chapelle, C.; Cohen, A.T.; Girard, P.; Huisman, M.V.; et al. Extended Anticoagulant Treatment with Full- or Reduced-Dose Apixaban in Patients with Cancer-Associated Venous Thromboembolism: Rationale and Design of the API-CAT Study. Thromb. Haemost. 2022, 122, 646–656. [Google Scholar] [CrossRef] [PubMed]
- Verhamme, P.; Yi, B.A.; Segers, A.; Salter, J.; Bloomfield, D.; Büller, H.R.; Raskob, G.E.; Weitz, J.I. Abelacimab for Prevention of Venous Thromboembolism. N. Engl. J. Med. 2021, 385, 609–617. [Google Scholar] [CrossRef]
- Klok, F.A.; Ageno, W.; Ay, C.; Bäck, M.; Barco, S.; Bertoletti, L.; Becattini, C.; Carlsen, J.; Delcroix, M.; van Es, N.; et al. Optimal follow-up after acute pulmonary embolism: A position paper of the European Society of Cardiology Working Group on Pulmonary Circulation and Right Ventricular Function, in collaboration with the European Society of Cardiology Working Group on Atherosclerosis and Vascular Biology, endorsed by the European Respiratory Society. Eur. Heart J. 2022, 43, 183–189. [Google Scholar] [CrossRef]
- Catella-Chatron, J.; Merah, A.; De Magalhaes, E.; Moulin, N.; Accassat, S.; Duvillard, C.; Mismetti, P.; Bertoletti, L. Chronic thromboembolic pulmonary hypertension suspicion after pulmonary embolism in cancer patients. Respir. Med. Res. 2019, 76, 34–37. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Authors | Number of Cancer Patients | Number of PE-Related Deaths, % | |
|---|---|---|---|
| Svendsen et al. [34] 1989 (Europe) | 6197 | 648 | 10.5% |
| Sakuma et al. [35] 2006 (Japan) | 65,181 | 1514 | 2.3% |
| Ögren et al. [36] 2006 (Europe) | 23,796 | 2369 5448 * | 10.0% 28.9% * |
| Gimbel et al. [33] 2021 (Europe) | 9571 | 1191 | 12.4% |
| Valerio et al. [37] 2021 (USA) | 127,945 | Category A ISTH 209 Category B ISTH 6571 | 0.2% 5.1% |
| Authors | N | Follow-Up (Month) | Death | Recurrent VTE | Bleeding | Sequel | Therapeutic Anticoagulation |
|---|---|---|---|---|---|---|---|
| Sun et al. [59] 2010 | 113 * | 9.3 | 50% | / | / | / | 45% |
| Den Exter et al. [60] 2011 | 51 | 3 | 27.5% | / | 3.9% | / | 100% |
| 6 | 35.3% | / | 5.9% | / | |||
| 9 | 43.1% | / | 5.9% | / | |||
| 12 | 43.1% | / | 5.9% | / | |||
| Abdel-Razeq et al. [61] 2011 | 34 | 1 | 26.5% | 5.9% | / | 5.9% | 85% |
| O’Connell et al. [62] 2011 | 96 | 2 | 16.7% | / | / | / | 84% |
| 6 | 33.3% | / | / | / | |||
| 12 | 62.5% | / | / | / | |||
| O’Connell et al. [63] 2011 | 21 | 12 | 47.6% | / | / | / | / |
| 24 | 57.1% | / | / | / | / | ||
| 36 | 66.7% | / | / | / | / | ||
| 48 | 76.8% | / | / | / | / | ||
| 60 | 100 | / | / | / | / | ||
| Dentali et al. [64] 2011 | 60 | 6 | 45% | / | / | / | 93% |
| Sahut D’Izarn et al. [65] 2012 | 66 | 6 | 17% | 6% | 4% | / | 100% |
| van Der Hulle et al. [66] 2016 | 926 | 6 | 37% | 5.8% | 4.7% | / | 79% |
| Peris et al. [67] 2016 | 715 | 12 | 20.1% | 28% | 6.9% | / | 98% |
| Myat Moe et al. [68] 2018 | 26 | 2 | 11.5% | / | / | / | 88.5% |
| 7 | 50% | / | / | / | |||
| Bozas et al. [69] 2018 | 234 | 1 | 3.4% | / | / | / | / |
| 3 | 15% | / | / | / | |||
| 6 | 31% | 2.6% | 2.1% | / | |||
| Ahn et al. [70] 2018 | 258 | 1 | 7.8% | <1% | 1.9 % | / | 96.1% |
| Chang et al. [58] 2019 | 474 | 5.6 | 50% | / | / | / | 52.3% |
| Kraaijpoel et al. [57] 2019 | 695 | 12 | 41% | 5.9% | 5.6% | / | 96.2% |
| Muñoz Martín et al. [71] 2020 | 25 | 1 3 | 0% | / 4% | / 4% | 100% | |
| Qdaisat et al. [72] 2021 | 904 | 0.25 | 1.8% 9.9% 22.1% | / | / | / | 92.5% |
| 1 | / | / | / | ||||
| 3 | / | / | / | ||||
| Maraveyas et al. [73] 2021 | 695 | 12 | 41% | 5.9% | 5.7% | 97% | |
| Peris et al. [74] 2021 | 946 | 3 | 11% | 1.6% | 3.2% | / | >95% |
| Study Design | Population of Non-Prophylactic IVCF | N | Recurrent VTE | All-Cause Mortality | |
|---|---|---|---|---|---|
| Olin 1987 [95] | Comparative nonrandomized Monocentric study | Brain cancer patients at high risk of bleeding | 24 | 4% in the IVCF group | 28% in each group |
| Cohen 1991 [96] | Comparative nonrandomized Monocentric study | Cancer patients | 18 | 0% in the IVCF group | / |
| Cohen 1992 [97] | Cohort study | Cancer patients | 41 | 2.4% | 56% |
| Hubbard 1994 [98] | Cohort study | advanced malignancies patients | 31 | 19.4% | / |
| Schwarz 1996 [99] | Cohort study | Cancer patients | 182 | 6.6% | 0% |
| Greenfield 1997 [100] | Registry study | Cancer patient followed for their risk of recurrent cancer | 166 | 36% recurrent VTE of the 86 patients presenting a recurrent cancer | 69.7% of the 166 IVCF |
| Barginear 2012 [101] | Randomized control study | Cancer patients | 32 | 3.1% | 0% |
| Mismetti 2015 [94] | Randomized control study | Hospitalized patients with PE and DVT | 33 | 3% | / |
| Brunson 2016 [102] | Cohort study | Hospitalized cancer patients | 2747 | Risk of VTE HR = 0.81, 95% CI (0.6–1.08) | Risk of short-term mortality HR = 1.12, 95% CI (0.99–1.26)). |
| Stein 2018 [103] | A population-based cohort study using administrative data | Hospitalized patients with PE | 6589 | / | 8.1% |
| Balabhadra 2020 [104] | A population-based cohort study using administrative data | cancer patients with a diagnosed VTE | 33,740 | HR = 0.69; 95% CI, 0.64–0.75; p < 0.001 | / |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poenou, G.; Dumitru Dumitru, T.; Lafaie, L.; Mismetti, V.; Ayoub, E.; Duvillard, C.; Accassat, S.; Mismetti, P.; Heestermans, M.; Bertoletti, L. Pulmonary Embolism in the Cancer Associated Thrombosis Landscape. J. Clin. Med. 2022, 11, 5650. https://doi.org/10.3390/jcm11195650
Poenou G, Dumitru Dumitru T, Lafaie L, Mismetti V, Ayoub E, Duvillard C, Accassat S, Mismetti P, Heestermans M, Bertoletti L. Pulmonary Embolism in the Cancer Associated Thrombosis Landscape. Journal of Clinical Medicine. 2022; 11(19):5650. https://doi.org/10.3390/jcm11195650
Chicago/Turabian StylePoenou, Géraldine, Teona Dumitru Dumitru, Ludovic Lafaie, Valentine Mismetti, Elie Ayoub, Cécile Duvillard, Sandrine Accassat, Patrick Mismetti, Marco Heestermans, and Laurent Bertoletti. 2022. "Pulmonary Embolism in the Cancer Associated Thrombosis Landscape" Journal of Clinical Medicine 11, no. 19: 5650. https://doi.org/10.3390/jcm11195650