
Update on Current Imaging of Systemic Lupus Erythematous in Adults and Juveniles
 ,
,
Abstract
:1. Introduction
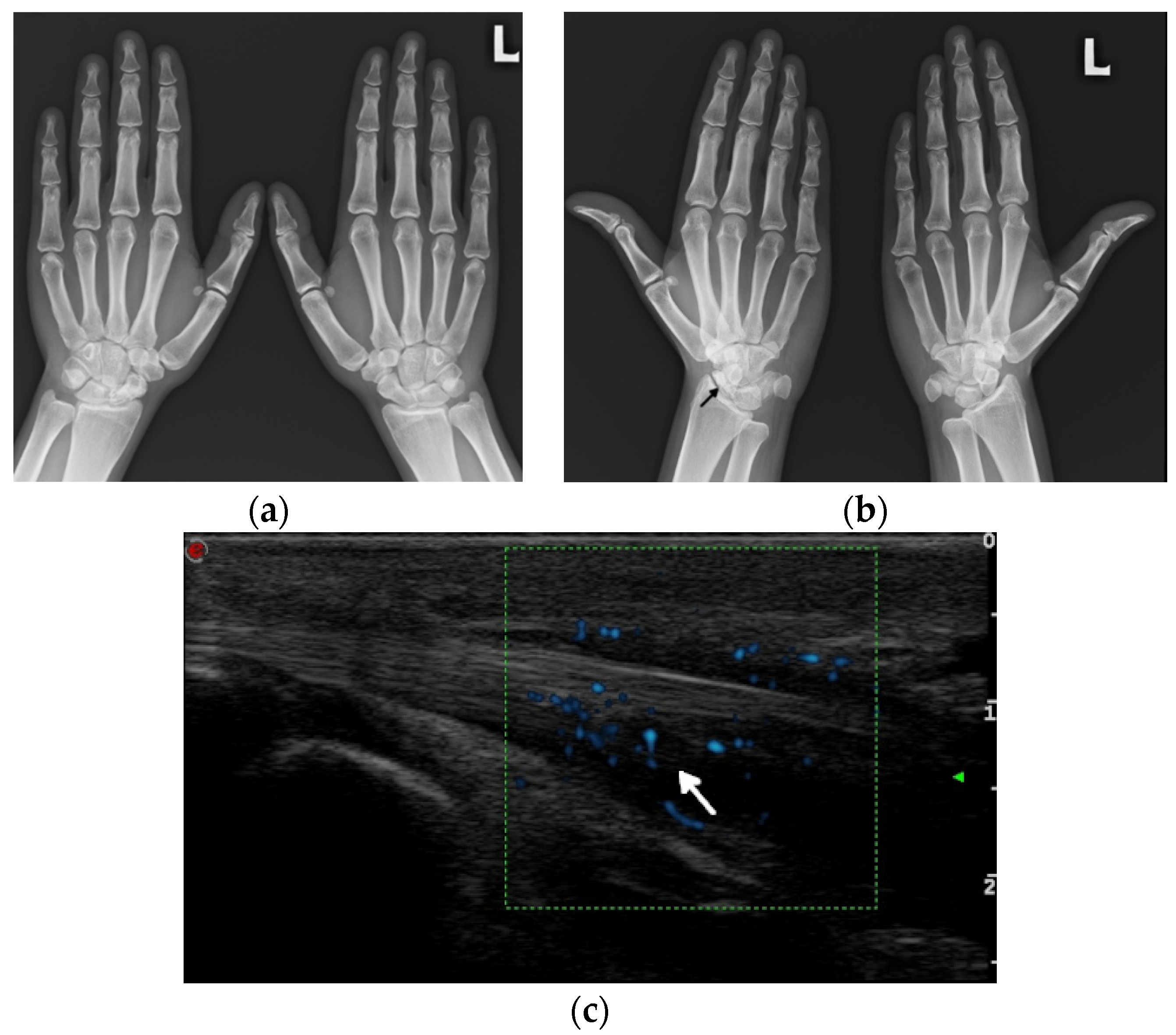
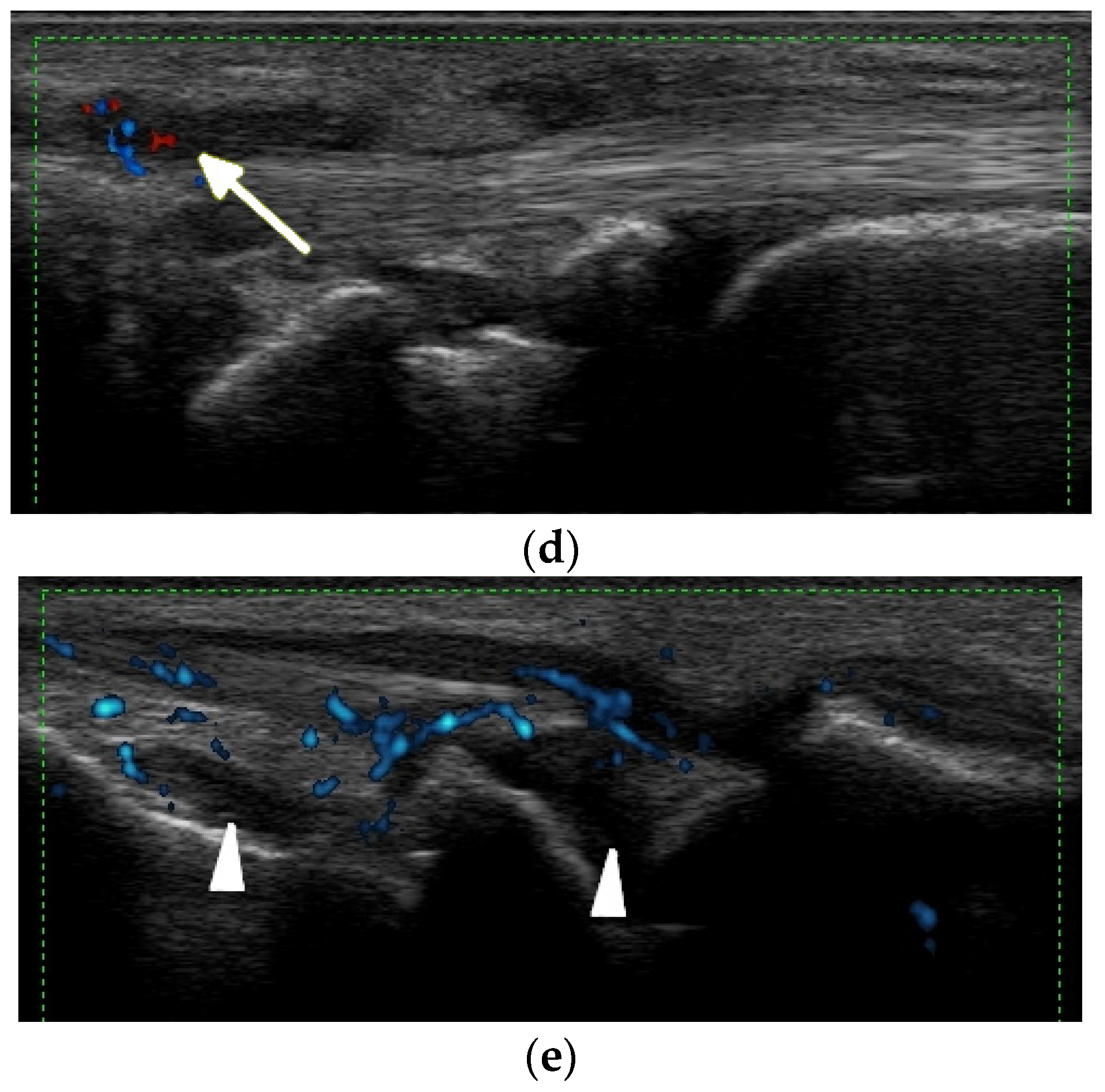
1.1. Nondeforming and Nonerosive Arthritis (NDNE)
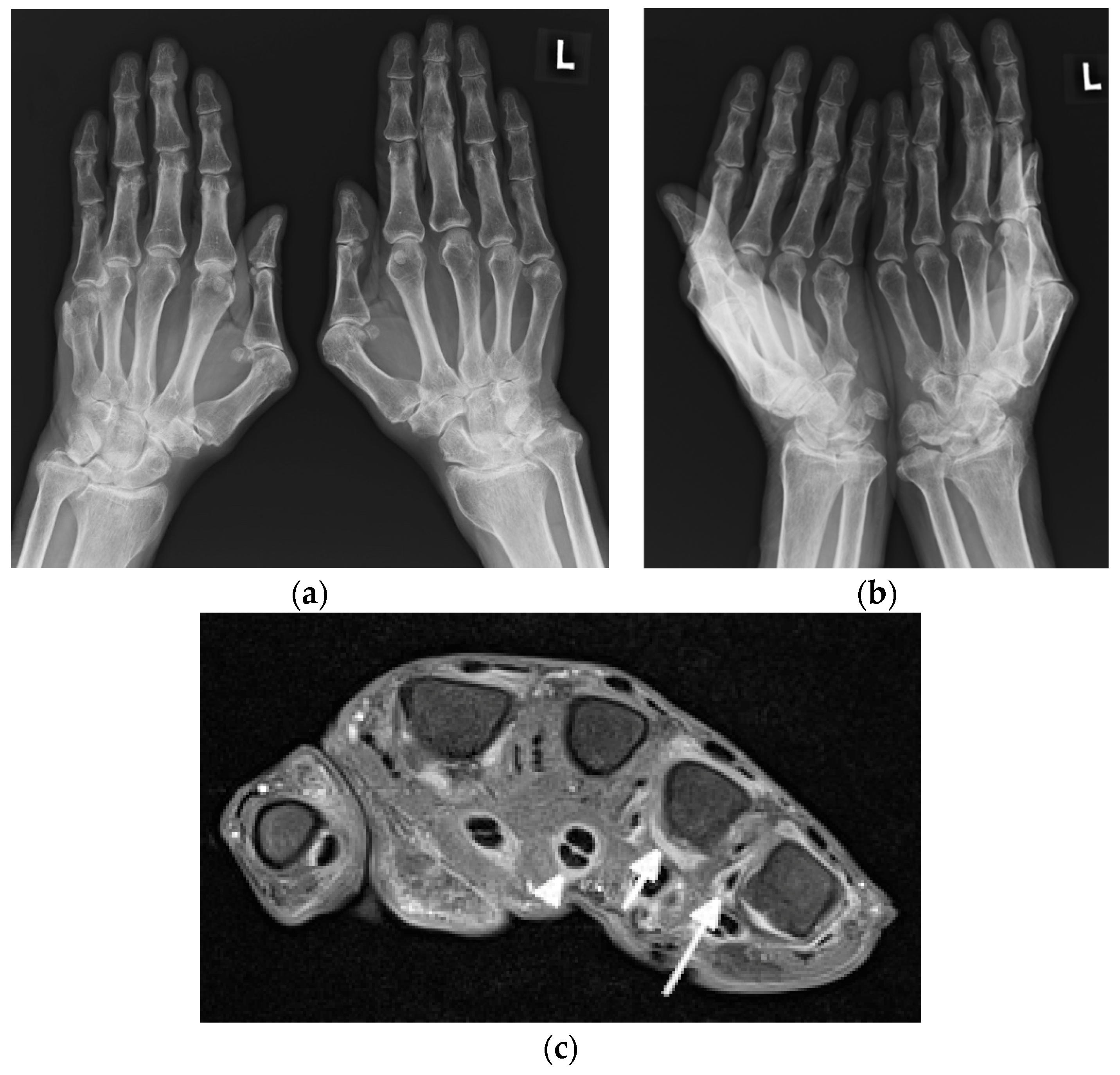
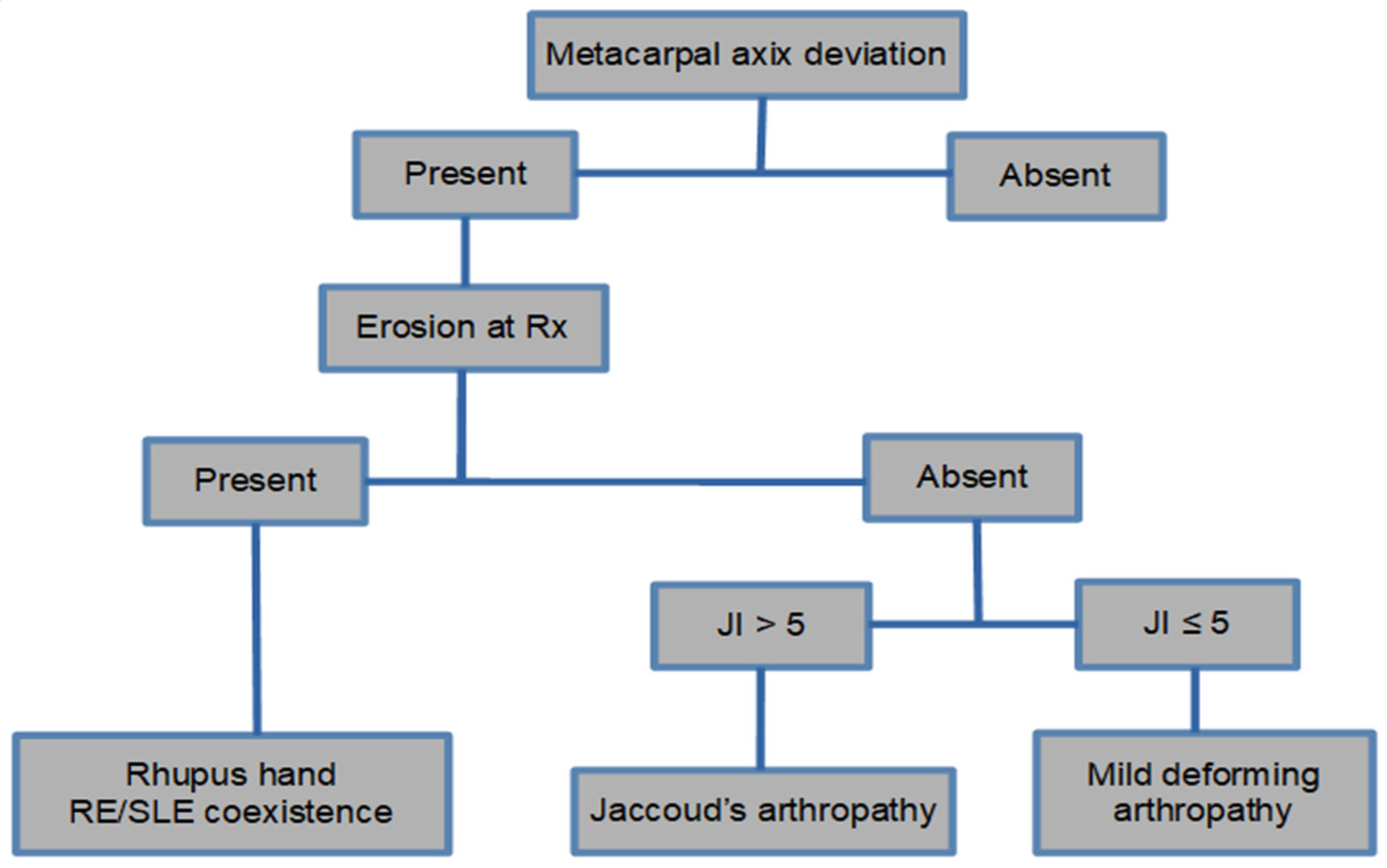
1.2. Deforming Nonerosive Arthropathy/Jaccoud’s Arthropathy (JA)/Lupus Hand
1.3. Erosive Arthropathy, Called Rhupus
2. Update on Imaging of SLE on Radiography, Ultrasonography, and MRI
2.1. Arthritis
2.1.1. Radiography
- Periarticular bone demineralization
- Periarticular soft tissue swelling
- Symmetrical polyarthritis, most commonly involving hands, wrists, knees, feet, and shoulders
- Preserved joint spaces
- Deforming, non-erosive arthropathy (Jaccoud’s arthropathy)
- Occasionally erosive arthropathy (rhupus)
- Acral sclerosis, acroosteolysis in some patients;
- Frequent osteonecrosis, most commonly of the femoral head, as the result of vasculitis and steroid therapy;
- Insufficiency fractures, possible due to disuse demineralization or osteopenia;
- Bacterial and fungal joint infections due to steroid administration and renal disease;
- Myositis, in a small number of patients, sometimes with the presence of calcifications;
- Uncommon spine manifestations, with atlanto-axial subluxation.
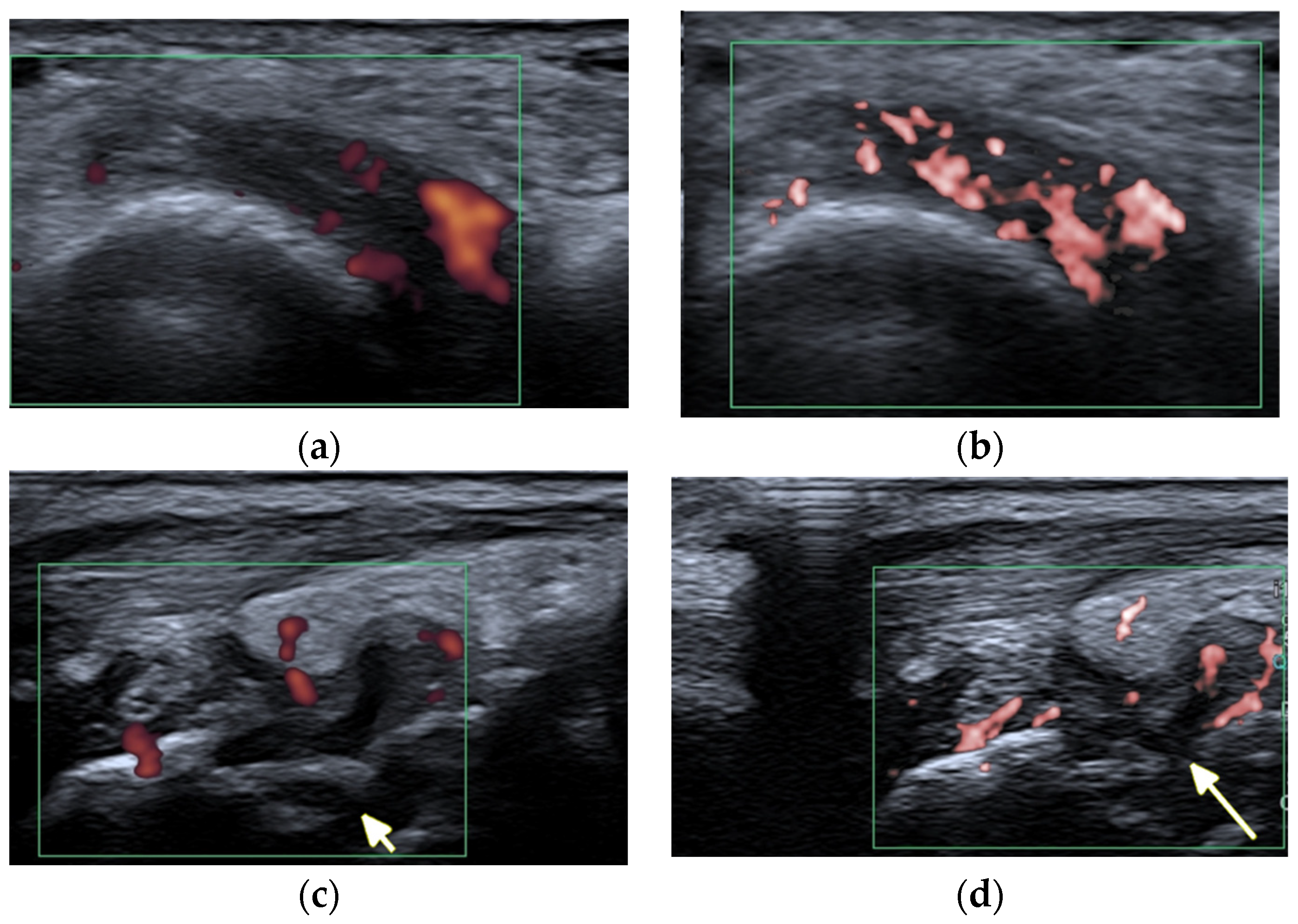
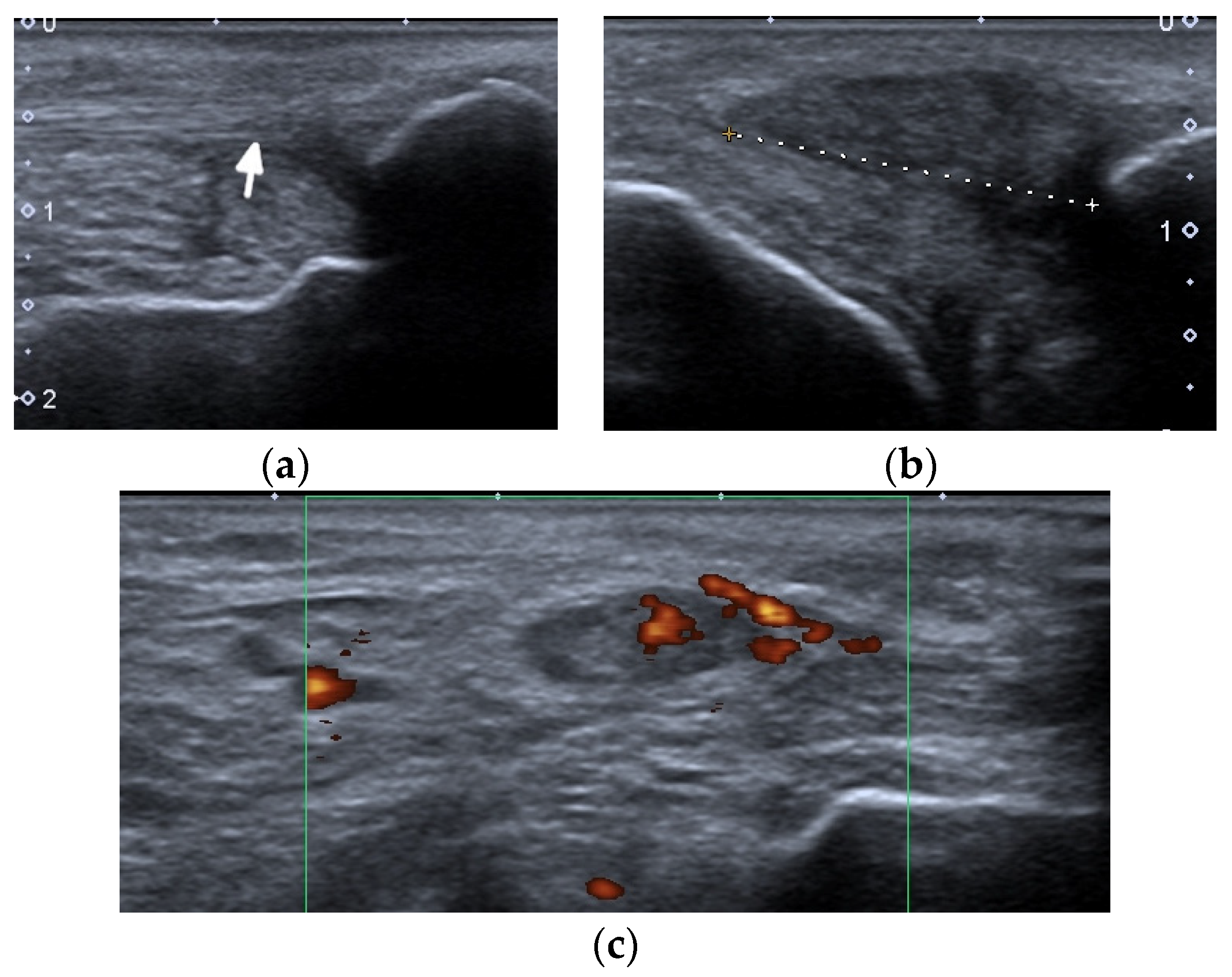
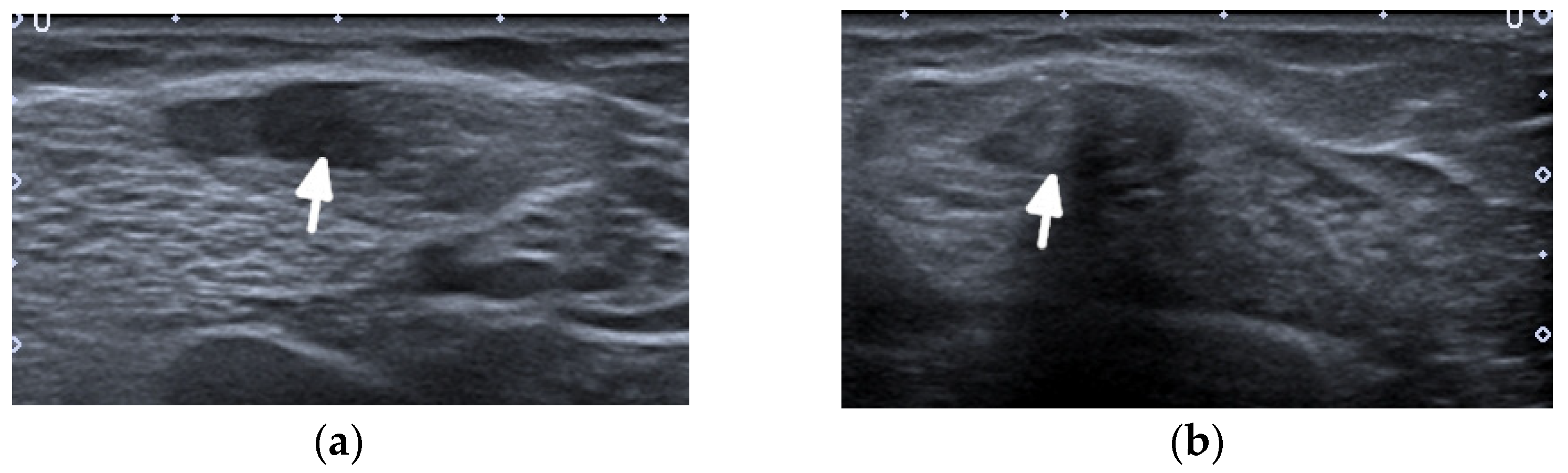
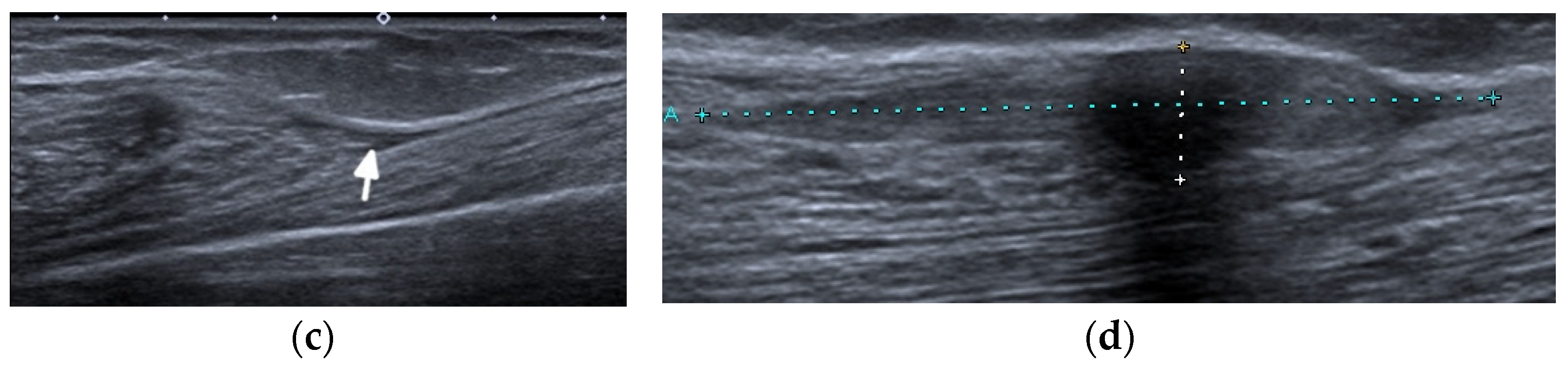
2.1.2. Ultrasound and Magnetic Resonance Imaging
2.2. Tendons
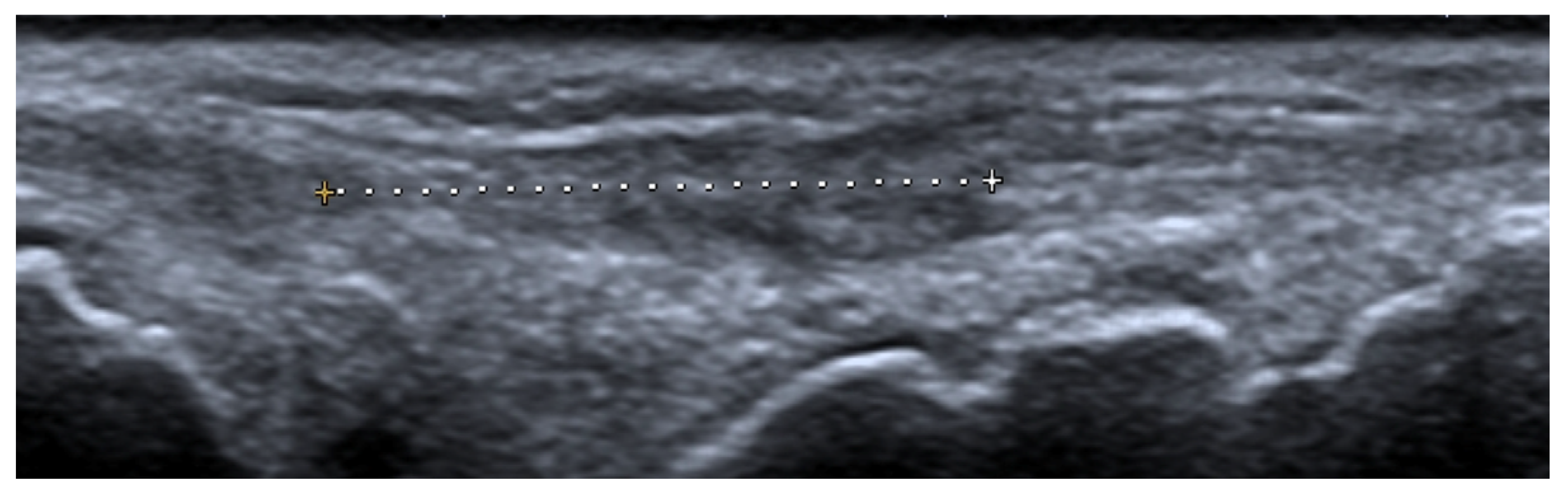
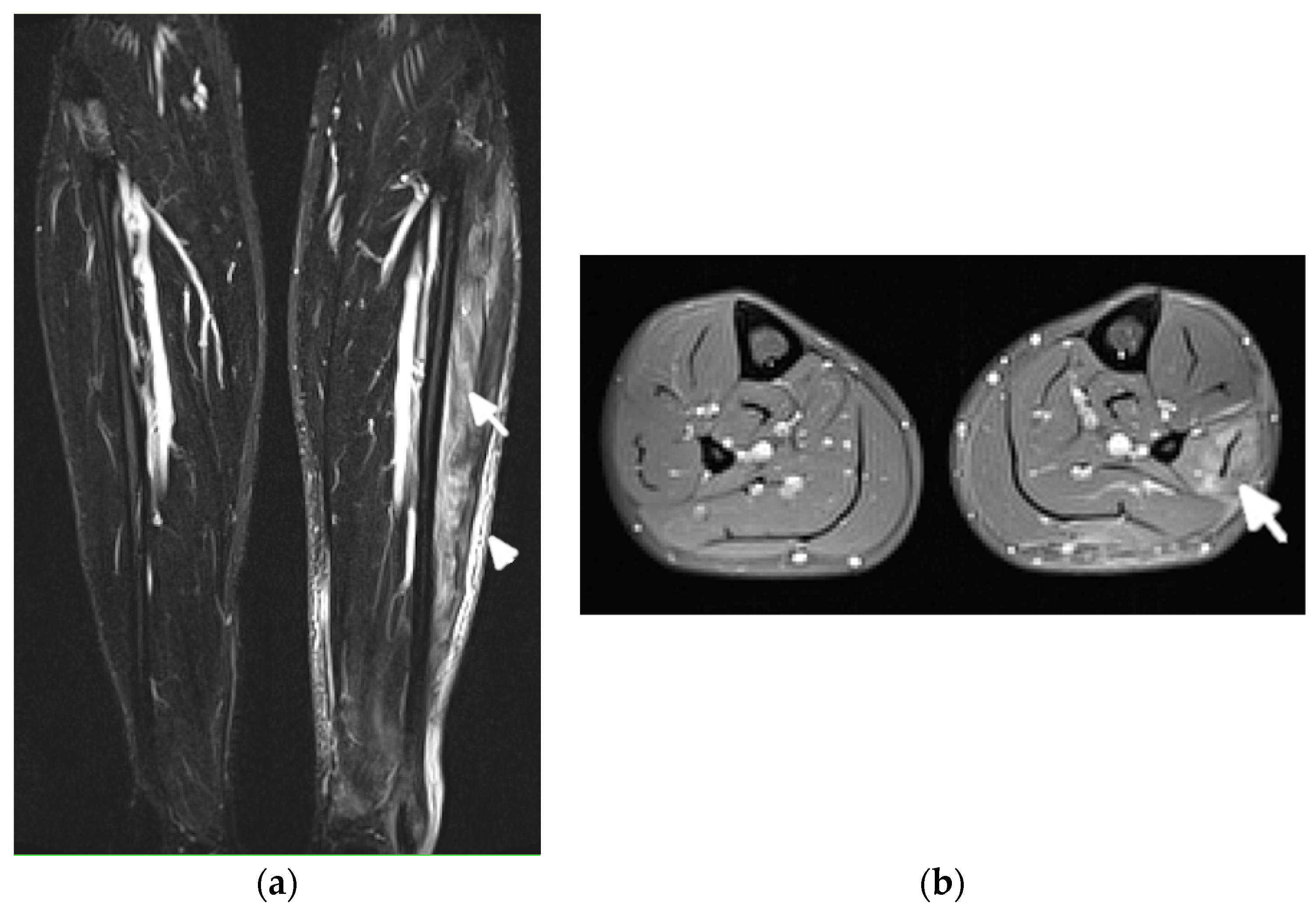
2.3. Myositis
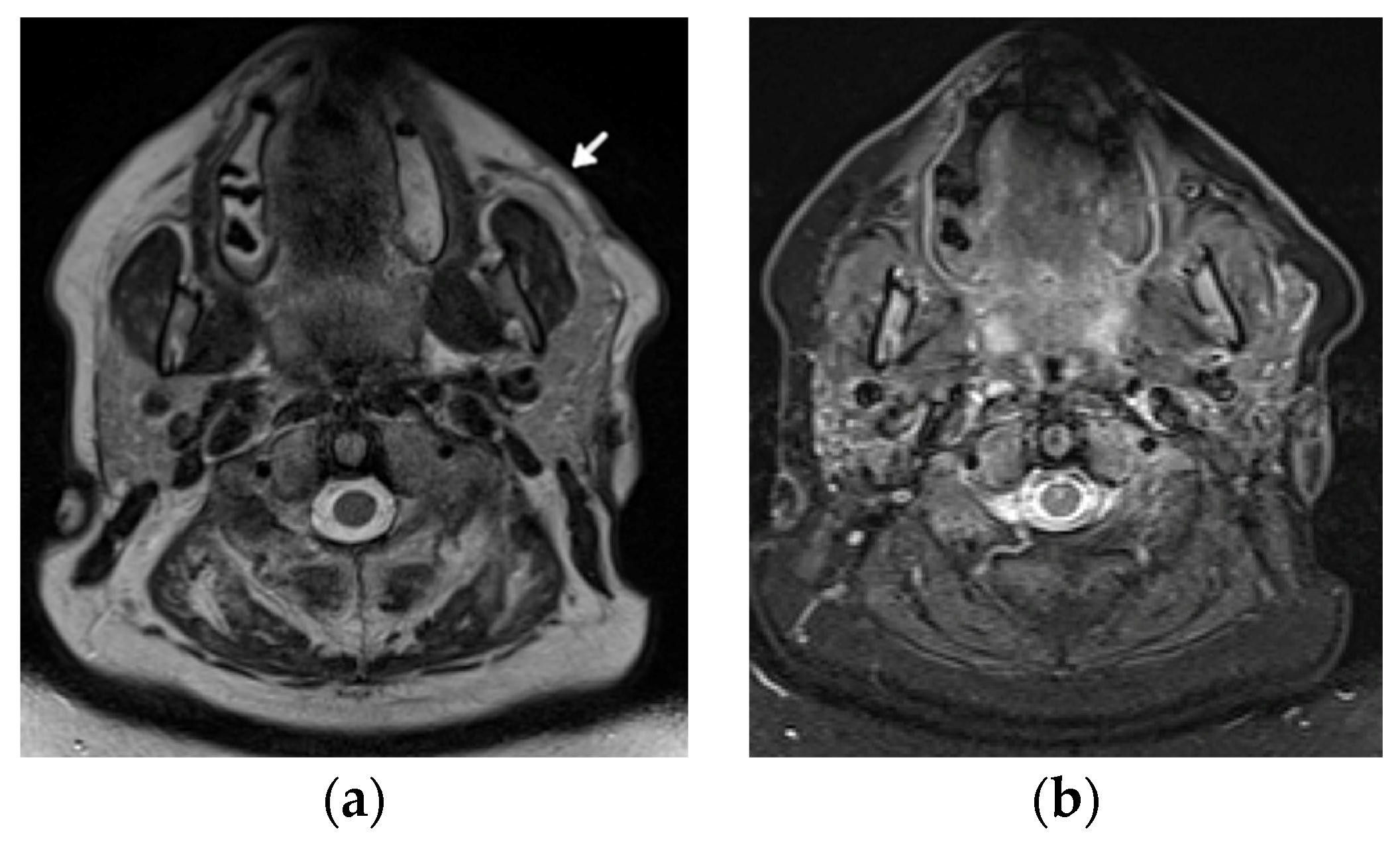
2.4. Adipose Tissue and Lupus Panniculitis
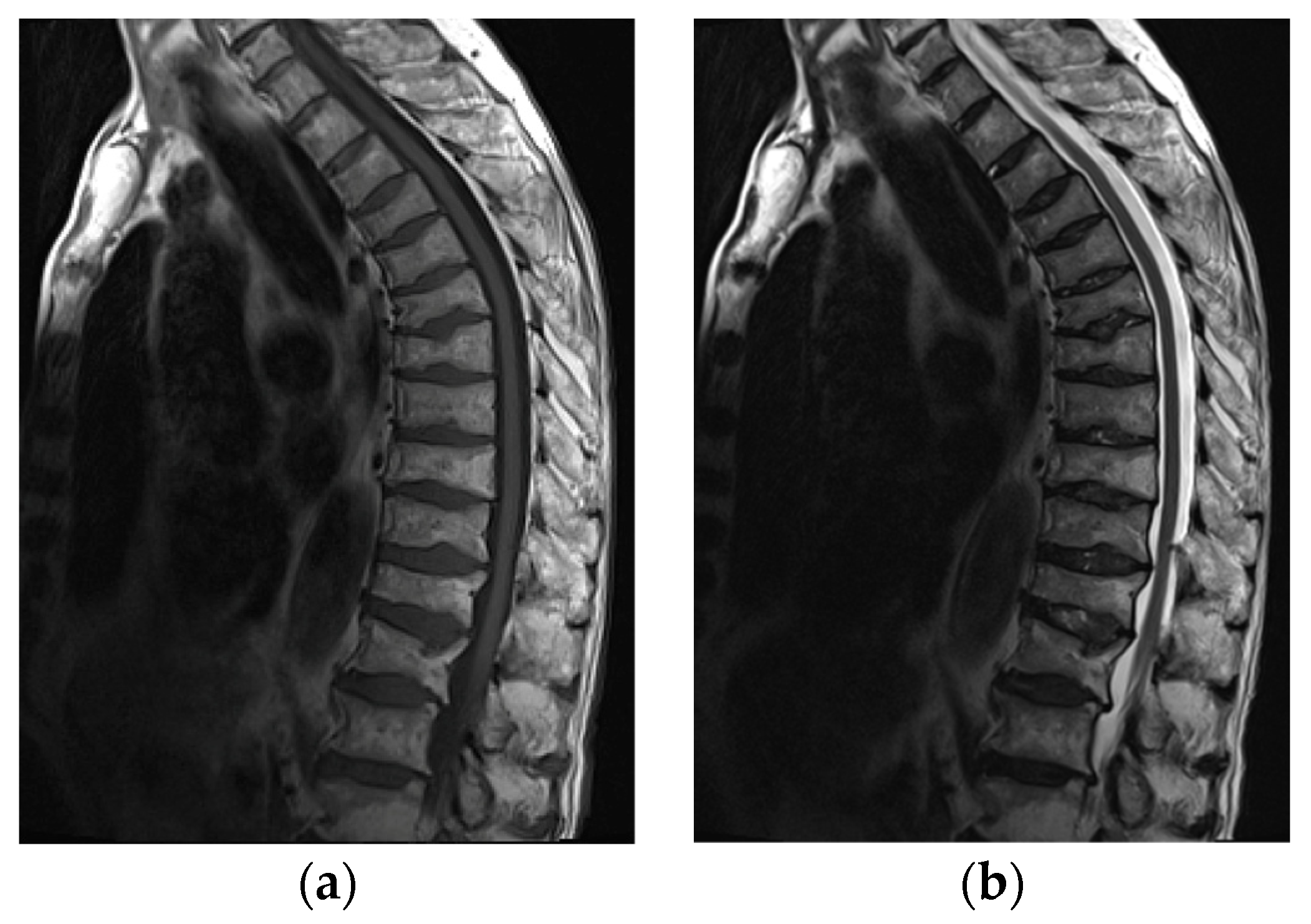
2.5. Bones
2.5.1. Osteonecrosis
2.5.2. Osteoporosis and Insufficiency Fractures
2.5.3. Calcifications and Acro-Osteolysis
3. Special Features of Juvenile Systemic Lupus Erythematosus
3.1. Artricular and Periarticular Abnormalities
3.2. Myositis
3.3. Osteonecrosis and Insufficiency Fracture
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ribeiro, D.S.; de Araújo Neto, C.; D’Almeida, F. Imaging findings of musculoskeletal disorders associated with systemic lupus erythematosus. Radiol. Bras. 2011, 44, 52–58. [Google Scholar] [CrossRef]
- Honghu, T.; Yi, L.; Hua, Z. Comparison of Role of Hand and Wrist Ultrasound in Diagnosis of Subclinical Synovitis in Patients with Systemic Lupus Erythematosus and Rheumatoid Arthritis: A Retrospective, Single-Center Study. Med. Sci. Monit. 2020, 26, e926436. [Google Scholar] [CrossRef]
- Ceccarelli, F.; Perricone, C.; Cipriano, E.; Massaro, L.; Natalucci, F.; Capalbo, G.; Leccese, I.; Bogdanos, D.; Spinelli, F.R.; Alessandri, C.; et al. Joint involvement in systemic lupus erythematosus: From pathogenesis to clinical assessment. Semin. Arthritis Rheum. 2017, 47, 53–64. [Google Scholar] [CrossRef]
- Zollars, E.S.; Hyer, M.; Wolf, B.; Chapin, R. Measuring lupus arthritis activity using contrasted high-field MRI. Associations with clinical measures of disease activity and novel patterns of disease. Lupus Sci. Med. 2018, 5, e000264. [Google Scholar] [CrossRef] [PubMed]
- Greenspan, A. Connective tissue arthropathies. Systemic lupus erythematosus. In Imaging in Rheumatology; Greenspan, A., Gershwin, A.E., Eds.; Wolters Kluwer: Philadelphia, PA, USA, 2018; pp. 310–313. [Google Scholar]
- Weissman, M.D.; Barbara, N. Systemic lupus erythematosus and related conditions and vasculitis syndrome. In Imaging of Arthritis and Metabolic Bone Disease; Weisman, B.N., Ed.; Elsevier: Philadelphia, PA, USA, 2009; pp. 376–382. [Google Scholar]
- Iagnocco, A.; Ceccarelli, F.; Rizzo, C.; Truglia, S.; Massaro, L.; Spinelli, F.R.; Vavala, C.; Valesini, G.; Conti, F. Ultrasound evaluation of hand, wrist and foot joint synovitis in systemic lupus erythematosus. Rheumatology 2013, 53, 465–472. [Google Scholar] [CrossRef] [PubMed]
- A Guillén-Astete, C.; Revenga-Martinez, M.; Zea-Mendoza, A.; Brito-Brito, E. Prevalence of subclinical synovitis of the hand in patients with systemic lupus erythematosus. Lupus 2020, 29, 1423–1429. [Google Scholar] [CrossRef] [PubMed]
- Sudoł-Szopińska, I.; Matuszewska, G.; Pracoń, G. Radiographic Atlas of Inflammatory Rheumatic Diseases; Medisfera: Otwock, Poland, 2022. [Google Scholar]
- Sudoł-Szopińska, I.; Teh, J.; Cotten, A. Rheumatoid Hand and Other Hand-deforming Rheumatic Conditions. Semin. Musculoskelet. Radiol. 2021, 25, 232–245. [Google Scholar] [CrossRef]
- Pracoń, G.; Gómez, M.P.A.; Simoni, P.; Gietka, P.; Sudoł-Szopińska, I. Conventional Radiography and Ultrasound Imaging of Rheumatic Diseases Affecting the Pediatric Population. Semin. Musculoskelet. Radiol. 2021, 25, 68–81. [Google Scholar] [CrossRef]
- Bywaters, E.G.L. The relation between heart and joint disease including “rheumatoid heart disease” and chronic post-rheumatic arthritis (type Jaccoud). Br. Heart J. 1950, 12, 101–131. [Google Scholar] [CrossRef]
- Van Vugt, R.M.; Derksen, R.H.W.M.; Kater, L.; Bijlsma, J.W.J. Deforming arthropathy or lupus and rhupus hands in systemic lupus erythematosus. Ann. Rheum. Dis. 1998, 57, 540–544. [Google Scholar] [CrossRef]
- Piga, M.; Saba, L.; Gabba, A.; Congia, M.; Balestrieri, A.; Mathieu, A.; Cauli, A. Ultrasonographic assessment of bone erosions in the different subtypes of systemic lupus erythematosus arthritis: Comparison with computed tomography. Arthritis Res. Ther. 2016, 18, 222. [Google Scholar] [CrossRef] [PubMed]
- Naredo, E.; Rodriguez-Garcia, S.C.; Terslev, L.; Martinoli, C.; Klauser, A.; Hartung, W.; Hammer, H.B.; Cantisani, V.; Zaottini, F.; Vlad, V.; et al. The EFSUMB Guidelines and Recommendations for Musculoskeletal Ultrasound—Part II: Joint Pathologies, Pediatric Applications, and Guided Procedures. Ultraschall Med. Eur. J. Ultrasound 2021, 43, 252–273. [Google Scholar] [CrossRef]
- Mahmoud, K.; Zayat, A.S.; Yusof, Y.; Dutton, K.; Teh, L.S.; Yee, C.-S.; D’Cruz, D.; Ng, N.; Isenberg, D.; Ciurtin, C.; et al. Ultrasound to identify systemic lupus erythematosus patients with musculoskeletal symptoms who respond best to therapy: The US Evaluation For mUsculoskeletal Lupus longitudinal multicentre study. Rheumatology 2021, 60, 5194–5204. [Google Scholar] [CrossRef]
- Bamber, J.; Cosgrove, D.; Dietrich, C.F.; Fromageau, J.; Bojunga, J.; Calliada, F.; Cantisani, V.; Correas, J.-M.; D’Onofrio, M.; Drakonaki, E.E.; et al. EFSUMB Guidelines and Recommendations on the Clinical Use of Ultrasound Elastography. Part 1: Basic Principles and Technology. Ultraschall Med. 2013, 34, 169–184. [Google Scholar] [CrossRef] [PubMed]
- Alves, E.M.; Macieira, J.C.; Borba, E.; Chiuchetta, F.A.; Santiago, M.B. Spontaneous tendon rupture in systemic lupus erythematosus: Association with Jaccoud’s arthropathy. Lupus 2010, 19, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Endo, Y.; Miller, T.T. Myositis and fasciitis: Role of imaging. Semin. Musculoskelet. Radiol. 2018, 22, 286–298. [Google Scholar]
- Di Matteo, A.; Smerilli, G.; Cipolletta, E.; Wakefield, R.J.; De Angelis, R.; Risa, A.M.; Salaffi, F.; Farah, S.; Villota-Eraso, C.; Maccarrone, V.; et al. Muscle involvement in systemic lupus erythematosus: Multimodal ultrasound assessment and relationship with physical performance. Rheumatology 2022, keac196. [Google Scholar] [CrossRef]
- Kimball, H.; Kimball, D.; Siroy, A.; Tuna, I.; Boyce, B.J.; Albayram, M.S. Novel diagnostic imaging features of facial lupus panniculitis: Ultrasound, CT, and MR imaging with histopathology correlate. Clin. Imaging 2019, 58, 177–181. [Google Scholar] [CrossRef]
- Chan, K.L.; Mok, C.C. Glucocorticoid-Induced Avascular Bone Necrosis: Diagnosis and Management. Open Orrthop. J. 2012, 6, 449–457. [Google Scholar] [CrossRef]
- Bultink, I.E.; Lems, W.F.; Kostense, P.J.; Dijkmans, B.A.C.; Voskuyl, A.E. Prevalence of and risk factors for low bone mineral density and vertebral fractures in patients with systemic lupus erythematosus. Arthritis Rheum. 2005, 52, 2044–2050. [Google Scholar] [CrossRef]
- Fan, Y.L.; Peh, W.C.G. Radiology of Osteoporosis: Old and New Findings. Semin. Musculoskelet. Radiol. 2016, 20, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Bazzocchi, A.; Guglielmi, G. Vertebral Fracture Identification. Semin. Musculoskelet. Radiol. 2016, 20, 317–329. [Google Scholar] [PubMed]
- Braunstein, E.M.; Weissman, B.N.; Sosman, J.L.; Schur, P.H. Radiologic findings in late-onset systemic lupus erythematosus. Am. J. Roentgenol. 1983, 140, 587–589. [Google Scholar] [CrossRef]
- O’Leary, D.; O’Connor, C.; Nertney, L.; MacDermott, E.J.; Mullane, D.; Franklin, O.; Killeen, O.G. Juvenile systemic lupus erythematosus presenting as pancarditis. Pediatr. Rheumatol. 2019, 17, 71. [Google Scholar] [CrossRef] [PubMed]
- Tucker, L.; Uribe, A.; Fernández, M.; Vilá, L.; McGwin, G.; Apte, M.; Fessler, B.; Bastian, H.; Reveille, J.; Alarcón, G. Adolescent onset of lupus results in more aggressive disease and worse outcomes: Results of a nested matched case–control study within LUMINA, a multiethnic US cohort (LUMINA LVII). Lupus 2008, 17, 314–322. [Google Scholar] [CrossRef]
- Levy, D.M.; Kamphuis, S. Systemic Lupus Erythematosus in Children and Adolescents. Pediatr. Clin. N. Am. 2012, 59, 345–364. [Google Scholar] [CrossRef]
- Demirkaya, E.; Özçakar, L.; Türker, T.; Haghari, S.; Ayaz, N.A.; Bakkaloǧlu, A.; Özen, S. Musculoskeletal sonography in juvenile systemic lupus erythematosus. Arthritis Care Res. 2009, 61, 58–60. [Google Scholar] [CrossRef]
- Gurion, R.; for the Atherosclerosis Prevention in Pediatric Lupus Erythematosus Investigators; Tangpricha, V.; Yow, E.; Schanberg, L.E.; McComsey, G.A.; Robinson, A.B. Avascular necrosis in pediatric systemic lupus erythematosus: A brief report and review of the literature. Pediatr. Rheumatol. 2015, 13, 13. [Google Scholar] [CrossRef]
- de Sousa, L.F.A.; Paupitz, J.A.; Aikawa, N.E.; Takayama, L.; Caparbo, V.F.; Pereira, R.M.R. Risk factors for bone loss in juvenile-onset systemic lupus erythematosus: A prospective study. Lupus 2019, 28, 1224–1232. [Google Scholar] [CrossRef]
- Adams, J.E. Bone Densitometry in Children. Semin. Musculoskelet. Radiol. 2016, 20, 254–268. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Jaccoud’s Arthropaty Index (JI) | Number of Affected Fingers | Score |
|---|---|---|
| Ulnar deviation | 1–4 | 2 |
| 5–8 | 3 | |
| ‘Swan-neck’ deformity | 1–4 | 2 |
| 5–8 | 3 | |
| Boutonniere deformity | 1–4 | 2 |
| 5–8 | 3 | |
| ‘Z’ deformity of thumb | 1 | 2 |
| 2 | 3 |
| Magnetic Resonance | Ultrasonography | Radiography | |
|---|---|---|---|
| Imaging | |||
| Effusions | Joint effusions | Periarticular bone demineralization | Nondeforming and nonerosive arthritis |
| Synovial thickening | Synovial thickening Hyperemia | Soft tissue swelling | |
| Postcontrast enhancement | |||
| Periarticular BME | |||
| Capsular inflammation (synovitis) Inflammation of the ligaments, tendon sheaths, tendons (tenosynovitis, tendinitis) | Capsular inflammation (synovitis) Inflammation of the ligaments, tendon sheaths and tendons (tenosynovitis, tendinitis) | Reversible malalignments | Deforming non erosive arthropathy/JA |
| Periarticular BME | |||
| Erosions, synovitis and tenosynovitis, tendinitis, Periarticular BME | Erosions, synovitis, tenosynovitis, tendinitis | Erosions and malaligments | Erosive arthropathy/rhupus |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sudoł-Szopińska, I.; Żelnio, E.; Olesińska, M.; Gietka, P.; Ornowska, S.; Power, D.J.; Taljanovic, M.S. Update on Current Imaging of Systemic Lupus Erythematous in Adults and Juveniles. J. Clin. Med. 2022, 11, 5212. https://doi.org/10.3390/jcm11175212
Sudoł-Szopińska I, Żelnio E, Olesińska M, Gietka P, Ornowska S, Power DJ, Taljanovic MS. Update on Current Imaging of Systemic Lupus Erythematous in Adults and Juveniles. Journal of Clinical Medicine. 2022; 11(17):5212. https://doi.org/10.3390/jcm11175212
Chicago/Turabian StyleSudoł-Szopińska, Iwona, Ewa Żelnio, Marzena Olesińska, Piotr Gietka, Sylwia Ornowska, Deborah Jane Power, and Mihra S. Taljanovic. 2022. "Update on Current Imaging of Systemic Lupus Erythematous in Adults and Juveniles" Journal of Clinical Medicine 11, no. 17: 5212. https://doi.org/10.3390/jcm11175212