
Head-Of-Bed Elevation (HOBE) for Improving Positional Obstructive Sleep Apnea (POSA): An Experimental Study
 , , , , , , , ,
, , , , , , , ,  , , , , , , , ,
, , , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
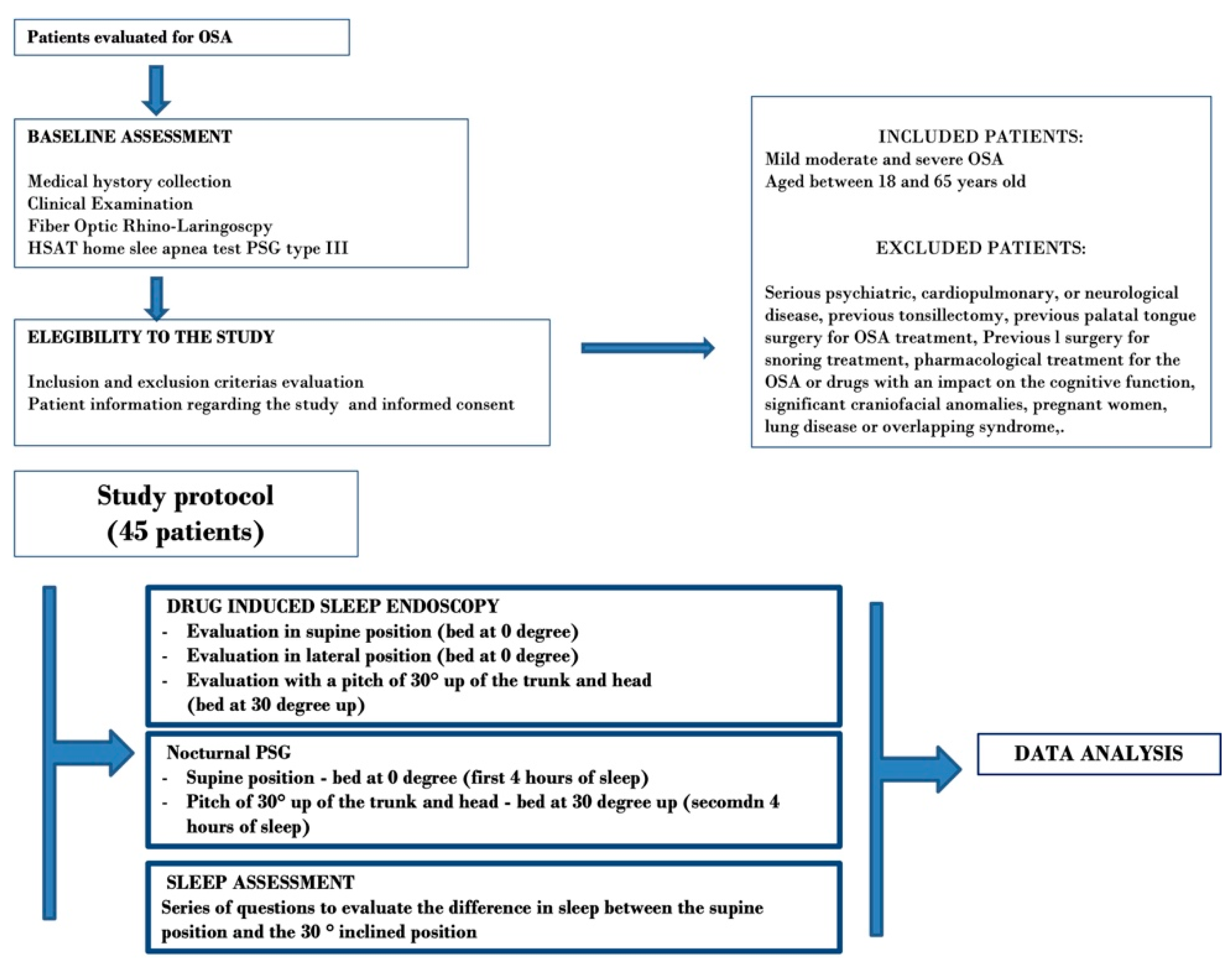
2.1. Trial Design
2.2. Study Protocol
- (1).
- A drug-induced sleep endoscopy (DISE), with evaluation of obstructions and collapse of the upper airways at 0° and in a HOBE position, with a head and trunk elevation of 30°.
- (2).
- Overnight PSG assessment in the hospital, with head and trunk elevation from 0° to 30° during the night.
- (3).
- Questions to evaluate the patients’ feedback to sleeping in HOBE position.
2.3. Drug Induced Sleep Endoscopy (DISE)
2.4. Polysomnography (PSG)
2.5. Feedback of Patients
2.6. Statistical Analysis
3. Results
3.1. DISE Evaluation
3.2. PSG Outcomes
3.3. BMI and 30° up Position
3.4. Lateral Position vs. 30° up Position
3.5. Patient Feedback
4. Discussion
Strengths and Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Iannella, G.; Magliulo, G.; Greco, A.; de Vincentiis, M.; Ralli, M.; Maniaci, A.; Pace, A.; Vicini, C. Obstructive Sleep Apnea Syndrome: From Symptoms to Treatment. Int. J. Environ. Res. Public Health 2022, 19, 2459. [Google Scholar] [CrossRef] [PubMed]
- Patil, S.P.; Schneider, H.; Schwartz, A.R.; Smith, P.L. Adult obstructive sleep apnea: Pathophysiology and diagnosis. Chest 2007, 132, 325–337. [Google Scholar] [CrossRef] [PubMed]
- De Vito, A.; Woodson, B.T.; Koka, V.; Cammaroto, G.; Iannella, G.; Bosi, M.; Pelucchi, S.; Filograna-Pignatelli, G.R.; El Chater, P.; Vicini, C. OSA Upper Airways Surgery: A Targeted Approach. Medicina 2021, 57, 690. [Google Scholar] [CrossRef] [PubMed]
- Epstein, L.J.; Kristo, D.; Strollo, P.J., Jr.; Friedman, N.; Malhotra, A.; Patil, S.P.; Weinstein, M.D. Adult Obstructive Sleep Apnea Task Force of the American Academy of Sleep Medicine. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J. Clin. Sleep Med. 2009, 5, 263–276. [Google Scholar]
- Neill, A.M.; Angus, S.M.; Sajkov, D.; McEvoy, R.D. Effects of sleep posture on upper airway stability in patients with obstructive sleep apnea. Am. J. Respir. Crit. Care Med. 1997, 155, 199–204. [Google Scholar] [CrossRef]
- McEvoy, R.D.; Sharp, D.J.; Thornton, A.T. The effects of posture on obstructive sleep apnea. Am. Rev. Respir. Dis. 1986, 133, 662–666. [Google Scholar]
- Iannella, G.; Magliulo, G.; Lo Iacono, C.A.M. Positional Obstructive Sleep Apnea Syndrome in Elderly Patients. Int. J. Environ. Res. Public Health 2020, 17, 1120. [Google Scholar] [CrossRef]
- Beyers, J.; Vanderveken, O.M.; Kastoer, C.; Boudewyns, A.; De Volder, I.; Van Gastel, A.; Verbraecken, J.A.; De Backer, W.A.; Braem, M.J.; Dieltjens, M.; et al. Treatment of sleep-disordered breathing with positional therapy: Long-term results. Sleep Breath. 2019, 23, 1141–1149. [Google Scholar] [CrossRef]
- Ravesloot, M.J.L.; Vonk, P.E.; Maurer, J.T.; Oksenberg, A.; de Vries, N. Standardized framework to report on the role of sleeping position in sleep apnea patients. Sleep Breath. 2021, 25, 1717–1728. [Google Scholar] [CrossRef]
- Mueller, C.E.; Li, H.; Begasse, S.M.; Sommer, J.U.; Stuck, B.A.; Birk, R. Sleep position, patient comfort, and technical performance with two established procedures for home sleep testing. Sleep Breath. 2021. [CrossRef]
- Souza, F.J.F.B.; Genta, P.R.; de Souza Filho, A.J.; Wellman, A.; Lorenzi-Filho, G. The influence of head-of-bed elevation in patients with obstructive sleep apnea. Sleep Breath. 2017, 21, 815–820. [Google Scholar] [CrossRef] [PubMed]
- Kastoer, C.; Benoist, L.B.L.; Dieltjens, M.; Torensma, B.; de Vries, L.H.; Vonk, P.E.; Ravesloot, M.J.L.; de Vries, N. Comparison of upper airway collapse patterns and its clinical significance: Drug-induced sleep endoscopy in patients without obstructive sleep apnea, positional and non-positional obstructive sleep apnea. Sleep Breath. 2018, 22, 939–948. [Google Scholar] [CrossRef] [PubMed]
- Ravesloot, M.J.; Frank, M.H.; van Maanen, J.P.; Verhagen, E.A.; de Lange, J.; de Vries, N. Positional OSA part 2: Retrospective cohort analysis with a new classification system (APOC). Sleep Breath. 2016, 20, 881–888. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.; Pignanelli, C.; Burr, J. The Effect of Body Position on Measures of Arterial Stiffness in Humans. J. Vasc. Res. 2020, 57, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.B.; Lan, M.Y.; Huang, Y.C.; Huang, T.T.; Lan, M.C. Effect of back-up head-elevated position during drug-induced sleep endoscopy in obstructive sleep apnea patients. Sleep Breath. 2021, 25, 685–693. [Google Scholar] [CrossRef]
- Zaremba, S.; Mueller, N.; Heisig, A.M.; Shin, C.H.; Jung, S.; Leffert, L.R.; Bateman, B.T.; Pugsley, L.J.; Nagasaka, Y.; Duarte, I.M.; et al. Elevated upper body position improves pregnancy-related OSA without impairing sleep quality or sleep architecture early after delivery. Chest 2015, 148, 936–944. [Google Scholar] [CrossRef]
- Skinner, M.A.; Kingshott, R.N.; Jones, D.R.; Homan, S.D.; Taylor, D.R. Elevated posture for the management of obstructive sleep apnea. Sleep Breath. 2004, 8, 193–200. [Google Scholar] [CrossRef]
- Safiruddin, F.; Koutsourelakis, I.; de Vries, N. Upper airway collapse during drug induced sleep endoscopy: Head rotation in supine position compared with lateral head and trunk position. Eur. Arch. Otorhinolaryngol. 2015, 272, 485–488. [Google Scholar] [CrossRef]
- De Vito, A.; Llatas, M.C.; Ravesloot, M.J.; Kotecha, B.; De Vries, N.; Hamans, E.; Maurer, J.; Bosi, M.; Blumen, M.; Heiser, C.; et al. European position paper on drug-induced sleep endoscopy: 2017 Update. Clin. Otolaryngol. 2018, 43, 1541–1552. [Google Scholar] [CrossRef]
- Kezirian, E.J.; Hohenhorst, W.; de Vries, N. Drug-induced sleep endoscopy: The VOTE classification. Eur. Arch. Otorhinolaryngol. 2011, 268, 1233–1236. [Google Scholar] [CrossRef]
- Tagaito, Y.; Isono, S.; Tanaka, A.; Ishikawa, T.; Nishino, T. Sitting posture decreases collapsibility of the passive pharynx in anesthetized paralyzed patients with obstructive sleep apnea. Anesthesiology 2010, 113, 812–818. [Google Scholar] [CrossRef] [PubMed]
- Cary, D.; Jacques, A.; Briffa, K. Examining relationships between sleep posture, waking spinal symptoms and quality of sleep: A cross sectional study. PLoS ONE 2021, 16, e0260582. [Google Scholar] [CrossRef] [PubMed]
- Iannella, G.; Magliulo, G.; Lo Iacono, C.A.M.; Visconti, I.C.; Lechien, J.R.; Perrone, T.; Cammaroto, G.; Meccariello, G.; Maniaci, A.; Cocuzza, S.; et al. Quality of Life and Excessive Daytime Sleepiness in Adults with Obstructive Sleep Apnea Who Are Treated with Multilevel Surgery or Adherent to Continuous Positive Airway Pressure. J. Clin. Med. 2022, 11, 2375. [Google Scholar] [CrossRef] [PubMed]
- Kimoff, R.J.; Cheong, T.H.; Olha, A.E.; Charbonneau, M.; Levy, R.D.; Cosio, M.G.; Gottfried, S.B. Mechanisms of apnea termination in obstructive sleep apnea. Role of chemoreceptor and mechanoreceptor stimuli. Am. J. Respir. Crit. Care Med. 1994, 149, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Vicini, C.; De Vito, A.; Iannella, G.; Gobbi, R.; Corso, R.M.; Montevecchi, F.; Polimeni, A.; De Vincentiis, M.; Meccariello, G.; D’agostino, G.; et al. The aging effect on upper airways collapse of patients with obstructive sleep apnea syndrome. Eur. Arch. Otorhinolaryngol. 2018, 275, 2983–2990. [Google Scholar] [CrossRef]
- Ottaviano, G.; Scadding, G.K.; Iacono, V.; Scarpa, B.; Martini, A.; Lund, V.J. Peak nasal inspiratory flow and peak expiratory flow. Upright and sitting values in an adult population. Rhinology 2016, 54, 160–163. [Google Scholar] [CrossRef]
- Burns, S.M.; Egloff, M.B.; Ryan, B.; Carpenter, R.; Burns, J.E. Effect of body position on spontaneous respiratory rate and tidal volume in patients with obesity, abdominal distension and ascites. Am. J. Crit. Care. 1994, 3, 102–106. [Google Scholar] [CrossRef]
- Hudgel, D.W.; Gordon, E.A.; Thanakitcharu, S.; Bruce, E.N. Instability of ventilatory control in patients with obstructive sleep apnea. Am. J. Respir. Crit. Care Med. 1998, 158, 1142–1149. [Google Scholar] [CrossRef]
- Redolfi, S.; Yumino, D.; Ruttanaumpawan, P.; Yau, B.; Su, M.C.; Lam, J.; Bradley, T.D. Relationship between overnight rostral fluid shift and Obstructive Sleep Apnea in nonobese men. Am. J. Respir. Crit. Care Med. 2009, 179, 241–246. [Google Scholar] [CrossRef]
- Lu, D.; Li, N.; Yao, X.; Zhou, L. Potential inflammatory markers in obstructive sleep apnea-hypopnea syndrome. Bosn J. Basic Med. Sci. 2017, 17, 47–53. [Google Scholar] [CrossRef]
- Gabryelska, A.; Szmyd, B.; Panek, M.; Szemraj, J.; Kuna, P.; Białasiewicz, P. Serum hypoxia-inducible factor-1α protein level as a diagnostic marker of obstructive sleep apnea. Pol. Arch. Intern. Med. 2020, 130, 158–160. [Google Scholar] [CrossRef] [PubMed]
- Gabryelska, A.; Stawski, R.; Sochal, M.; Szmyd, B.; Białasiewicz, P. Influence of one-night CPAP therapy on the changes of HIF-1α protein in OSA patients: A pilot study. J. Sleep Res. 2020, 29, e12995. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PATIENT’S FEATURES | |
|---|---|
| TOTAL PATIENTS 45 | |
| Age | 46.4 ± 14.5 |
| Male | 39 (86.6%) |
| Female | 6 (13.3%) |
| BMI (average value) | 27.2 ± 3.1 |
| Epworth sleepiness scale (average value) | 8.3 ± 4.0 |
| Comorbidities | |
| Hypertension | 12 (26.6%) |
| Diabetes | 2 (4.4%) |
| Heart attack | 1 (2.2) |
| Other cardiovascular comorbidities | 3 (6.6%) |
| BASELINE PSG | |
| AHI | 26.2 ± 9.9 |
| Oxigen Desaturation Index (ODI) | 24.5 ± 9.2 |
| Average SpO2 | 91 ± 5.2 |
| Lower Oxigen Saturation | 81.9 ± 6.1 |
| CT90 | 7.5 ± 3.6 |
| Snoring percentage | 19.3 ± 9.9 |
| Positional patients according to lateral position (Cartwright classification) | 17/45 (37%) |
| DISE EVALUATION | |||||
|---|---|---|---|---|---|
| TOTAL PATIENTS 45 | |||||
| Supine with Bed 0° Degree | Supine Wit Bed 30° Elevated | p-Value (Chi Square Test) | |||
| Number | % | Number | % | ||
| Velum | |||||
| 0 (no obstruction) | - | - | 6 | 13.30% | 0.02 |
| 1 (subtotal obstruction) | 8 | 17.80% | 13 | 28.80% | 0.31 |
| 2 (total obstruction) | 37 | 82.20% | 26 | 57.70% | 0.02 |
| Oropharynx | |||||
| 0 (no obstruction) | 1 | 2.30% | 6 | 13.30% | 0.1 |
| 1 (subtotal obstruction) | 17 | 37.70% | 24 | 53.40% | 0.2 |
| 2 (total obstruction) | 27 | 60% | 15 | 33.30% | 0.01 |
| Tongue base | |||||
| 0 (no obstruction) | 7 | 15.50% | 11 | 24.40% | 0.4 |
| 1 (subtotal obstruction) | 20 | 44.50% | 22 | 48.90% | 0.8 |
| 2 (total obstruction) | 18 | 40% | 12 | 26.60% | 0.2 |
| Epiglottis | |||||
| 0 (no obstruction) | 25 | 55.50% | 26 | 57.70% | >0.05 |
| 1 (subtotal obstruction) | 11 | 24.50% | 12 | 26.70% | >0.05 |
| 2 (total obstruction) | 9 | 20% | 7 | 15.50% | >0.05 |
| PSG OUTCOMES | |||
|---|---|---|---|
| 0 Degree | 30 Degree | p Value Wilcoxon Signed-Rank Test Non Parametric Test | |
| AHI (average value) | 23.8 ± 13.3 | 17.7 ± 12.4 | 0.03 |
| Percentage of Apneas | 55 ± 28.1 | 44 ± 25.8 | 0.05 |
| Percentage of Hypopneas | 45 ± 28.7 | 56 ± 27.1 | 0.05 |
| Oxigen Desaturation Index (ODI) | 21.2 ± 10 | 16.1 ± 11.7 | 0.03 |
| Average SpO2 | 92 ± 3.3 | 93.7 ± 2.2 | 0.02 |
| Lower Oxigen Saturation | 83.4 ± 4.8 | 87.2 ± 3.1 | 0.0001 |
| CT90 | 6.5 ± 4.6 | 5.1 ± 3.4 | 0.1 |
| Snoring percentage | 17.3 ± 11.5 | 12.5 ± 12.6 | 0.05 |
| Patient’s Feedback TOTAL PATIENTS 45 | YES Number | YES Percentage | NO Number | NO Percentage |
|---|---|---|---|---|
| Did you sleep well last night? | 37 | 82.2% | 8 | 17.8% |
| Have you noticed any differences between the second part of sleep in an elevated position and the first part in supine position? | 10 | 22.2% | 35 | 77.8% |
| Do you think that can sleep every night with a Head-of-bed elevation? | 34 | 75.5% | 11 | 24.4% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iannella, G.; Cammaroto, G.; Meccariello, G.; Cannavicci, A.; Gobbi, R.; Lechien, J.R.; Calvo-Henríquez, C.; Bahgat, A.; Di Prinzio, G.; Cerritelli, L.; et al. Head-Of-Bed Elevation (HOBE) for Improving Positional Obstructive Sleep Apnea (POSA): An Experimental Study. J. Clin. Med. 2022, 11, 5620. https://doi.org/10.3390/jcm11195620
Iannella G, Cammaroto G, Meccariello G, Cannavicci A, Gobbi R, Lechien JR, Calvo-Henríquez C, Bahgat A, Di Prinzio G, Cerritelli L, et al. Head-Of-Bed Elevation (HOBE) for Improving Positional Obstructive Sleep Apnea (POSA): An Experimental Study. Journal of Clinical Medicine. 2022; 11(19):5620. https://doi.org/10.3390/jcm11195620
Chicago/Turabian StyleIannella, Giannicola, Giovanni Cammaroto, Giuseppe Meccariello, Angelo Cannavicci, Riccardo Gobbi, Jerome Rene Lechien, Christian Calvo-Henríquez, Ahmed Bahgat, Giuseppe Di Prinzio, Luca Cerritelli, and et al. 2022. "Head-Of-Bed Elevation (HOBE) for Improving Positional Obstructive Sleep Apnea (POSA): An Experimental Study" Journal of Clinical Medicine 11, no. 19: 5620. https://doi.org/10.3390/jcm11195620