
Association between High Lipid Burden of Target Lesion and Slow TIMI Flow in Coronary Interventions
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. PCI and NIRS-IVUS
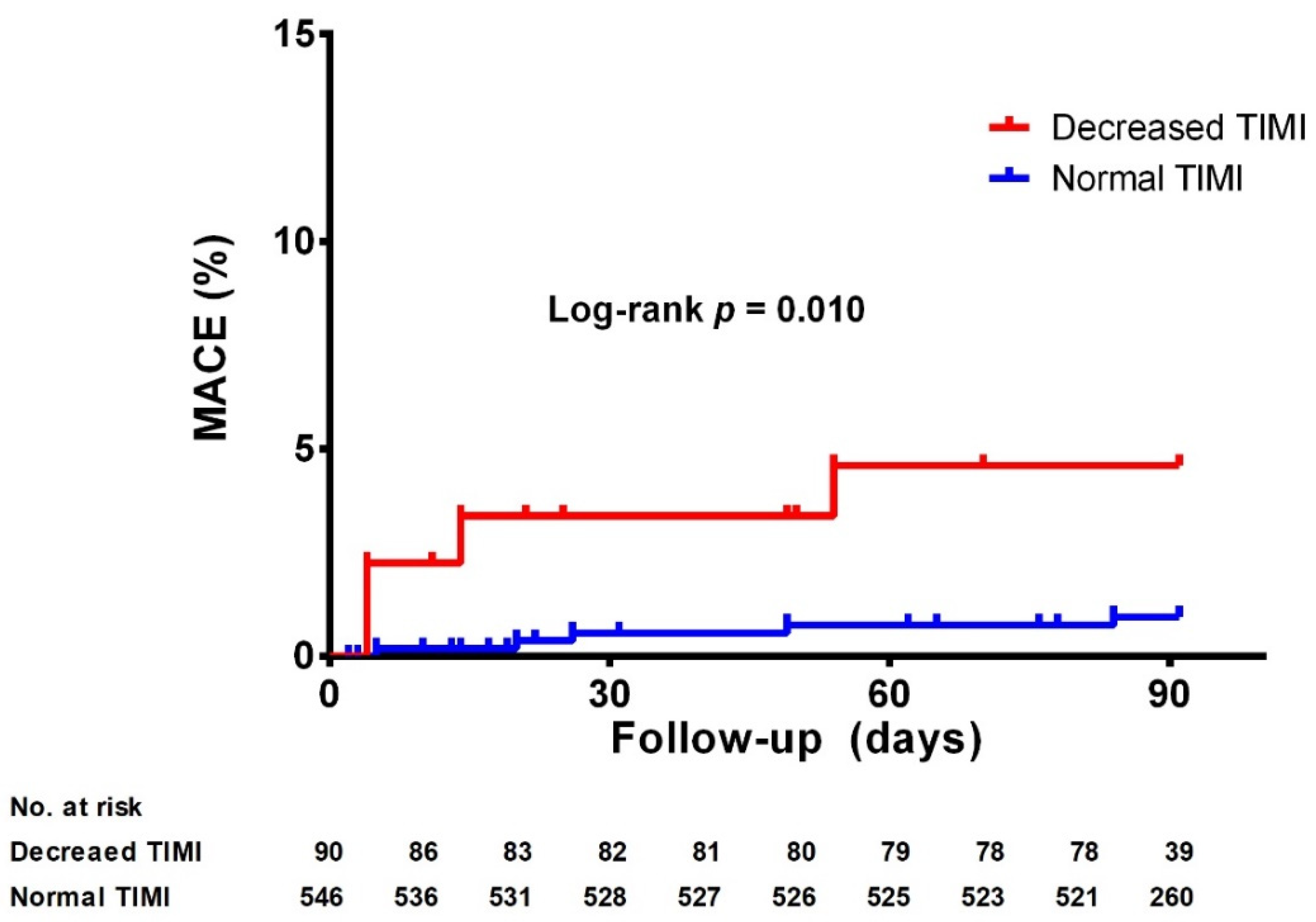
2.3. Clinical Outcomes
2.4. Statistics
3. Results
3.1. Baseline and Lesion Characteristics
3.2. Association between TIMI Flow and maxLCBI4mm
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Investigators, G.A. The effects of tissue plasminogen activator, streptokinase, or both on coronary-artery patency, ventricular function, and survival after acute myocardial infarction. N. Engl. J. Med. 1993, 329, 1615–1622. [Google Scholar] [CrossRef]
- Morishima, I.; Sone, T.; Okumura, K.; Tsuboi, H.; Kondo, J.; Mukawa, H.; Matsui, H.; Toki, Y.; Ito, T.; Hayakawa, T. Angiographic no-reflow phenomenon as a predictor of adverse long-term outcome in patients treated with percutaneous transluminal coronary angioplasty for first acute myocardial infarction. J. Am. Coll. Cardiol. 2000, 36, 1202–1209. [Google Scholar] [CrossRef]
- Harrison, R.W.; Aggarwal, A.; Ou, F.S.; Klein, L.W.; Rumsfeld, J.S.; Roe, M.T.; Wang, T.Y. Incidence and outcomes of no-reflow phenomenon during percutaneous coronary intervention among patients with acute myocardial infarction. Am. J. Cardiol. 2013, 111, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Endo, M.; Hibi, K.; Shimizu, T.; Komura, N.; Kusama, I.; Otsuka, F.; Mitsuhashi, T.; Iwahashi, N.; Okuda, J.; Tsukahara, K.; et al. Impact of ultrasound attenuation and plaque rupture as detected by intravascular ultrasound on the incidence of no-reflow phenomenon after percutaneous coronary intervention in ST-segment elevation myocardial infarction. JACC Cardiovasc. Interv. 2010, 3, 540–549. [Google Scholar] [CrossRef]
- Naghavi, M.; Libby, P.; Falk, E.; Casscells, S.W.; Litovsky, S.; Rumberger, J.; Badimon, J.J.; Stefanadis, C.; Moreno, P.; Pasterkamp, G.; et al. From vulnerable plaque to vulnerable patient: A call for new definitions and risk assessment strategies: Part I. Circulation 2003, 108, 1664–1672. [Google Scholar] [CrossRef]
- Naghavi, M.; Libby, P.; Falk, E.; Casscells, S.W.; Litovsky, S.; Rumberger, J.; Badimon, J.J.; Stefanadis, C.; Moreno, P.; Pasterkamp, G.; et al. From vulnerable plaque to vulnerable patient: A call for new definitions and risk assessment strategies: Part II. Circulation 2003, 108, 1772–1778. [Google Scholar] [CrossRef]
- Erlinge, D.; Maehara, A.; Ben-Yehuda, O.; Bøtker, H.E.; Maeng, M.; Kjøller-Hansen, L.; Engstrøm, T.; Matsumura, M.; Crowley, A.; Dressler, O.; et al. Identification of vulnerable plaques and patients by intracoronary near-infrared spectroscopy and ultrasound (PROSPECT II): A prospective natural history study. Lancet 2021, 397, 985–995. [Google Scholar] [CrossRef]
- Goldstein, J.A.; Grines, C.; Fischell, T.; Virmani, R.; Rizik, D.; Muller, J.; Dixon, S.R. Coronary embolization following balloon dilation of lipid-core plaques. JACC Cardiovasc. Imaging 2009, 2, 1420–1424. [Google Scholar] [CrossRef]
- Gardner, C.M.; Tan, H.; Hull, E.L.; Lisauskas, J.B.; Sum, S.T.; Meese, T.M.; Jiang, C.; Madden, S.P.; Caplan, J.D.; Burke, A.P.; et al. Detection of lipid core coronary plaques in autopsy specimens with a novel catheter-based near-infrared spectroscopy system. JACC Cardiovasc. Imaging 2008, 1, 638–648. [Google Scholar] [CrossRef]
- Cha, J.J.; Hong, S.J.; Lim, S.B.; Joo, H.J.; Park, J.H.; Yu, C.W.; Ahn, T.H.; Lim, D.S. An Overview of Near-Infrared Spectroscopy-Intravascular Ultrasound and Its Applications in Coronary Artery Disease. J. Cardiovasc. Interv. 2022, 1, 1–6. [Google Scholar] [CrossRef]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, K. ‘Ten Commandments’ for the Fourth Universal Definition of Myocardial Infarction 2018. Eur. Heart J. 2019, 40, 226. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Garcia, H.M.; McFadden, E.P.; Farb, A.; Mehran, R.; Stone, G.W.; Spertus, J.; Onuma, Y.; Morel, M.A.; van Es, G.A.; Zuckerman, B.; et al. Standardized End Point Definitions for Coronary Intervention Trials: The Academic Research Consortium-2 Consensus Document. Circulation 2018, 137, 2635–2650. [Google Scholar] [CrossRef]
- Karlsson, S.; Anesater, E.; Fransson, K.; Andell, P.; Persson, J.; Erlinge, D. Intracoronary near-infrared spectroscopy and the risk of future cardiovascular events. Open Heart 2019, 6, e000917. [Google Scholar] [CrossRef]
- Madder, R.D.; Husaini, M.; Davis, A.T.; VanOosterhout, S.; Khan, M.; Wohns, D.; McNamara, R.F.; Wolschleger, K.; Gribar, J.; Collins, J.S.; et al. Large lipid-rich coronary plaques detected by near-infrared spectroscopy at non-stented sites in the target artery identify patients likely to experience future major adverse cardiovascular events. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.L.; Karagounis, L.A.; Becker, L.C.; Sorensen, S.G.; Menlove, R.L. TIMI perfusion grade 3 but not grade 2 results in improved outcome after thrombolysis for myocardial infarction. Ventriculographic, enzymatic, and electrocardiographic evidence from the TEAM-3 Study. Circulation 1993, 87, 1829–1839. [Google Scholar] [CrossRef]
- Ndrepepa, G.; Mehilli, J.; Schulz, S.; Iijima, R.; Keta, D.; Byrne, R.A.; Pache, J.; Seyfarth, M.; Schomig, A.; Kastrati, A. Prognostic significance of epicardial blood flow before and after percutaneous coronary intervention in patients with acute coronary syndromes. J. Am. Coll. Cardiol. 2008, 52, 512–517. [Google Scholar] [CrossRef]
- Maznyczka, A.M.; Carrick, D.; Carberry, J.; Mangion, K.; McEntegart, M.; Petrie, M.C.; Eteiba, H.; Lindsay, M.; Hood, S.; Watkins, S.; et al. Sex-based associations with microvascular injury and outcomes after ST-segment elevation myocardial infarction. Open Heart 2019, 6, e000979. [Google Scholar] [CrossRef]
- Cenko, E.; van der Schaar, M.; Yoon, J.; Kedev, S.; Valvukis, M.; Vasiljevic, Z.; Asanin, M.; Milicic, D.; Manfrini, O.; Badimon, L.; et al. Sex-Specific Treatment Effects After Primary Percutaneous Intervention: A Study on Coronary Blood Flow and Delay to Hospital Presentation. J. Am. Heart Assoc. 2019, 8, e011190. [Google Scholar] [CrossRef] [Green Version]
- Faile, B.A.; Guzzo, J.A.; Tate, D.A.; Nichols, T.C.; Smith, S.C.; Dehmer, G.J. Effect of sex, hemodynamics, body size, and other clinical variables on the corrected thrombolysis in myocardial infarction frame count used as an assessment of coronary blood flow. Am. Heart J. 2000, 140, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Glagov, S.; Weisenberg, E.; Zarins, C.K.; Stankunavicius, R.; Kolettis, G.J. Compensatory enlargement of human atherosclerotic coronary arteries. N. Engl. J. Med. 1987, 316, 1371–1375. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, T.; Mintz, G.S.; De Bruyne, B.; Farhat, N.Z.; Inaba, S.; Cao, Y.; Marso, S.P.; Weisz, G.; Serruys, P.W.; Stone, G.W.; et al. Relationship between left main coronary artery plaque burden and nonleft main coronary atherosclerosis: Results from the PROSPECT study. Coron Artery Dis 2018, 29, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Pagliaro, P.; Penna, C. Hypertension, hypertrophy, and reperfusion injury. J. Cardiovasc. Med. 2017, 18, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Van der Wal, A.C.; Becker, A.E. Atherosclerotic plaque rupture--pathologic basis of plaque stability and instability. Cardiovasc. Res. 1999, 41, 334–344. [Google Scholar] [CrossRef]
- Bourantas, C.V.; Garcia-Garcia, H.M.; Farooq, V.; Maehara, A.; Xu, K.; Genereux, P.; Diletti, R.; Muramatsu, T.; Fahy, M.; Weisz, G.; et al. Clinical and angiographic characteristics of patients likely to have vulnerable plaques: Analysis from the PROSPECT study. JACC Cardiovasc. Imaging 2013, 6, 1263–1272. [Google Scholar] [CrossRef] [PubMed]
- Madder, R.D.; Smith, J.L.; Dixon, S.R.; Goldstein, J.A. Composition of target lesions by near-infrared spectroscopy in patients with acute coronary syndrome versus stable angina. Circ. Cardiovasc. Interv. 2012, 5, 55–61. [Google Scholar] [CrossRef]
- Topol, E.J.; Yadav, J.S. Recognition of the importance of embolization in atherosclerotic vascular disease. Circulation 2000, 101, 570–580. [Google Scholar] [CrossRef]
- Waksman, R.; Di Mario, C.; Torguson, R.; Ali, Z.A.; Singh, V.; Skinner, W.H.; Artis, A.K.; Cate, T.T.; Powers, E.; Kim, C.; et al. Identification of patients and plaques vulnerable to future coronary events with near-infrared spectroscopy intravascular ultrasound imaging: A prospective, cohort study. Lancet 2019, 394, 1629–1637. [Google Scholar] [CrossRef]
- Terada, K.; Kubo, T.; Madder, R.D.; Ino, Y.; Takahata, M.; Shimamura, K.; Shiono, Y.; Nishi, T.; Emori, H.; Higashioka, D.; et al. Near-infrared spectroscopy to predict microvascular obstruction after primary percutaneous coronary intervention. EuroIntervention 2021, 17, e999–e1006. [Google Scholar] [CrossRef]
- Goldstein, J.A.; Maini, B.; Dixon, S.R.; Brilakis, E.S.; Grines, C.L.; Rizik, D.G.; Powers, E.R.; Steinberg, D.H.; Shunk, K.A.; Weisz, G.; et al. Detection of lipid-core plaques by intracoronary near-infrared spectroscopy identifies high risk of periprocedural myocardial infarction. Circ. Cardiovasc. Interv. 2011, 4, 429–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Total | Normal TIMI | Decreased TIMI | p-Value | |
|---|---|---|---|---|
| (n = 636) | (n = 546) | (n = 90) | ||
| Sex (female) | 167 (26.3%) | 157 (28.8%) | 10 (11.1%) | 0.001 |
| Age (years) | 65.5 ± 10.7 | 65.5 ± 10.5 | 65.7 ± 11.5 | 0.876 |
| Hypertension | 389 (61.2%) | 343 (62.8%) | 46 (51.1%) | 0.035 |
| Diabetes mellitus | 205 (32.2%) | 184 (33.7%) | 21 (23.3%) | 0.052 |
| Dyslipidemia | 116 (18.2%) | 105 (19.2%) | 11 (12.2%) | 0.140 |
| Congestive heart failure | 27 (4.2%) | 22 (4.0%) | 5 (18.5%) | 0.506 |
| LV EF (%) | 55.7 ± 8.5 | 55.9 ± 8.4 | 54.3 ± 8.9 | 0.122 |
| Current smoker | 129 (20.3%) | 104 (19.0%) | 25 (27.8%) | 0.123 |
| Family Hx. of CAD | 72 (11.3%) | 65 (11.9%) | 7 (7.8%) | 0.252 |
| Hx. of PCI | 68 (10.7%) | 60 (11.0%) | 8 (8.9%) | 0.713 |
| Hx of CABG | 7 (1.1%) | 7 (1.3%) | 0 (0.0%) | 1.000 |
| Hx of CVA | 78 (12.3%) | 66 (12.1%) | 12 (14.2%) | 0.739 |
| Clinical presentation | 0.063 | |||
| Stable angina | 308 (48.4%) | 270 (49.5%) | 38 (42.2%) | |
| Unstable angina | 249 (39.2%) | 215 (39.4%) | 34 (37.8%) | |
| NSTEMI | 49 (7.7%) | 40 (7.3%) | 9 (10.0%) | |
| STEMI | 30 (4.7%) | 21 (3.8%) | 9 (10.0%) | |
| Presentation as ACS | 328 (51.6%) | 276 (50.5%) | 52 (57.8%) | 0.204 |
| Peak CK-MB (ng/mL) | 3.50 (2.10–9.38) | 3.28 (2.03–7.79) | 8.29 (3.10–50.60) | <0.001 |
| Total | Normal TIMI | Decreased TIMI | p-Value | |
|---|---|---|---|---|
| (n = 636) | (n = 546) | (n = 90) | ||
| Dual antiplatelet therapy | 573 (90.1%) | 489 (89.6%) | 84 (93.3%) | 0.358 |
| ACEI/ARB | 335 (52.7%) | 291 (53.3%) | 44 (48.9%) | 0.508 |
| BB | 238 (37.4%) | 194 (35.5%) | 44 (48.9%) | 0.021 |
| CCB | 255 (40.1%) | 230 (42.1%) | 25 (27.8%) | 0.014 |
| Diuretics | 78 (12.3%) | 69 (12.6%) | 9 (10.0%) | 0.594 |
| Statins | 596 (93.7%) | 508 (93.0%) | 88 (97.8%) | 0.139 |
| Ezetimibe | 175 (27.5%) | 158 (28.9%) | 17 (18.9%) | 0.064 |
| Total | Normal TIMI | Decreased TIMI | p-Value | |
|---|---|---|---|---|
| (n = 636) | (n = 546) | (n = 90) | ||
| Extent of coronary disease | 0.132 | |||
| 0-vessel disease | 3 (0.5%) | 2 (0.4%) | 1 (1.1%) | |
| 1-vessel disease | 289 (45.4%) | 241 (44.1%) | 48 (53.3%) | |
| 2-vessel disease | 196 (30.8%) | 175 (32.1%) | 20 (22.2%) | |
| 3-vessel disease | 148 (23.3%) | 127 (23.3%) | 21 (23.3%) | |
| LM disease | 92 (14.5%) | 84 (15.4%) | 8 (8.9%) | 0.144 |
| Device selection | ||||
| Balloon diameter | 2.5 ± 0.4 | 2.5 ± 0.4 | 2.45 ± 0.3 | 0.627 |
| Stent diameter | 3.4 ± 1.2 | 3.3 ± 1.3 | 3.5 ± 0.6 | 0.302 |
| Stent length | 22.2 ± 7.4 | 22.1 ± 7.4 | 22.9 ± 6.8 | 0.384 |
| Post-balloon diameter | 3.5 ± 0.5 | 3.5 ± 0.5 | 3.6 ± 0.7 | 0.099 |
| IVUS parameter | ||||
| Reference diameter | 3.6 ± 0.6 | 3.6 ± 0.6 | 3.7 ± 0.7 | 0.174 |
| Reference vessel area | 12.7 ± 4.5 | 12.7 ± 4.5 | 14.1 ± 4.7 | 0.002 |
| Minimal luminal diameter | 0.8 ± 0.4 | 0.8 ± 0.4 | 0.7 ± 0.4 | 0.024 |
| Minimal lumen area | 3.0 ± 6.6 | 3.0 ± 7.1 | 2.9 ± 1.3 | 0.854 |
| Area of stenosis | 77.6 ± 13.0 | 77.6 ± 12.2 | 78.0 ± 17.1 | 0.749 |
| Lesion length | 21.2 ± 11.2 | 21.0 ± 11.3 | 22.7 ± 10.6 | 0.190 |
| Minimal stent diameter | 3.1 ± 0.6 | 3.1 ± 0.6 | 3.2 ± 0.6 | 0.113 |
| Target lesion LCBI | ||||
| maxLCBI4mm (pre PCI) | 317 (154–484) | 300 (143–468) | 392 (211–592) | 0.001 |
| maxLCBI4mm (post PCI) | 53 (0–193) | 49 (0–187) | 78 (0–243) | 0.316 |
| Univariable | Multivariable | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Clinical characteristics | ||||||
| Female sex | 0.31 | 0.15–0.61 | 0.001 | 0.15 | 0.05–0.52 | 0.003 |
| Age | 1.00 | 0.98–1.02 | 0.875 | |||
| Hypertension | 0.62 | 0.40–0.97 | 0.036 | 0.51 | 0.27–0.96 | 0.038 |
| Diabetes mellitus | 0.60 | 0.36–1.00 | 0.053 | 0.69 | 0.32–1.46 | 0.329 |
| Dyslipidemia | 0.589 | 0.30–1.14 | 0.114 | 1.00 | 0.40–2.51 | 0.994 |
| Current smoker | 1.76 | 1.02–3.03 | 0.042 | 1.89 | 0.86–4.18 | 0.114 |
| Congestive heart failure | 1.40 | 0.52–3.80 | 0.510 | |||
| Hx of CVD | 1.12 | 0.58–2.17 | 0.739 | |||
| Hx of PCI | 0.79 | 0.36–1.71 | 0.551 | |||
| Hx of CABG | 0.00 | |||||
| FHx of CAD | 0.62 | 0.28–1.41 | 0.256 | |||
| Presentation as ACS | 1.34 | 0.85–2.10 | 0.205 | |||
| Angiographic characteristics | ||||||
| Complex lesion | 0.70 | 0.44–1.10 | 0.081 | 0.60 | 0.30–1.21 | 0.152 |
| LM disease | 1.86 | 0.87–3.99 | 0.109 | 4.88 | 1.10–21.6 | 0.037 |
| pre-PCI maxLCBI4mm ≥ 354 | 2.17 | 1.38–3.42 | 0.001 | 2.59 | 1.33–5.04 | 0.005 |
| Device selection | ||||||
| Balloon diameter | 0.90 | 0.38–2.11 | 0.811 | |||
| Balloon length | 1.18 | 1.06–1.31 | 0.003 | 1.12 | 0.98–1.28 | 0.092 |
| Stent diameter | 1.07 | 0.93–1.23 | 0.350 | |||
| Stent length | 1.05 | 0.98–1.01 | 0.384 | |||
| Post-balloon diameter | 1.57 | 0.97–2.54 | 0.066 | 1.37 | 0.51–3.64 | 0.528 |
| Post-balloon length | 1.01 | 0.93–1.10 | 0.744 | |||
| IVUS parameter | ||||||
| Reference diameter | 1.27 | 0.90–1.81 | 0.175 | 1.03 | 0.43–2.45 | 0.953 |
| Minimal luminal diameter | 0.46 | 0.24–0.90 | 0.024 | 0.30 | 0.10–0.90 | 0.032 |
| Minimal lumen area | 1.00 | 0.96–1.04 | 0.862 | |||
| Area of stenosis | 1.04 | 1.01–1.07 | 0.003 | 1.07 | 1.00–1.15 | 0.065 |
| Lesion length | 1.01 | 0.99–1.03 | 0.192 | |||
| Minimal stent diameter | 1.34 | 0.92–1.97 | 0.131 | 0.91 | 0.32–2.60 | 0.859 |
| Presence of plaque attenuation | 1.76 | 1.12–2.76 | 0.014 | 2.71 | 1.42–5.18 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, S.; Cha, J.-J.; Hong, S.J.; Kim, J.H.; Joo, H.J.; Park, J.H.; Yu, C.W.; Ahn, T.H.; Lim, D.-S. Association between High Lipid Burden of Target Lesion and Slow TIMI Flow in Coronary Interventions. J. Clin. Med. 2022, 11, 5401. https://doi.org/10.3390/jcm11185401
Lim S, Cha J-J, Hong SJ, Kim JH, Joo HJ, Park JH, Yu CW, Ahn TH, Lim D-S. Association between High Lipid Burden of Target Lesion and Slow TIMI Flow in Coronary Interventions. Journal of Clinical Medicine. 2022; 11(18):5401. https://doi.org/10.3390/jcm11185401
Chicago/Turabian StyleLim, Subin, Jung-Joon Cha, Soon Jun Hong, Ju Hyeon Kim, Hyung Joon Joo, Jae Hyoung Park, Cheol Woong Yu, Tae Hoon Ahn, and Do-Sun Lim. 2022. "Association between High Lipid Burden of Target Lesion and Slow TIMI Flow in Coronary Interventions" Journal of Clinical Medicine 11, no. 18: 5401. https://doi.org/10.3390/jcm11185401