
Brain-Derived Neurotrophic Factor Expression in Patients with Acute Pulmonary Embolism Compared to the General Population: Diagnostic and Prognostic Implications

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Statistical Analysis
3. Results
3.1. General Charactersistics
3.2. Biomarkers and BDNF Profile
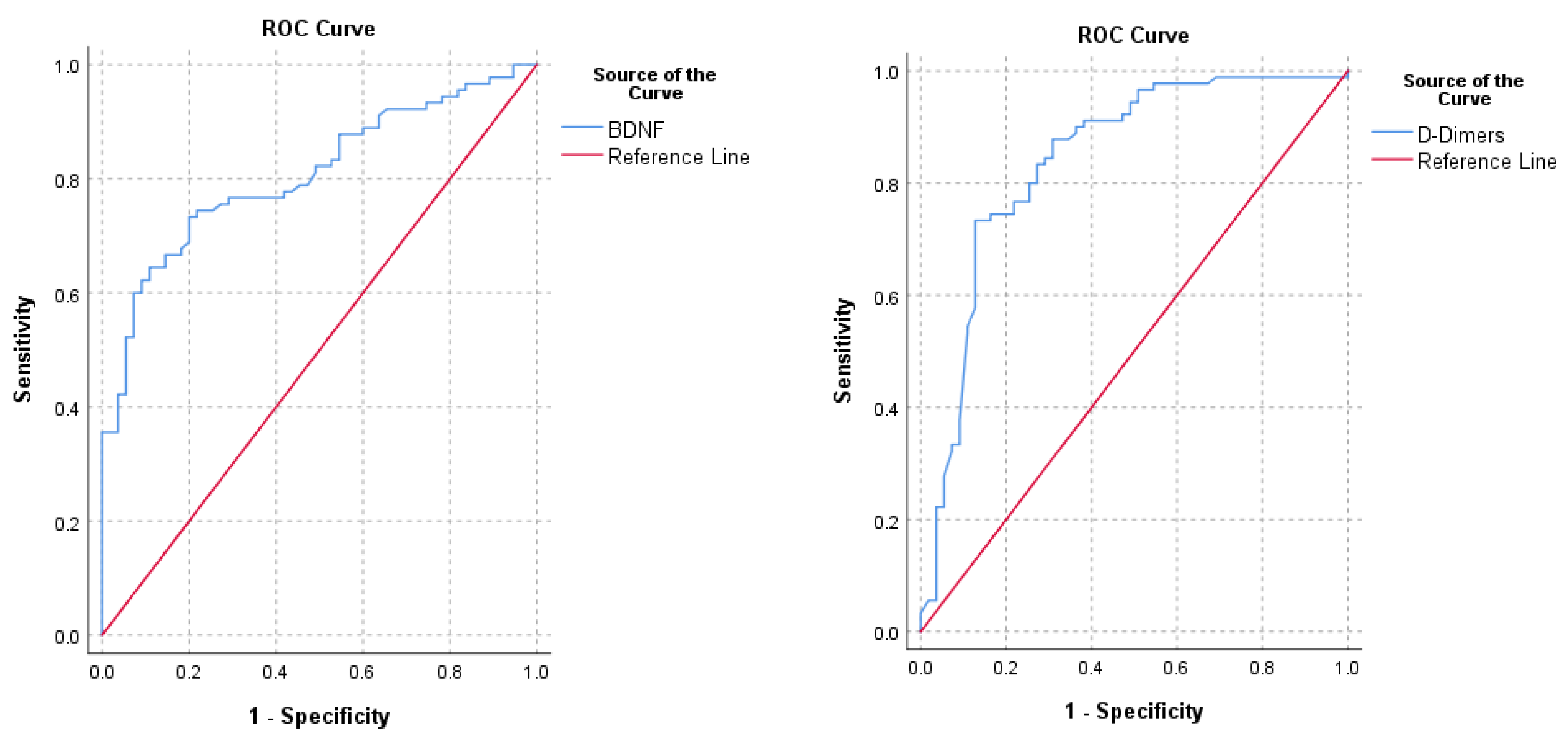
3.3. BDNF for Diagnosis of PE
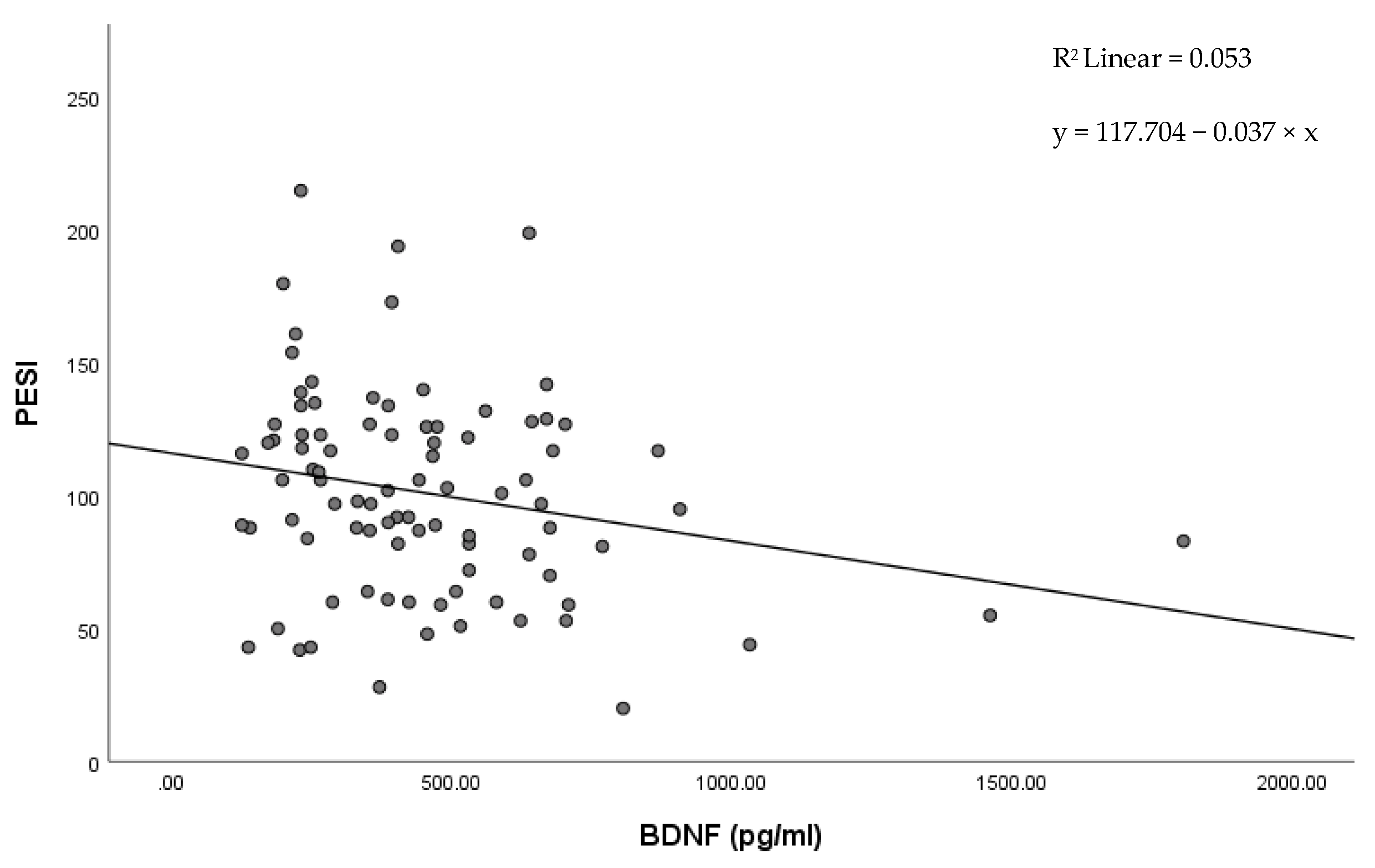
3.4. BDNF for Risk Stratification of PE
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wendelboe, A.M.; Raskob, G.E. Global burden of thrombosis: Epidemiologic aspects. Circ. Res. 2016, 118, 1340–1347. [Google Scholar] [CrossRef] [PubMed]
- Bĕlohlávek, J.; Dytrych, V.; Linhart, A. Pulmonary embolism, part I: Epidemiology, risk factors and risk stratification, pathophysiology, clinical presentation, diagnosis and nonthrombotic pulmonary embolism. Exp. Clin. Cardiol. 2013, 18, 129–138. [Google Scholar] [PubMed]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.-J.; Harjola, V.-P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D.; et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Heart J. 2020, 41, 543–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, P.D.; Fowler, S.E.; Goodman, L.R.; Gottschalk, A.; Hales, C.A.; Hull, R.D.; Leeper, K.V.; Popovich, J.; Quinn, D.A.; Sos, T.A.; et al. Multidetector computed tomography for acute pulmonary embolism. N. Engl. J. Med. 2006, 354, 2317–2327. [Google Scholar] [CrossRef] [Green Version]
- Kearon, C.; de Wit, K.; Parpia, S.; Schulman, S.; Afilalo, M.; Hirsch, A.; Spencer, F.A.; Sharma, S.; D’Aragon, F.; Deshaies, J.-F.; et al. Diagnosis of Pulmonary Embolism with d-Dimer Adjusted to Clinical Probability. N. Engl. J. Med. 2019, 381, 2125–2134. [Google Scholar] [CrossRef]
- Youssf, A.R.I.; Ismail, M.F.M.; ElGhamry, R.; Reyad, M.R. Diagnostic accuracy of D-dimer assay in suspected pulmonary embolism patients. Egypt. J. Chest Dis. Tuberc. 2014, 63, 411–417. [Google Scholar] [CrossRef] [Green Version]
- Bellesini, M.; Robert-Ebadi, H.; Combescure, C.; Dedionigi, C.; Le Gal, G.; Righini, M. D-dimer to rule out venous thromboembolism during pregnancy: A systematic review and meta-analysis. J. Thromb. Haemost. 2021, 19, 2454–2467. [Google Scholar] [CrossRef]
- Caliskan, T.; Turkoglu, O.; Canoglu, K.; Ayten, O.; Saylan, B.; Okutan, O.; Kartaloglu, Z. The Comparison Between Non-High Risk Patients with and Without Cancer Diagnosed with Pulmonary Embolism. Medeni. Med. J. 2021, 36, 30–35. [Google Scholar] [CrossRef]
- Kermani, P.; Hempstead, B. BDNF actions in the cardiovascular system: Roles in development, adulthood and response to injury. Front. Physiol. 2019, 10, 455. [Google Scholar] [CrossRef]
- Feng, N.; Huke, S.; Zhu, G.; Tocchetti, C.G.; Shi, S.; Aiba, T.; Kaludercic, N.; Hoover, D.B.; Beck, S.E.; Mankowski, J.L.; et al. Constitutive BDNF/TrkB signaling is required for normal cardiac contraction and relaxation. Proc. Natl. Acad. Sci. USA 2015, 112, 1880–1885. [Google Scholar] [CrossRef] [Green Version]
- Helan, M.; Aravamudan, B.; Hartman, W.R.; Thompson, M.A.; Johnson, B.D.; Pabelick, C.M.; Prakash, Y.S. BDNF secretion by human pulmonary artery endothelial cells in response to hypoxia. J. Mol. Cell. Cardiol. 2014, 68, 89–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hang, P.-Z.; Zhu, H.; Li, P.-F.; Liu, J.; Ge, F.-Q.; Zhao, J.; Du, Z.-M. The emerging role of bdnf/trkb signaling in cardiovascular diseases. Life 2021, 11, 70. [Google Scholar] [CrossRef] [PubMed]
- Di Nisio, M.; Squizzato, A.; Rutjes, A.W.S.; Büller, H.R.; Zwinderman, A.H.; Bossuyt, P.M.M. Diagnostic accuracy of D-dimer test for exclusion of venous thromboembolism: A systematic review. J. Thromb. Haemost. 2007, 5, 296–304. [Google Scholar] [CrossRef]
- Wang, Z.; Wang, S.; Liu, Y.; Gao, S.; Yu, Y.; Hu, Z. Serum Levels of BDNF in Patients with Adenoma and Colorectal Cancer. Dis. Markers 2021, 2021, 8867368. [Google Scholar] [CrossRef] [PubMed]
- Christian, L.M.; Mitchell, A.M.; Gillespie, S.L.; Palettas, M. Serum brain-derived neurotrophic factor (BDNF) across pregnancy and postpartum: Associations with race, depressive symptoms, and low birth weight. Psychoneuroendocrinology 2016, 74, 69–76. [Google Scholar] [CrossRef] [Green Version]
- Usul, E.; Ozkan, S.; Höke, M.H.; Kaya, A.E.; Ucar, F.; Cimen, T. Relationship between right ventricular dilatation and blood copeptin levels in patients with acute pulmonary embolism. Clin. Respir. J. 2020, 14, 965–972. [Google Scholar] [CrossRef]
- Ozmen, C.; Deveci, O.S.; Karaaslan, M.B.; Baydar, O.; Akray, A.; Deniz, A.; Cagliyan, C.E.; Hanta, I.; Usal, A. Predictive value of plasma copeptin level for diagnosis and mortality of pulmonary embolism. Rev. Assoc. Med. Bras. 2020, 66, 1645–1650. [Google Scholar] [CrossRef]
- Becattini, C.; Vedovati, M.C.; Agnelli, G. Prognostic value of troponins in acute pulmonary embolism: A meta-analysis. Circulation 2007, 116, 427–433. [Google Scholar] [CrossRef] [Green Version]
- Klok, F.A.; Mos, I.C.M.; Huisman, M.V. Brain-type natriuretic peptide levels in the prediction of adverse outcome in patients with pulmonary embolism: A systematic review and meta-analysis. Am. J. Respir. Crit. Care Med. 2008, 178, 425–430. [Google Scholar] [CrossRef]
- Petris, A.; Tatu-Chitoiu, G.; Coman, I.; Tint, D.; Ra, C.; Chioncel, V.; Darabantiu, D.; Cimpoesu, D.; Antohi, L.; Sorodoc, L.; et al. Biomarkers in emergency cardiology: Cardio-pulmonary resuscitation, acute coronary syndromes, pulmonary thromboembolism, acute aortic syndrome and acute heart failure. Rom. J. Cardiol. 2017, 27, 333–348. [Google Scholar]
- Pruszczyk, P.; Goliszek, S.; Lichodziejewska, B.; Kostrubiec, M.; Ciurzyński, M.; Kurnicka, K.; Dzikowska-Diduch, O.; Palczewski, P.; Wyzgal, A. Prognostic value of echocardiography in normotensive patients with acute pulmonary embolism. JACC Cardiovasc. Imaging 2014, 7, 553–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coutance, G.; Cauderlier, E.; Ehtisham, J.; Hamon, M.; Hamon, M. The prognostic value of markers of right ventricular dysfunction in pulmonary embolism: A meta-analysis. Crit. Care 2011, 15, R103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Araz, O.; Yilmazel Ucar, E.; Yalcin, A.; Kelercioglu, N.; Meral, M.; Gorguner, A.M.; Akgun, M. Predictive value of serum Hs-CRP levels for outcomes of pulmonary embolism. Clin. Respir. J. 2016, 10, 163–167. [Google Scholar] [CrossRef]
- Branchford, B.R.; Carpenter, S.L. The role of inflammation in venous thromboembolism. Front. Pediatr. 2018, 6, 142. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.-Y.; Ben, S.-Q.; Chen, H.-L.; Ni, S.-S. The prognostic value of pulmonary embolism severity index in acute pulmonary embolism: A meta-analysis. Respir. Res. 2012, 13, 111. [Google Scholar] [CrossRef] [Green Version]
- Cordeanu, M.; Gaertner, S.; Faller, A.; Mirea, C.; Le Ray, I.; Stephan, D. Prognostic value of the simplified PESI score in comparison with the 2014 ESC risk model in pulmonary embolism. Int. J. Cardiol. 2016, 220, 623–624. [Google Scholar] [CrossRef]
- Aujesky, D.; Roy, P.-M.; Verschuren, F.; Righini, M.; Osterwalder, J.; Egloff, M.; Renaud, B.; Verhamme, P.; Stone, R.A.; Legall, C.; et al. Outpatient versus inpatient treatment for patients with acute pulmonary embolism: An international, open-label, randomised, non-inferiority trial. Lancet 2011, 378, 41–48. [Google Scholar] [CrossRef]
- Meyer, G.; Vicaut, E.; Danays, T.; Agnelli, G.; Becattini, C.; Beyer-Westendorf, J.; Bluhmki, E.; Bouvaist, H.; Brenner, B.; Couturaud, F.; et al. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N. Engl. J. Med. 2014, 370, 1402–1411. [Google Scholar] [CrossRef]
- Pius-Sadowska, E.; Machaliński, B. BDNF—A key player in cardiovascular system. J. Mol. Cell. Cardiol. 2017, 110, 54–60. [Google Scholar] [CrossRef]
- Wu, H.; Cao, G.; Wang, Y.; Tian, H.; Du, R. Increased Serum CA125 and Brain-Derived Neurotrophic Factor (BDNF) Levels on Acute Myocardial Infarction: A Predictor for Acute Heart Failure. Med. Sci. Monit. 2019, 25, 913–919. [Google Scholar] [CrossRef]
- Matsumoto, J.; Takada, S.; Furihata, T.; Nambu, H.; Kakutani, N.; Maekawa, S.; Mizushima, W.; Nakano, I.; Fukushima, A.; Yokota, T.; et al. Brain-Derived Neurotrophic Factor Improves Impaired Fatty Acid Oxidation Via the Activation of Adenosine Monophosphate-Activated Protein Kinase-ɑ-Proliferator-Activated Receptor-r Coactivator-1ɑ Signaling in Skeletal Muscle of Mice With Heart Failure. Circ. Heart Fail. 2021, 14, e005890. [Google Scholar] [CrossRef] [PubMed]
- Shibata, A.; Hanatani, A.; Izumi, Y.; Kitada, R.; Iwata, S.; Yoshiyama, M. Serum brain-derived neurotrophic factor level and exercise tolerance complement each other in predicting the prognosis of patients with heart failure. Heart Vessels 2018, 33, 1325–1333. [Google Scholar] [CrossRef] [PubMed]
- Takashio, S.; Sugiyama, S.; Yamamuro, M.; Takahama, H.; Hayashi, T.; Sugano, Y.; Izumiya, Y.; Hokimoto, S.; Minamino, N.; Yasuda, S.; et al. Significance of low plasma levels of brain-derived neurotrophic factor in patients with heart failure. Am. J. Cardiol. 2015, 116, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Kadowaki, S.; Shishido, T.; Honda, Y.; Narumi, T.; Otaki, Y.; Kinoshita, D.; Nishiyama, S.; Takahashi, H.; Arimoto, T.; Miyamoto, T.; et al. Additive clinical value of serum brain-derived neurotrophic factor for prediction of chronic heart failure outcome. Heart Vessels 2016, 31, 535–544. [Google Scholar] [CrossRef] [PubMed]
- Bahls, M.; Könemann, S.; Markus, M.R.P.; Wenzel, K.; Friedrich, N.; Nauck, M.; Völzke, H.; Steveling, A.; Janowitz, D.; Grabe, H.-J.; et al. Brain-derived neurotrophic factor is related with adverse cardiac remodeling and high NTproBNP. Sci. Rep. 2019, 9, 15421. [Google Scholar] [CrossRef] [Green Version]
- Kwapiszewska, G.; Chwalek, K.; Marsh, L.M.; Wygrecka, M.; Wilhelm, J.; Best, J.; Egemnazarov, B.; Weisel, F.C.; Osswald, S.L.; Schermuly, R.T.; et al. BDNF/TrkB signaling augments smooth muscle cell proliferation in pulmonary hypertension. Am. J. Pathol. 2012, 181, 2018–2029. [Google Scholar] [CrossRef]
- Autry, A.E.; Monteggia, L.M. Brain-derived neurotrophic factor and neuropsychiatric disorders. Pharmacol. Rev. 2012, 64, 238–258. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.-P.; Li, X.-M.; Chen, H.-W.; Cui, J.-Y.; Niu, L.-L.; He, Y.-B.; Tian, X.-L. Depression, anxiety and influencing factors in patients with acute pulmonary embolism. Chin. Med. J. 2011, 124, 2438–2442. [Google Scholar]
- Whooley, M.A.; Wong, J.M. Depression and cardiovascular disorders. Annu. Rev. Clin. Psychol. 2013, 9, 327–354. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.-M.; Stewart, R.; Kim, J.-W.; Kang, H.-J.; Lee, J.-Y.; Kim, S.-Y.; Kim, S.-W.; Shin, I.-S.; Hong, Y.J.; Ahn, Y.; et al. Modifying effects of depression on the association between BDNF methylation and prognosis of acute coronary syndrome. Brain Behav. Immun. 2019, 81, 422–429. [Google Scholar] [CrossRef]
- Han, W.; Zhang, C.; Wang, H.; Yang, M.; Guo, Y.; Li, G.; Zhang, H.; Wang, C.; Chen, D.; Geng, C.; et al. Alterations of irisin, adropin, preptin and BDNF concentrations in coronary heart disease patients comorbid with depression. Ann. Transl. Med. 2019, 7, 298. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Total (n = 145) | Pulmonary Embolism (n = 90) | Study Group (n = 55) | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Min | Mean ± STD | Max | Min | Mean ± STD | Max | Min | Mean ± STD | Max | ||
| Age (years) | 18 | 61.6 ± 14.30 | 91 | 18 | 62.83 ± 14.49 | 90 | 29 | 59.5 ± 13.84 | 91 | p = 0.182 |
| Gender (N, %) | Male 82 (56.55%) | Female 63 (43.44%) | Male 51 (56.67%) | Female 39 (43.33%) | Male 31 (56.36%) | Female 24 (43.63%) | p = 0.554 | |||
| Systolic blood pressure (mmHg) | 50 | 127.40 ± 21.53 | 200 | 50 | 122.03 ± 22.26 | 200 | 110 | 136.69 ± 16.67 | 185 | p < 0.001 |
| Diastolic blood pressure (mmHg) | 18 | 66.06 ± 13.83 | 110 | 18 | 62.83 ± 14.49 | 91 | 60 | 71.36 ± 10.86 | 110 | p < 0.001 |
| Heart rate (bpm) | 50 | 88.48 ± 19.71 | 150 | 53 | 95.41 ± 19.88 | 150 | 50 | 77.11 ± 13.60 | 111 | p < 0.001 |
| Oxygen saturation in ambient air (%) | 81 | 94.84 ± 4.89 | 100 | 81 | 92.05 ± 4.19 | 99 | 97 | 99.41 ± 0.78 | 100 | p < 0.001 |
| Surgery within 30 days | 11 (7.59%) | 7 (7.78%) | 4 (7.27%) | p = 0.936 | ||||||
| Active cancer | 13 (8.96%) | 11 (12.2%) | 2 (3.63%) | p = 0.089 | ||||||
| Post-partum | 2 (1.38%) | 1 (1.11%) | 1 (1.81%) | p = 0.715 | ||||||
| Diabetes mellitus | 29 (20%) | 16 (17.77%) | 13 (23.63%) | p = 0.365 | ||||||
| Arterial hypertension | 69 (47.58%) | 47 (52.22%) | 22 (40%) | p = 0.184 | ||||||
| Smoking | 46 (31.72%) | 33 (36.67%) | 13 (23.63%) | p = 0.152 | ||||||
| BMI (kg/m2) | 17.16 | 26.06 ± 3.79 | 40.4 | 17.16 | 26.32 ± 4.32 | 40.4 | 20.31 | 25.64 ± 2.68 | 36.45 | p = 0.303 |
| Leucocytes (×109/L) | 4.06 | 9.75 ± 3.57 | 23.9 | 4.06 | 10.32 ± 4.22 | 23.9 | 5.11 | 8.81 ± 1.78 | 15.33 | p = 0.013 |
| Hemoglobin (g/L) | 9.2 | 13.29 ± 1.58 | 17.9 | 9.2 | 13.17 ± 1.77 | 17.9 | 9.2 | 13.48 ± 1.19 | 17 | p = 0.249 |
| Thrombocytes (×109/L) | 93 | 253.51 ± 100.20 | 745 | 96 | 253.45 ± 120.16 | 745 | 93 | 253.61 ± 54.55 | 415 | p = 0.992 |
| CRP (mg/dL) | 0.02 | 5.37 ± 11.77 | 118 | 0.08 | 8 ± 14.29 | 118 | 0.02 | 1.08 ± 1.74 | 11 | p < 0.001 |
| Glucose (mg/dL) | 70 | 113.43 ± 33.53 | 310 | 80 | 117.19 ± 39.34 | 310 | 70 | 107.36 ± 19.84 | 160 | p = 0.09 |
| Creatinine (mg/dL) | 0.42 | 0.97 ± 0.38 | 3.71 | 0.42 | 0.97 ± 0.43 | 3.71 | 0.6 | 0.98 ± 0.27 | 1.77 | p = 0.796 |
| LVEF (%) | 15 | 51.28 ± 7.43 | 65 | 15 | 51.4 ± 7.3 | 65 | 35 | 51.09 ± 0.98 | 65 | p = 0.809 |
| RV diameter (mm) | 22 | 32.69 ± 6.69 | 50 | 24 | 35.7 ± 6.48 | 50 | 22 | 27.7 ± 3.25 | 35 | p < 0.001 |
| TAPSE (mm) | 11 | 20.07 ± 4.15 | 30 | 11 | 18.23 ± 4.03 | 30 | 19 | 23.09 ± 2.03 | 28 | p < 0.001 |
| sPAP (mmHg) | 10 | 26.08 ± 9.63 | 58 | 10 | 28.27 ± 11.05 | 58 | 15 | 22.49 ± 5.03 | 35 | p = 0.232 |
| RV/LV ratio | N/A | ≤1 | >1 | N/A | p < 0.01 | |||||
| 56 (62.2%) | 34 (37.8%) | |||||||||
| Characteristics | PE Patients | ||||
|---|---|---|---|---|---|
| PESI score | Min. | Mean ± STD | Max. | ||
| 20 | 101.13 ± 38.14 | 215 | |||
| PESI stratification | Class I | Class II | Class III | Class IV | Class V |
| 20 (22.2%) | 9 (10%) | 19 (21.1%) | 19 (21.1%) | 23 (25.6%) | |
| sPESI | <1 | ≥1 | |||
| 29 (32.2%) | 61 (67.8%) | ||||
| Thrombolysis | No | Yes | |||
| 69 (76.7%) | 21 (23.3%) | ||||
| Death in 30 days | No | Yes | |||
| 81 (90%) | 9 (10%) | ||||
| Biomarker | PE Group (n = 90) | Control Group (n = 55) | p-Value |
|---|---|---|---|
| D-dimers (µg/mL) | 5.1 (3.05–5.23) | 1.27 (0.67–3.12) | p < 0.001 |
| hsTnI (ng/L) | 24.5 (5.45–75.75) | 4.83 (1.23–12) | p < 0.001 |
| NT-proBNP (pg/mL) | 1482.5 (239–3255) | 86.3 (30–150) | p < 0.001 |
| BDNF (pg/mL) | 403 (252–582) | 644 (576–784) | p < 0.001 |
| Parameter | BDNF | |
|---|---|---|
| r | p-Value | |
| Age | 0.044 | 0.681 |
| Sex | −0.119 | 0.263 |
| BMI | −0.052 | 0.627 |
| Cancer | −1.04 | 0.211 |
| SBP | 0.069 | 0.521 |
| HR | −0.162 | 0.130 |
| Oxygen saturation | 0.076 | 0.479 |
| Hemoglobin | −0.100 | 0.350 |
| Leukocytes | −0.166 | 0.117 |
| Thrombocytes | −0.172 | 0.104 |
| CRP | −0.155 | 0.143 |
| RVd | −0.231 | 0.029 |
| TAPSE | 0.254 | 0.016 |
| sPAP | −0.127 | 0.232 |
| LVEF | 0.126 | 0.235 |
| hs cTnI | −0.038 | 0.723 |
| D-dimers | −0.48 | 0.651 |
| NT-proBNP | −0.275 | 0.009 |
| RV/LV ratio > 1 | −0.154 | 0.149 |
| Biomarker | Odds Ratio | 95% CI for Exp(B) | p-Value | |
|---|---|---|---|---|
| Lower | Upper | |||
| D-dimers | 2.34 | 1.75 | 3.14 | p < 0.01 |
| BDNF | 0.65 | 0.53 | 0.79 | p < 0.01 |
| Biomarker | sPESI < 1 (n = 29) | sPESI ≥ 1 (n = 61) | p-Value | Standard Therapy (n = 69) | Thrombolytic Therapy (n = 21) | p-Value | Survivors (n = 81) | Non-Survivors (n = 9) | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| BDNF | 515 (360–690) | 386 (233–483) | 0.009 | 441 (311–635) | 263 (223–454) | 0.01 | 423 (259–628) | 283 (232–430) | 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haba, M.Ș.C.; Tudorancea, I.; Mihai, C.T.; Onofrei, V.; Costache, I.I.; Petriș, A.O.; Șorodoc, L. Brain-Derived Neurotrophic Factor Expression in Patients with Acute Pulmonary Embolism Compared to the General Population: Diagnostic and Prognostic Implications. J. Clin. Med. 2022, 11, 4948. https://doi.org/10.3390/jcm11174948
Haba MȘC, Tudorancea I, Mihai CT, Onofrei V, Costache II, Petriș AO, Șorodoc L. Brain-Derived Neurotrophic Factor Expression in Patients with Acute Pulmonary Embolism Compared to the General Population: Diagnostic and Prognostic Implications. Journal of Clinical Medicine. 2022; 11(17):4948. https://doi.org/10.3390/jcm11174948
Chicago/Turabian StyleHaba, Mihai Ștefan Cristian, Ionuț Tudorancea, Cosmin Teodor Mihai, Viviana Onofrei, Irina Iuliana Costache, Antoniu Octavian Petriș, and Laurențiu Șorodoc. 2022. "Brain-Derived Neurotrophic Factor Expression in Patients with Acute Pulmonary Embolism Compared to the General Population: Diagnostic and Prognostic Implications" Journal of Clinical Medicine 11, no. 17: 4948. https://doi.org/10.3390/jcm11174948